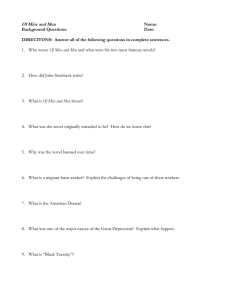
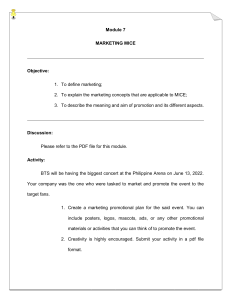
BASIC RESEARCH www.jasn.org Downloaded from http://journals.lww.com/jasn by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AW nYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 07/30/2023 IL-17C/IL-17 Receptor E Signaling in CD4+ T Cells Promotes TH17 Cell-Driven Glomerular Inflammation Sonja Krohn, Jasper F. Nies, Sonja Kapffer, Tilman Schmidt, Jan-Hendrik Riedel, Anna Kaffke, Anett Peters, Alina Borchers, Oliver M. Steinmetz, Christian F. Krebs, Jan-Eric Turner, Silke R. Brix, Hans-Joachim Paust, Rolf A. K. Stahl, and Ulf Panzer III. Medizinische Klinik, Universitätsklinikum Hamburg-Eppendorf, Hamburg, Germany ABSTRACT The IL-17 cytokine family and the cognate receptors thereof have a unique role in organ-specific autoimmunity. Most studies have focused on the founding member of the IL-17 family, IL-17A, as the central mediator of diseases. Indeed, although pathogenic functions have been ascribed to IL-17A and IL-17F in the context of immune-mediated glomerular diseases, the specific functions of the other IL-17 family members in immunity and inflammatory kidney diseases is largely unknown. Here, we report that compared with healthy controls, patients with acute Anti-neutrophil cytoplasmatic antibody (ANCA)-associated crescentic glomerulonephritis (GN) had significantly elevated serum levels of IL-17C (but not IL-17A, F, or E). In mouse models of crescentic GN (nephrotoxic nephritis) and pristane-induced lupus nephritis, deficiency in IL-17C significantly ameliorated the course of GN in terms of renal tissue injury and kidney function. Deficiency of the unique IL-17C receptor IL-17 receptor E (IL-17RE) provided similar protection against crescentic GN. These protective effects associated with a reduced TH17 response. Bone marrow transplantation experiments revealed that IL-17C is produced by tissue-resident cells, but not by lymphocytes. Finally, IL-17RE was highly expressed by CD4+ TH17 cells, and loss of this expression prevented the TH17 responses and subsequent tissue injury in crescentic GN. Our findings indicate that IL-17C promotes TH17 cell responses and immune-mediated kidney disease via IL-17RE expressed on CD4+ TH17 cells. Targeting the IL-17C/IL-17RE pathway may present an intriguing therapeutic strategy for TH17-induced autoimmune disorders. J Am Soc Nephrol 29: 1210–1222, 2018. doi: https://doi.org/10.1681/ASN.2017090949 The identification and characterization of IL-17A– producing CD4+ T cells, referred to as TH17 cells,1,2 have substantially advanced our understanding of organ-specific autoimmunity and are a topic of intense ongoing clinical and basic research. TH17 cells, characterized by the expression of the Received September 1, 2017. Accepted January 3, 2018. S.Krohn and J.F.N. contributed equally to this work. Published online ahead of print. Publication date available at www.jasn.org. Correspondence: Dr. Ulf Panzer, Medizinische Klinik, Universitätsklinikum Hamburg-Eppendorf, III. Martinistraße 52, 20246 Hamburg, Germany. Email: panzer@uke.uni-hamburg.de Copyright © 2018 by the American Society of Nephrology 1210 ISSN : 1046-6673/2904-1210 Significance Statement Recent studies have established the crucial role of the TH17/IL-17A pathway in the pathogenesis of autoimmune diseases, such as human and experimental crescentic GN. So far, the focus of most studies has been on the IL-17 founding member IL-17A as the central mediator of diseases. Here, we report that serum IL-17C levels were significantly elevated in patients with ANCA-associated crescentic GN. Moreover, using a murine model of crescentic GN, we provide direct evidence that IL-17C promotes TH17 cell responses and kidney injury via IL-17 receptor E, expressed on CD4+ TH17 cells. These findings have significant implications for the understanding of how the IL-17 cytokine family contributes to organ-specific TH17 autoimmunity and potentially for the development of novel treatment strategies. J Am Soc Nephrol 29: 1210–1222, 2018 www.jasn.org RESULTS Serum IL-17C Levels Are Elevated in Patients with ANCA-Associated Crescentic GN Using an ultrasensitive electrochemiluminescence immunoassay, we analyzed the serum levels of IL-17A, C, E, and F in 70 patients with biopsy-confirmed, acute ANCA-associated crescentic GN and in 20 healthy controls. Unexpectedly, we J Am Soc Nephrol 29: 1210–1222, 2018 IL-17F IL-17A Protein [pg/mL] Protein [pg/mL] 30 10 4 2 1500 500 150 100 50 0 0 Controls Controls ANCA GN ANCA GN IL-17E IL-17C *** Protein [pg/mL] Protein [pg/mL] 20 10 6 4 2 0 2.0 1.0 0.4 0.2 0.0 Controls ANCA GN Controls TNF-α ANCA GN IL-6 *** *** 20 60 Protein [pg/mL] Protein [pg/mL] Downloaded from http://journals.lww.com/jasn by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AW nYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 07/30/2023 transcription factor RORgt3 and the expression of CCR6,4,5 play a pivotal role in crescentic GN by producing proinflammatory cytokines.6–9 In particular, IL-17A and IL-17F may mediate tissue injury by the induction of renal CXCL1 and CXCL5 expression.10–12 These chemokines, in turn, recruit neutrophils into the kidney, which ultimately contributes to the organ damage.13 The IL-17 cytokine family consists of six members (IL-17A– F), of which IL-17A and F are the most closely related and best characterized ones.14 Their biologic effects are mediated by binding to heterodimeric receptors of the IL-17 receptor family (IL-17RA–RE). Except for the receptor for IL-17B (IL-17RB), all receptor complexes contain the ubiquitously expressed subunit IL-17RA and a second, ligand-specific receptor. So far, only the roles of IL-17A and IL-17F have been analyzed in the pathogenesis of immune-mediated glomerular diseases.10,11,15–17 The potential effect of the other IL-17 family members in renal autoimmunity and inflammation is unknown. First, we assessed the serum levels of the IL-17 family members in patients with ANCA-associated crescentic GN and analyzed the systemic and renal expression patterns of these cytokines and their receptors during the time course of an experimental model of crescentic GN (nephrotoxic nephritis [NTN]).18 Unexpectedly, these analyses demonstrated an upregulation of IL-17C and its specific receptor IL-17RE, suggesting a functional role for the IL-17C/IL-17RE axis in immune-mediated kidney diseases, and represented the rationale for our study. Pioneer studies indicated that IL-17C might share similar biologic features with IL-17A, as it stimulates inflammation by upregulating cytokines and chemokines that are characteristic of a TH17 response in epithelial cells.19 Moreover, the involvement of IL-17C in the immunopathogenesis of murine models for multiple sclerosis and arthritis,20,21 potentially by direct effects on the TH17 response, has been reported.20 The goal of this study was to elucidate the role of the IL-17C/ IL-17RE axis in immune-mediated glomerular diseases. We therefore induced an experimental model of crescentic GN (NTN) to (1) define the effect of IL-17C and its receptor IL17RE on the clinical outcome of the GN, (2) determine the significance of this ligand receptor pair for the T-cell immune response, and (3) identify the mechanisms by which the IL17C/IL-17RE pathway might drive renal tissue injury in experimental crescentic GN. BASIC RESEARCH 10 6 4 2 0 20 10 5 0 Controls ANCA GN Controls ANCA GN Figure 1. IL-17C levels are significantly elevated in patients with ANCA-associated crescentic GN. Serum level of IL-17 cytokines, TNF-a, and IL-6 in patients with ANCA-associated GN. Quantitative measurement of IL-17A, C, E, F, TNF-a, and IL-6 in the serum of patients with biopsy-proven ANCA GN (n=70) and healthy controls (n=20). Symbols represent individual data points with the mean as a horizontal line (***P,0.001). observed a marked elevation (P,0.001) in IL-17C protein levels in the ANCA GN patient group compared with healthy controls (Figure 1). No significant differences were detected in the levels of the remaining IL-17 family members (Figure 1). We also analyzed the levels of TNF-a and IL-6 as general markers for inflammation, which were significantly higher in the patient population compared with the control group (Figure 1). The clinical and demographic baseline characteristics of the patient group are shown in Supplemental Figure 1. IL-17C and IL-17RE Expression Is Upregulated in Experimental Crescentic GN Next, we aimed at investigating the expression pattern of the IL17 family members and their receptors during the time course of NTN. Renal quantitative PCR (qPCR) analyses during different periods of time (day 0 to day 30) of nephritic mice revealed the regulation of Il-17a mRNA expression, which is in agreement with our previous data.22 In addition, Il-17c expression was upregulated 12 hours after NTN induction (Figure 2A). A similar mRNA expression pattern of Il-17a and Il-17c was detected in the spleen (Figure 2B). We also IL-17C in Renal Inflammation 1211 BASIC RESEARCH A www.jasn.org Kidney 30 20 10 30 20 10 5d 10d 20d 30d Con 12h 24h 3d 20 10 0 30 20 10 5d 10d 20d 30d 30 20 10 0 40 30 20 10 24h 10d 10 5 40 30 20 10 4 3 2 1 0 Con Il-17e 24h 10d 30d Con 12h 24h 3d Il-17f 30 20 10 0 5 40 30 20 10 0 30d 5d 10d 20d 30d Il-17re 100 60 50 mRNA expression [x-fold of control] mRNA expression [x-fold of control] 40 5d 10d 20d 30d Il-17rc 100 60 50 30d 100 60 50 10d 1 Con 12h 24h 3d 0 0 24h 2 30d mRNA expression [x-fold of control] 20 Con 3 Il-17d 30 10d 4 0 Con mRNA expression [x-fold of control] mRNA expression [x-fold of control] Kidney 5 Il-17c 40 5d 10d 20d 30d Il-17ra 100 60 50 30d 100 60 50 24h 10 Con 12h 24h 3d 0 Con 20 5d 10d 20d 30d mRNA expression [x-fold of control] 40 10d 30 Il-17b mRNA expression [x-fold of control] mRNA expression [x-fold of control] Il-17a 24h 80 60 40 0 Con 12h 24h 3d C 100 60 50 5d 10d 20d 30d Il-17f 80 60 40 Spleen Con 10 Con 12h 24h 3d 0 Con 12h 24h 3d 20 5d 10d 20d 30d mRNA expression [x-fold of control] 30 30 Il-17e mRNA expression [x-fold of control] mRNA expression [x-fold of control] Il-17d 80 60 40 80 60 40 0 0 Con 12h 24h 3d B Il-17c 80 60 40 mRNA expression [x-fold of control] mRNA expression [x-fold of control] Il-17b 0 mRNA expression [x-fold of control] Downloaded from http://journals.lww.com/jasn by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AW nYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 07/30/2023 mRNA expression [x-fold of control] Il-17a 80 60 40 4 3 2 1 0 Con 24h 10d 30d Con 12h 24h 3d 5d 10d 20d 30d Figure 2. Expression of IL-17C and IL-17RE is upregulated in experimental crescentic GN. Renal expression of the IL-17 family and their receptors in crescentic GN. (A) qPCR analysis of Il-17a–f mRNA expression levels in the kidney, (B) the spleen, and (C) renal expression levels of Il-17ra, Il-17rc, and Il-17re at indicated time points after NTN induction. Controls (Con; n=5) and nephritic wild-type mice (n=4–7). mRNA levels are expressed as x-fold of controls. Symbols represent individual data points with the mean as a horizontal line. 1212 Journal of the American Society of Nephrology J Am Soc Nephrol 29: 1210–1222, 2018 www.jasn.org model. The histologic and functional parameters were analyzed to compare the clinical outcome in wild-type and Il-17c2/2 mice upon NTN induction (Figure 3). Quantification of the renal tissue damage, in terms of glomerular crescent formation and tubulointerstitial injury 10 days after NTN induction, revealed a reduction in Il-17c2/2 mice (Figure 3, A and B). In line with these results, we also found a significant reduction in BUN levels, and to a lesser degree in serum creatinine levels, whereas we did not find any changes in the urinary albumin-to-creatinine ratio (ACR) (Figure 3C). Assessment of renal leukocyte recruitment by immunohistochemical staining revealed that the tubulointerstitial infiltration of F4/80+ macrophages and CD3+ T cells was significantly IL-17C Promotes Renal Tissue Injury in Crescentic GN On the basis of the expression pattern of Il-17c in human and experimental GN described above, we examined whether IL17C signaling is involved in the pathogenesis of crescentic GN. Therefore, we analyzed Il-17c2/2 mice using the NTN mouse A Il-17c-/- NTN WT NTN PAS Control C 20 Con NTN 40 20 0 Con p=0.06 ** 80 BUN [mg/dL] 40 0 60 Interstitial Area [%] Crescents [%] 60 *** 60 40 20 0 NTN Con WT NTN 0.8 250 0.6 200 ACR [g/g] *** Serum Creatinine [mg/dL] B 0.4 0.2 150 100 50 0 0.0 Con NTN Con 60 40 20 0 Con NTN CD3+ cells / gcs MAC-2+ cells / gcs F4/80+ cells / hpf 80 6 10 8 6 4 2 0 Con NTN E 4 2 0 *** 100 CD3+ cells / hpf * 100 NTN Il-17c-/- D Con 80 60 40 20 0 NTN Con NTN F WT NTN Il-17c-/- NTN *** GR1+ cells / lpf 20 GR1+ Downloaded from http://journals.lww.com/jasn by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AW nYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 07/30/2023 observed a regulation of the mRNA expression of Il-17rc and Il-17re, which are the specific receptor subunits of IL-17A and IL-17C, respectively (Figure 2C). The receptor chain IL-17RA, which serves as a common receptor chain for all IL-17 ligands (except for IL-17B), was highly expressed throughout the course of crescentic GN, but did not show any changes in its expression pattern (Figure 2C). BASIC RESEARCH 15 10 5 0 Con NTN Figure 3. IL-17C promotes renal tissue injury in crescentic GN. (A) Representative photographs of PAS-stained kidney sections from control (Con), nephritic wild-type (WT), and nephritic Il-17c2/2 mice at day 10 of NTN (original magnification, 3400). (B) Quantification of glomerular crescent formation and tubulointerstitial damage. A combination of results from two independent experiments is shown. Controls (n=5), nephritic wild-type (n=11), and nephritic Il-17c2/2 mice (n=15). (C) BUN, serum creatinine, and ACR determined in the aforementioned groups. (D) Quantification of tubulointerstitial F4/80+, glomerular MAC-2+ and CD3+, and tubulointerstitial CD3+ cells in the aforementioned groups. (E) Representative photographs of GR-1–stained kidney sections from nephritic wild-type and nephritic Il-17c2/2 mice. Original magnification, 3400. (F) Quantification of tubulointerstitial GR-1+ cells in the aforementioned groups. Symbols represent individual data points with the mean as a horizontal line (*P,0.05; **P,0.01; ***P,0.001). J Am Soc Nephrol 29: 1210–1222, 2018 IL-17C in Renal Inflammation 1213 BASIC RESEARCH www.jasn.org Downloaded from http://journals.lww.com/jasn by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AW nYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 07/30/2023 Figure 4. IL-17C-driven tissue injury in crescentic GN is IL-17A-dependent. (A) Representative FACS plots of intracellular cytokine staining for IL-17A and IFN-g in renal T cells (pregated on singlets, live, CD45+, CD3+, and CD4+ cells). (B) Quantification of intracellular cytokine FACS analysis for IL-17A, IL-17F, and IFN-g in renal CD4+ T cells. Data are representative of two independent experiments 1214 Journal of the American Society of Nephrology J Am Soc Nephrol 29: 1210–1222, 2018 www.jasn.org reduced in nephritic Il-17c2/2 mice (Figure 3D). Staining of tubulointerstitial GR-1+ neutrophils showed a significant reduction in these cells in nephritic Il-17c2/2 mice (Figure 3, E and F). Downloaded from http://journals.lww.com/jasn by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AW nYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 07/30/2023 Amelioration of the GN Disease Course in Il-17c2/2 Mice Is a Consequence of a Reduced TH17/IL-17A Response To elucidate the immunologic mechanisms that lead to a less severe course of GN in Il-17c2/2 mice, we investigated the renal and systemic immune responses in these animals in more detail. Flow cytometry studies revealed a significant reduction in renal TH17 cells, whereas the TH1 cell response in the kidney was unaffected (Figure 4, A and B). To determine whether IL-17C might also modulate systemic immunity in the NTN model, we measured the serum concentration of several cytokines, including IL-17C. The concentration of IL-17C in the serum of nephritic mice was increased at day 10 and, as expected, was not detectable in nephritic Il-17c2/2 mice (Figure 4C). The analysis of serum IL-17A levels revealed a significant reduction in nephritic Il-17c2/2 mice compared with nephritic wild-type mice. Other effector cytokines related to TH17 immune responses did not show significant differences. The IFN-g serum level was slightly, but significantly, increased in Il-17c2/2 mice. IL-17C did not have major effects on the humoral immune response because nephritic wild-type and nephritic Il-17c2/2 mice had similar serum titers of anti-sheep total IgG, IgG1, IgG2a/c, IgG2b, and IgG3 antibodies directed against the nephritogenic antigen (Supplemental Figure 2, A and B). To further investigate the influence of IL-17C on the local immune/inflammatory response in the kidney, expression analyses of the renal cortex using a cytokine and chemokine pathwayfocused PCR array (RT2 Profiler) were performed. These analyses revealed a predominant downregulation of TH17/IL-17A–specific target genes in nephritic Il-17c2/2 mice (Figure 4D). Accordingly, qPCR analysis confirmed significantly reduced Cxcl2 and Cxcl5 mRNA expression in nephritic Il-17c2/2 mice. Likewise, we found a reduction in the neutrophil-attracting chemokine Cxcl1 as well as Ccl20, which interacts with the chemokine receptor CCR6 expressed on TH17 cells (Figure 4E). Moreover, IL-17C deficiency resulted in a reduction in the renal expression of IL1b and IL-6, whereas IL-23 expression was not affected (Figure 4E). This suggests that the downregulated TH17/IL-17A immune BASIC RESEARCH response in nephritic Il-17c2/2 mice might be responsible for the less severe crescentic GN. To test this hypothesis, we treated nephritic wild-type and nephritic Il-17c2/2 mice with a neutralizing anti–IL-17A antibody. IL-17A neutralization diminished the differences in kidney damage between the wild-type and knockout groups (Figure 4F). In line with these results, we did not observe a difference in the functional parameters of BUN, serum creatinine, or ACR (Figure 4G). Taken together, these results strongly indicate that the ameliorated GN disease course in Il-17c2/2 mice is a consequence of a reduced TH17/IL-17A response. IL-17C Is Produced by Resident Tissue Cells To study whether IL-17C in the kidney is mainly produced by resident renal tissue cells or by hematopoietic cells, we performed bone marrow (BM) transplantation studies using wild-type and Il-17c2/2 mice. Twenty-four hours after induction of nephritis (the time point of highest renal Il-17c mRNA expression), we obtained high Il-17c expression levels in animals with wild-type renal tissue cells. By contrast, Il-17c mRNA expression in Il17c2/2 mice receiving wild-type BM or Il-17c2/2 BM was not elevated (Supplemental Figure 3). These data indicate that Il17c is mainly expressed by resident kidney cells. IL-17C Does Not Induce Chemokine Expression in Resident Kidney Cells In order to investigate whether IL-17C has direct effects on resident kidney cells, murine proximal tubular and murine mesangial cells were cultured and stimulated with IL-17C (1–100 ng/ml), or TNF-a and IL-17A as positive control. RT-PCR analysis revealed the mRNA expression of IL-17RA and IL-17RE in both cell lines (data not shown). Stimulation with IL-17C alone had no effect on Cxcl1 and Cxcl5 mRNA expression and protein formation (Supplemental Figure 4, A– D), but a moderate, synergistic effect was observed after stimulation together with a IL-22 or TNF-a (data not shown). Taken together, these results argue against major effects of IL-17C on resident kidney cells, which is in contrast to the pathophysiologic concept of IL-17A and IL-17F. IL-17RE Deficiency Ameliorates Renal Injury in Crescentic GN To analyze whether deficiency in IL-17RE, the specific receptor of IL-17C, also protects against immune-mediated glomerular with nephritic wild-type (WT; n=6) and nephritic Il-17c2/2 mice (n=10). (C) Serum cytokine levels measured by electrochemiluminescence immunoassay analysis. Data are representative of two independent experiments with controls (Con; n=3), nephritic wild-type (n=7), and nephritic Il-17c2/2 mice (n=11). (D) Cytokine and chemokine expression profiles of nephritic Il-17c2/2 and nephritic wild-type control mice. The expression levels are normalized to the housekeeping gene b-actin (Actb). (E) qPCR analysis of renal Cxcl1, Cxcl2, Cxcl5, and Cxcl9, as well as Ccl5 and Ccl20 mRNA expression. A combination of results from two independent experiments is shown, from controls (n=5), nephritic wild-type (n=11), and nephritic Il-17c2/2 mice (n=15). mRNA levels are expressed as x-fold of controls. (F) Quantification of glomerular crescent formation and tubulointerstitial damage of controls (n=5), nephritic wild-type (n=8), and nephritic Il-17c2/2 mice (n=6) treated with a neutralizing anti–IL-17A antibody (400 mg administered intraperitoneally at days 2, 4, and 8 after NTN induction). (G) Levels of BUN and serum creatinine, and ACR determined in the aforementioned groups. Data are presented as bar graphs with the mean6SEM or symbols, which represent individual data points with the mean as a horizontal line (*P,0.05; **P,0.01). J Am Soc Nephrol 29: 1210–1222, 2018 IL-17C in Renal Inflammation 1215 BASIC RESEARCH www.jasn.org significantly reduced in nephritic Il-17re2/2 mice (Figure 5, E and F). Control IL-17RE Is Required for the Promotion of Renal TH17 Cell Responses In line with the observed immunologic phenotype in Il-17c2/2 mice, IL-17RE deficiency resulted in a significant reduction in the renal TH17 cell response in GN, whereas no effect was seen on the TH1 cell population (Figure 6, A and B). Analyses of the mRNA expression profiles of whole renal cortices revealed that the absence of IL-17RE had a predominant effect on TH17/IL-17A target genes because the neutrophil-attracting chemokines Cxcl1 and Cxcl5 showed a decreased upregulation in nephritic Il-17re2/2 mice compared with their nephritic wild-type counterparts (Figure 6C). In contrast, TH1 target Il17-re-/- NTN WT NTN PAS A C 40 20 0 40 20 0 Con NTN * 150 BUN [mg/dL] Interstitial Area [%] Crescents [%] 60 *** 60 100 50 0 Con NTN Con * 0.8 500 400 0.6 ACR [g/g] *** 80 Serum Creatinine [mg/dL] B 0.4 0.2 0.0 NTN 300 200 100 Con 0 NTN Con NTN D * 10 0 6 4 2 0 Con NTN WT NTN 3 2 1 40 20 0 Con NTN 0 Con WT E 60 CD3+ cells / hpf 20 4 CD3+ cells / gcs 8 MAC-2+ cells / gcs F4/80+ cells / hpf 30 Il-17re-/- NTN NTN Con NTN Il-17re-/- F * GR1+ cells / lpf 15 GR1+ Downloaded from http://journals.lww.com/jasn by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AW nYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 07/30/2023 disease, we compared the clinical course of experimental GN between wild-type mice and Il-17re2/2 mice. The evaluation of kidney sections stained with periodic acid–Schiff (PAS) for the presence of crescents and tubulointerstitial injury revealed a significant reduction in the destruction of regular tissue structures in nephritic Il-17re2/2 mice (Figure 5, A and B). BUN and serum creatinine levels of nephritic Il-17re2/2 mice were significantly reduced as compared with nephritic wild-type mice (Figure 5C), but no effect on ACR was detectable (Figure 5C). The migration of F4/80+ macrophages and CD3+ T cells into the kidney revealed no difference among nephritic wildtype and nephritic Il-17re2/2 mice (Figure 5D), whereas the number of glomerular Mac-2+ mononuclear phagocytes was increased in nephritic Il-17re2/2 mice (Figure 5D). Most importantly, the tubulointerstitial GR-1+ cell infiltration was 10 5 0 Con NTN Figure 5. IL-17RE–mediated signaling aggravates crescentic GN. (A) Representative photographs of PAS-stained kidney sections from control (Con), nephritic wild-type (WT), and nephritic Il-17re2/2 mice at day 9 of NTN (original magnification, 3400). (B) Quantification of glomerular crescent formation and tubulointerstitial damage. Data are representative of two independent experiments. Controls (n=2), nephritic wild-type (n=6), and nephritic Il-17re2/2 mice (n=5). (C) BUN, serum creatinine, and ACR were determined in the aforementioned groups. (D) Quantification of tubulointerstitial F4/80+, glomerular MAC-2+, glomerular CD3+, and tubulointerstitial CD3+ cells in the aforementioned groups. (E) Representative photographs of GR-1–stained kidney sections from nephritic wild-type and nephritic Il-17re2/2 mice. Original magnification, 3400. (F) Quantification of tubulointerstitial GR-1+ cells in the aforementioned groups. Symbols represent individual data points with the mean as a horizontal line (*P,0.05; ***P,0.001). 1216 Journal of the American Society of Nephrology J Am Soc Nephrol 29: 1210–1222, 2018 www.jasn.org WT NTN IL-17A Il-17re-/- NTN IL-17RE Is Expressed by CD4+ TH17 Cells and Is Instrumental for TH17 Responses and Subsequent Tissue Injury in Crescentic GN IFN-γ * 20 15 10 5 0 8 6 4 2 0 NTN Cxcl1 ** mRNAexpression [x-fold of control] 500 50 40 30 20 10 0 NTN WT C % IFN-γ+ of CD4+ cells 25 % IL-17F+ of CD4+ cells % IL-17A+ of CD4+ cells B 400 NTN Il-17re-/Cxcl5 Cxcl2 ** 800 10000 8000 600 300 6000 400 200 4000 200 100 0 2000 0 Con NTN 0 Con Ccl20 Ccl5 NTN Cxcl9 8 8 1500 Con NTN 10 2000 mRNAexpression [x-fold of control] Downloaded from http://journals.lww.com/jasn by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AW nYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 07/30/2023 genes such as Ccl5 and Cxcl9 were not affected in nephritic Il-17re2/2 mice. The serum titers of anti-sheep total IgG, IgG1, IgG2a/c, IgG2b, and IgG3 antibodies of nephritic wild-type and nephritic Il-17re2/2 mice showed no effect of IL-17RE–mediated signaling on the humoral immune response (Supplemental Figure 2, C and D). Kidney A BASIC RESEARCH 6 6 4 1000 4 500 2 2 0 0 Con NTN 0 Con WT NTN Con NTN Il-17re-/- Figure 6. IL-17RE promotes renal TH17 cell responses in crescentic GN. (A) Representative FACS plots of intracellular cytokine staining for IL-17A and IFN-g in renal T cells (pregated on singlets, live, CD45+, CD3+, and CD4+ cells). (B) Quantification of intracellular cytokine FACS analysis for IL-17A, IL-17F, and IFN-g in renal CD4+ T cells. Nephritic wild-type (WT; n=6) and nephritic Il-17re2/2 mice (n=5). (C) Renal qPCR J Am Soc Nephrol 29: 1210–1222, 2018 To investigate the cellular expression pattern of IL-17RE, NK1.1 + NK cells, CD11b + /CD11c + /MHC2 + monocytes/macrophages, CD19+ B cells, and CD3+/CD4+ T cells from the kidneys of control and nephritic mice were sorted by FACS. Subsequent RT-PCR analysis revealed that Il17re expression is primarily upregulated by CD4 + T cells (Figure 7A). Using IL17A YFP+ fate reporter mice,23 we isolated CD4+ TH17 cells from the kidney and, by qPCR, compared their Il-17re mRNA expression with CD4 + T H 17 2 cells. As shown in Figure 7B, Il-17re expression was increased in the T H 17 cell population. Finally, we polarized CD4+ T cells in vitro in TH1, TH17, regulatory T cells, and T H 0 cells and assessed the Il-17re expression. In line with the other experiments, TH17 cells demonstrated the highest expression level of the receptor (Figure 7C). Because of the lack of suitable IL-17RE antibodies, it is currently not feasible to confirm these data by flow cytometry. To study the potential function of IL17RE in the TH17 response, we isolated CD4+ T cells from the spleen of CD45.1 wild-type and CD45.2 Il-17re 2 /2 mice and transferred them into Rag12/2 mice (competitive adoptive transfer, 1:1 ratio), mRNA expression analysis of Cxcl1, Cxcl2, Cxcl5, and Cxcl9, as well as Ccl5 and Ccl20. mRNA levels are expressed as x-fold of controls (Con). Data are representative of two independent experiments with controls (n=2), nephritic wild-type (n=6), and nephritic Il17re2/2 mice (n=5). Data are presented as individual data points with the mean as a horizontal line (*P,0.05; **P,0.01). IL-17C in Renal Inflammation 1217 www.jasn.org B + Mo/MФ (CD11b ) B cells (CD19 ) T cells (CD3+) 0.0 0.5 1.0 1.5 2.0 50 10 5 0 2.5 % of IL-17A+ CD4+ cells CD45.1 (WT) CD4 100 TH0 TH1 TH17 Treg ** WT Il-17re-/- 60 40 20 0 Rag1-/- NTN + Il-17re-/- CD4+ cells F ** 80 PAS Crescents [%] Rag1 Control 10 NTN Rag1-/- NTN + WT CD4+ cells -/- 20 80 CD45.2 (KO) E 30 0 D IL-17A 40 IL-17A- IL-17A+ YFP- YFP+ Il-17re mRNA expression [x-fold of non-nephritic group] 60 40 20 *** 80 0 60 40 20 0 Con NTN Con NTN G ** 10 5 0 H 100 50 0 Con NTN 80 150 60 100 40 50 20 NTN 1.0 0.5 Con NTN Cxcl5 ** 150 100 Ccl20 Cxcl9 ns 400 1000 300 800 600 200 400 50 0 NTN Rag1-/Rag1-/- + WT CD4+ cells Rag1-/- + Il-17re-/- CD4+ T cells 1.5 Cxcl2 200 Con 2.0 0.0 Con Cxcl1 0 2.5 MAC2+ cells / gcs 15 ** 150 F4/80+ cells / hpf GR1+ cells / lpf 20 mRNA expression [x-fold of control] Downloaded from http://journals.lww.com/jasn by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AW nYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 07/30/2023 + 15 mRNA expression [x-fold of TH0] NK cells (NK1.1+) Il-17re C Il-17re mRNA expression [x-fold of IL-17A- YFP-] A Interstitial Area [%] BASIC RESEARCH 100 0 Con NTN 200 0 Con NTN 0 Con NTN Con NTN Figure 7. IL-17RE is highly expressed by CD4+ T cells and promotes renal tissue injury in crescentic GN. (A) Regulation of Il-17re mRNA expression on selected FACS sorted renal leukocyte subsets under nephritic conditions (n=4). (B) Il-17re mRNA expression profile of IL17A2, YFP2, and IL-17A+, YFP+ sorted renal CD4+ T cells of nephritic IL-17A YFP+ fate reporter mice. (C) Il-17re mRNA expression profile of cells isolated from naïve mice and cultured under TH0-, TH1-, TH17-, or Treg-polarizing conditions for 65 hours (n=5). mRNA levels are expressed as x-fold of controls. (D) Representative FACS plots and quantification of IL-17A+ cells from nephritic Rag12/2 mice repopulated with CD45.1 wild-type (WT) and CD45.2 Il-17re2/2 CD4+ T cells. (n=7). (E) Representative photographs of PASstained kidney sections of Rag12/2 controls (Con; n=3), nephritic Rag12/2 mice repopulated with 1.53106 wild-type CD4+ T cells (n=6), and nephritic Rag12/2 mice repopulated with 1.53106 Il-17re2/2 CD4+ T cells (n=8) at day 10 of NTN (original magnification, 3400). (F) Quantification of glomerular crescent formation and tubulointerstitial damage of the aforementioned groups. 1218 Journal of the American Society of Nephrology J Am Soc Nephrol 29: 1210–1222, 2018 www.jasn.org Downloaded from http://journals.lww.com/jasn by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AW nYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 07/30/2023 which are deficient in T cells and B cells. Subsequently, we induced NTN and analyzed the “origin” of renal TH17 cells at day 10, using the congenic markers CD45.1 and CD45.2. As shown in Figure 7D, the deficiency in IL-17RE on CD4+ T cells led to a significantly reduced renal TH17 cell response compared with the wild-type group. In addition, we performed adoptive transfer experiments to investigate the effect of IL-17RE–expressing CD4+ T cells on the clinical course of crescentic GN. Therefore, CD4+ T cells from the spleen of wild-type and Il-17re2/2 mice were isolated and separately transferred into Rag12/2 mice. Six days after the adoptive cell transfer, NTN was induced. Rag12/2 mice reconstituted with Il-17re2/2 CD4+ T cells developed a less severe course of the GN with respect to glomerular crescent formation and tubulointerstitial injury (Figure 7, E and F). In agreement with the reduced TH17 response, the recruitment of neutrophils into the kidney was decreased (Figure 7G), as was the expression of Cxcl5 (Figure 7H). IL-17C Plays a Role in a Chronic Model of Lupus Nephritis We then assessed the effect of IL-17C deficiency in the chronic model of pristane-induced lupus nephritis. The application of pristane resulted in early mortality because of the development of severe pulmonary vasculitis,24 which was comparable between wild-type and Il-17c2/2 mice (Supplemental Figure 5A). Twelve months after pristane injection (the point of time when lupus nephritis was established), renal analysis was performed. PAS staining of renal tissue sections showed glomerular alterations, including hypercellularity, segmental proliferation, hyalinosis, and capillary wall thickening, as well as an increase of glomerular area as a sign of immune-mediated kidney damage (Supplemental Figure 5, B and C). A comparison of pristane-treated wildtype and Il-17c2/2 mice revealed that the percentage of abnormal glomeruli tended to be reduced in Il-17c2/2 mice (Supplemental Figure 5C), and the glomerular area of pristane-treated Il-17c2/2 mice was significantly decreased compared with pristane-treated wild-type mice (Supplemental Figure 5C). Moreover, BUN levels were significantly reduced in Il-17c2/2 lupus mice (Supplemental Figure 5D). Humoral immunity and immunologic reactivity were determined by analyzing glomerular IgG deposition and anti-dsDNA and anti–U1-snRNP autoantibody production, respectively. No difference was observed between wild-type and Il-17c 2/2 lupus mice (Supplemental Figure 5, E–G). BASIC RESEARCH DISCUSSION Here, we demonstrate that the IL-17C/IL-17RE axis significantly contributes to renal tissue injury in a murine model of crescentic GN. Our findings indicate that IL-17C promotes TH17 cell responses via IL-17RE, expressed on CD4+ TH17 cells. This results in increased renal expression of IL-17 target genes, such as the chemokines CXCL1 and CXCL5, and further recruitment of neutrophils, ultimately leading to tissue injury. In recent years IL-17A and, to lesser degree, IL-17F and IL17RA have been identified as important proinflammatory regulators and potential therapeutic targets in autoimmune and inflammatory kidney diseases, including human and experimental crescentic GN.6–8,25–28 However, the potential function of other IL-17 cytokines and IL-17 receptors is still unclear. We measured serum protein levels of the IL-17 cytokine family members in 70 patients with ANCA-associated GN, the most common form of crescentic GN. Surprisingly, we found no significant differences in IL-17A, E, and F levels in the ANCA GN patient group compared with healthy controls, but a highly significant increased level of IL-17C. An upregulated expression of IL-17C was also detectable in a model of crescentic GN (NTN), suggesting a potential role of this cytokine in crescentic GN. We were not able to detect significant serum levels of IL-17B and D. The biologic role of IL-17C is not well characterized and its function in renal autoimmune and inflammatory kidney diseases is unknown. IL-17C was cloned in 2000 by large-scale screen of expressed sequence tag databases for proteins homologous to IL17A.29 Six years later, the specific receptor subunit IL-17RE was identified by a sequence-based homology search.30 The observation that IL-17C binds to IL-17RE was made in 2011.19,20 During the past decade, the interaction of IL-17C and IL17RE has been reported to have proinflammatory effects by stimulating innate immune responses on epithelial cells in response to bacterial or sterile inflammatory stimuli.31,32 Toll-like receptor signaling has been identified as one pathway to upregulate IL-17C in these disease entities.19 IL-17C then drives innate immune responses in an autocrine manner in epithelial cells to fight off the infection. Yet little is known about the involvement of the IL-17C/IL-17RE axis in the pathogenesis of autoimmune diseases. Recently, it was suggested that the axis plays a role in autoimmune hepatitis by induction of IL-2 in CD4 + T cells which, in turn, stimulate NK cells to cause hepatic damage.33 Also, IL-17C had proinflammatory effects in an imiquimod-induced mouse model of autoimmune skin inflammation.19 Chang et al. suggested that IL-17RE is expressed on TH17 cells and that its signaling has an effect on the IL-17A production (G) Quantification of tubulointerstitial GR-1+ cells, tubulointerstitial F4/80+ cells, and glomerular MAC-2+ cells in the aforementioned groups. (H) Renal qPCR mRNA expression analysis of Cxcl1, Cxcl2, Cxcl5, and Cxcl9, as well as Ccl20. mRNA levels are expressed as x-fold of controls. Data are presented as bar graphs with the mean6SEM or symbols, which represent individual data points with the mean as a horizontal line (**P,0.01; ***P,0.001). J Am Soc Nephrol 29: 1210–1222, 2018 IL-17C in Renal Inflammation 1219 BASIC RESEARCH www.jasn.org Downloaded from http://journals.lww.com/jasn by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AW nYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 07/30/2023 of cultured TH17 cells overexpressing the receptor subunit.20 They also report that IL-17C is implicated in the pathogenesis of experimental autoimmune encephalomyelitis. Moreover, IL17C serum levels were increased in patients with active inflammatory bowel diseases.34 We studied the function of IL-17C in a well established model of crescentic GN (NTN). Compared with wild-type mice, IL-17C–deficient mice developed less severe disease, with significantly better renal function, and a reduced frequency of glomerular crescent formation and tubulointerstitial tissue injury. In line with this, the lack of IL-17RE (the unique receptor for IL-17C) also resulted in an ameliorated course of the GN in terms of renal function and tissue damage. Additionally, studies in the chronic model of pristane-induced lupus nephritis showed that IL-17C–deficient lupus mice had a moderately improved course of the disease. In summary, these results demonstrated for the first time the pathogenic role of the IL-17C/IL-17RE axis in immune-mediated glomerular disease. Mechanistically, we provide evidence that the IL-17C/IL17RE axis directly stimulates the nephritogenic TH17 response and thereby promotes renal tissue injury in crescentic GN. This hypothesis is on the basis of the finding that (1) renal IL-17A–producing TH17 cells, the expression of IL-17 target genes, and the infiltration of neutrophils were selectively reduced in nephritic Il-17c2/2 and Il-17re2/2 mice; (2) application of a neutralizing IL-17A antibody diminished the observed differences in kidney damage between nephritic wild-type and Il-17c2/2 animals; (3) IL-17RE is highly expressed on renal CD4+ TH17 cells; and (4) the transfer of IL17RE–deficient CD4+ T cell into Rag12/2 mice resulted in a reduced renal TH17 response and subsequent tissue injury in crescentic GN. Our attempts to study the IL-17C/IL-17RE–induced signaling pathways in TH17 cells that potentiate the TH17 cell response were hampered by the lack of suitable FACS antibodies for IL-17RE and the lack of available IL-17RE reporter mice, and remains to be fully elucidated. First experiments indicated that IL-17C/IL-17RE did not influence the polarization of naïve T cells toward TH17 cells in vitro (data not shown), suggesting that other pathways such as TH17 cell maintenance, expansion, or stabilization are involved in the process. Our study highlighted major differences in the biologic function of IL-17C compared with IL-17A and IL-17F. IL17C is predominantly expressed by resident cells in the kidney, whereas in the spleen different cell populations, including mononuclear phagocytes, expressed IL-17C mRNA. Further studies are clearly needed to characterize in detail the cellular source of IL-17C under inflammatory and homeostatic conditions. So far, we have not been able to establish reliable IL-17C immunohistochemical staining in the kidney or spleen. In contrast, IL-17A and F are derived from renal TH17 cells or gd T cells in GN. Moreover, IL-17C has only weak effects on resident kidney cells, in terms of proinflammatory chemokine induction, but directly promotes systemic TH17 response via 1220 Journal of the American Society of Nephrology IL-17RE signaling. This is different compared with IL-17A and F, which are supposed to act locally on renal cells and might explain why systemic levels of IL-17C reflect the local TH17 response in the kidney better than IL-17A or F. On the basis of our finding that IL-17C stimulates the TH17 cell response upstream of IL-17A, targeting of the IL-17C/IL-17RE pathway may present an intriguing therapeutic strategy for TH17driven autoimmune and inflammatory diseases, especially because neutralization of the TH17/IL-17A axis has already been confirmed to be an effective concept of treating autoimmune diseases such as psoriasis.35,36 CONCISE METHODS Human Study Cohort A total of 70 patients were recruited in this study (Hamburg Glomerulonephritis Registry). The inclusion criterion was biopsyproven, ANCA-associated GN. The trial was performed in accordance with the declaration of Helsinki. After informed consent was obtained, patient data and renal biopsy samples were collected according to the guidelines of the respective local ethics committees. Animals Il-17c2/2 mice were obtained from the Mutant Mouse Regional Resource Centers (University of California, Davis, CA). Il-17re2/2 mice were kindly provided by Bristol-Myers Squibb Company (Princeton, NJ). Rag12/2 mice were obtained from the Jackson Laboratory. All mice were on the C57BL/6J background. Age-matched C57BL/6J wild-type controls were bred in our facility. All mice were raised under specific pathogen-free conditions. All animal experiments were performed according to national and institutional animal care and ethical guidelines and were approved by the local authorities. Induction of Experimental GN and Functional Studies NTN was induced by intraperitoneal injection of 2.5 mg of nephrotoxic sheep serum per gram of body weight into 8–12-week-old male mice.10 Lupus nephritis was induced by intraperitoneal injection of 0.5 ml pristane into 8–10-week-old male mice.37,38 Urine samples were collected by housing the mice in metabolic cages for 3–5 hours. Urinary albumin excretion was determined by standard ELISA technology (Mice-Albumin Kit; Bethyl), and urinary creatinine, BUN, and serum creatinine levels were measured using standard laboratory methods. qPCR Analyses Total RNA of the renal cortex and cell subsets were prepared according to standard laboratory methods. qPCR analyses were performed for 40 cycles on a StepOnePlus Real-Time PCR system (Applied Biosystems, Foster City, CA). The samples were run in duplicate and normalized to 18S rRNA. The cytokine and chemokine expression profiles were determined using the Mouse cytokines & chemokines RT2 Profiler PCR Array (Qiagen, Hilden, Germany). The samples were normalized to the housekeeping gene b-actin (Actb). Data were analyzed using the StepOne Software v2.0. J Am Soc Nephrol 29: 1210–1222, 2018 www.jasn.org Electrochemiluminescence Immunoassay Downloaded from http://journals.lww.com/jasn by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AW nYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 07/30/2023 Mouse cytokine serum levels as well as serum samples from patient visits to our clinic, thawed on ice, were analyzed using a customized Meso Scale Discovery immunoassay (U-Plex Th17 Combo 2). This technology includes biotinylated and conjugated SULFO-TAG detection antibodies to simultaneously measure different analytes in a one microtiter well. Unprocessed serum from each patient (50 ml) was thawed and analyzed for the cytokines according to the manufacturer’s protocol (Meso Scale Discovery, Rockville, MD). Electrochemiluminescence was detected using the QuickPlex SQ120 instrument. Analyses were performed with the MSD Discovery Workbench software v4.0. Morphologic Analyses Immunohistochemistry was performed using routine laboratory methods. Glomerular crescent formation and tubulointerstitial injury were assessed in PAS-stained paraffin sections in a blinded fashion, as described.11 BASIC RESEARCH Assessment of the Humoral and Cellular Nephritogenic Immune Responses Mouse anti-sheep IgG antibody titers were determined in sera by ELISA as previously described.42 Anti–dsDNA-IgG and anti–U1-snRNP-IgG antibodies were analyzed by ELISA as previously described.11 Flow Cytometry Cells were stained with fluorochrome-labeled antibodies directed against CD45, CD3, CD4, CD8, gdTCR, NK1.1, IL-17A, IL-17F, IL22, IFN-g, CD11b, and Ly6G (BioLegend, BD Biosciences, eBioscience, or R&D Systems) as previously described.39 Flow cytometry measurements were performed using the BD FACS LSR II. Data were analyzed by using the FlowJo software (Tree Star). Neutralization Experiments The animals were treated with 400 mg of a neutralizing mouse antimurine IL-17A antibody (clone MM17F3; BioCell). The antibody was injected intraperitoneally on days 2, 4, and 8 after induction of NTN, as described.22 Isolation of Leukocytes from Murine Kidney The leukocytes from murine kidneys were isolated as previously described.39 Briefly, kidneys were digested for 45 minutes at 37°C by adding 0.4 mg/ml collagenase D (Roche, Mannheim, Germany) and 0.01 mg/ml DNase I (Roche) to RPMI 1640 (Life Technologies, Karlsruhe, Germany) medium supplemented with 10% heat-inactivated FCS (Gibco, Eggenstein, Germany). Subsequently, kidneys were finely minced using the gentle MACS Dissociator (Miltenyi Biotec, Teterow, Germany). Single-cell suspensions were separated using Percoll density gradient centrifugation. Culturing and Stimulation of Mouse Kidney Tubular and Mesangial Cells Mouse kidney tubular cells40 and mouse kidney mesangial cells41 were cultured in DMEM medium (Life Technologies) containing 3%–10% FCS (Gibco), 100 U/ml penicillin, and 100 mg/ml streptomycin (Life Technologies) at 37°C with 5% CO2. The cells were incubated in serum-free DMEM medium 24 hours before stimulation. Cells were stimulated with IL-17C (10 ng/ml), TNF-a (10 ng/ml), and IL-22 (100 ng/ml), or with a combination. Cells were harvested after 4 hours of stimulation and stored at 280°C for mRNA analyses. The protein levels in the supernatant were determined after 24 hours of incubation, using a specific ELISA according to the manufacturer’s protocol (R&D Systems, Wiesbaden, Germany). CD4+ T Cell Polarization For polarization of naïve CD4+ cells, splenocytes were isolated from naïve wild-type mice using the MACS CD4+ T Cell Isolation Kit, mouse (Miltenyi Biotec). A total of 23105 cells/well was plated in anti-CD3 antibody-coated 96-well plates (eBioscience, San Diego, CA) and incubated for 65 hours with soluble anti-CD28. The following cytokines and neutralizing antibodies were used: for TH0 conditions, anti–IFN-g and IL-2; for TH1-polarizing conditions, anti–IL-4 and recombinant IL-12; for TH17-polarizing conditions, anti–IL-4, anti–IFN-g, IL-6, TGF-b, IL-1b, and IL-23; and for Treg-polarizing conditions, anti–IFN-g, IL-2, and TGF-b (all BioLegend). J Am Soc Nephrol 29: 1210–1222, 2018 BM Transplantation BM transplantation was performed as previously described.12 Briefly, age-matched Il-17c2/2 mice and C57BL/6J wild-type mice received 9.5 Gy total body irradiation. Each recipient mouse (Il-17c2/2 mice or wild-type) obtained 303106 BM cells (Il-17c2/2 or wild-type cells) by intravenous injection. NTN was induced 2 weeks after irradiation and BM transplantation. Cell Transfer in Rag12/2 Mice CD4+ cells were isolated by magnetic-activated cell sorting with the Mouse CD4+ Cell Isolation Kit II (Miltenyi Biotec). We intravenously injected 1.53106 cells into Rag12/2 mice. NTN was induced 6 days after cell transfer. Statistical Analyses The results are shown as the mean6SEM when presented as a bar graph or as single data points with the mean in a scatter dot plot. Differences between two individual experimental groups were compared using a two-tailed t test. For survival analysis the Kaplan–Meier plot with a log-rank test was used. P,0.05 was considered to be statistically significant. ACKNOWLEDGMENTS FACS sorting was performed at the Universitätsklinikum HamburgEppendorf FACS sorting core facility. This study was supported by grants from the Deutsche Forschungsgemeinschaft(Sonderforschungsbereich1192: toU.P. andR.A.K.S.). DISCLOSURES None. REFERENCES 1. Park H, Li Z, Yang XO, Chang SH, Nurieva R, Wang YH, et al: A distinct lineage of CD4 T cells regulates tissue inflammation by producing interleukin 17. Nat Immunol 6: 1133–1141, 2005 IL-17C in Renal Inflammation 1221 BASIC RESEARCH www.jasn.org Downloaded from http://journals.lww.com/jasn by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AW nYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 07/30/2023 2. Harrington LE, Hatton RD, Mangan PR, Turner H, Murphy TL, Murphy KM, et al: Interleukin 17-producing CD4+ effector T cells develop via a lineage distinct from the T helper type 1 and 2 lineages. Nat Immunol 6: 1123–1132, 2005 3. Ivanov II, McKenzie BS, Zhou L, Tadokoro CE, Lepelley A, Lafaille JJ, et al: The orphan nuclear receptor RORgammat directs the differentiation program of proinflammatory IL-17+ T helper cells. Cell 126: 1121– 1133, 2006 4. Hirota K, Yoshitomi H, Hashimoto M, Maeda S, Teradaira S, Sugimoto N, et al: Preferential recruitment of CCR6-expressing Th17 cells to inflamed joints via CCL20 in rheumatoid arthritis and its animal model. J Exp Med 204: 2803–2812, 2007 5. Reboldi A, Coisne C, Baumjohann D, Benvenuto F, Bottinelli D, Lira S, et al: C-C chemokine receptor 6-regulated entry of TH-17 cells into the CNS through the choroid plexus is required for the initiation of EAE. Nat Immunol 10: 514–523, 2009 6. Turner JE, Paust HJ, Steinmetz OM, Panzer U: The Th17 immune response in renal inflammation. Kidney Int 77: 1070–1075, 2010 7. Kitching AR, Holdsworth SR: The emergence of TH17 cells as effectors of renal injury. J Am Soc Nephrol 22: 235–238, 2011 8. Krebs CF, Schmidt T, Riedel JH, Panzer U: T helper type 17 cells in immune-mediated glomerular disease. Nat Rev Nephrol 13: 647–659, 2017 9. Suárez-Fueyo A, Bradley SJ, Klatzmann D, Tsokos GC: T cells and autoimmune kidney disease. Nat Rev Nephrol 13: 329–343, 2017 10. Paust HJ, Turner JE, Steinmetz OM, Peters A, Heymann F, Hölscher C, et al: The IL-23/Th17 axis contributes to renal injury in experimental glomerulonephritis. J Am Soc Nephrol 20: 969–979, 2009 11. Riedel JH, Paust HJ, Krohn S, Turner JE, Kluger MA, Steinmetz OM, et al: IL-17F promotes tissue injury in autoimmune kidney diseases. J Am Soc Nephrol 27: 3666–3677, 2016 12. Disteldorf EM, Krebs CF, Paust HJ, Turner JE, Nouailles G, Tittel A, et al: CXCL5 drives neutrophil recruitment in TH17-mediated GN. J Am Soc Nephrol 26: 55–66, 2015 13. Caster DJ, Powell DW, Miralda I, Ward RA, McLeish KR: Re-examining neutrophil participation in GN. J Am Soc Nephrol 28: 2275–2289, 2017 14. Gaffen SL, Jain R, Garg AV, Cua DJ: The IL-23-IL-17 immune axis: From mechanisms to therapeutic testing. Nat Rev Immunol 14: 585–600, 2014 15. Ooi JD, Phoon RK, Holdsworth SR, Kitching AR: IL-23, not IL-12, directs autoimmunity to the Goodpasture antigen. J Am Soc Nephrol 20: 980– 989, 2009 16. Tulone C, Giorgini A, Freeley S, Coughlan A, Robson MG: Transferred antigen-specific T(H)17 but not T(H)1 cells induce crescentic glomerulonephritis in mice. Am J Pathol 179: 2683–2690, 2011 17. Zhang Z, Kyttaris VC, Tsokos GC: The role of IL-23/IL-17 axis in lupus nephritis. J Immunol 183: 3160–3169, 2009. 18. Artinger K, Kirsch AH, Aringer I, Moschovaki-Filippidou F, Eller P, Rosenkranz AR, et al: Innate and adaptive immunity in experimental glomerulonephritis: A pathfinder tale. Pediatr Nephrol 32: 943–947, 2017 19. Ramirez-Carrozzi V, Sambandam A, Luis E, Lin Z, Jeet S, Lesch J, et al: IL-17C regulates the innate immune function of epithelial cells in an autocrine manner. Nat Immunol 12: 1159–1166, 2011 20. Chang SH, Reynolds JM, Pappu BP, Chen G, Martinez GJ, Dong C: Interleukin-17C promotes Th17 cell responses and autoimmune disease via interleukin-17 receptor E. Immunity 35: 611–621, 2011 21. Yamaguchi Y, Fujio K, Shoda H, Okamoto A, Tsuno NH, Takahashi K, Yamamoto K: IL-17B and IL-17C are associated with TNF-alpha production and contribute to the exacerbation of inflammatory arthritis. J Immunol, 179: 7128–7136, 2007. 22. Paust HJ, Turner JE, Riedel JH, Disteldorf E, Peters A, Schmidt T, et al: Chemokines play a critical role in the cross-regulation of Th1 and Th17 immune responses in murine crescentic glomerulonephritis. Kidney Int 82: 72–83, 2012 23. Hirota K, Duarte JH, Veldhoen M, Hornsby E, Li Y, Cua DJ, et al: Fate mapping of IL-17-producing T cells in inflammatory responses. Nat Immunol 12: 255–263, 2011 1222 Journal of the American Society of Nephrology 24. Kluger MA, Melderis S, Nosko A, Goerke B, Luig M, Meyer MC, et al: Treg17 cells are programmed by Stat3 to suppress Th17 responses in systemic lupus. Kidney Int 89: 158–166, 2016 25. Koga T, Ichinose K, Tsokos GC: T cells and IL-17 in lupus nephritis. Clin Immunol 185: 95–99, 2017 26. Ramani K, Pawaria S, Maers K, Huppler AR, Gaffen SL, Biswas PS: An essential role of interleukin-17 receptor signaling in the development of autoimmune glomerulonephritis. J Leukoc Biol 96: 463–472, 2014 27. Ghali JR, O’Sullivan KM, Eggenhuizen PJ, Holdsworth SR, Kitching AR: Interleukin-17RA promotes humoral responses and glomerular injury in experimental rapidly progressive glomerulonephritis. Nephron 135: 207–223, 2017 28. Kurts C, Panzer U, Anders HJ, Rees AJ: The immune system and kidney disease: Basic concepts and clinical implications. Nat Rev Immunol 13: 738–753, 2013 29. Li H, Chen J, Huang A, Stinson J, Heldens S, Foster J, et al: Cloning and characterization of IL-17B and IL-17C, two new members of the IL-17 cytokine family. Proc Natl Acad Sci U S A 97: 773–778, 2000 30. Li TS, Li XN, Chang ZJ, Fu XY, Liu L: Identification and functional characterization of a novel interleukin 17 receptor: A possible mitogenic activation through ras/mitogen-activated protein kinase signaling pathway. Cell Signal 18: 1287–1298, 2006 31. Song X, Zhu S, Shi P, Liu Y, Shi Y, Levin SD, et al: IL-17RE is the functional receptor for IL-17C and mediates mucosal immunity to infection with intestinal pathogens. Nat Immunol 12: 1151–1158, 2011 32. Peng T, Chanthaphavong RS, Sun S, Trigilio JA, Phasouk K, Jin L, et al: Keratinocytes produce IL-17c to protect peripheral nervous systems during human HSV-2 reactivation. J Exp Med 214: 2315–2329, 2017 33. Huang J, Yuan Q, Zhu H, Yin L, Hong S, Dong Z, Jin W, Dong C: IL-17C/ IL-17RE augments T cell function in autoimmune hepatitis. J Immunol 198: 669–680, 2017 34. Friedrich M, Diegelmann J, Schauber J, Auernhammer CJ, Brand S: Intestinal neuroendocrine cells and goblet cells are mediators of IL17A-amplified epithelial IL-17C production in human inflammatory bowel disease. Mucosal Immunol 8: 943–958, 2015 35. Leonardi C, Matheson R, Zachariae C, Cameron G, Li L, Edson-Heredia E, et al: Anti-interleukin-17 monoclonal antibody ixekizumab in chronic plaque psoriasis. N Engl J Med 366: 1190–1199, 2012 36. Mease PJ, Genovese MC, Greenwald MW, Ritchlin CT, Beaulieu AD, Deodhar A, et al: Brodalumab, an anti-IL17RA monoclonal antibody, in psoriatic arthritis. N Engl J Med 370: 2295–2306, 2014 37. Summers SA, Hoi A, Steinmetz OM, O’Sullivan KM, Ooi JD, Odobasic D, et al: TLR9 and TLR4 are required for the development of autoimmunity and lupus nephritis in pristane nephropathy. J Autoimmun 35: 291–298, 2010 38. Kitching AR, Holdsworth SR, Ploplis VA, Plow EF, Collen D, Carmeliet P, et al: Plasminogen and plasminogen activators protect against renal injury in crescentic glomerulonephritis. J Exp Med 185: 963–968, 1997 39. Krebs CF, Paust HJ, Krohn S, Koyro T, Brix SR, Riedel JH, et al: Autoimmune renal disease is exacerbated by S1P-receptor-1-dependent intestinal Th17 cell migration to the kidney. Immunity 45: 1078–1092, 2016 40. Wolf G, Mueller E, Stahl RA, Ziyadeh FN: Angiotensin II-induced hypertrophy of cultured murine proximal tubular cells is mediated by endogenous transforming growth factor-beta. J Clin Invest 92: 1366–1372, 1993 41. Wolf G, Haberstroh U, Neilson EG: Angiotensin II stimulates the proliferation and biosynthesis of type I collagen in cultured murine mesangial cells. Am J Pathol 140: 95–107, 1992 42. Paust HJ, Ostmann A, Erhardt A, Turner JE, Velden J, Mittrücker HW, et al: Regulatory T cells control the Th1 immune response in murine crescentic glomerulonephritis. Kidney Int 80: 154–164, 2011 This article contains supplemental material online at http://jasn.asnjournals. org/lookup/suppl/doi:10.1681/ASN.2017090949/-/DCSupplemental. J Am Soc Nephrol 29: 1210–1222, 2018