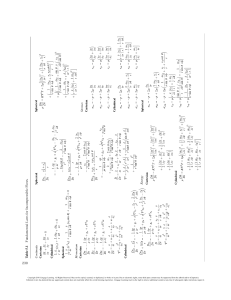
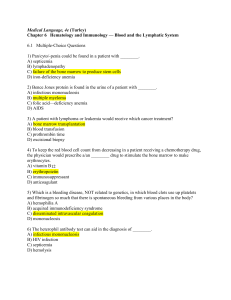
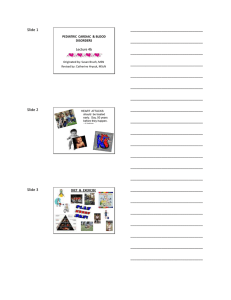
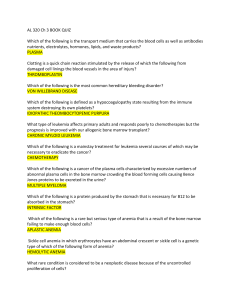
C H A P T E R 7 THE HEMATOLOGIC SYSTEM CHAPTER OUTLINE 88 Anatomy and Physiology of the Hematologic System 89 Blood Transfusions and Blood Products 90 Disorders 87 Copyright 2010 Cengage Learning. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. Due to electronic rights, some third party content may be suppressed from the eBook and/or eChapter(s). Editorial review has deemed that any suppressed content does not materially affect the overall learning experience. Cengage Learning reserves the right to remove additional content at any time if subsequent rights restrictions require it. Anatomy and Physiology of the Hematologic System Bone Marrow A. Found inside all bones in the body; primary function is hematopoiesis (manufacture of blood cells) B. Kinds of bone marrow 1. Red: a. Carries out hematopoiesis b. Found in ribs, vertebral column, and other flat bones 2. Yellow: a. Red marrow that has changed to fat b. Does not carry out hematopoiesis 3. All blood cells start as stem cells in bone marrow. C. Blood A. Plasma 1. Liquid part of blood 2. Yellow in color 3. Consists of serum and fibrinogen 4. Contains plasma proteins B. Red blood cells (RBCs) contain hemoglobin, which is needed to carry oxygen. 1. Normal: male = 4.6 to 6.0 million; female = 4.0 to 5.0 million 2. Decreased RBCs may be caused by hemorrhage, anemias, chronic infections, leukemias, multiple myeloma, chronic renal failure, pregnancy, or overhydration. 3. Increased RBCs may be caused by disease, dehydration, hemoconcentration, high altitudes, chronic obstructive pulmonary disease (COPD), or cardiovascular disease. 4. Hematocrit (Hct): the percentage of blood that is RBCs a. Normal: male = 40% to 54%; female = 36% to 46% b. Decreased level may be caused by acute blood loss, anemias, lymphomas, leukemias, multiple myeloma, malnutrition, vitamin deficiencies, pregnancy, rheumatoid arthritis, or drug toxicity. c. Increased level may be caused by dehydration, hypovolemia, diarrhea, polycythemia vera, diabetic acidosis, COPD, transient ischemic attack (TIA), or eclampsia. 5. Hemoglobin (Hgb): a protein found in RBCs that contains iron, which carries oxygen and gives blood its red color a. Normal: male = 13.5 to 18 g/dL; female = 12 to 16 m/dL 7 88 D. E. F. b. Decreased level may be caused by anemias, hemorrhage, cirrhosis, leukemias, Hodgkin’s disease, cancer, pregnancy, kidney diseases, or drug toxicity. c. Increased level may be caused by dehydration/hemoconcentration, polycythemia, high altitudes, COPD, burns, or drug toxicity. Platelets (thrombocytes): necessary for clotting 1. Normal: 150,000 to 500,000 2. Thrombocytopenia may be caused by leukemias, aplastic anemia, or idiopathic thrombocytopenia purpura (ITP), liver diseases, kidney diseases, or drug toxicity. 3. Increased levels may be caused by polycythemia vera, trauma, acute blood loss, metastatic carcinoma, high altitudes, or severe exercise. White blood cells (WBCs): part of the body’s defense system to fight infections 1. Also called neutrophils or leukocytes 2. Normal: 5000 to 10000 3. Leukopenia (low WBC) is a common side effect of chemotherapy treatment. 4. Leukocytosis (too many WBCs) may indicate an infection. Blood groups 1. RBCs carry antigens, which determine the blood groups. 2. ABO groups a. Client has A antigens (type A blood), B antigens (type B blood), both A and B antigens (type AB blood), or no antigens (type O blood). b. If a person receives blood with A or B antigens that are not in their own blood, RBC antibodies are formed against them. Rh typing 1. Identifies presence (Rh positive) or absence (Rh negative) of Rh antigen 2. Anti-Rh antibodies are not automatically formed in an Rh-negative person, but if Rh-positive blood is given, antibody formation starts and a second exposure to the Rh antigen will trigger a transfusion reaction. SPLEEN A. Largest lymphatic organ; lies beneath the diaphragm, behind and to the left of the stomach B. Functions NCLEX-PN® Review Copyright 2010 Cengage Learning. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. Due to electronic rights, some third party content may be suppressed from the eBook and/or eChapter(s). Editorial review has deemed that any suppressed content does not materially affect the overall learning experience. Cengage Learning reserves the right to remove additional content at any time if subsequent rights restrictions require it. 1. Blood filtration system and reservoir 2. Important hematopoietic site in fetus; postnatally produces monocytes and lymphocytes 3. Important in phagocytosis; removes old and misshapen RBCs 4. Involved in antibody production by plasma cells 5. Involved in iron metabolism 6. In an adult, functions of the spleen can be taken over by the reticuloendothelial system if spleen is removed. Blood Transfusions and Blood Products A. Purpose 1. Improve oxygen transport—RBCs 2. Volume expansion—whole blood, plasma, and albumin 3. Provide proteins—fresh frozen plasma, albumin, and plasma protein fraction 4. Coagulation factors—cryoprecipitate, fresh frozen plasma, and fresh whole blood 5. Platelets—platelet concentrate and fresh whole blood B. Types of blood and blood products 1. Whole blood a. Provides all components b. Takes 12 to 24 hours for Hgb and Hct to rise c. Volume overload can occur from large volume. d. Complications include hepatitis, acquired immunodeficiency syndrome (AIDS), transfusion reaction, sodium (Na) and potassium (K) excess, and calcium depletion from citrate (preservative) in massive transfusions. e. Usually administered at rate of three to four hours for 1 unit 2. RBCs (packed RBCs) a. RBCs provide twice the amount of Hgb as an equivalent amount of whole blood. b. Complications include transfusion reactions; less frequently than with whole blood because plasma proteins are not given c. Takes two to four hours to administer 1 unit 3. Fresh frozen plasma a. Contains all coagulation factors b. Can be stored for 12 months c. Takes 20 minutes to thaw and then is hung immediately and infused quickly because it loses its coagulation factors rapidly at room temperature 4. Platelets a. Will raise the recipient’s platelet count by 10,000/L b. One unit pooled from 4 to 8 units of whole blood c. Single donor platelet transfusions may be necessary for clients who have developed antibodies; may need compatibility testing d. Infused quickly 5. Factor VIII fractions (cryoprecipitate) a. Contains factor VIII, fibrinogen, and factor XIII b. Used in the treatment of hemophilia c. Infused quickly C. Management of clients receiving blood products 1. Determine a prior history of transfusions or transfusion reactions. 2. 18- or 19-gauge needle used 3. Sodium chloride always used as intravenous (IV) solution; never use dextrose solution; dextrose causes agglutination of blood cells 4. Two nurses (usually registered nurses [RNs]) MUST verify ABO group, Rh type, patient and blood numbers, and expiration date. 5. Before starting transfusion, take baseline vital signs including temperature. 6. Initially, infusion rate is 2 cc/min. 7. Stay with client for first 15 minutes and monitor vital signs, including temperature, frequently (temperature elevation suggests a transfusion reaction). 8. Monitor for transfusion reactions: a. Hemolytic (1) Causes (a) ABO or Rh incompatibility (antibodies in recipient plasma react with antigen in donor cells) (b) Use of dextrose solutions (agglutinated cells block capillary blood flow) (2) Manifestations include headache, lumbar or sternal pain, nausea, vomiting, chills, flushing, jaundice, dyspnea, signs of shock, renal shutdown, or disseminated intravascular coagulation (DIC). (3) Stop IV infusion; saline IV; send blood unit and client blood to the lab b. Allergic (1) Transfer of an antigen or antibody from donor or recipient; client has immune sensitivity to foreign serum protein; allergic donors 7 THE HEMATOLOGIC SYSTEM 89 Copyright 2010 Cengage Learning. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. Due to electronic rights, some third party content may be suppressed from the eBook and/or eChapter(s). Editorial review has deemed that any suppressed content does not materially affect the overall learning experience. Cengage Learning reserves the right to remove additional content at any time if subsequent rights restrictions require it. (2) Manifestations are allergies—urticaria, laryngeal edema, wheezing, dyspnea, bronchospasm, or anaphylaxis (3) Stop transfusion; give antihistamine and epinephrine as ordered. 9. Document carefully. Include type of blood component, blood unit number, date and time infusion starts and ends, amount infused, client reaction, and vital signs. Disorders ANEMIAS Anemia is an insufficient number of RBCs. Anemia can be caused by blood loss, manufacture of insufficient RBCs, or abnormal destruction of RBCs. Iron Deficiency Anemia A. Chronic microcytic (little cells), hypochromic (little color) anemia caused by either inadequate absorption or excessive loss of iron B. Assessment 1. Fatigue, dizziness 2. Pallor 3. Cold sensitivity 4. Palpitations 5. Brittle hair and nails 6. Decreased Hgb, Hct, and RBC C. Nursing diagnoses (Table 7–1) D. Management 1. Assess for bleeding; stool for occult blood 2. Rest 3. Iron administration a. Intramuscular (IM); give Z track deep IM; do not massage after IM injection; encourage walking b. Oral (1) Preferred route (2) Liquid stains teeth; administer with a straw. (3) Give WITH meals to decrease gastrointestinal (GI) irritation. c. Increase intake of iron-containing foods (1) Iron-containing foods include meats, egg yolks, green leafy vegetables, raisins, enriched breads, and cereals. Table 7–1 Nursing Diagnoses Related to Anemia • Activity intolerance related to impaired oxygen transport secondary to diminished RBC count • Deficient knowledge Source: Delmar/Cengage Learning 7 90 (2) Give iron foods with vitamin C to enhance absorption of iron. Pernicious Anemia A. Chronic, progressive anemia caused by a deficiency of vitamin B12 in the blood stream. The most common cause is deficiency of intrinsic factor, which is normally produced by the gastric mucosa. 1. Intrinsic factor is necessary for the absorption of vitamin B12 into the blood stream. 2. Vitamin B12 deficiency diminishes DNA synthesis, which results in defective maturation of RBCs and GI tract cells and poor functioning of the nervous system. 3. Factors related to development of pernicious anemia a. Aging b. Immune system destroys stomach (parietal) cells that produce intrinsic factor. c. Gastric surgery such as gastrectomy and gastric bypass d. Intestinal disease such as Crohn’s disease that decreases absorption of vitamin B12 from the intestines B. Assessment 1. Anemia and pallor 2. Fatigue 3. Sore mouth and beefy red tongue 4. Decreased hydrochloric acid (HCl) in stomach 5. Paresthesias and paralysis 6. Depression and psychosis C. Diagnosis 1. Complete blood count (CBC) and blood studies to detect anemia, vitamin B12 levels, and homocysteine levels (elevated in pernicious anemia) 2. Gastric analysis to determine HCl level 3. Schilling test a. Radioactive vitamin B12 given orally (PO) b. 24-hour urine collected; decreased amount of vitamin B12 in urine if pernicious anemia D. Nursing diagnoses (Table 7–1) E. Management NCLEX-PN® Review Copyright 2010 Cengage Learning. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. Due to electronic rights, some third party content may be suppressed from the eBook and/or eChapter(s). Editorial review has deemed that any suppressed content does not materially affect the overall learning experience. Cengage Learning reserves the right to remove additional content at any time if subsequent rights restrictions require it. 1. Vitamin B12 administration for life as monthly injections, gel or nasal spray, or patches 2. Iron and folic acid 3. Transfusions if severe Aplastic Anemia A. Depression of WBC, RBC, and platelet production due to bone marrow destruction; can be either idiopathic or secondary; secondary causes include chemical toxins, drugs (chloramphenicol), radiation, and immunologic therapy B. Assessment 1. Fatigue and dyspnea (due to decreased RBCs) 2. Infections (due to decreased WBCs) 3. Bleeding tendencies (due to decreased platelets) 4. Bone marrow biopsy shows fatty marrow with few developing cells. C. Management 1. Remove offending agent 2. Blood transfusions 3. Prevent and treat infections: a. Protective isolation b. High-protein, high-vitamin diet c. Good mouth care 4. Bone marrow transplant 5. Prevent and treat bleeding episodes: a. Use a soft toothbrush and electric razor b. No IM injections c. Observe for bleeding D. Management 1. Eliminate causative factors if possible. 2. Corticosteroids (autoimmune types) 3. Folic acid to assist in RBC production 4. Transfusions 5. Splenectomy (in adults; children need spleen for antibody formation) Sickle Cell Anemia A. Most common inherited disorder in African American population; 10% of African Americans have sickle cell trait B. Transmitted as autosomal recessive gene (Figure 7–1) 1/4 25% 2/4 50% 1/4 25% Dark side of circle = sickle cell trait Hemolytic Anemia A. Anemia caused by increased destruction of RBCs; can be inherited (sickle cell anemia or thalassemia), acquired (transfusion reaction), or of an unknown cause B. Assessment 1. Pallor due to decreased RBCs; jaundice as a result of rapid destruction of RBCs 2. Fatigue due to decreased RBCs 3. Chills, fever, and pain 4. Hematuria 5. Decreased Hgb and Hct C. Nursing diagnoses (Table 7–2) Table 7–2 Nursing Diagnoses Related to Sickle Cell Anemia • • • • • • • • • Activity intolerance Ineffective health maintenance Impaired gas exchange Risk for ineffective gastrointestinal perfusion Risk for ineffective renal perfusion Risk for decreased cardiac tissue perfusion Acute pain Deficient knowledge Disabled family coping Source: Delmar/Cengage Learning Figure 7–1 Sickle cell anemia: method of inheritance. Source: Delmar/Cengage Learning 1. Both parents must carry the gene for a child to develop the condition. 2. When both parents carry the gene, there is a 25% chance with each pregnancy of having a child with the disorder; a 50% chance with each pregnancy of having a child who is a carrier; and a 25% chance with each pregnancy of having a child who will be disease and carrier free. 3. Inherited diseases transmitted as autosomal recessive include sickle cell anemia, cystic fibrosis, phenylketonuria (PKU), and TaySachs. C. Pathophysiology (Figure 7–2) 1. Structure of Hgb is changed; Hgb S contains deformed, rigid, S-shaped cells and has reduced oxygen-carrying capacity; Hgb S replaces all or part of Hgb in RBCs. 2. When oxygen is released, the shape of the RBCs changes from round and pliable to crescentshaped, rigid, and inflexible. 3. RBCs live for six to 20 days instead of 120 days, causing hemolytic anemia. 7 THE HEMATOLOGIC SYSTEM 91 Copyright 2010 Cengage Learning. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. Due to electronic rights, some third party content may be suppressed from the eBook and/or eChapter(s). Editorial review has deemed that any suppressed content does not materially affect the overall learning experience. Cengage Learning reserves the right to remove additional content at any time if subsequent rights restrictions require it. RBC Normal Red Blood Cell 9. Splenectomy 10. Bone marrow transplant; not routinely performed because of difficulty finding suitable donor and high risk of complications CLOTTING DISORDERS Hemophilia Sickled RBC Figure 7–2 Pathophysiology of sickle cell anemia. Source: Delmar/Cengage Learning 4. Local hypoxia and continued sickling lead to blockage of blood vessels. 5. No symptoms before six to 12 months of age because of high fetal Hgb 6. Sickling is caused by decreased oxygen saturation, which is caused by high altitudes, dehydration, and acidosis. 7. Sickle cell crisis (Figure 7–3) a. Sickled cells clump together and obstruct blood vessels, causing increased blood viscosity and producing more sickling and hypoxia. b. Symptoms occur in areas where circulation is obstructed; may be renal, joint pain, pneumonias, leg ulcers, abdominal pain, stroke, etc. c. Enlarged liver and spleen from rapid RBC breakdown D. Assessment findings 1. Decreased Hgb 2. Sickle cell test and Sickledex: screening test results do not differentiate between trait and disease 3. Hgb electrophoresis—differentiates between trait and disease E. Management 1. Hydration (PO and IV) 2. Oxygenation 3. Correct acidosis 4. Analgesics for pain (no aspirin; may cause acidosis, which causes sickling) 5. Antibiotics for infections 6. Hydroxyurea (Droxia, Hydrea) for adults; daily use reduces painful crises 7. Exchange transfusions 8. Bed rest during crises 7 92 A. Inherited bleeding disorder caused by a deficit of one of the clotting factors B. Classic hemophilia (factor VIII deficiency) most common C. Transmission 1. Carried on the X chromosome 2. Manifested primarily in the male 3. European Caucasians primarily affected D. Pathophysiology of classic hemophilia: deficiency of factor VIII affects intrinsic clotting mechanism E. Assessment findings 1. Bleeding after minor injuries 2. Hemarthrosis (bleeding into joints such as knees, ankles, elbows, or wrists) F. Nursing diagnoses (Table 7–3) G. Management 1. Control acute bleeding a. Ice compresses to promote vasoconstriction b. Immobilization of bleeding area c. Fibrin foam d. Topical epinephrine e. Cryoprecipitate (frozen factor VIII) f. Desmopressin (DDAVP) IV or nasal spray 2. Prevent bleeding episodes a. No aspirin or ibuprofen or other anticoagulants b. Factor can be given two or three times a week to prevent bleeding episodes in clients with severe hemophilia. c. Avoid activities such as contact sports that are likely to cause bleeding. 3. Care for hemarthrosis a. Immobilize joint b. Bed cradle to keep bed clothes off joint c. Passive range of motion (ROM) 48 hours after bleeding is controlled; stop if there is pain Disseminated Intravascular Coagulation (DIC) A. Widespread formation of thromboses in the microcirculation, mainly within the capillaries, with subsequent depletion of clotting factors, resulting in hemorrhage from kidneys, brain, adrenals, heart, and other organs; clientss are usually critically ill with a surgical, hemolytic, obstetric, or neoplastic disease NCLEX-PN® Review Copyright 2010 Cengage Learning. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. Due to electronic rights, some third party content may be suppressed from the eBook and/or eChapter(s). Editorial review has deemed that any suppressed content does not materially affect the overall learning experience. Cengage Learning reserves the right to remove additional content at any time if subsequent rights restrictions require it. Effects of Sickle Cell Anemia on the Body Acidosis, Dehydration Oxygen Tension Hemolysis Slowed Circulation Sickled RBC Anemia Clumping & Thrombosis Ischemia Kidneys Extremities Brain Lung Eyes GI Figure 7–3 Effects of sickle cell anemia on the body. Source: Delmar/Cengage Learning Table 7–3 Nursing Diagnoses Related to Hemophilia • • • • Acute pain Impaired walking Impaired oral mucus membranes Ineffective health maintenance Source: Delmar/Cengage Learning B. Pathophysiology 1. Underlying disease causes release of thromboplastic substances into blood that promote fibrin deposits throughout the microcirculation. 2. Microthrombi form in many organs, causing microinfarcts and tissue necrosis. 3. RBCs are trapped in fibrin strands and hemolyzed. Platelets, prothrombin, and other clotting factors are destroyed, causing bleeding. 4. Excessive clotting activates the fibrinolytic inhibiting platelet function, causing further bleeding. C. Assessment findings 1. Petechiae and ecchymoses 2. Excessive bleeding from IVs, surgery, or childbirth 3. Oliguria and acute renal failure 4. Prothrombin time (PT) and partial thromboplastin time (PTT) prolonged 5. Decrease in clotting factors 7 THE HEMATOLOGIC SYSTEM 93 Copyright 2010 Cengage Learning. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. Due to electronic rights, some third party content may be suppressed from the eBook and/or eChapter(s). Editorial review has deemed that any suppressed content does not materially affect the overall learning experience. Cengage Learning reserves the right to remove additional content at any time if subsequent rights restrictions require it. D. Management 1. Control of underlying disease process 2. Transfusions of blood, platelets, and clotting factors 3. Heparin (stops clotting in microcirculation and frees clotting materials) 4. Prevent bleeding: a. No injections b. Handle gently c. Nontraumatic mouth care d. No aspirin WHITE CELL DISORDERS Infectious Mononucleosis (“Kissing Disease”) A. An acute infectious disease caused by the EpsteinBarr virus characterized by increased monocytes that affects primarily children and young adults B. Assessment findings 1. Lymphadenopathy 2. Headache, sore throat 3. Mental and physical fatigue 4. Spleen and liver enlargement 5. Heterophil antibody agglutination and Monospot tests positive 6. Incubation period of two to six weeks; spread by oral secretions C. Management 1. No specific treatment or immunization (rarely hospitalized) 2. Rest for several weeks to months 3. Treat secondary infections if they develop. Table 7–4 Nursing Diagnoses Related to Leukemia • • • • • Risk for infection Risk for injury Delayed growth and development Powerlessness Social isolation Source: Delmar/Cengage Learning 5. Enlarged liver and spleen 6. Abdominal pain, weight loss, and nausea 7. Bone pain due to expansion of marrow D. Nursing diagnoses (Table 7–4) E. Management 1. Chemotherapy: side effects include bone marrow depression, nausea, vomiting, alopecia, and/or stomatitis 2. Radiation therapy 3. Biological therapy such as monoclonal antibodies or interferon 4. Stem-cell transplantation a. Autologous: stem cells taken from client, treated to kill leukemia cells, and frozen to be given to client after chemotherapy and radiation have destroyed sick bone marrow b. Allogeneic (donor): stem cells (bone marrow) taken from compatible donor and administered to client after chemotherapy and radiation have destroyed sick bone marrow 5. Support child during painful procedures, such as bone marrow aspirations, lumbar punctures, and venipuncture. 6. Help client and family cope with a possible fatal illness. Leukemia A. A progressive, malignant disease of the bloodforming organs marked by distorted proliferation and development of leukocytes and their precursors in the blood and bone marrow; the most common form of childhood cancer; some forms occur in adults B. Pathophysiology 1. Uncontrolled proliferation of WBC precursors 2. Normal WBCs, RBCs, and platelets crowded out by leukemic cells 3. Type of leukemia is designated by the type of cell proliferating (myelocytic leukemia, acute lymphocytic leukemia). C. Assessment findings 1. Anemia, pallor, and dyspnea (due to decreased RBCs) 2. Ecchymoses and bleeding (due to decreased platelets) 3. Infections (due to decreased normal WBCs) 4. Lymphadenopathy 7 94 OTHER MALIGNANT DISORDERS Hodgkin’s Lymphoma A. A primary lymph node neoplastic disease characterized by painless progressive enlargement of the lymph nodes, spleen, and lymphoid tissues; often begins in a cervical node and spreads through the body; occurs primarily in adolescents and young adults B. Assessment findings 1. Lymphadenopathy usually starting with cervical nodes 2. Sweating, weakness, fever 3. Itching 4. Staging: a. Stage I—only one lymph node involved (good prognosis) b. Stage II—two or more nodes on same side of diaphragm (good prognosis) NCLEX-PN® Review Copyright 2010 Cengage Learning. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. Due to electronic rights, some third party content may be suppressed from the eBook and/or eChapter(s). Editorial review has deemed that any suppressed content does not materially affect the overall learning experience. Cengage Learning reserves the right to remove additional content at any time if subsequent rights restrictions require it. c. Stage III—nodes on both sides of diaphragm involved (poor prognosis) d. Stage IV—diffuse involvement with one or more extralymphatic organs involved (very poor prognosis) C. Management 1. Radiation used alone for localized disease 2. Chemotherapy a. Used in combination with radiation for advanced disease b. Usually, a combination of drugs is used. 3. Protect client from infections; remember that both the disease and the treatment reduce ability to fight infections. 4. Splenectomy in advanced disease Non-Hodgkin’s Lymphoma A. Tumor originating in the lymphoid tissue that is diffuse, disseminates easily, and is difficult to control B. Assessment findings: similar to Hodgkin’s lymphoma C. Management 1. Chemotherapy 2. Radiation 3. Surgery for diagnosis and staging 4. Nursing care similar to Hodgkin’s lymphoma Multiple Myeloma A. A malignant neoplasm in which the plasma cells proliferate and invade the bone marrow, causing destruction of the bone and resulting in pathologic fractures and bone pain; affects primarily men after the age of 40 B. Pathophysiology 1. Bone demineralization and destruction with osteoporosis and a negative calcium balance 2. Disruption of RBC, WBC, and thrombocyte production C. Assessment findings 1. Headache and bone pain 2. Pathological fractures and skeletal deformities of sternum and ribs 3. Osteoporosis and loss of height 4. Renal calculi 5. Anemia, infections, and bleeding tendencies 6. Hypercalcemia 7. Spinal cord compression and paraplegia 8. Urine positive for Bence-Jones protein D. Management 1. Drug therapy a. Analgesics for bone pain b. Cancer chemotherapy to reduce tumor mass c. Antibiotics to treat infections d. Gamma globulin to prevent infections e. Corticosteroids and mithramycin for severe hypercalcemia 2. 3. 4. 5. 6. 7. f. Medications such as etidronate (Didronel) or alendronate (Fosamax) to slow the loss of calcium from the bones Radiation therapy to reduce tumor mass Transfusions Comfort measures for bone pain Ambulation to slow demineralization Push fluids to prevent kidney stones from calcium overload Safety: clients prone to pathological fractures, bleeding, and infection Human Immunodeficiency Virus (HIV) and Acquired Immunodeficiency Syndrome (AIDS) A. HIV positive means that person has been exposed to HIV and has developed antibodies to try to fight the virus. HIV decreases human T-cell lymphocytes and suppresses the cellular immune response. B. AIDS occurs when the T-cell lymphocyte count is below 200 and the person develops opportunistic infections and unusual neoplasms. C. Risk factors 1. Sexually active homosexual and bisexual men 2. IV drug abusers 3. Hemophiliacs and recipients of blood transfusions 4. Children of persons with AIDS 5. Heterosexual partners of persons with AIDS 6. Tattoos and body piercings if unsterile equipment used D. Assessment findings 1. Nonspecific symptoms such as weight loss, fatigue, diarrhea, fever, and pallor 2. Dyspnea and hypoxemia due to pneumonia 3. Neurological dysfunction secondary to acute meningitis, dementia, and encephalopathy 4. Opportunistic infections a. Pneumocystis carinii pneumonia b. Herpes simplex virus, cytomegalovirus, and Epstein-Barr virus c. Fungal infections in brain, lungs, and esophagus d. Infections caused by mycobacterium avium complex (MAC), which causes fever and weight loss 5. Neoplasms a. Kaposi’s sarcoma b. CNS lymphoma c. Burkitt’s lymphoma d. Non-Hodgkin’s lymphoma 6. Leukopenia, anemia, and thrombocytopenia 7. Elevated transaminases and alkaline phosphatase 8. Low serum albumin 7 THE HEMATOLOGIC SYSTEM 95 Copyright 2010 Cengage Learning. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. Due to electronic rights, some third party content may be suppressed from the eBook and/or eChapter(s). Editorial review has deemed that any suppressed content does not materially affect the overall learning experience. Cengage Learning reserves the right to remove additional content at any time if subsequent rights restrictions require it.