POLYPHARMACY – PREVALENCE AND RISK FACTORS AMONG ELDERLY PATIENTS
IN GOVERNMENT MEDICAL COLLEGE, TANDA, DISTT KANGRA (HP)
Priya S1, Gupta NL2, Chauhan HS3
1
MPH Scholar, Center for Public Health & Healthcare Administration, Eternal
University, Baru Sahib, HP, India
2
Associate Professor& HoD, Psychology Department, Eternal University,
Baru Sahib, HP, India
3
Professor cum Head of Department, Center for Public Health & Healthcare
Administration, Eternal University, Baru Sahib, HP, India
ABSTRACT
The growing size of the elderly population in developing world including India is undoubtedly
posing mounting pressures on various socio-economic fronts including increased inter-personal
and health related problems, health care expenses etc. Moreover, this considerable population
faces multiple physiological, medical and psychological problems with aging that are different
than that of other stages; chronic diseases are common, the rate of drug related problems, drug
interactions and inappropriate medication use is much disturbing and at times severe. So, there
is an emerging need to pay greater attention to age-related issues. The aim of this study was to
assess the prevalence of polypharmacy and its risk factors among elderly OPD patients of
Government Medical College and Hospital, Tanda. A cross-sectional study was conducted on
371 elderly patients of ≥ 60 years old with concomitant use of 4 or more medications, defined as
Polypharmacy. The results found that the percent prevalence of polypharmacy among the study
population was 33.7%. The commonest disease affecting elderly was joint diseases, followed by
hypertension, diabetes mellitus, respiratory disorders and sleep disorders. The study found that
the use of polypharmacy was affected significantly by age (p= 0.01), place of residence (p = 0.05)
and source of income (p= 0.04). No statistically significant relationship between polypharmacy
and other factors (gender, educational status, family status, marital status) was found.
The generated data of this study can be used to implement various programmes on awareness
and prevention regarding Polypharmacy to reduce the adverse effects and misery to the elderly.
Further, this can be utilized by programmers, policymakers, researchers, academicians and
social workers who are working in the field of health of geriatrics. Keywords: Geriatrics, Elderly,
Aging, Polypharmacy, Concomitant
INTRODUCTION
The growing size of the elderly population in developing world including India is undoubtedly
posing mounting pressures on various socio economic fronts including increased interpersonal
and health problems, health care expenditures. Polypharmacy in a managed care setting
presents a unique set of challenges and opportunities [1] . Despite improved health care system
issues of elderly health are yet not well addressed. Polypharmacy, a preventable and significant
contributor to morbidity and mortality in the geriatric population [2]. Aging is associated with
multiple chronic diseases which are inter-related to the problems influenced by inappropriate
intake of medication which is a less explored aspect of geriatric health. Population ageing is a
result of high life expectancy and declining fertility. It is now a global phenomenon as in almost
every country older population is rapidly increasing. The aged population is being projected to
be around 1.5 billion in 2050, with 80% of them in the developing countries [3]. There are
numerous definitions used in the literature for polypharmacy such as two or more drugs for 240
days or more, concurrent use of two or more drugs, use of four or more medications, use of five
43
or more different prescription medications etc. WHO defined Polypharmacy as “Use of more
medications than clinically necessary” [4]
Therefore, there is a great challenge and an emerging need to pay attention to age-related
issues of this kind as the care of elderly is human right issue and is inbuilt in the value system of
Indian culture. It is our responsibility to provide elderly a safe supportive environment for their
well-being. Though, Government of India is fully committed and is playing a vital role in
formulating and implementing policies in order to create an enabling environment for the older
persons to lead an active and productive life, yet the efforts fall short of the need in this
context.
NEED FOR THE STUDY
The Census 2011 in India concludes that there are nearly 104 million elderly persons (aged 60
years or above); 53 million females and 51 million males which constitutes to 8.6% of the total
Indian population [7]. The Global Age Watch Index 2014, ranks India as 71 st out of 96 countries
on the basis of social and economic well-being of elderly (60 years plus) care. As per HelpAge
International after compiling data from various world international agencies. The age index
looked at four key domains – income security, health status, employment and education and
enabling environment. India scored poorly in all the four domains. With poor access to
healthcare facilities, India ranked 85th in health status. Though ranked among the lowest overall,
India fared a bit better than neighbouring countries. Afghanistan was ranked as the worst place
for older people, while Sweden was rated as the best country to grow old in. [8] The various
survey reports state that India’s strong economic performance and its already large and growing
population of older people has not yet resulted in widespread income security and access to
healthcare in older age. [9]
India considered as an ‘ageing population’ has the second highest population of elderly in the
world, projected to rise to 12% of the total population by 2020 with 80% of elderly living in rural
areas, 40% below the poverty line, over 73% illiterate, about 90% of them having no official
social security and 73% of deaths accounting to heart diseases, smoking and cancers. [9]
In the modern era, increasing use of inappropriate and multiple medication among elderly is
emerging as a major public health concern as it leads to many complexities during old age with
the detrimental effect (even death at times) on the health of elderly and the quality of life of the
elderly. There are few studies on the predictors of polypharmacy among elderly in India. Thus,
there is reasonable need to undertake this study.
With this study, we will be able to assess the level of polypharmacy that is prevalent among the
elderly population. The generated data of this study can then be utilised in various programmes
to take adequate measures to reduce its adverse effects and misery to the elderly. More
emphasis should be laid down for the proper use of medication and to improve the comfort
level among elderly patients and the health providers to talk and communicate freely about
their health issues. Findings of the study will be helpful for the policymakers, researchers,
academician and social workers who are working in the field of health.
OBJECTIVES
• To assess the prevalence of polypharmacy among the elderly patients in Government
Medical College, Tanda, Distt-Kangra (HP)
• To determine association between socio-demographic factors with polypharmacy.
METHODOLOGY
Study Design- A cross-sectional descriptive design was adopted to carry out the study.
44
Study population- The study population constituted of patients above 60 years of age in Dr
RPGMC, Tanda, District Kangra, HP.
Sample sizen
=
NZ2p (1-p)
d2 (N-1) + Z2p (1-p)
Since the population of the area was finite(less than 50,000)
n = Sample size
Z = Standards normal variable with 95% confidence interval i.e. 1.96
d= (allowable error) = 5% = .05
N= Total population from OPD of 8 departments (4258)
P= Estimated Prevalence 0.5
Putting the values in the formula;
n
=
4258(1.96)20.5(1-0.5)
(0.05)2 4257 + (1.96)2 0.5(1-0.5)
=
353 {Adding 5% Non- Response Rate}
=
371
Sampling technique- Proportionate sampling technique was used. Sampling was done based on
the records obtained from the record section of Dr RPGMC, Tanda.
Population of the study / sample- The study sample was chosen using proportionate sampling
from 8 departments of the hospital that concerned with treatment of geriatrics patient. These
departments were- General Medicine, Surgery, Orthopaedics & Physiotherapy, Dental,
Psychiatry, ENT, Ophthalmology, Gynaecology & Obstetrics.
Inclusion criteria
•
•
Elderly aged above 60 year who were willing to participate in the study.
Elderly present in the OPD at the time of study.
Exclusion criteria
•
•
•
Elderly suffering from cancers and other traumatic disorders.
IPD patients.
Mentally disturbed patients.
Data Collection Tool-Data was collected using structured survey questionnaire by the
researcher. Hospital visits were conducted to interview and fill the questionnaire from the
elderly who had come to the hospital to visit the doctor. For the elderly who could not
answer or were not in a good condition, then questions were asked from the relatives or
the care givers accompanying them. The questionnaire comprised of two parts. Part A
comprised of the demographic profile of the elderly patients, while part B comprised of
the health profile of the patients.
45
Validity and Reliability-Validation and reliability was done with the reference of research
papers. The questionnaire was prepared in an easy way for the better understanding of the
respondents. Expert opinion was taken whenever needed.
Study Period- The study period allotted for the completion of thesis was from January 2018 to
July 2018. The data collection particularly was done in January 2018-Fenruary 2018.
Data analysis software SPSS version 23 was used for data entry, processing and analysis.
Ethical consideration- The research was conducted after taking approval from the Institutional
Review Committee (IRC) of Eternal University. Verbal and written consent were taken from
participants. Privacy of the information was maintained and used for research objective only.
Following descriptive and inferential statistics were performed for data analyses• Frequencies and percentages of different variables to check the prevalence of
polypharmacy.
• Chi-square test to examine significant statistics of polypharmacy with socio-demographic
variables.
RESULTS
The table below describes the demographic characteristics of the study population i.e; Age,
gender, education status, marital status, family type and place of residence.
Table 1: Socio – demographic profile of the respondents
Demographic factors
Age
60-65
66-70
71-75
76-80
81 -85
86 and above
Gender
Male
Female
Qualifications
Illiterate
Literate
Primary
Secondary
Graduate & above
Marital status
Married
Unmarried
Widow/widower
Dietary pattern
Vegetarian
Non-vegetarian
Mixed diet
46
Frequency
Perce
nt%
111
86
71
56
19
28
29.9%
23.2%
19.1%
15.1%
5.1%
7.5%
188
183
50.7%
49.3%
79
67
99
80
46
21.3%
18.1%
26.7%
21.6%
12.4%
153
23
195
41.2%
6.2%
52.6%
209
25
137
56.3%
6.7%
36.9%
Family status
Nuclear
Joint
Extended
Place of residence
Rural
Urban
Old age homes
Others(labour huts, slums etc)
Source of income
Still working
Retired & pensioner
Retired but not pensioner
No source of income
Figure 1
Figure 2
Figure 3
47
165
133
73
44.5%
35.8%
19.7%
266
39
47
19
71.7%
10.5%
12.7%
5.1%
52
86
87
146
14.0%
23.2%
23.5%
39.4%
Table 2: Morbidity of the study population
Disease
Frequency
Hypertension & CVDs
Diabetes
Joint disorders
Respiratory diseases
Depression or sleep disorders
Perce
nt
73.0%
60.6%
82.2%
59.3%
30.2%
271
225
305
220
112
The above Table shows that the commonest disease affecting elderly were joint disorders
(82.2%), followed by hypertension (73.0%), diabetes mellitus (60.6%), respiratory disorders
(59.3%) and sleep disorders (30.2%).
Table 3: Prevalence of polypharmacy
Taking ≥4 medications
Frequency Percent
Yes
125
33.7
No
246
66.3
Total
371
100.0
Prevalence = Elderly population taking more than 4 medications
Study population or the sample of this study
Percent prevalence = 33.7% (0.33)
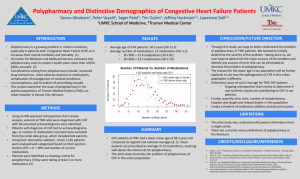
Table 4: Frequency of medicines taken by the respondents according to age group.
Age Interval
Number of drugs taken by the patients
0
1
2
3
4
5
Total
60-65
3
24
32
9
8
5
111
66-70
1
24
26
9
3
3
86
71-75
1
13
22
13
0
2
71
76-80
0
12
22
12
8
2
56
81 -85
0
1
6
3
8
1
19
86 and above
0
1
7
5
13
2
28
Total
5
75
115
51
110
15
371
Mean number of medications used per elderly patient was 2.62 (SD = 1.249).
Table 5: Frequency of current medication
Taking any medications at present
Frequency
Percentage
Yes
358
96.5
No
13
3.5
Classification of medicine use
Frequency
Percent
Minor Polypharmacy
246
66.3
48
Major Polypharmacy
125
33.7
Total
371
100.0
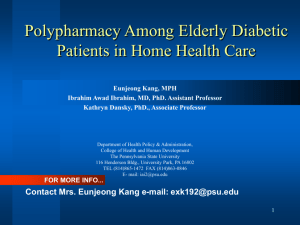
Table 6: Association between Polypharmacy and Socio-Demographic variables
Socio-Demographic variables Chi square
Degree
of p-value
freedom
Age
14.78
5
0.011*
Gender
3.61
1
0.062
Educational status
4.20
4
0.378
Marital status
2.96
2
0.227
Family status
0.62
2
0.732
Place of residence
7.63
3
0.054
Source of income
8.21
3
0.042*
*Statistically significant at p<0.05, ** Statistically highly significant at p<0.01
The Table above shows that use of polypharmacy is affected significantly by age (p= 0.01), and
source of income (p= 0.04), no statistically significant relationship between polypharmacy and
other factors (gender, educational status, family status, marital status and Place of residence)
was found.
DISCUSSION
Polypharmacy, a phenomenon less considered and an emerging public health concern in
elderly persons are becoming very common now a days. This study was conducted to find
out the prevalence of polypharmacy and its factors among 371 elderly OPD patients of
Government Medical College and Hospital, HP. For the purpose of this study,
Polypharmacy was considered as the use of 4 or more drugs by elderly visiting the OPD for
their morbid or comorbid conditions.The results obtained from the study have been
discussed herein.
Demographic profile
The study reveals that highest number of respondents were in the age group 60-65 years
(29.5%), and minimum, (7.5%) were aged above 86 years. Mean age of the respondents
was 71.14±8.196 which differed from the mean age of other studies, 80.24 years in the
prospective study conducted at the emergency department of General and Oncological
Hospital of Kifissia (Vrettos et al, 2017), 60.4±14.1 years in an observational,
cross-sectional, descriptive study of patients in internal medicine outpatient clinics at
Riyadh, Saudi Arabia (Salih et al, 2013). [5,6]
The current study showed that the majority group, (79%) of the respondents were literate
and (21%) were illiterate whereas most of the patients, (64.2%), were illiterate according
to an observational, cross-sectional, study of patients followed up in internal medicine
outpatient clinics. (Salih et al, 2013). [6] In the present study, males (50.7%) slightly
outnumbered females (49.3%) as well as widow/widower (52.6%) outnumbered married
(41.2%). It also shows that (44.5%) of the respondents were living in nuclear family,
(35.8%) in joint family and (10.7%) were living as extended family. Majority (71.7%) hailed
from rural area, (10.5%) from urban area, (12.7%) were inmates of old age homes and
(5.1%) from rural labour huts/ slums/ ashrams. It also shows that (39.4%) of the
respondents had no source of income, (23.5%) were retired but not pensioner, about
(23.2%) were retired and pensioner and (14.0%) were still working.
49
Prevalence of Polypharmacy and Health profile
The present study revealed that 4.0% of the participants were using 5 medicines, 29.7%
more than 4 drugs and 66.30 % were using 0- 3 medicines which on comparison with the
Data from third National Health and Nutrition Examination Survey (NHANES III) revealed
that 74% of elderly people used prescription medications. Persons aged 65-74 years, half
of them used 2 or more prescription drugs, 12% used 5 or more prescription drugs and
those aged 75 and above, 60% used at least two prescription drugs and 16% use at least
five. The study found 33.7% prevalence of polypharmacy among the study population
which showed considerable dissimilarity to the previous studies like a cross-sectional
study carried out in Mangaluru, showed 66.19% polypharmacy (Rakesh et al, 2017), global
longitudinal study carried out in Mumbai showed the prevalence as 4.2% (Dutta,IIPS &
Prashad, TISS, 2015), prospective multi-center cross-sectional study found prevalence was
41%. (Faten, 2008), in Nyeri PGH the prevalence of polypharmacy among patients of
above 65 years was found to be 5.15% (Mwaniki, 2014), a cross sectional study in old age
home in Hassan revealed 58.3% Polypharmacy (Geeta et al,2017), an observational,
cross-sectional, study at King Abdulaziz Medical City, Riyadh, Saudi Arabia revealed
prevalence was 89.1% (Salih et al,2013), In a descriptive analytic cross-sectional
study among residents of Tehranthe prevalence was found to be 52.3%(Hamid et al,2014)
[14,3,4,10,12,6,11]
The study indicated higher proportion of polypharmacy among males (57.6%) as
compared to females (42.4%) in rural area. This was although similar to the study carried out in
Mumbai with higher proportion of polypharmacy among males, but it was conducted in urban
area. The finding of the present study that maximum polypharmacy was found in (60-65) years age
group differed from the study that found more polypharmacy among (70-79) years old age groups.
(Dutta IIPS and Prashad TISS, 2015),while a Cross sectional study carried out old age home in
Hassan revealed highest polypharmacy in age group between 71-75 years (Geeta et al, 2017) [3,12]
Mean number of medications used by elderly patients was 2.62 ±1.25 in the current study,
which showed dissimilarity with other similar studies; in a Tertiary Care Hospital in
Puducherry the mean number of drugs were found as 5.48±2.46 (Kartik et al, 2016), the
prospective multi-center cross-sectional study on the population of the three districts
(Nablus, Tulkarm, and Jenin) showed mean number of medications used by each elder as
4.48±2.2(Faten, 2008), and in a study among residents of Tehranthe mean number of
medications used was 5.1±3.22(Hamid et al,2014).[13,4,11]
The current study suggested that prevalence of joint disorders was highest, followed by
hypertension, diabetes mellitus, respiratory diseases and sleep disorders which showed
some similarity to the prospective multi-centre cross-sectional study conducted among
the population of the three districts (Nablus, Tulkarm, and Jenin) revealing the
commonest disease affecting elderly was hypertension, followed by joint diseases,
diabetes mellitus, and cardiovascular disease (Faten, 2008).[4] The maximum number of
medications were taken for respiratory disorders (68.5%), followed by (60.4%) for
Hypertension & CVDs, (57.1%) for Diabetes Mellitus, (53.1%) for Joint Disorders and
(22.1%) for Depression & Sleep disorders. However, a cross sectional study carried out in
Hassan revealed that the most common medication was used for Gastro intestinal
disorders (78.3%) (Geeta et al, 2017)[4,12]
Relationship of Polypharmacy with demographic Variables
50
The study showed that polypharmacy was significantly associated with age (p= 0.01) and
source of income (p= 0.04). However, no statistically significant relationships between
polypharmacy and other factors (gender and educational, family and marital status and
place of residence) were found whereas the prospective multi-center cross-sectional study
conducted among the population of the three districts (Nablus, Tulkarm, and Jenin)
showed dissimilarity that polypharmacy is affected significantly by gender (p = 0.015), no
statistically significant relationship between polypharmacy and other factors (age, place of
residence, marital status, level of education, and income.(Faten, 2008) [4]
LIMITATIONS
1. This study only involved the OPD patients visiting the hospital and in-patients were not
included. Further, the community population was not involved.
3. The sample of the study was small viewing the large elderly suffering population, so, future
studies need to include a large sample size so that reliable inferences can be drawn and
generalized.
CONCLUSIONS & RECOMMENDATIONS
1. The prevalence of polypharmacy was found to be 33.7% among the elderly population. Joint
disorders were highest, followed by hypertension, diabetes mellitus, respiratory diseases and
sleep disorders. Males (57.6%) out-numbered females (42.4%) on polyphamacy. The present
study concluded that polypharmacy is an emerging public health concern among elderly in India.
Self-rated findings suggest joint disorders was highest, followed by hypertension, diabetes
mellitus, respiratory diseases and sleep disorders are the major risk factors of polypharmacy
among elderly in India.
2. Integrated educational and counselling programs focussed on the elderly age group should be
designed for the elderly so that they are able to understand the concerns and consequences of
excessive medication.
3. Since the only focus of the study was the use of polypharmacy & its associated factors, thus
more research needs to be done to have insight into the geriatric health and the consequences
of polypharmacy.
REFERENCES
1. Mohammed et al (2012) Indian Journal of Pharmacy Practice Volume 5 Issue 3 Jul - Sep,
2012
2. KA Wang1*, M Camargo2, RR Veluswamy3 (2013) Evidence-based strategies to reduce
polypharmacy: A review OA Elderly Medicine 2013 Nov 01;1(1):6. Evidence-based
strategies to reduce polypharmacy: A review
3. Mili Dutta (IIPS), Lokender Prashad (TISS) (2015)International Journal Of Public Mental
Health And Neurosciences ISSN: 2394-4668 (Published jointly by Azyme Biosciences (P)
Ltd., IJPMN, Volume 2, Issue 2, August -2015.
4. Faten Tahseen et al (2008) Prevalence and Risk Factors affecting polypharmacy among
elderly patients in the North of West
5. Ioannis
Vrettos,
Panagiota
Voukelatou, Apostolos
Katsoras, Despoina
Theotoka, and Andreas Kalliakmanis (2017) Diseases Linked to Polypharmacy in Elderly
Patientshttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC5757103/Curr
Gerontol
Geriatr Res
6. Salih Bin Salih, Muhammad Yousuf, Huda Durihim, Hind Almodaimegh1, Hani
Tamim2 (2013) Prevalence and associated factors of polypharmacy among adult
Saudi medical outpatients at a tertiary care center. Journal of Family and
51
CommunityMedicinehttp://www.jfcmonline.com/temp/JFamCommunityMed2031
62-4754289_131222.pdf
7. Ministry of Statistics and Programme Implementation Government of India
www.mospi.gov.
8. Global Age Watch Index 2014 http://www.dnaindia.com/india/report-90-of-india-selders-work-to-survive-1896924
9. Global Age Watch Index 2014, https://www.dnaindia.com/analysis/standpoint-elderlycare-why-india-is-one-of-the-worst-countries-to-grow-old-in-2138686
10. Annie Wamaitha Mwaniki (2014) Polypharmacy and quality prescribing in geriatric
patients: a case study of Nyeri Provincial general Hospital
11. Hamid Reza Yavari , Ahmad Ali Akbari Kamrani , Enayatollah Bakhshi , Malihe
Saboor , Robab Sahhaf (2014)Association Between Polypharmacy and SocioDemographic Factors Among Elderly Residents of Kahrizak Charity Foundation, Tehran
URL: http://salmandj.uswr.ac.ir/article-1-523-en.html
12. Geeta Rathod, Nalini G. K., Jayashree V. Nagaral, Sahana G. N., Deepak P., M. Prema,
Nuthan Kumar U. S., (2017) Factors associated with polypharmacy in geriatrics Indian
journal of basic &clinical pharmacology
13. Kartik Janardan Salwe, Dharani Kalyansundaram, and Yogesh Bahurupi(2016)A Study on
Polypharmacy and Potential Drug-Drug Interactions among Elderly Admitted in
Department of Medicine of a Tertiary Care Hospital in Puducherry. J Clin Diagn Res
14. KB Rakesh, Mukta N Chowta, Ashok K Shenoy, Rajeshwari Shastry, Sunil B Pai
(2017) Evaluation of polypharmacy and appropriateness of prescription in geriatric
patients: A cross-sectional study at a tertiary care hospital. Department of Pharmacology,
Kasturba Medical College, Manipal University, Mangaluru, Karnataka, India
52