Entrenamiento Control Motor Lumbopélvico: Evidencia Científica
advertisement

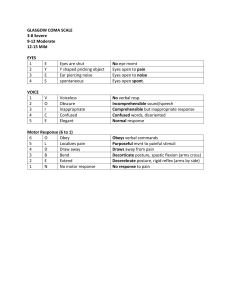
1 Máster Fisioterapia Manual Avanzada y Ejercicio Terapéutico Universidad Complutense de Madrid Entrenamiento del Control Motor Lumbopélvico Evidencia científica M Alicia Urraca Gesto Fisioterapeuta ¿QUÉ ES EL CONTROL MOTOR LUMBOPÉLVICO? Es el entrenamiento del control muscular necesario para hacer frente a las demandas funcionales de la columna. Entrenamos una faja muscular que da soporte a la columna y al tronco. Se define como restaurar o mejorar la capacidad del sistema neuromuscular de controlar y proteger la columna de la lesión o la recaída. fisioterapiamanual.es ¿QUÉ ES IMPORTANTE SOBRE EL CONTROL MOTOR LUMBOPÉLVICO? Objetivo: reentrenamiento de los músculos locales con un patrón respiratorio óptimo, en coordinación con la musculatura más superficial. Se basa en la evidencia experimental que muestra una alteración en la función de los músculos más profundos en los pacientes con dolor lumbar, frente a sujetos sanos. Se centra en: - entrenamiento de baja carga - posturas y movimientos cotidianos - dentro de las demandas funcionales y limitaciones específicas de cada paciente. fisioterapiamanual.es Entrenamiento del Control Motor Lumbopélvico - 18 de marzo de 2021 2 El entrenamiento del control motor mejora la habilidad del SNC para la eficacia del movimiento. FLUIDEZ vs RIGIDEZ fisioterapiamanual.es Restaurar control óptimo de columna y pelvis Optimizar la carga en columna y pelvis Demandas funcionales del paciente ENTRENAMIENTO DEL CONTROL MOTOR Coordinación de funciones (estabilidad, continencia, respiración) Patrones de activación muscular Postura Movimiento Función sensorial Factores psicosociales fisioterapiamanual.es ¿DOS TENDENCIAS? • Restaurar la coordinación y el control de los músculos del tronco para mejorar el control de la columna lumbar y la pelvis Ejercicios de control motor • Restaurar la capacidad, fuerza y resistencia, de los músculos del tronco para hacer frente a las demandas de control Ejercicios de McGill fisioterapiamanual.es Hodges PW Entrenamiento del Control Motor Lumbopélvico - 18 de marzo de 2021 3 SISTEMA LOCAL O PROFUNDO Músculos profundos que se insertan directamente en la columna Cruzan uno o pocos segmentos Poseen un brazo de momento limitado para mover la articulación. Proporcionan, por su anatomía, estabilidad segmentaria Multífidus profundos (MF) Transverso Abdominal (TrAb) Diafragma Suelo Pélvico Oblicuo Interno (OI): porción inferior? Psoas Mayor: porción profunda? Cuadrado Lumbar: porción medial? fisioterapiamanual.es Bergmark A 1989 SISTEMA GLOBAL O SUPERFICIAL Músculos con inserciones en tórax y pelvis Cruzan múltiples segmentos Gran capacidad para generar movimiento: control de la orientación de tórax y pelvis y equilibrar fuerzas externas Oblicuo externo Oblicuo interno Recto abdominal Erector espinal … fisioterapiamanual.es Bergmark A 1989 Musculatura local monoarticular: ayuda a la estabilidad antigravitatoria tónica tendencia a la debilidad Musculatura global poliarticular: producen movimiento tienden a la pérdida de extensibilidad, rigidez CONTROL SEGMENTARIO CONTROL POLISEGMENTARIO MUSCULATURA MUSCULATURA SEGMENTOS ¡¡¡DEBEN FUNCIONAR COORDINADOS!!! fisioterapiamanual.es Entrenamiento del Control Motor Lumbopélvico - 18 de marzo de 2021 4 TRANSVERSO DEL ABDOMEN FASC. SUP: estabilizan la caja torácica FASC. MEDIOS: se insertan en la fascia toracolumbar y contribuyen al control de la columna lumbar FASC. INF: nacen de la cresta iliaca, dan soporte al contenido abdominal y generan fuerzas de compresión de las ASI. Controla la presión intraabdominal Tensa la fascia toracolumbar fisioterapiamanual.es Urquhart 2005 HALLAZGOS CONTROLES La contracción del TrAb es anticipatoria al movimiento voluntario, independientemente de la dirección del movimiento. La activación del resto de los músculos abdominales sí depende de la dirección de movimiento. Esta “anticipación” se pierde o retrasa en el paciente con dolor lumbar. Se reduce su actividad tónica y disminuye su área de sección. fisioterapiamanual.es DOLOR LUMBAR CRÓNICO Hodges PW, Richardson CA1996 MULTIFIDUS Fibras superficiales: dependientes de la dirección del movimiento; ejercen control de la orientación espinal (lordosis). Fibras profundas: estabilizadoras, regulan la compresión vertebral. Independientes del movimiento, con activación anticipatoria al movimiento voluntario. fisioterapiamanual.es Moseley 2002 Entrenamiento del Control Motor Lumbopélvico - 18 de marzo de 2021 5 HALLAZGOS Desde las 3 primeras semanas de dolor hay cambios en las fibras tipo I del multífido. La atrofia del multífido es segmentaria, unilateral a la lesión. No tiene una recuperación espontánea, a pesar de la resolución de los síntomas. El multífido en el paciente con dolor lumbar crónico tiene menor área de sección y mayor infiltración grasa que en el paciente sano. Freeman 2010 Hides 2008 fisioterapiamanual.es MUSCULATURA SUPERFICIAL MUSCULATURA PROFUNDA Están activos en sujetos sanos Dependiendo de la dirección del movimiento, de forma específica Independientemente de la dirección del movimiento y de forma anticipatoria Evidencia en dolor lumbar Actividad aumentada al menos en uno de ellos Actividad dañada, disminuida, enlentecida fisioterapiamanual.es PRESIÓN INTRA-ABDOMINAL Controlada por el TrAb, (OBLICUO INTERNO, OBLICUO EXTERNO!!), DIAFRAGMA, SUELO PÉLVICO Respiración, tránsito intestinal, ESTABILIDAD: COORDINACIÓN DE FUNCIONES ESENCIALES fisioterapiamanual.es Hodges 2005 Smith 2014 Entrenamiento del Control Motor Lumbopélvico - 18 de marzo de 2021 6 PROGRESION EN EL ENTRENAMIENTO AISLAMIENTO - FASE COGNITIVA: CONTROL INTERVERTEBRAL CADENA CERRADA - FASE ASOCIATIVA: CONTROL DE LA ORIENTACIÓN LUMBOPÉLVICA, TORAX Y CABEZA CADENA ABIERTA - FASE AUTÓNOMA: CONTROL DEL EQUILIBRIO CORPORAL fisioterapiamanual.es Ejercicios de control motor FASE I ENTRENAMIENTO RESPIRATORIO CONTROL DEL MOVIMIENTO LUMBOPÉLVICO ENTRENAMIENTO AISLADO. Transverso del Abdomen ENTRENAMIENTO AISLADO. Multífido Lumbar CO-CONTRACCÓN. TrAb, Suelo Pélvico y MF lumbar IDEAS “Cambiar el modo en el que manejas tu cuerpo” “La práctica hace que se quede, no que sea perfecto” CALIDAD frente a CANTIDAD CONTROL MOTOR frente a FUERZA Alerta mente/cuerpo: el cerebro tiene que “ENCONTRAR” EL MÚSCULO El ejercicio aprendido con ATENCIÓN puede cambiar los patrones motores La forma de hacer que vuelva a ser automático es la práctica consciente repetida fisioterapiamanual.es Entrenamiento del Control Motor Lumbopélvico - 18 de marzo de 2021 CONTROL DEL MOVIMIENTO LUMBOPÉLVICO 7 Sentido de la posición y del movimiento lumbopélvico - Conciencia, precisión y control - Calidad frente a cantidad - Control independiente en cadera, pelvis y columna Flexión Neutro Extensión CONTROL DEL MOVIMIENTO LUMBOPÉLVICO CALIDAD DE LA MOVILIDAD PÉLVICA - Calidad del movimiento y Rango de movilidad - Activación de erectores espinales CONTROL DE LAS REGIONES ADYACENTES - Empuje de los MMII PREFERENCIA DIRECCIONAL - Movilidad de buena o mala calidad en uno o ambos movimientos RESPIRACIÓN - Capacidad de continuar con el patrón respiratorio durante el movimiento REPETICIÓN - Capacidad de realizar hasta 10 repeticiones con buena calidad fisioterapiamanual.es Elgueta-Cancino E et al. 2014 Ejercicios de control motor FASE I ENTRENAMIENTO AISLADO El cerebro tiene que “encontrar” el músculo - Conciencia, precisión y control - Calidad frente a cantidad - Control frente a fuerza - Feedback manual y verbal, ecografía (RUSI) Entrenamiento del Control Motor Lumbopélvico - 18 de marzo de 2021 8 CONTRACCIÓN DEL TrAb “Intenta juntar las dos EIAS” “Intenta llevar el ombligo hacia el pubis” “Piensa en contraer el suelo pélvico” “Aleja la tripa de mi mano” fisioterapiamanual.es POSICIÓN NEUTRA EN DECÚBITO LATERAL fisioterapiamanual.es CUADRUPEDIA fisioterapiamanual.es Entrenamiento del Control Motor Lumbopélvico - 18 de marzo de 2021 9 RESPUESTAS INCORRECTAS ACTIVACIÓN DEL OBLICUO EXTERNO: disminución del ángulo infraesternal, bloqueo costal lateral, pliegue supraumbilical, báscula posterior ACTIVACIÓN DEL OBLICUO INTERNO: aumento del ángulo infraesternal, expansión torácica lateral, protusión abdominal VALSALVA: aumento de PIA BLOQUEO ABDOMINAL fisioterapiamanual.es PUNTOS DE CONTROL DE RIGIDEZ GLOBAL BALANCEO TORÁCICO: empujes manuales oscilatorios: desde la parte lateral del tórax. Debe haber movimiento y ser simétrico PATRÓN RESPIRATORIO: debe haber expansión costal (lateral++) ROTACIÓN INTERNA Y EXTERNA DE LA CADERA: intento de mover el MI desde la rodilla MOVIMIENTO DE LOS DEDOS DE LOS PIES: en el paso a bipedestación fisioterapiamanual.es TÉCNICAS DE CORRECCIÓN Reduce la velocidad 50% Reduce el esfuerzo 50% (piensa más que contrae) Cambia la posición Asegura la columna neutra (OE++) Aleja la atención del abdomen con el suelo pélvico, la parte interna de los muslos o los multífidos ¡¡¡FEEDBACK PALPATORIO!!! fisioterapiamanual.es Entrenamiento del Control Motor Lumbopélvico - 18 de marzo de 2021 10 ¿CÓMO SE PROGRESA? Conseguir la contracción de los músculos profundos: - Independiente - Cognitiva - Con feedback mínimo - Con esfuerzo mínimo - Mantenimiento de 10” - Con un patrón óptimo relajado Co-activación de los músculos profundos Corrección de postura y patrón de movimiento Costa 2009 fisioterapiamanual.es Lumbar Multifidus CONTRACCIÓN DEL MULTÍFIDO “Intenta unir las dos EIPS” “Intenta crecer” “Piensa en arquear la espalda sin moverte” - “Imagina que unes las dos EIPS” o “intenta aproximar mis dedos” - “Piensa en arquear la espalda sin moverte” - “Imagina que acercas la columna lumbar a la cadera desde ambos lados, con la misma tensión” - “Intenta crecer o alargarte” - “Imagina una tensión que va desde la parte posterior del pubis hasta la zona del MF que estamos palpando” fisioterapiamanual.es Ejercicios de control motor FASE II ENTRENAMIENTO EN SEDESTACIÓN ENTRENAMIENTO EN BIPEDESTACIÓN TRANSICIÓN SEDESTACIÓN A BIPEDESTACIÓN ENTRENAMIENTO EN FLEXIÓN Y EXTENSIÓN Posturas Movimientos Actividades Entrenamiento del Control Motor Lumbopélvico - 18 de marzo de 2021 11 SENTARSE EN LOS TALONES fisioterapiamanual.es POSICIÓN NEUTRA EN SEDESTACION fisioterapiamanual.es fisioterapiamanual.es Elgueta-Cancino E et al. 2014 Entrenamiento del Control Motor Lumbopélvico - 18 de marzo de 2021 POSICIÓN NEUTRA EN BIPEDESTACIÓN 12 fisioterapiamanual.es INCLINACIÓN ANTERIOR DEL TRONCO fisioterapiamanual.es INCLINACIÓN ANTERIOR EN BIPEDESTACIÓN fisioterapiamanual.es Entrenamiento del Control Motor Lumbopélvico - 18 de marzo de 2021 13 SENTADILLAS fisioterapiamanual.es FASE III: ESTABILIZACIÓN FORTALECIMIENTO fisioterapiamanual.es FASE III: ESTABILIZACIÓN-FORTALECIMIENTO Implica el movimiento de los segmentos espinales: salir de la columna neutra Integración de los sistemas local y global Debe lograr: función y movimiento normales Capacidad de controlar el movimiento toraco-pélvico: mover el tórax sobre la pelvis, y viceversa fisioterapiamanual.es Entrenamiento del Control Motor Lumbopélvico - 18 de marzo de 2021 14 ¿CÓMO SE PROGRESA? Conseguir la contracción de los músculos profundos: - Independiente - Cognitiva - Con feedback mínimo - Con esfuerzo mínimo - Mantenimiento de 10” - Con un patrón óptimo relajado Co-activación de los músculos profundos Corrección de postura y patrón de movimiento Costa 2009 fisioterapiamanual.es ¿CÓMO SE PROGRESA? - Coordinación apropiada de los músculos superficiales con los profundos - Control de la posición lumbar neutra durante el movimiento de las extremidades - Control adecuado durante tareas funcionales específicas: necesidades y demandas del paciente - Para facilitar el entrenamiento al paciente descompondremos las tareas o reduciremos la carga. Costa 2009 fisioterapiamanual.es ¿CÓMO DISEÑO EL PROGRAMA DEL PACIENTE? ¿Con qué estrategia consigue el paciente la activación profunda sin sobreactivación superficial? ¿Qué posturas o movimientos necesitan ser controlados? ¿Qué estrategias de feedback necesita para practicar en casa de forma apropiada? ¿Cuál es la dosificación del trabajo domiciliario? fisioterapiamanual.es Entrenamiento del Control Motor Lumbopélvico - 18 de marzo de 2021 Low-Back Pain Patients Learn to Adapt Motor Behavior WithWith Adverse Secondary Consequences Behavior Adverse Secondary Consequences 2 Jaap H. van Dieën,1 Herta Flor, and Paul W. Hodges3 1 2 Jaap H. van Dieën, Herta Flor, and Paul W. Hodges3 1 Department 1 of Human Movement Science, MOVE Research Institute Amsterdam, Vrije Universiteit Amsterdam, Department of Human Movement Science, MOVE Research Institute Amsterdam, Vrije Universiteit Amsterdam, Amsterdam, the Netherlands, 2Department of Cognitive and Clinical Neuroscience, Central Institute of Mental Amsterdam, the Netherlands, 2Department of Cognitive and Clinical Neuroscience, Central Institute of Mental Health, Medical Faculty Mannheim, Heidelberg University and Department of Psychology, School of Social Sciences, Health, Medical Faculty Mannheim, Heidelberg University and Department of Psychology, School of Social Sciences, 3 3 University of Mannheim, Germany; and The University of Queensland, Centre for Clinical Research Excellence in in University of Mannheim, Germany; and The University of Queensland, Centre for Clinical Research Excellence Spinal Pain,Spinal InjuryPain, andInjury Health, Health Rehabilitation Sciences, Brisbane Queensland, Australia andSchool Health,ofSchool ofand Health and Rehabilitation Sciences, Brisbane Queensland, Australia Ejercicios de control motor 15 ARTICLE VAN DIEËN, J.H.,DIEËN, H. FLOR, P.W. HODGES. Low-Back pain patients learn tolearn adapt behavior withwith adverse secondary VAN J.H., and H. FLOR, and P.W. HODGES. Low-Back pain patients to motor adapt motor behavior adverse secondary consequences. Exerc. SportExerc. Sci. Rev., 45, No. pp.No. 223–229, 2017. We hypothesize that changes in motor behavior in individuals consequences. Sport Vol. Sci. Rev., Vol.4,45, 4, pp. 223–229, 2017. We hypothesize that changes in motor behavior in individuals pain are adaptations aimed at minimizing real or perceived risk of further pain. Through reinforcement learning, with low-backwith painlow-back are adaptations aimed at minimizing the real ortheperceived risk of further pain. Through reinforcement learning, painpain andand subsequent adaptations in lessmotor dynamic motor behavior, to increased and impoverished sensory feedback, which Low-Back Pain result Patients Learn tobehavior, Adapt Motor subsequent adaptations in lessresult dynamic leading toleading increased loading loading and impoverished sensory feedback, which contribute toAdverse cortical reorganization and proprioceptive impairments thatthe reduce to control movement in a robust manner. contribute to cortical reorganization and Secondary proprioceptive impairments that reduce abilitythetoability control lumbarlumbar movement in a robust manner. Behavior With Consequences Key Words: reinforcement learning, nociception, postural control, motorsensory control,feedback, sensory feedback, perceived Key Words: reinforcement learning, nociception, postural control, motor control, perceived risk of risk painof pain Jaap H. van Dieën,1 Herta Flor,2 and Paul W. Hodges3 1 Department of Human Movement Science, MOVE Research Institute Amsterdam, Vrije Universiteit Amsterdam, Amsterdam, the Netherlands, 2Department of Cognitive and Clinical Neuroscience, Central Institute of Mental Health, Medical Faculty Mannheim, Heidelberg University and Department of Psychology, School of Social Sciences, University of Mannheim, Germany; and 3The University of Queensland, Centre for Clinical Research Excellence inbehind motor control changes in LBP should lead to more effecbehind motor control changes in LBP should lead to more effecSpinal Pain, Injury and Health, of Health and Rehabilitation Sciences, Brisbane Queensland, Australia tive treatments. Key School Points Los cambios en el Keycomportamiento motor son tive el treatments. resultado de un Points Motor control in LBP is changed at many levels of the ner• Low-back pain tends to change motor behavior toward Motor control inStudies LBP isofchanged at many levels of the nervous system. individuals with and without LBP have • Low-back pain tends to change motor behavior toward increased coactivation, reduced deep muscle activity, and vous system. Studies of individuals withtrunk and muscle without LBP have proceso de aprendizaje por refuerzo para minimizar la pérdida reported differences in voluntary activation (45), increased coactivation, reduced deep muscle activity, and less within-subject variance. differences voluntary muscle activation • Minimizing a weighted sum of costs, including the risk reportedtrunk less within-subject variance. muscle in reflexes (32), trunk and trunk kinematics (20)(45), and in nociceptive input, predicts • Minimizing aofweighted sum and of costs, including they riskla these trunk muscle (32), and trunk (20) andoutputs in corticalreflexes mapping of sensory inputs kinematics from (5), and motor de control sobre la postura ylosing elcontrol movimiento provocación del dolor. pain-related changes. input, predicts these of losing control and nociceptive (36), theoftrunk. However, literature is far fromoutputs consistent corticalto mapping sensory inputs the from (5), and motor VAN DIEËN, J.H., H. FLOR, and P.W. HODGES. Low-Back pain patients learn to adapt motor behavior with adverse secondary consequences. Exerc. Sport Sci. Rev., Vol. 45, No. 4, pp. 223–229, 2017. We hypothesize that changes in motor behavior in individuals with low-back pain are adaptations aimed at minimizing the real or perceived risk of further pain. Through reinforcement learning, pain and subsequent adaptations result in less dynamic motor behavior, leading to increased loading and impoverished sensory feedback, which contribute to cortical reorganization and proprioceptive impairments that reduce the ability to control lumbar movement in a robust manner. Key Words: reinforcement learning, nociception, postural control, motor control, sensory feedback, perceived risk of pain • In addition to actual benefits with respect to risk and pain-related changes. regarding the nature of these differences. For example, accord(36), behindbe motor controlby changes in LBP should leadto to more effec-the trunk. However, the literature is far from consistent nociception, changes may driven maximization • In addition to actual benefits with respect to risk and tive treatments. ingthe to anature systematic review, there is support of both an increase regarding of these differences. accordofchanges perceived benefits. may be driven by maximizationy más actividad Este proceso predice nociception, mayor coactivación de laForof example, a decrease of trunk muscle activation in individuals with • Originally adaptive changes have negative consequences ing to aand systematic review, there is support both an increase of perceivedthat benefits. LBP (45).of trunk muscle activation in individuals with may outweigh benefits in the long term. and a decrease • Originally adaptive changes have negative consequences musculatura superficial. LBP (45).Here, we propose a hypothesis on how LBP affects motor that may outweigh benefits in the long term. control, which may account for these inconsistencies. In reinKey Points Motor control in LBP is changed at many levels of the nervous system. Studies of individuals with and without LBP have reported differences in voluntary trunk muscle activation (45), trunk muscle reflexes (32), and trunk kinematics (20) and in cortical mapping of sensory inputs from (5), and motor outputs to (36), the trunk. However, the literature is far from consistent INTRODUCTION regarding the nature of these differences. For example, accordforcement learning, a reward (positive reinforcement) or the ing to prevalent a systematic review, is support is of the both an increase Low-back pain (LBP) is widely and,there globally, and a decrease of trunk muscle activation in individuals with absence or reduction of a cost (negative reinforcement) increases leading cause of years lived with due to the functional LBPdisability (45). the likelihood that a performed behavior will be repeated and Here, we propose and a hypothesis on howrecurLBP affects motor limitations, limited benefits of treatment, frequent control, which may account for these inconsistencies. In reinthus learned. In this context, movement-related pain may funcINTRODUCTION rence (15). Motor control exercise is alearning, commonly treatment forcement a rewardused (positive reinforcement) or the Low-back pain (LBP) is widely prevalent and, globally, is the tion as a negative reinforcement and the sense of being able to absence or reduction of a cost (negative reinforcement) increases leading cause of years lived disability due to the functional forwith LBP. Although systematicthe reviews support its effectiveness, likelihood that a performed behavior will be repeated and prevent pain provocation as a positive reinforcement. Motor limitations, limited benefits of treatment, and frequent recurlearned. In thissize context, movement-related pain may funclike other treatments for LBP,thusthe effect is not large (33). rence (15). Motor control exercise is a commonly used treatment can be considered as the outcome of a learning process as a negative reinforcement and the sense of being able control to for LBP. Although systematic reviews understanding support its effectiveness, A better of thetion nature of and the mechanisms prevent pain provocation as a positive reinforcement. Motor aimed at optimizing a combination of costs and rewards. For like other treatments for LBP, the effect size is not large (33). control can be considered as the outcome of a learning process A better understanding of the nature of and the mechanisms clarity, either costs or rewards usually are inverted, such that a aimed at optimizing a combination of costs and rewards. For clarity, either costs or rewards usually are inverted, such that a sum of weighted costs can be minimized or a sum of weighted Address for correspondence: Jaap H. van Dieën, Department of Human Movement sum of weighted costs can be minimized or a sum of weighted Address for correspondence: Jaap H. van Dieën, Department of Human Movement Science, Research Institute Science, MOVE Research Institute Amsterdam,MOVE Vrije Universiteit Amsterdam, Van der Amsterdam, rewards Vrije can beUniversiteit maximized. Amsterdam, Van der rewards can be maximized. Boechorststraat 9, NL-1081 BT Amsterdam, the Netherlands (E-mail: j.van.dieen@vu.nl). conditions, costs associated with control efforts Boechorststraat 9, NL-1081 BT Amsterdam, In thepain-free Netherlands (E-mail: j.van.dieen@vu.nl). Accepted for publication: February 7, 2017. or muscle activation are considered most important. We assume In pain-free conditions, costs associated with control efforts Editor:Address Roger M. Enoka, Accepted forJaap publication: 2017. for Ph.D. correspondence: H. vanFebruary Dieën,7,Department of Human Movement that with LBP, weighting of costs associated with potential loss or muscle activation are considered most important. We assume Editor:Institute Roger M.Amsterdam, Enoka, Ph.D.Vrije Universiteit Amsterdam, Van der Science, MOVE Research 0091-6331/4504/223–229 of control over posture and movement and costs associated with Exercise and Sport Sciences Reviews that with LBP, weighting of costs associated with potential loss potential pain provocation increase, and one learns to minimize Boechorststraat 9, NL-1081 BT Amsterdam, the Netherlands (E-mail: j.van.dieen@vu.nl). DOI: 10.1249/JES.0000000000000121 0091-6331/4504/223–229 this new weighted sum of costs. Although the resulting muscle Copyright © 2017 by the American College of Sports Medicine of control over posture and movement and costs associated with Accepted for publication: February 7, 2017. • Low-back pain tends to change motor behavior toward increased coactivation, reduced deep muscle activity, and less within-subject variance. • Minimizing a weighted sum of costs, including the risk of losing control and nociceptive input, predicts these pain-related changes. • In addition to actual benefits with respect to risk and nociception, changes may be driven by maximization of perceived benefits. • Originally adaptive changes have negative consequences that may outweigh benefits in the long term. Here, we propose a hypothesis on how LBP affects motor control, which may account for these inconsistencies. In reinforcement learning, a reward (positive reinforcement) or the absence or reduction of a cost (negative reinforcement) increases the likelihood that a performed behavior will be repeated and thus learned. In this context, movement-related pain may function as a negative reinforcement and the sense of being able to prevent pain provocation as a positive reinforcement. Motor control can be considered as the outcome of a learning process aimed at optimizing a combination of costs and rewards. For clarity, either costs or rewards usually are inverted, such that a sum of weighted costs can be minimized or a sum of weighted rewards can be maximized. In pain-free conditions, costs associated with control efforts Exercise and Sport Sciences Reviews or muscle activation considered most important. Wetoassume Editor: Roger M. Enoka, Ph.D. potential painare provocation increase, and one learns minimize DOI: 10.1249/JES.0000000000000121223 that with of costs associated with thisLBP, newweighting weighted sum of costs. Although thepotential resulting loss muscle Copyright © 2017 by the American College of Sports Medicine 0091-6331/4504/223–229 of control over posture and movement and costs associated with Copyright © 2017 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited. Exercise and Sport Sciences Reviews potential pain provocation increase, and one learns to minimize 223 DOI: 10.1249/JES.0000000000000121 this new weighted sum of costs. Although the resulting muscle Copyright © 2017 by the American College of Sports Medicine INTRODUCTION Low-back pain (LBP) is widely prevalent and, globally, is the leading cause of years lived with disability due to the functional limitations, limited benefits of treatment, and frequent recurrence (15). Motor control exercise is a commonly used treatment for LBP. Although systematic reviews support its effectiveness, like other treatments for LBP, the effect size is not large (33). A better understanding of the nature of and the mechanisms ARTICLE ARTICLE 223 Low-Back Pain Patients Learn to Adapt Motor Low-Back Pain Patients Learn to Adapt Motor Behavior With Adverse Secondary Consequences Behavior With Adverse Secondary Consequences Copyright © 2017 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited. Copyright © 2017 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited. 2 Jaap H. van Dieën,1 Herta Flor, and Paul W. Hodges3 1 2 Jaap H. van Dieën, Herta Flor, and Paul W. Hodges3 1 Department 1 of Human Movement Science, MOVE Research Institute Amsterdam, Vrije Universiteit Amsterdam, Department of Human Movement Science, MOVE Research Institute Amsterdam, Vrije Universiteit Amsterdam, Amsterdam, the Netherlands, 2Department of Cognitive and Clinical Neuroscience, Central Institute of Mental Amsterdam, the Netherlands, 2Department of Cognitive and Clinical Neuroscience, Central Institute of Mental Health, Medical Faculty Mannheim, Heidelberg University and Department of Psychology, School of Social Sciences, Health, Medical Faculty Mannheim, Heidelberg University and Department of Psychology, School of Social Sciences, 3 University of Mannheim, Germany;Germany; and 3Theand University of Queensland, Centre for Clinical Research Excellence in in University of Mannheim, The University of Queensland, Centre for Clinical Research Excellence Spinal Pain,Spinal InjuryPain, andInjury Health, Health Rehabilitation Sciences, Brisbane Queensland, Australia andSchool Health,ofSchool ofand Health and Rehabilitation Sciences, Brisbane Queensland, Australia Ejercicios de control motor ARTICLE VAN DIEËN, J.H.,DIEËN, H. FLOR, P.W. HODGES. Low-Back pain patients learn tolearn adapt behavior withwith adverse secondary VAN J.H., and H. FLOR, and P.W. HODGES. Low-Back pain patients to motor adapt motor behavior adverse secondary consequences. Exerc. SportExerc. Sci. Rev., 45, No. pp.No. 223–229, 2017. We hypothesize that changes in motor behavior in individuals consequences. Sport Vol. Sci. Rev., Vol.4,45, 4, pp. 223–229, 2017. We hypothesize that changes in motor behavior in individuals pain are adaptations aimed at minimizing real or perceived risk of further pain. Through reinforcement learning, with low-backwith painlow-back are adaptations aimed at minimizing the real ortheperceived risk of further pain. Through reinforcement learning, painpain andand subsequent adaptations in lessmotor dynamic motor behavior, to increased and impoverished sensory feedback, which Low-Back Pain result Patients Learn tobehavior, Adapt Motor subsequent adaptations in lessresult dynamic leading toleading increased loading loading and impoverished sensory feedback, which contribute toAdverse cortical reorganization and proprioceptive impairments thatthe reduce to control movement in a robust manner. contribute to cortical reorganization and Secondary proprioceptive impairments that reduce abilitythetoability control lumbarlumbar movement in a robust manner. Behavior With Consequences Key Words: reinforcement learning, nociception, postural control, motorsensory control,feedback, sensory feedback, perceived Key Words: reinforcement learning, nociception, postural control, motor control, perceived risk of risk painof pain Jaap H. van Dieën,1 Herta Flor,2 and Paul W. Hodges3 1 Department of Human Movement Science, MOVE Research Institute Amsterdam, Vrije Universiteit Amsterdam, Amsterdam, the Netherlands, 2Department of Cognitive and Clinical Neuroscience, Central Institute of Mental Health, Medical Faculty Mannheim, Heidelberg University and Department of Psychology, School of Social Sciences, University of Mannheim, Germany; and 3The University of Queensland, Centre for Clinical Research Excellence inbehind motor control changes in LBP should lead to more effecbehind motor control changes in LBP should lead to more effecSpinal Pain, Injury and Health, of Health and Rehabilitation Sciences, Brisbane Queensland, Australia tive treatments. Key School Points tive treatments. Points Motor control in LBP is changed at many levels of the ner• Low-back pain tends to change motor behavior toward La reeducación delKey control motor debería dirigirse acontrol la activación Motor inStudies LBP isofchanged at many levels of the nervous system. individuals with and without LBP have • Low-back pain tends to change motor behavior toward increased coactivation, reduced deep muscle activity, and vous system. Studies of individuals withtrunk and muscle without LBP have reported differences in voluntary activation (45), increased coactivation, reducedvariance. deep muscle activity, and less within-subject reported differences voluntary muscle activation • Minimizing a weighted sum of costs, including the risk less within-subject variance. de la musculatura profunda, a la inhibición de la superficial, al trunk muscle in reflexes (32), trunk and trunk kinematics (20)(45), and in losing control nociceptive input, • Minimizing aofweighted sum and of costs, including thepredicts risk these trunk muscle and trunk (20) andoutputs in corticalreflexes mapping(32), of sensory inputs kinematics from (5), and motor pain-related changes. input, predicts these of losing control and nociceptive to (36), theoftrunk. However, the literature is far fromoutputs consistent cortical mapping sensory inputs from motor entrenamiento de propiocepción y with a respect inculcar confianza en la(5),is and • In addition to actual benefits to risk and pain-related changes. the nature ofthe these differences. example, accordto (36),regarding the trunk. However, literature farFor from consistent nociception, changes may be driven by maximization • In addition to actual benefits with respect to risk and ingthe to anature systematic review, there is support of both an increase regarding of these differences. For example, accordof perceived benefits. nociception, changes may be driven by maximization capacidad para controlar movimiento a decrease of trunk muscle activation in individuals with •el Originally adaptive changes havelumbar. negative consequences ing to aand systematic review, there is support of both an increase of perceived benefits. VAN DIEËN, J.H., H. FLOR, and P.W. HODGES. Low-Back pain patients learn to adapt motor behavior with adverse secondary consequences. Exerc. Sport Sci. Rev., Vol. 45, No. 4, pp. 223–229, 2017. We hypothesize that changes in motor behavior in individuals with low-back pain are adaptations aimed at minimizing the real or perceived risk of further pain. Through reinforcement learning, pain and subsequent adaptations result in less dynamic motor behavior, leading to increased loading and impoverished sensory feedback, which contribute to cortical reorganization and proprioceptive impairments that reduce the ability to control lumbar movement in a robust manner. Key Words: reinforcement learning, nociception, postural control, motor control, sensory feedback, perceived risk of pain Key Points • Low-back pain tends to change motor behavior toward increased coactivation, reduced deep muscle activity, and less within-subject variance.that may outweigh • Minimizing a weighted sum of costs, including the risk of losing control and nociceptive input, predicts these pain-related changes. • In addition to actual benefits with respect to risk and nociception, changes may be driven by maximization of perceived benefits. • Originally adaptive changes have negative consequences that may outweigh benefits in the long term. behind motor control changes in LBP should lead to more effective treatments. Motor control in LBP is changed at many levels of the nervous system. Studies of individuals with and without LBP have reported voluntary trunk muscle activation (45), LBP (45).of trunk muscle activation in individuals with benefits in differences the longinterm. and • Originally adaptive changes have negative consequences trunk muscle reflexes (32), and trunk kinematics (20) a anddecrease in corticalterm. mapping of sensory inputs from (5), andLBP motor outputs (45).Here, we propose a hypothesis on how LBP affects motor that may outweigh benefits in the long to (36), the trunk. However, the literature is far from consistent control, which may account for these inconsistencies. In reinINTRODUCTION Here, regarding the nature of these differences. For example, accord- we propose a hypothesis on how LBP affects motor forcement learning, a reward (positive reinforcement) or the ing to prevalent a systematic review, there is support is of the both an increase Low-back pain (LBP) is widely and, globally, control, which or may account these inconsistencies. In increases reinand a decrease of trunk muscle activation in individuals with absence reduction of afor cost (negative reinforcement) INTRODUCTION leading cause of years lived with due to the functional LBPdisability (45). forcement reward (positive reinforcement) or theand the learning, likelihood athat a performed behavior will be repeated Low-back limitations, pain (LBP)limited is widely prevalent and, globally, is the Here, we propose a hypothesis on howrecurLBP affects motor benefits of treatment, and frequent absence or reduction ofthis a cost (negative reinforcement) increases control, which may account for these inconsistencies. In reinthus learned. In context, movement-related pain may funcINTRODUCTION leading causerence of years lived with disability due to the functional (15). Motor control exercise is a commonly used treatment forcement learning, a reward (positive reinforcement) or the Low-back pain (LBP) is widely prevalent and, globally, is the the increases likelihood a performed behavior willsense be repeated tion as athat negative reinforcement and the of being and able to absence or reduction of a costrecurreinforcement) limitations, limited benefits offunctional treatment, and frequent leading cause of years lived disability due to the forwith LBP. Although systematic reviews support its(negative effectiveness, the likelihood that a performed behavior will bethus repeated and learned. Inpain this context, movement-related pain may funcprevent provocation as a positive reinforcement. Motor limitations, limited benefits of treatment, and frequent recurrence (15). Motor control exercise is aLBP, commonly used treatment thus learned. In thissize context, movement-related pain may funclike other treatments for the effect is not large (33). rence (15). Motor control exercise is a commonly used treatment canreinforcement be considered asand thethe outcome learning as acontrol sense of of abeing ableprocess to tion as a negative reinforcement and the sense oftion being able to negative forfor LBP. LBP. AlthoughAlthough systematic reviews support its effectiveness, A better understanding of the nature ofeffectiveness, and the mechanisms systematic reviews support itsprovocation prevent pain as a positive reinforcement. Motor at optimizing as a combination of costs and rewards. like other treatments for LBP, the effect size is not large (33). preventaimed pain provocation a positive reinforcement. MotorFor can benot considered as the outcome of a learning process other treatments forandLBP, the effectcontrol size is large (33). A like better understanding of the nature of the mechanisms clarity, costs orasrewards usually of area inverted, that a aimed at optimizing a combination of costs and rewards. For control can beeither considered the outcome learning such process A better understanding of the nature ofclarity, andeither the costsmechanisms or rewards usually are inverted, such that a sum of weighted costs can be minimized or a rewards. sum of weighted Address for correspondence: Jaap H. van Department Movement aimed at optimizing a combination of costs and For sumDieën, of weighted costs canof beHuman minimized or a sum of weighted Address for correspondence: Jaap H. van Dieën, Department of Human Movement Science, Research Institute Science, MOVE Research Institute Amsterdam,MOVE Vrije Universiteit Amsterdam, Van der Amsterdam, rewards Vrije can beUniversiteit maximized. Amsterdam, Van der can be clarity, rewards either costs or maximized. rewards usually are inverted, such that a Boechorststraat 9, NL-1081 BT Amsterdam, the Netherlands (E-mail: j.van.dieen@vu.nl). conditions, costs associated with control efforts Boechorststraat 9, NL-1081 BT Amsterdam, In thepain-free Netherlands (E-mail: j.van.dieen@vu.nl). Accepted for publication: February 7, 2017. In pain-free costs associated withofcontrol efforts or muscle activation are considered most important. We assume sum of weighted costsconditions, can be minimized or a sum weighted Editor:Address Roger M. Enoka, Accepted forJaap publication: 2017. for Ph.D. correspondence: H. vanFebruary Dieën,7,Department of Human Movement that with LBP, weighting of costs associated with potential loss or muscle activation are considered most important. We assume Editor:Institute Roger M.Amsterdam, Enoka, Ph.D.Vrije Universiteit Amsterdam, Van der Science, MOVE Research 0091-6331/4504/223–229 rewards of control over posture and movement and costs associated withcan be maximized. Exercise and Sport Sciences Reviews that with LBP, weighting of costs associated with potential loss potential pain provocation increase, and one learns to minimize Boechorststraat 9, NL-1081 BT Amsterdam, the Netherlands (E-mail: j.van.dieen@vu.nl). DOI: 10.1249/JES.0000000000000121 Inmuscle pain-free conditions, costs associated with control efforts 0091-6331/4504/223–229 this new weighted sum of costs. Although the resulting Copyright © 2017 by the American College of Sports Medicine of control over posture and movement and costs associated with Accepted for publication: February 7, 2017. Exercise and Sport Sciences Reviews or muscle activation considered most important. Wetoassume Editor: Roger M. Enoka, Ph.D. potential painare provocation increase, and one learns minimize DOI: 10.1249/JES.0000000000000121223 that with of costs associated with thisLBP, newweighting weighted sum of costs. Although thepotential resulting loss muscle Copyright © 2017 by the American College of Sports Medicine 0091-6331/4504/223–229 of control over posture and movement and costs associated with Copyright © 2017 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited. Exercise and Sport Sciences Reviews potential 223 pain provocation increase, and one learns to minimize DOI: 10.1249/JES.0000000000000121 this new weighted sum of costs. Although the resulting muscle Copyright © 2017 by the American College of Sports Medicine Copyright © 2017 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited. 223 Copyright © 2017 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited. ¿ES EFICAZ EL CONTROL MOTOR LUMBOPÉLVICO? ¿En el tratamiento de la Espondilolistesis? ¿Frente al placebo? ¿En el Dolor Lumbar Crónico Inespecífico? ¿Como Prevención de Recurrencia? ¿En el Dolor Lumbar con Hernia Discal? ¿En el Dolor Lumbopélvico del Embarazo y Postparto? ¿En la Diástasis Púbica? fisioterapiamanual.es Entrenamiento del Control Motor Lumbopélvico - 18 de marzo de 2021 16 ESPONDILOLISTESIS Reducción de dolor y discapacidad funcional y aumento de la movilidad en flexión y extensión de cadera en el grupo de estabilización O´Sullivan 1997 fisioterapiamanual.es DOLOR LUMBAR CRÓNICO INESPECÍFICO El control motor reduce el dolor y la discapacidad en el paciente con dolor lumbar. Los pacientes que realizan ejercicios de control motor mejoran su capacidad funcional y calidad de vida. Shaughnessy M 2004 Maher 2005 Goldby 2006 Cairns 2006 Franca 2010 fisioterapiamanual.es Contents lists available at ScienceDirect Musculoskeletal Science and Practice journal homepage: www.elsevier.com/locate/msksp Review article Effectiveness of movement control exercise on patients with non-specific low back pain and movement control impairment: A systematic review and Contents lists available at ScienceDirect meta-analysis Hannu Antero Luomajokia,∗, Maria Beatriz Bonet Beltrana, Silvia Careddua,b, Christoph Michael Bauera,c a b c Musculoskeletal Science and Practice Zurich University of Applied Sciences ZHAW, School of Health Professions, Institute of Physiotherapy, Technikumstrasse 71, Postfach, 8401 Winterthur, Switzerland Physio & Sport Luzern, Bruchstrasse 11, 6003 Luzern, Switzerland University of Tampere, School of Medicine, Kalevantie 4, FI-33014, University of Tampere, Tampere, Finland Movement Control Exercise may be more effective in journal homepage: www.elsevier.com/locate/msksp improving disability in the short and long term for people with LBP and Movement Control Impairment compared to other Review article interventions. A R T I C LE I N FO A B S T R A C T Keywords: Systematic review Meta-analysis Movement control exercise Movement control impairment Low back pain Background: Patients with low back pain (LBP) and movement control impairment (MVCI) show altered spinal movement patterns. Treatment that aims to change movement behaviour could benefit these patients. Objective: To assess the effectiveness of movement control exercise (MVCE) in terms of clinically relevant measures (disability and pain) on patients with NSLBP. Methods: A systematic review and meta-analysis were conducted. CINAHL, MEDLINE, PUBMED and PEDro databases were searched for RCT's evaluating MVCE treatment in patients with NSLBP from review inception to April 2017. Authors were contacted to obtain missing data and outcomes. PEDro was used to assess methodological quality of the studies and the GRADE approach was used to assess the overall quality of evidence Data were combined using a random effects meta-analysis and reported as standardized mean differences (SMD). Results: Eleven eligible RCT's including a total of 781 patients were found. Results show ‘very low to moderate quality’ evidence of a positive effect of MVCE on disability, both at the end of treatment and after 12 months (SMD -0.38 95%CI -0.68, −0.09 respectively 0.37 95%CI -0.61,-0.04). Pain intensity was significantly reduced after MVCE at the end of treatment (SMD -0.39 95%CI -0.69, −0.04), but not after 12 months (SMD -0.27, 95%CI -0.62, 0.09). Conclusions: MVCE intervention for people with NSLBP and MVCI appears to be more effective in improving disability compared to other interventions, both over the short and long term. Pain was reduced only in the short term. An important factor is the initial identification of patients with MVCI. Registration of the study: The study protocol registration number is CRD42016036662 on PROSPERO. Effectiveness of movement control exercise on patients with non-specific Pain was reduced in the short term, but not over the long term. low back pain and movement control impairment: A systematic review and meta-analysis Hannu Antero Luomajokia,∗, Maria Beatriz Bonet Beltrana, Silvia Careddua,b, Christoph Michael Bauera,c 1. Introduction a b c Low back pain (LBP) is a common condition that affects most people at some point in their lives, with up to an 84% lifetime prevalence (Airaksinen et al., 2006). The prevalence depends on factors such as sex, age, educational level and occupation (Delitto et al., 2012). It results in significant health and socioeconomic problems, being associated with work absenteeism, disability and high costs, both for patients and society (Saragiotto et al., 2016b). From 85% to 95% of affected LBP patients no pathoanatomic cause can be identified (Hoy et al., 2010) and they are designated as suffering from non-specific low back pain (NSLBP). One proposed mechanism driving NSLBP is movement control impairment (MVCI). The latter is defined as an alteration of the spinal alignment and movement pattern in a specific direction (Sahrmann, 2002; Harris-Hayes and Van Dillen, 2009). It has been suggested that it is a clinical feature of patients with NSLBP (O'Sullivan, 2005). This impairment occurs secondary to the presence of pain and can be due to abnormal tissue loading, lack of proprioceptive awareness and, possibly, the lack of a withdrawal reflex motor response (O'Sullivan, 2005). Other circumstances, such as psychological, social and neurophysiological factors, could contribute to reinforce this disorder (O'Sullivan, 2005). Zurich University of Applied Sciences ZHAW, School of Health Professions, Institute of Physiotherapy, Technikumstrasse 71, Postfach, 8401 Winterthur, Switzerland Physio & Sport Luzern, Bruchstrasse 11, 6003 Luzern, Switzerland University of Tampere, School of Medicine, Kalevantie 4, FI-33014, University of Tampere, Tampere, Finland A R T I C LE I N FO Keywords: Systematic review Meta-analysis Movement control exercise Movement control impairment Low back pain Abbreviations: MVCE, Movement control exercises; MVCI, Movement control impairment; LBP, Low back pain; NSLBP, Non-specific low back pain; SD, Standard deviation; SMD, Standardized mean differences ∗ Corresponding author. E-mail addresses: luom@zhaw.ch (H.A. Luomajoki), beabonet19@hotmail.com (M.B. Bonet Beltran), caredsil@zhaw.ch (S. Careddu), christoph.bauer@zhaw.ch (C.M. Bauer). A B S T R A C T https://doi.org/10.1016/j.msksp.2018.03.008 Received 6 July 2017; Received in revised form 4 March 2018; Accepted 26 March 2018 Background: Patients with low back pain (LBP) and movement control impairment (MVCI) show altered spinal movement patterns. Treatment that aims to change movement behaviour could benefit these patients. Objective: To assess the effectiveness of movement control exercise (MVCE) in terms of clinically relevant measures (disability and pain) on patients with NSLBP. Methods: A systematic review and meta-analysis were conducted. CINAHL, MEDLINE, PUBMED and PEDro databases were searched for RCT's evaluating MVCE treatment in patients with NSLBP from review inception to April 2017. Authors were contacted to obtain missing data and outcomes. PEDro was used to assess methodological quality of the studies and the GRADE approach was used to assess the overall quality of evidence Data were combined using a random effects meta-analysis and reported as standardized mean differences (SMD). Results: Eleven eligible RCT's including a total of 781 patients were found. Results show ‘very low to moderate Entrenamiento del Control Motor Lumbopélvico - 18 de marzo de 2021 d at ClinicalTrials.gov (US National Institutes of Health; NCT01061632). The authors certify that they have no affiliations with or y with a direct financial interest in the subject matter or materials discussed in the article. Address correspondence to Dr Ulrika ehabilitation, Umeå University, Vårdvetarhuset, Umeå 901 87 Sweden. E-mail: ulrika.aasa@umu.se ! Copyright ©2015 Journal [ RESEARCH REPORT Journal of Orthopaedic & Sports Physical Therapy® Downloaded from www.jospt.org at UIC Library of Health Sciences on February 6, 2015. For personal use only. No other uses without permission. Copyright © 2015 Journal of Orthopaedic & Sports Physical Therapy®. All rights reserved. 1,2 2,3 17 ] BJÖRN AASA, RPT, MaSci • LARS BERGLUND, RPT, MaSci • PETER MICHAELSON, RPT, PhD • ULRIKA AASA, RPT, PhD journal of orthopaedic & sports physical therapy | volume 45 | number 2 | february 2015 | 4 3 77 Individualized Low-Load Motor Control Exercises and Education Versus a HighLoad Lifting Exercise and Education 1/22/2015 to Improve Activity, Pain Intensity, and Physical Performance in Patients With Low [ RESEARCH REPORT ] Back Pain: A Randomized Controlled Trial 10:45:51 AM BJÖRN AASA, RPT, MaSci1,2 • LARS BERGLUND, RPT, MaSci2,3 • PETER MICHAELSON, RPT, PhD4 • ULRIKA AASA, RPT, PhD3 ! STUDY DESIGN: Randomized controlled trial. ! BACKGROUND: Low back pain is a common ! RESULTS: Both interventions resulted in significant within-group improvements in pain intensity, strength, and endurance. The LMC group showed significantly greater improvement on the Patient-Specific Functional Scale (4.2 points) compared with the HLL group (2.5 points) (P<.001). There were no significant betweengroup differences in pain intensity (P = .505), strength, and 1 of the 3 endurance tests. However, the LMC group showed an increase (from 2.9 to 5.9) on the movement control test subscale, whereas the HLL group showed no change (from 3.9 to 3.1) (P<.001). T here is growing evidence that altered posture and movement patterns are common in patients with low back pain (LBP).10,11,27,33,41 It is proposed that the repetition Journal of Orthopaedic & Sports Physical Therapy® Downloaded from www.jospt.org at UIC Library of Health Sciences on February 6, 2015. For personal use only. No other uses without permission. Copyright © 2015 Journal of Orthopaedic & Sports Physical Therapy®. All rights reserved. Motor Control Una intervenciónIndividualized de controlLow-Load motor de baja carga puede tener Exercises Education a Highmejores resultados en and control de laVersus actividad y el movimiento Load Lifting Exercise and Education comparado con carga alta, pero no en intensidad de dolor, fuerza o to Improve Activity, Pain Intensity, and resistencia. Physical Performance in Patients With Low Back Pain: A Randomized Controlled Trial disorder. Patients with low back pain frequently have aberrant and pain-provocative movement patterns that often are addressed with motor control exercises. ! OBJECTIVE: To compare the effects of low-load motor control (LMC) exercise and those of a highload lifting (HLL) exercise. ! METHODS: Seventy participants with recurrent low back pain, who were diagnosed with nociceptive mechanical pain as their dominating pain pattern, were randomized to either LMC or HLL exercise treatments. Participants were offered 12 treatment sessions over an 8-week period. All participants were also provided with education regarding pain mechanisms. ! METHODS: Participants were assessed prior to and following treatment. The primary outcome measures were activity (the Patient-Specific Functional Scale) and average pain intensity over the last 7 days (visual analog scale). The secondary outcome measure was a physical performance test battery that included 1 strength, 3 endurance, and 7 movement control tests for the lumbopelvic region. ! STUDY DESIGN: Randomized controlled trial. ! BACKGROUND: Low back pain is a common ! CONCLUSION: An LMC intervention may result in superior outcomes in activity, movement control, and muscle endurance compared to an HLL intervention, but not in pain intensity, strength, or endurance. Registered at ClinicalTrials.gov (NCT01061632). ! LEVEL OF EVIDENCE: Therapy, level 2b–. J Orthop Sports Phys Ther 2015;45(2):77-85. doi:10.2519/jospt.2015.5021 ! KEY WORDS: deadlift, functional rehabilitation, motor learning, stabilization exercises, subgrouping ! RESULTS: Both interventions resulted in significant within-group improvements in pain of altered alignments and movements may result in localized regions of tissue stress,1 which may provide a basis for ongoing nociceptive pain of mechanical character.38 A variety of interventions have been proposed to retrain postures and movement patterns. Common features are the use of relearning strategies and exercises to change spinal alignment,27,32,33,43 movement patterns,6,7,27,32,33,41,43 and muscle recruitment patterns in global7 and/or local muscles.9,15,22,40 Though there is no consensus on the umbrella term for these exercises, the present study refers to them as motor control exercises. According toevidence here is growing Shumway-Cook and Woollacott,34 mo- T that altered posture and movement patterns are Norrlandsklinikens Sweden. Department of Surgical and Perioperative Sciences,The UmeåLMC University, Umeå, Sweden. Department of Community Medicine and intensity, strength, and endurance. disorder. Patients with lowhälsocentral, back pain Umeå, frequently of Health Sciences, Luleå University of Technology, Luleå, Sweden. This study was conducted in an outpatient physical Rehabilitation, Umeå University, Umeå, Sweden. 4Department common in patients with group showed significantly greater improvement have aberrant and pain-provocative movement therapy clinic in Umeå, Sweden. This research was supported by 2 grants from Visare Norr and Norrbottens Läns Landsting. The study was approved by the Regional Ethical Review 10,11,27,33,41 on the Patient-Specific Functional Scale (4.2 patterns that often are addressed with motor Board in Umeå, Sweden (09-200M) and registered at ClinicalTrials.gov (US National Institutes of Health; NCT01061632). The authors that theypain have no affiliations with or lowcertify back (LBP). It financial involvement in any organization or entity with apoints) direct financial interestwith in thethe subject materials discussed in the article. Address correspondence to Dr Ulrika compared HLLmatter groupor (2.5 points) control exercises. proposed that©2015 the repetition Aasa, Department of Community Medicine and Rehabilitation, UmeåThere University, Vårdvetarhuset, Umeåbetween901 87 Sweden. E-mail: is ulrika.aasa@umu.se Journal ! Copyright (P<.001). were no significant ® ! OBJECTIVE: To compare the effects of low-load of Orthopaedic & Sports Physical Therapy group differences in pain intensity (P = .505), of altered alignments and movements motor control (LMC) exercise and those of a highstrength, and 1 of the 3 endurance tests. However, may result in localized regions of tissue load lifting (HLL) exercise. journal of orthopaedic & sports physical therapy | volume 45 | number 2 | february 2015 | 77 the LMC group showed an increase (from 2.9 stress,1 which may provide a basis for ! METHODS: Seventy participants with recurrent to 5.9) on the movement control test subscale, ongoing nociceptive pain of mechanical low back pain, who were diagnosed with nocicepwhereas the HLL group showed no change (from tive mechanical pain as their dominating pain character.38 3.9 to 3.1) (P<.001). 45-02 Aasa.indd 77 1/22/2015 10:45:51 AM pattern, were randomized to either LMC or HLL A variety of interventions have been exercise treatments. Participants were offered ! CONCLUSION: An LMC intervention may proposed to retrain postures and move12 treatment sessions over an 8-week period. All result in superior outcomes in activity, movement ment patterns. Common features are the participants were also provided with education control, and muscle endurance compared to an use of relearning strategies and exercises regarding pain mechanisms. HLL intervention, but not in pain intensity, strength, to change spinal alignment,27,32,33,43 moveor endurance. Registered at ClinicalTrials.gov ! METHODS: Participants were assessed prior ment patterns,6,7,27,32,33,41,43 and muscle (NCT01061632). to and following treatment. The primary outcome recruitment patterns in global7 and/or measures were activity (the Patient-Specific ! LEVEL OF EVIDENCE: Therapy, level 2b–. Functional Scale) and average pain intensity over local muscles.9,15,22,40 Though there is no J Orthop Sports Phys Ther 2015;45(2):77-85. the last 7 days (visual analog scale). The secondary consensus on the umbrella term for these doi:10.2519/jospt.2015.5021 outcome measure was a physical performance test exercises, the present study refers to them ! KEY WORDS: deadlift, functional rehabilitation, battery that included 1 strength, 3 endurance, and 7 as motor control exercises. According to movement control tests for the lumbopelvic region. motor learning, stabilization exercises, subgrouping 1 2 3 Shumway-Cook and Woollacott,34 mo- 1 Norrlandsklinikens hälsocentral, Umeå, Sweden. 2Department of Surgical and Perioperative Sciences, Umeå University, Umeå, Sweden. 3Department of Community Medicine and Rehabilitation, Umeå University, Umeå, Sweden. 4Department of Health Sciences, Luleå University of Technology, Luleå, Sweden. This study was conducted in an outpatient physical therapy clinic in Umeå, Sweden. This research was supported by 2 grants from Visare Norr and Norrbottens Läns Landsting. The study was approved by the Regional Ethical Review Board in Umeå, Sweden (09-200M) and registered at ClinicalTrials.gov (US National Institutes of Health; NCT01061632). The authors certify that they have no affiliations with or financial involvement in any organization or entity with a direct financial interest in the subject matter or materials discussed in the article. Address correspondence to Dr Ulrika Aasa, Department of Community Medicine and Rehabilitation, Umeå University, Vårdvetarhuset, Umeå 901 87 Sweden. E-mail: ulrika.aasa@umu.se ! Copyright ©2015 Journal of Orthopaedic & Sports Physical Therapy® journal of orthopaedic & sports physical therapy | volume 45 | number 2 | february 2015 | 77 45-02 Aasa.indd 77 1/22/2015 10:45:51 AM RECURRENCIA DEL DOLOR GRUPO CONTROL: 84% de recurrencia a un año, 56% dolor más incapacitante e intenso que el inicial GRUPO DE ESTABILIZACIÓN: 30% de recurrencia a un año, 33% de los casos de dolor intenso. 1ER AÑO COMO PERÍODO DE INTERVENCIÓN!!! Hides 2001 fisioterapiamanual.es HERNIA DISCAL: CIRUGÍA vs ESTABILIZACIÓN Tras 1 año no hay diferencias entre dos grupos de tratamiento: uno ha sufrido una cirugía de fusión vertebral, y otro una intervención cognitiva con ejercicios de estabilización y generales. fisioterapiamanual.es Los ejercicios con intervención cognitiva son una alternativa efectiva, con menor coste, a la artrodesis lumbar. Brox 2006 Entrenamiento del Control Motor Lumbopélvico - 18 de marzo de 2021 18 EMBARAZO GRUPO DE ESTABILIZACIÓN: - 75% Oswestry <25 - Disminución del dolor matutino y vespertino - Mejor calidad de vida (actividad física) - Pruebas físicas claramente mejores - Menor tasa de recurrencia a los 2 años GRUPO CONTROL: 25% Oswestry <25 Las diferencias se mantienen a los 2 años!!! fisioterapiamanual.es Stuge 2004 Stuge 2006 EMBARAZO Mujeres SANAS hasta 36 semanas de embarazo - GRUPO EXPERIMENTAL: ejercicio aeróbico y control motor - GRUPO CONTROL: cuidados habituales DOLOR LUMBOPÉLVICO: GE 55% GC 82% Menor nivel de dolor y discapacidad y mayor calidad de vida SKLEMPE KOKIC I 2017 fisioterapiamanual.es DIASTASIS PÚBICA Incidencia de 2,8% Tratamiento quirúrgico recomendado con separación >4cm? Tratamiento conservador: Reposo, mejor en decúbito lateral Cinturón pélvico Marcha con ayudas técnicas si es necesario Evitar la separación de los miembros inferiores y las actividades en carga, como la bipedestación Fisioterapia: CONTROL MOTOR (Shim & Oh 2012) DISFUNCIÓN PÚBICA (Depledge 2005) fisioterapiamanual.es • Tras 2 semanas de tratamiento: NPRS desciende de 9 a 4, PSFS mejora de 8.0 a 3.3, y la radiología muestra una mejora del 36% en la diástasis y es capaz de caminar 30m con faja pélvica. Urraca Gesto MA 2015 Entrenamiento del Control Motor Lumbopélvico - 18 de marzo de 2021 19 LO MÁS RECIENTE WHICH SPECIFIC MODES OF EXERCISE TRAINING ARE MOST EFFECTIVE FOR TREATING LOW BACK PAIN? NETWORK METAANALYSIS. 2020. DOSE-RESPONSE-RELATIONSHIP OF STABILISATION EXERCISES IN PATIENTS WITH CHRONIC NON-SPECIFIC LOW BACK PAIN: A SR WITH META-REGRESSION. 2020 fisioterapiamanual.es REVISIONES SISTEMÁTICAS Motor control exercise for Chronic Non-Specific LBP (PEDro synthesis). 2017. “THIS REVIEW PROVIDES SUPPORT FOR THE USE OF MCE IN PATIENTS WITH NSLBP”. Chou R et al. Nonpharmacologic therapies for LBP: a SR for an American College of Physicians Clinical Practice Guideline. Ann Inter Med 2017. “MCE SLIGHTLY MORE EFFECTIVE THAN GENERAL EXERCISE FOR PAIN AND FUNCTION”. Saragiotto BT et al. Motor control exercise for CLBP. Cochrane Database of Systematic Reviews 2016. “MCE HAS A CLINICALLY IMPORTANT EFFECT COMPARED WITH EXERCISE PLUS EPA… CHOICE OF EXERCISE SHOULD DEPEND ON PATIENT OR THERAPIST PREFERENCES, TRAINING, COSTS”. Byström MG et al. Motor control exercises reduces pain and disability in chronic and recurrent LBP: a MA. Spine 2013. “MCE IS SUPERIOR TO GENERAL EXERCISE, MANUAL THERAPY AND MINIMAL INTERVENTION IN REGARD TO DISABILITY AND PAIN”. fisioterapiamanual.es ¿QUÉ SABEMOS? Es una intervención más eficaz que el placebo Es EFICAZ en disminución de dolor. Es SUPERIOR en mejora del dolor y discapacidad al tratamiento habitual (información, educación, prescripción de ejercicio, medicación analgésica) y a una terapia física multimodal (electroterapia o fisioterapia con ejercicio general) a corto, medio y largo plazo Es EFICAZ en disminución de la DISCAPACIDAD, mejora la FUNCIÓN REDUCE la RECURRENCIA del dolor lumbar inespecífico Es un tratamiento eficaz en el dolor lumbar y pélvico en el embarazo fisioterapiamanual.es Entrenamiento del Control Motor Lumbopélvico - 18 de marzo de 2021