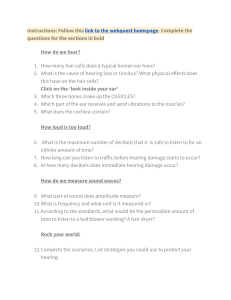
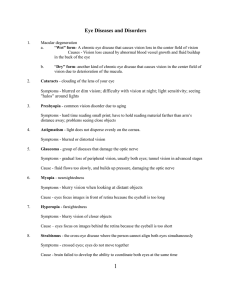
Nuts & Bolts Robert L. Martin Introducing “open-ear” couplers for testing open-fitted hearing aids By Robert L. Martin Sales of open-fitted hearing aids are exploding. Patients love how natural their amplified voices sound and the big improvement in word understanding that these instruments can provide. I believe open-fitted hearing aids will soon dominate the new user market, and the number of units sold will skyrocket as news of their success reaches consumers. When these hearing aids are fitted on appropriate candidates, the patient benefits are very great and the negatives are negligible. However, until now, there has been no simple way to conduct meaningful tests on these hearing aids without doing real-ear tests on the patient. This article introduces two new devices that can do this. The first is an ear simulator developed by Michael J. Rensink, MD, an otolaryngologist; you use your real-ear system to make measurements with this device. The second is a completely open coupler developed by Frye Electronics; measurements are done in the test box. As you know, conventional test couplers are closed, airtight cavities. It is possible to test an open-fitted hearing aid with a traditional closed coupler. However, the results become meaningless when the hearing aids are placed on the patient’s ears; the frequency response and feedback characteristics are entirely different in a closed cavity from how they are in the ear, where the open fitting allows almost all the low-frequency sound to escape. Our industry needs a reliable way to simulate open fittings without the patient’s being present. Clinicians need measurements that tell them how much amplification the patient will receive. The ear simulator and open coupler also give us a convenient way to study feedback without irritating or alarming the patient. THE RENSINK EAR SIMULATOR Dr. Rensink designed the ear simulator shown in Figures 1 to 3. It is a 3-cc syringe inserted Figure 1. into a rubber ear. Figure 1 shows the syringe with the needle removed and discarded. The rubber plunger on the injection shaft of the syringe has been removed and reinserted back into the syringe to the 2-cc line. The cavity (column of air) created in the open end of the syringe matches the diameter and length of the human ear canal. Figure 2 shows the syringe pushed into a rubber ear. The rubber ear adds “air” to Figure 2. 48 The Hearing Journal the simulator to match the external ear. This simple, inexpensive, easy-to-make device reacts to amplification just as the human ear does. Real-ear measurements from a human ear (mine) and the real-ear measurement from the open-ear simulator are nearly identical. Figure 3 shows the Rensink ear simulator with the real-ear measurement tube in the syringe and the reference microphone in place. Important note: When you make a real-ear measurement on an open fitting, you place the reference microphone on the ear (or beside the ear simulator) for sound field leveling, but turn it off when making an aided measurement. Sound from the openfitted hearing instrument will be “heard” by the reference microphone and affect the measurement. Here are some advantages of using the Rensink ear simulator: ❖ The total volume of air and the length of the air cavity in the coupler are about the same as in the human ear canal. Therefore, the acoustical response measured in this cavity matches that of the ear. ❖ The coupler is inexpensive and easy to make. ❖ The coupler enables clinicians to study open fittings when the patients are not present. Why use an ear simulator in the clinic? I have been conducting research on open-fitted hearing aids for the past 2 years. I’ve learned that these hearing aids can give patients with mild high-frequency hearing loss wonderful hearing and good word understanding in most listening conditions. Unfortunately, despite what you may have heard—even from supposed experts—there are many patients who will not benefit from open-fitted hearing aids. For example, open fittings are not suitable for patients Figure 3. who need significant gain in the lower frequencies or for people with severe-to-profound hearing loss in the higher frequencies. Real-ear tests tell us exactly how much amplification we are giving the patient with an open fitting. However, if we want to pre-fit the instruments or to study feedback when the patient is absent, the only choice has been to fit the hearing aids on our- Nuts & Bolts August 2006 • Vol. 59 • No. 8 Figure 4. Figure 5. selves or members of our staff. If you’ve run real-ear tests on yourself, you know it is difficult, and you end up with sore eardrums! Making an open-ear simulator It is easy to make an open-ear simulator like that invented by Michael Rensink. Here’s how. Obtain a 3-cc syringe and dispose of the needle properly. Pull the rubber end (the plunger) off the injection shaft. Carefully push the rubber plunger into the syringe to the “2-cc” line. Run a real-ear test (unaided) on your ear and save the curve. Run a real-ear test on the open end of the syringe. Move the rubber plunger in the syringe until the peaks of these two curves match. Push the syringe into a rubber ear. THE FRYE OPEN COUPLER Figure 4 is a photograph of a prototype of the new Frye open coupler, while Figure 5 shows a coupler and attached measurement microphone in the sound box. This coupler allows the clinician to do measurements in the sound box and August 2006 • Vol. 59 • No. 8 roughly approximate the amplification that will be delivered by an open-fitted instrument. The open-fitted instrument is inserted into the coupler and measurements are made. Neither the Rensink nor the Frye device in any way reduces our reliance on or need for real-ear tests. Real-ear studies always provide the most accurate measures of a hearing aid’s performance. However, using an ear simulator and/or an “open” coupler offers several advantages. ❖ It is much easier to place a hearing aid on a coupler than on a patient. ❖ You don’t need to worry about feedback bothering the patient. ❖ You can make all your pre-fit programming adjustments before the patient comes to the office. In short, these devices can make our jobs easier. IN CONCLUSION Our profession is going through a learning curve regarding the use of open-fitted instruments. Some practitioners want to fit them on people with substantial hearing loss, e.g., a flat 65-dB hearing loss. This is a mistake. Open fittings give you little or no amplification in the lower frequencies. You quickly learn the limits of open fittings when you adjust the programming and measure the result on an open coupler. The good news is that open-fitted hearing aids perform fantastically when fitted on appropriate patients (people with mild-to-moderate hearing loss in the higher frequencies). The potential market growth for these instruments is almost unlimited. You can easily make yourself a Rensink ear simulator using a common surgical syringe, or you can purchase a new “open coupler” from Frye. I suggest you spend some time measuring the amplification produced by open-fitted instruments so you learn their limitations. Without measurements you end up relying on marketing information and feedback from patients, which is not necessarily reliable. Measurements are part of the science of our profession. Robert L. Martin, PhD, has been a Dispensing Audiologist in private practice in the San Diego area for more than 30 years and has been writing Nuts & Bolts since 1989. Readers may contact Dr. Martin at 7750 University Avenue, La Mesa, CA 91941. Nuts & Bolts Circle 135 on Reader Service Card The Hearing Journal 51