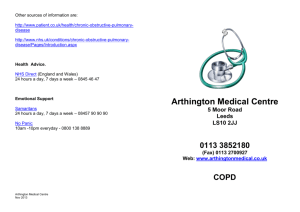
PERSPECTIVE Small Airways in COPD Peter J. Barnes, D.M., D.Sc. Chronic obstructive pulmonary disease (COPD) is a major and growing global health problem. It ranked as the sixth most common cause of death worldwide in 1990, and the Global Burden of Disease Study predicted that it would become the third most common cause by 2020.1 COPD has already risen to fourth place and is the only common cause of death in the United States whose prevalence has increased over the past 20 years. Even more important, it is an increasingly common cause of chronic disability and is predicted to become the fifth most common cause of disability in the world by 2020. COPD is also an increasingly common cause of hospital admissions and loss of time from work, resulting in a major health care expenditure that now exceeds the costs associated with asthma by more than a factor of three. Yet among common diseases, COPD has been relatively neglected, with less investment in research on its underlying cellular and molecular mechanisms and no therapies that have been shown to slow the relentless progression of the disease. COPD is caused by long-term exposure to inhaled noxious gases and particles; cigarette smoke accounts for more than 90 percent of cases in developed countries. In developing countries, the inhalation of smoke from biomass fuels is also an important cause of COPD, particularly among women who cook in poorly ventilated homes. COPD develops in only a minority of heavy smokers (10 to 20 percent), indicating that there are differences in individual susceptibility to the effects of cigarette smoking. The classic epidemiologic studies of Fletcher and Peto demonstrated that death and disability from COPD were related to an accelerated decline in lung function over time, with a loss of more than 50 ml per year in the forced expiratory volume in one second (FEV1), as compared with a normal loss of 20 ml per year.2 The progressive reduction in FEV1 and increasing severity of disease over time result in increasing shortness of breath on exertion that slowly advances to respiratory failure. n engl j med 350;26 www.nejm.org There has been much debate about the reasons for this accelerated loss in FEV1 and its relation to the pathogenesis of the disease. Three major mechanisms have been implicated (see Figure). The first is a loss of elasticity and the destruction of the alveolar attachments of airways within the lung as a result of emphysema, which results in a loss of support and closure of small airways during expiration. The second is the narrowing of small airways as a result of inflammation and scarring, and the third is the blocking of the lumen of small airways with mucous secretions. These three mechanisms interact with one another, and all may be induced by cigarette smoking and the inhalation of noxious agents, but the contribution of each mechanism may vary from person to person. The narrowing of small airways results in hyperinflation of the lungs, which are unable to empty; this effect, in turn, results in dyspnea on exertion and, eventually, even at rest. Hogg and colleagues in this issue of the Journal (pages 2645–2653) provide new information about the role of small airways in the progression of COPD, obtained by carefully quantifying the histologic changes in small airways at different stages in the disease and relating these changes to the impairment in FEV1. A major finding of their study is the significant association between the severity of disease, as measured by the percent of the predicted value for FEV1, and the thickness of the walls of small airways. The increased airway thickness results from infiltration by inflammatory cells (macrophages, neutrophils, and lymphocytes), as well as from structural changes, including increases in smooth muscle and fibrosis under the epithelium and in the outer part of the wall. A weaker association was found between the severity of disease and the degree of occlusion of the lumen by mucous secretions from surface goblet cells and an inflammatory exudate. A striking feature of the most severe disease was the presence of lymphoid follicles composed of B lymphocytes surrounded by T lymphocytes, suggesting an acquired immune response, june 24, 2004 The New England Journal of Medicine Downloaded from nejm.org at UNIVERSITY OF SUSSEX on August 11, 2015. For personal use only. No other uses without permission. Copyright © 2004 Massachusetts Medical Society. All rights reserved. 2635 Small Airways in COPD PERSPECTIVE Chronic Obstructive Pulmonary Disease Luminal occlusion by secretion of mucus glycoproteins and inflammatory exudate Fibrosis Loss of elasticity and disrupted alveolar attachments Thickening of airway wall Lymphoid follicles in severe disease Goblet cells Figure. Small-Airway Obstruction in Chronic Obstructive Pulmonary Disease (COPD). Airflow in small airways (internal diameter, <2 mm) may be limited in COPD by three mechanisms. First, alveolar attachments may have reduced elasticity and become disrupted as a result of emphysema. Second, the airway wall may be thickened by an inflammatory-cell infiltrate (composed of macrophages, neutrophils, and B and T lymphocytes), by structural changes (increased thickness of airway smooth muscle and fibrosis), and in severe disease, by lymphoid follicles. Third, the airway lumen may be occluded by mucous secretions (mucus glycoproteins secreted from surface goblet cells and inflammatory exudate). possibly to bacterial antigens arising from the chronic bacterial colonization that is a feature of severe disease. This study highlights the importance of inflammation in small airways as a determinant of the progression and severity of disease. The inflammatory response in patients with COPD represents an amplification of the inflammatory response to irritants that is seen in normal smokers.3 The molecular mechanisms underlying this amplification are uncertain, but they may result from gene polymor- 2636 phisms. What is remarkable is that the inflammatory response in COPD appears to increase with the severity of disease and therefore with time, rather than “burning out,” as it has been shown to do in other chronic inflammatory diseases such as rheumatoid arthritis and interstitial lung disease. This observation has important implications for future therapy for COPD and suggests that treatments directed at these mechanisms should be of value at all stages of the disease, even in patients with the most severe illness. n engl j med 350;26 www.nejm.org june 24, 2004 The New England Journal of Medicine Downloaded from nejm.org at UNIVERSITY OF SUSSEX on August 11, 2015. For personal use only. No other uses without permission. Copyright © 2004 Massachusetts Medical Society. All rights reserved. Small Airways in COPD PERSPECTIVE The study by Hogg et al. also confirms previous reports that the inflammatory response in the airways of patients with COPD does not resolve on the cessation of smoking: all the patients with very severe disease and most of those with severe disease had stopped smoking many years previously. This finding suggests that the inflammation, at least in severe disease, becomes independent of the causal mechanism. The reason for the persistence of inflammation is unknown, but a clue may be provided by the increased numbers of activated T lymphocytes, which may include memory T cells that may perpetuate the chronic inflammatory response. This hypothesis suggests that immunosuppressant therapies may be of value. The airway inflammation in COPD appears to be resistant to corticosteroids, and there appears to be an active cellular mechanism of corticosteroid resistance.4 New therapies must target the inflammation in small airways as well as emphysema in the lung parenchyma.5 Although emphysema is now detectable with the use of high-resolution computed tomography, it is difficult to quantify the narrowing of small airways: imaging techniques have inadequate resolution, and physiological measurements are difficult to interpret because there is abnormal airflow in larger airways. Therefore, it will be difficult to assess the effects of new treatments on small-airway function, and it will be important to develop new techniques in order to do so. For now, the data presented by Hogg et al. focus our attention on the inflammatory response of small airways, a neglected area of research. From the National Heart and Lung Institute, Imperial College, London. 1. Lopez AD, Murray CC. The global burden of disease, 19902020. Nat Med 1998;4:1241-3. 2. Fletcher C, Peto R. The natural history of chronic airflow obstruction. BMJ 1977;1:1645-8. 3. Barnes PJ. New concepts in chronic obstructive pulmonary disease. Annu Rev Med 2003;54:113-29. 4. Barnes PJ, Ito K, Adcock IM. Corticosteroid resistance in chronic obstructive pulmonary disease: inactivation of histone deacetylase. Lancet 2004;363:731-3. 5. Barnes PJ. New treatments for COPD. Nat Rev Drug Discov 2002;1:437-46. Pediatric Renal-Replacement Therapy — Coming of Age Dawn S. Milliner, M.D. Before the middle of the 20th century, the prospect that a child with end-stage renal disease (ESRD) would reach adulthood was essentially nil. Once dialysis and transplantation became available, that death sentence was lifted, as increasing numbers of children with ESRD were offered renal-replacement therapy. Now, most can expect to live for many years. The time course of this improvement in prognosis is reflected in the data from the Australia and New Zealand Dialysis and Transplant Registry presented by McDonald and Craig in this issue of the Journal (pages 2654–2662). These authors examined the long-term survival of children and adolescents who were less than 20 years of age when renalreplacement therapy was provided, and their report chronicles the marked improvement in expected survival during the past four decades. Similar improvement in prognosis has been evident throughout the developed world. n engl j med 350;26 www.nejm.org Renal failure during childhood has profound effects. Abnormalities of skeletal development, with associated growth retardation, affect most patients. Abnormal neurocognitive development, pubertal delay, and disordered psychosocial maturation also occur. Renal-replacement therapy in the form of dialysis provides only a small fraction of normal renal clearance. Dialysis alleviates — but does not eliminate — uremic symptoms such as fatigue and anorexia and does not address the nearly universal abnormalities of growth and development. In contrast, renal transplantation can provide renal function that is 40 to 80 percent of the normal level. A successful transplantation is followed by improved linear growth, particularly in younger children; improved cognitive performance, as reflected by standardized neurocognitive testing and school attendance; enhanced psychosocial development; and an improved quality of life for the june 24, 2004 The New England Journal of Medicine Downloaded from nejm.org at UNIVERSITY OF SUSSEX on August 11, 2015. For personal use only. No other uses without permission. Copyright © 2004 Massachusetts Medical Society. All rights reserved. 2637