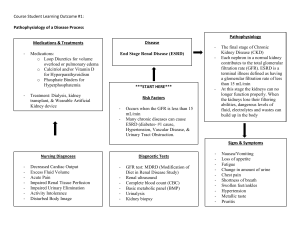
BIOCHEMICAL INVESTIGATION OF RENAL FUNCTIONS & DISORDERS/RENAL FUNCTION TEST PRESENTED BY: OLOYEDE OLUWADAMILOLA G. OUTLINE ● ● ● ● ● Introduction Functional Anatomy of the Kidney Functions of the Kidney Disorders of the Kidney Renal Function Tests INTRODUCTION ● ● ● ● The kidneys are a pair of bean-shaped or ovoid organs about the size of a clenched fist. They are lie retroperitoneally against the posterior abdominal wall on each side of the vertebral column at level T12-L3 vertebrae. During life, the kidneys are reddish brown and measure approximately 10 cm in length, 5cm in width and 5.5cm in thickness. Weight is 150g. Each kidney has a vertical cleft at the concave medial margin. This is the Renal hilum. The renal hilum is the entrance to a space within the kidney, the Renal Sinus. Structures that serve the kidneys (vessels, nerves, ureter) enter and exit the renal sinus via the renal hilum. INTRODUCTION ● ● ● ● ● Arterial supply: Renal arteries arising from the abdominal aorta Venous drainage: Renal veins The kidneys receive about 20% of the cardiac output under normal conditions. The kidneys have 2 regions: ○ Renal cortex ○ Renal medulla The renal medulla contains 8-10 renal pyramids FUNCTIONAL ANATOMY OF THE KIDNEYS NEPHRON ● ● ● ● The nephron is the functional unit of the kidney. Each kidney contains about 1 million nephrons. The kidneys cannot regenerate nephrons. Therefore, with renal injury, disease or normal aging, the number of nephrons gradually decreases. Types: a. Cortical nephrons b. Juxtamedullary nephrons NEPHRON ● Each nephron is made up of 5 main functional segments: a. Glomeruli b. Proximal Convoluted Tubules c. Loops of Henle d. Distal Convoluted Tubules e. Collecting Ducts GLOMERULI ● ● ● The glomeruli, located in the cortex of the kidney, are invaginated and surround a capillary network of blood vessels derived from the afferent arterioles, and draining into the efferent arterioles. The glomerular capillaries are covered by epithelial cells, and the total glomerulus is encased in the Bowman’s capsule. Small molecules and water are passively filtered during the passage of blood through these capillaries, the ultrafiltrate passing through the vessel walls and the glomerular membranes into the glomerular spaces (Bowman’s capsule). GLOMERULI ● ● The filtration barrier is has a structure to restrict the filtration of large proteins into the Bowman’s capsule. The filtration barrier consists of 3 parts: ○ The fenestrations of the capillary endothelium, which blocks blood cells and platelets ○ The thick, combined basal laminae, or Glomerular Basement Membrane, which restricts large proteins and some organic anions ○ The filtration slit diaphragms between pedicels, which restrict some small proteins and organic anions PROXIMAL CONVOLUTED TUBULE ● ● ● ● ● ● ● The proximal tubules are also located in the cortex and receive filtrate from the glomerular spaces. It is the most metabolically active part of the nephron. The cells of the PCT have abundant mitochondria and are specialized for both reabsorption and secretion. Extremely high permeability to water Na-K ATPase Pump on basolateral membrane Major function: Reabsorption of all organic nutrients (glucose, amino acids), all proteins, most water and electrolytes( Na, K, Cl, HCO-, H2O); secretion of organic anions and cations, H+, and NH4+ Convolution of the proximal tubules increases the tubular length and therefore contact between the luminal fluid and the proximal tubular cells. LOOPS OF HENLE ● ● ● ● ● The loop of Henle consists of 3 limbs: ○ Thin Descending, ○ Thin Ascending & ○ Thick Ascending Thin Descending Limb: Consists of thin epithelial cells with low metabolic activity. Highly permeable to water. Thick Ascending Limb: Consists of thick epithelial cells with high metabolic activity. Impermeable to water (important for urine concentration). Na-K ATPase Pump on basolateral membrane and Na-K-2Cl Co-transporter Pump on luminal membrane Reabsorbs Na, Cl, K, Ca, Mg, HCO3 DISTAL CONVOLUTED TUBULE ● ● ● ● Activity of Na-K ATPase is highest Na-Cl Co-transporter on luminal membrane Reabsorbs Na, Cl First portion forms the Macula Densa in the Juxtaglomerular Apparatus. It provides feedback control of GFR and RBF. JUXTAGLOMERULAR APPARATUS ● ● ● The juxtaglomerular apparatus consists of the juxtaglomerular cells of the afferent glomerular arteriole, the efferent glomerular arteriole, the extraglomerular mesangial cells, and that small portion of the distal tubule known as the macula densa that is located beside the renal glomerulus. This structure has specialized cell types: the macula densa of the distal tubule, the renincontaining cells of the afferent arteriole, and the interstitial lacis cells of the glomerular mesangium. The juxtaglomerular apparatus functions to maintain blood pressure and to act as a quality control mechanism to ensure proper glomerular flow rate and efficient sodium reabsorption. COLLECTING DUCTS ● ● ● Na-K ATPase Pump on basolateral membrane Principal Cells: Regulated reabsorption of water & electrolytes; regulated secretion of K+ Intercalated Cells: Reabsorption of K+ (low-K+ diet); help maintain acid-base balance RENAL INTERSTITIUM ● ● In all parenchymal organs, including the kidney, the interstitium is situated in the space between the basement membranes of the epithelial cells and of the nutritive capillaries. The renal interstitium is defined as the intertubular, extraglomerular, extravascular space of the kidney. It is bounded on all sides by tubular and vascular basement membranes and is filled with cells, extracellular matrix, and interstitial fluid. FUNCTIONS OF THE KIDNEY ● ● ● ● Endocrine Function Homeostatic Function Excretory Function Gluconeogenesis ENDOCRINE FUNCTION ● ● ● The kidneys produce hormone, Erythropoietin. The main function of this hormone is stimulate the production of red blood cells (erythrocytes)by the haematopoietic stem cells in the bone marrow. Stimulus: Hypoxia ENDOCRINE FUNCTION ● ● ● The kidneys also contribute to short-term arterial pressure by secreting hormones and vasoactive substances such as RENIN. The juxtaglomerular cells secrete renin in response to decreased renal blood flow. Renin then activates the Renin-Angiotensin Aldosterone System (RAAS) ENDOCRINE FUNCTION ● ● The kidneys produce the active form of Vitamin D, CALCITRIOL (1,25-dihydroxyvitamin D3). Calcitriol is essential for normal calcium deposition in the bone and calcium reabsorption by the GIT. EXCRETORY FUNCTION ● ● ● The kidneys are the primary means for eliminating waste products of metabolism. These products include: a. Urea b. Creatinine c. Uric acid d. End products of haemoglobin breakdown (e.g Bilirubin) e. Metabolites of various hormones The kidneys also eliminate most toxins and foreign substances that are either produced by the body or ingested, such as pesticides, drugs and food additives. HOMEOSTATIC FUNCTION ● ● ● Kidneys regulate water and electrolyte balance by matching fluid output with intake. The kidney helps maintain acid-base balance by eliminating excess acid in the form of hydrogen ions or producing bicarbonate to neutralize excess acid. Kidneys regulate blood pressure by excreting variable amounts of sodium and water, or by secreting precursors (Renin) of vasoactive substances (Angiotensin II). GLUCONEOGENESIS ● ● Kidneys synthesize glucose from amino acids, lactate and glycerol during prolonged fasting, a process referred to as Gluconeogenesis. The Kidney’s capacity to add glucose to the blood during prolonged periods of fasting rivals that of the liver. DISORDERS OF THE KIDNEY PATHOPHYSIOLOGY OF RENAL DISORDERS ● ● ● Renal dysfunction of any kind affects all parts of the nephron to some extent, although sometimes, either glomerular or tubular dysfunction is predominant. The net effect of renal disease on plasma and urine depends on the proportion of glomeruli to tubules affected and on the number of nephrons involved. To understand the consequences of renal disease it is good to compare what happens in the plasma and urine when there’s is low GFR and normal tubular function and vice versa. REDUCED GFR WITH NORMAL TUBULAR FUNCTION ● ● ● The total amounts of urea and creatinine excreted are affected by the GFR. If the filtration rate fails to balance that of production, plasma concentrations will rise. Plasma concentrations rise because less than normal is filtered. More of the reduced amount reaching the proximal tubule can be reabsorbed, and the capacity for secretion is impaired if the filtered volume is too low to accept the ions, further contributing to high plasma concentrations. REDUCED GFR WITH NORMAL TUBULAR FUNCTION PLASMA ● ● ● ● ● Uraemia & Creatininemia Low bicarbonate concentration, with low pH (acidosis) Hyperkalemia Hyperuricemia Hyperphosphatemia URINE ● ● ● Oliguria (reduced volume) Low (appropriate) sodium concentration - only if RBF is low, stimulating aldosterone secretion High (appropriate) urea concentration and therefore a high osmolality - only if ADH secretion is stimulated REDUCED TUBULAR FUNCTION WITH NORMAL GFR ● ● ● Damage to tubular cells impairs adjustment of the composition and volume of the urine. Impaired solute reabsorption from proximal tubules reduces isosmotic water reabsorption. Countercurrent multiplication may also be affected, therefore the ability of the collecting ducts to respond to ADH is reduced. A large volume of inappropriately urine is produced. REDUCED TUBULAR FUNCTION WITH NORMAL GFR PLASMA ● ● ● Normal urea and creatinine concentration (normal glomerular function) Due to proximal tubular failure ○ Hypophosphatemia, hypomagnesaemia, hypouricaemia Due to proximal or distal tubular failure ○ Low Bicarbonate concentration and low pH ○ Hypokalaemia REDUCED TUBULAR FUNCTION WITH NORMAL GFR URINE ● ● ● Due to proximal tubular failure ○ Glycosuria ○ Generalized amino aciduria ○ Phosphaturia ○ Possible tubular proteinuria Due to proximal and/or distal tubular failure ○ Increased volume ○ Inappropriately high pH Due to distal tubular failure ○ Inappropriately high Sodium concentration (even in RBF is low) ○ Inappropriately low Urea concentration and osmolality (even if ADH is stimulated) CLINICAL FEATURES OF RENAL DISORDERS UREA & CREATININE ● ● ● ● ● Plasma concentrations depend largely on glomerular function. Urinary concentrations depend largely on tubular function. Difference between plasma and urinary concentrations is due to tubular function. The more the tubular function is impaired, the nearer the plasma concentrations will be to the urinary concentration. Urinary concentration inappropriate to the state of hydration of the body suggest tubular damage, regardless of the degree of glomerular dysfunction. CLINICAL FEATURES OF RENAL DISORDERS SODIUM ● ● Plasma concentration is not primarily affected by renal diseases. The urinary volume depends on the difference between volume filtered in the glomerulus and volume reabsorbed by tubules. WATER ● ● As 99% of filtered water is normally reabsorbed, a small reabsorption impairment causes a large increase in urine volume. Polyuria results from predominant tubular dysfunction, even though glomerular filtration is reduced. CLINICAL FEATURES OF RENAL DISORDERS POTASSIUM, PHOSPHATE & URATE ● ● ● Degree of retention depends on balance between degree of glomerular retention and loss due to reduced absorptive capacity of the proximal tubules. Plasma concentration rises if little is filtered due to predominant glomerular dysfunction, even though there is failure of reabsorption. Plasma concentration is normal or even low, if tubular dysfunction predominates as the impaired reabsorption is balanced by the glomerular retention. RENAL FUNCTION TESTS RENAL FUNCTION TESTS ● ● Renal function tests are a group of laboratory tests useful in investigating and evaluating kidney function. They include: a. Glomerular Function Tests b. Renal Tubular Function Tests GLOMERULAR FUNCTION TESTS ● ● As glomerular function deteriorates, substances that are normally cleared by the kidneys, such as urea and creatinine, accumulate in the plasma. The glomerular function tests include: a. Measurement of Plasma Concentrations of Urea and Creatinine b. Plasma Clearance as an Assessment of GFR c. Cystatin C MEASUREMENT OF PLASMA CONCENTRATIONS OF UREA & CREATININE ● ● ● Normal range of Plasma Urea Concentration is 1.0 – 15mmol/L. Raised Plasma Urea Concentration is always accompanied with elevated Plasma Creatinine Concentration. The rate at which urea is reabsorbed from the collecting ducts is dependent on ○ The amount filtered by the glomerulus ○ Rate of luminal fluid flow MEASUREMENT OF PLASMA CONCENTRATIONS OF UREA & CREATININE Basis ● ● ● Plasma Urea Concentration greater than 15mmol/L indicates impaired glomerular function. Urea concentration rises when production exceeds clearance or when clearance is impaired. In renal dysfunction caused by reduced GFR, the plasma urea concentration rises faster than creatinine. Causes of Increase in Plasma Urea Concentration ● ● ● High protein diet. Absorption of amino acids and peptides from digested blood after haemorrhage into the gastrointestinal lumen (proctitis, cancers, tumors, haemorrhoids). Increased catabolism due to starvation, tissue damage, sepsis or steroid treatment. MEASUREMENT OF PLASMA CONCENTRATIONS OF UREA & CREATININE Basis ● ● Plasma Urea Concentration less than 1.o mmol/L could be due to increased GFR (most common) or decreased synthesis Urea concentration is lowered when clearance is increased or production is reduced Causes of less than 1.0mmol/L Plasma Urea Concentration (due to increased GFR) ● ● ● Pregnancy (commonest in young women) Over-enthusiastic intravenous infusion (commonest in hospital patients) Syndrome of inappropriate ADH Secretion MEASUREMENT OF PLASMA CONCENTRATIONS OF UREA & CREATININE Causes of less than 1.0mmol/L Plasma Urea Concentration (due to decreased synthesis) ● ● ● ● Low protein intake Very severe liver disease (low amino acid deamination) Use of amino acids for protein anabolism during growth, especially in children Inborn errors of the urea cycle (rare, and usually occur in infants) CLEARANCE AS AN ASSESSMENT OF GLOMERULAR FILTRATION ● ● ● ● ● ● ● Clearance is the volume of plasma that could theoretically be completely cleared of a substance in 1 minute. Only substances freely filtered by the glomeruli and not acted on by the tubules can be used to give true measurement of GFR. Exogenous substances that can be used for measuring clearance include: ○ Inulin ○ Radiochromium-labelled EDTA Endogenous substance commonly used is Creatinine The reciprocal of plasma creatinine concentration is called Renal Index Creatinine Clearance vs Inulin Clearance vs Urea Clearance Creatinine Clearance vs Plasma Creatinine Concentration CLEARANCE AS AN ASSESSMENT OF GLOMERULAR FILTRATION CYSTATIN C ● ● Plasma Cystatin C (Cys C) is an endogenous marker that may be used to replace Creatinine Unlike endogenous substances like Creatinine, it is neither secreted into the renal tubules nor reabsorbed back into the bloodstream. RENAL TUBULAR FUNCTION TEST ● ● ● Proximal Tubular Function Test Distal Tubular Function Test Water Deprivation Test REFERENCES ● ● ● Clinical Biochemistry and Metabolic Medicine by Martin A Crook Guyton and Hall Textbook of Medical Physiology by John E. Hall Clinically Oriented Anatomy by Keith L. Moore, Arthur F. Dalley, Anne M. R. Agur