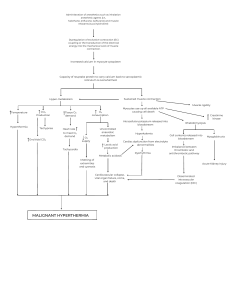
PAER 311 WEEK 3: ELECTROTHERAPY ES TO MUSCLE CONTRACTION NMES – NEUROMUSCULAR ELECTRICAL STIMULATION • • • • Use of electrical current on MOTOR NERVES to produce contractions on INNERVATED MUSCLES. Requirements: INTACT & FUNCTIONING PNS. Can: o Strengthen muscle o Improve cardiovascular health o Retard or prevent muscle atrophy o Reduce spasticity o Restore function Uses: CVA, SCI, sports-related injury, post-op conditions, healthy athelets. Order of Recruitme nt Force Onset Physiologicallyinitiated Contraction Small Nerve Fibers (SlowTwitch Type I ms fibers): x Low-Force • Fatigueresistant • Atrophyresistant ElecrticallyStimulated Ms Contraction Largest Nerve Fibers (FastTwitch Type II ms fibers): • Strongest • Quickest x fatigues rapidly x disuse: atrophies rapidly Large Gradually increase Small Reached Threshold: All motor units fire simultaneously Rapid, Jerky Smooth TWO MECHANISMS TO STRENGTHEN MUSCLES Overload Principle Greater Load placed on a muscle + Higher force of muscle contraction = More muscle strength gained With Physio Exercise: Load can be progressively increased by increasing the RESISTANCE Specificity Theory Muscle contractions specifically strengthen the muscle fibers that contract Electrical stimulation has more effect on type II muscle fibers than on type I muscle fibers. With Electrical Stimulation Connection: Increased by: • Increasing total current amount • Adjusting pulse duration and amplitude • Changing electrode size • Increasing externally applied resistance Electrical Stimulation of Muscle Contraction To produce STRENGTH gains in: • ES ms contraction: very effective in strengthening muscle weakened by disuse However, patients should perform both electrically stimulated and physiological contraction, if possible, to optimize the functional integration of strength gains produced by stimulation • Healthy muscles: force of the stimulated contraction needs to be at least 50% of the maximum voluntary isometric contraction (MVVIC) force o Greatest strength gains will be achieved with the maximally tolerated force of contraction After an Injury: initially have a force of as little as 10% of MVIC o Stronger contractions will be more effective if they are tolerated and will be necessary to achieve full strength. 1|Page To optimize ENDURANCE gains • • Prolonged periods of stimulation with lowerforce contractions • CLINICAL APPLICATION ORTHOPEDIC CONDITIONS SURGICAL • Applying NMES prior surgery → increased post-operative strength & more rapid functional improvement • following orthopedic surgery → immobilization + rest = Type II Fiber Atrophy ACL Reconstruction Surgery • Electrical stimulation can retard early decline of isometric quads strength TKA: Total Knee Arthroplasty • Voluntary Exercise + NMES = improved quads strength ORTHOPEDIC CONDITIONS NON-SURGICAL Knee 1. Osteoarthritis & Rheumatoid Arthritis • Chronic inflammatory Conditions -> Type II Muscle Fibers Atrophy • NMES: Decreases pain, increases quads strength, improves functional performance (walking and stair climbing) 2. PFS: Patellofemoral Syndrome • NMES to VVMO -> Increases VMO force generation Biceps • NMES to Biceps during Resisted Elbow Flexion = accelerated strengthening & functional recovery NEUROLOGICAL DISORDERS • ES can increase strength & improve motor control in patients c CNS damage ( SCI, CVA & other neuro conditions ), AS LONG AS PERIPHERAL MOTOR NERVES ARE INTACT. • Sensory input produced by motor level stimulation may provide cue for patient to • initiate movement or activate ms group 0r may promote reflexive motor contraction. Sensory stimulation s motor level stimulation may also enhance brain plasticity & cortical motor output. Patterned sensory level stimulation, using an intermittent stimulus, c an on:off time but s stimulation of ms contractions may enhance motor control by promoting reciprocal inhibition 0f antagonist ms. FES: Functional Electrical Stimulation - NMES + functional activity by stimulating contractions at the time during an activity when ms should contract.) SCI: • ES does not reverse spinal cord damage, but reduces complications & improves quality of life NMES COUNTERACTS DISUSE MUSCLE ATROPHY AND IMPROVES CIRCULATION FES contracts muscles to assist with locomotion and to assist with other body functions • Criteria to be effective: - LMN, NMJ & ms must be intact + method of delivery must be acceptable to pt - Contracts ms to assist c locomotion & other body functions - Must produce a contraction of sufficient force to carry out desired activity - Must be painless - Must be able to be controlled & repeated SCI: • FES for Ambulation - Locomotion produced required patients to use a walker for stability & support - Locomotion was very slow & requires high-level of energy expenditure by patient - Only practical for short distances around home; impractical for community mobility NMES of Glutes → increase tissue Oxygenation & redistribute surface pressure → reduced risk of Pressure Ulcer 2|Page Electrically stimulated Cycling → increases BMD (Bone Mineral Density) by 10% - 30% → reduced risk of Osteoporosis & associated fractures Multiple Sclerosis (MS): ES on Peroneal Nerve during swing phase -> Improves walking speed & decreased energy expenditure Implantable FES Systems • Phrenic Nerve Stimulation → contracts diaphragm to assist with inspiration Abdominal & Chest Wall Stimulation → improves coughing and clearing secretions Sacral Nerve Stimulation → assists bowel & bladder voiding SPORTS MEDICINE/PERFORMANCE Most sports require Agility, Coordination of Agonist/Antagonist muscle Groups, Flexibility, Proprioception & Motor Control & Balance ↓ NOT IMPROVED WITH NMES CVA/Stroke: a. Stimulation of weakened lower extremity agonist muscle = improves voluntary recruitment of motor units, improve gait, increase Ankle DF torque, reduce agonist-antagonist cocontraction, increase probability of returning home. b. NMES of Antagonist Muscle = can reduce spasticity (by activating reciprocal inhibition of agonist muscle), improve strength and improve function c. NMES to Sequentially Stimulate Agonist followed by Antagonist Muscle = To mimic “typical” behavior of individuals with CNS dysfunction = More effectively reduces spasticity CVA/Stroke continuation Estimulated muscle contractions can support or assist c joint positioning or movement, functioning similarly to an orthosis 1. Shoulder Subluxation 2. Peroneal N. Stimulation = assists DF in Swing phase of Gait 3. Grasp 4. Stationary Cycling Sensory Level ES = reduces spasticity, increase strength, & increase function; enhances brain plasticity → enhancing cortical motor output. Other Neurological Conditions: • ES can be used in any patients with CNS dysfunction with an intact PNS such as those with TBI (Traumatic Brain Injury), MS (Multiple Sclerosis), or CP (Cerebral Palsy) • Cerebral Palsy (CP): NMES + Dynamic Bracing = decrease spasticity, increases function and grip strength and improve posture Addition of NMES to a training program → assists in sports that rely more heavily on strength NMES is NOT a substitute for sport-specific training, and it CANNOT overcome deficits in coordination, balance, and motor control • For NonAthletes, incorporating NMES into rehab program can likely improve strength, but is NOT a substitute for a comprehensive program of exercises that challenges multiple systems simultaneously in a functional manner. OTHER CONDITIONS a. Swallowing difficulties (dysphagia) b. Preventing ms atrophy that occurs in astronauts as a result of living in a ZeroGravity environment c. Disuse Atrophy in patients confined to bed d. Urinary Incontinence associated with Pelvic Floor Dysfunction e. Promote Blood Flow in Healthy Individuals and in patients c poor circulation f. Promoting venous circulation and preventing DVTs EMS – ELECTRICAL MUSCLE STIMULATION • • • • Application of electrical currently directly to MUSCLE to produce a ms contraction For DENERVATED ms o Denervation causes ms atrophy & fibrosis → ES on ms retards or even reverses these A Continuous Direct Current (DC) applied for a number of seconds to produce contractions Electrical current must be longer than 10 milliseconds 3|Page Precautions for the use of Electrical Currents for Muscle Contraction • • • • • • • • Cardiac disease Impaired mentation or sensation Malignant tumors Skin irritation or open wounds o Be aware of potential DOMS (delated onset muscle soreness) after electrical stimulation Demand pacemaker or unstable arrhythmias Over the carotid sinus Venous or arterial thrombosis or thrombophlebitis Pelvis, abdomen, trunk, and low back during pregnancy o Additional: Epilepsy, Pharyngeal/Laryngeal muscle o Don’t use ES to contract muscle if it will disrupt healing (torn muscle, tendinitis) PARAMETERS FOR INNERVATED MUSCLE Electrodes Electrode Placement: Patient with allergic reaction to adhesive electrodes: • • One electrode: over the motor point Other electrode: on the muscle • Electrodes o Must be parallel to the direction of muscle fibers o At least 2 inches apart Motor Point: - Where an electrical stimulus will produce the greatest contraction with the least amount of electricity - Area of skin where motor nerve enters the muscle - Mostly over the middle of the muscle belly Electrodes 4|Page 5|Page Motor Points of the Posterior Aspects of Upper Extremity MOTOR POINTS AREA Motor points of muscle innervated by facial nerves Motors points of the anterior aspect of upper extremity MUSCLE 1. Frontalis 2. Corrugator 3. Orbicularis Oculi 4. Nasalis 5. Zygomaticus 6. Buccinator 7. Levators of upper lip 8. Orbicularis Oris 9. Depressor anguli oris 10. Depressor labii infirioris 11. Mentalis 1. Middle fibers of deltoid 2. Anterior Deltoid 3. Pectoralis Major 4. Coraco Brachalis 5. Biceps Brachii 6. Pronator Teres 7. Brachioradialis 8. Flexor Carpi Ulnaris 9. Flexor Carpi Radialis 10. Palmaris Longus 11. Flexor Digitorum Profundus 12. Flexor Policis Longus 13. Flexor Digitorum Superficialis 14. Abductor Policis Longus 15. Opponencepolicis 16. Flexor Policis 17. Abductor Digiti Minimi Motor Points of Back Motor Points of Muscle on the Anterior Aspect of the Lower Extremity Motor Points of Muscle on the Posterior Aspect of the Lower Extremity 18. Flexor and Opponence Digiti Minimi 19. Lumbricals 1. Deltoid Medial Head 2. Deltoid Posterior Head 3. Deltoid Lateral Head 4. Triceps Long Head 5. Triceps Medial Head 6. Extensor Carpi Radialis Longus 7. Extensor Carpi Radialis Brevis 8. Extensor Digitorum 9. Supinator 10. Extensor Carpi Ulnaris 11. Extensor Digiti Minimi 12. Abductor Policis Brevis and Extensor Policis Brevis 13, Extensor Policis Longus 1. Trapezius Upper Fibers 2. Supra Spinatus 3. Rhomboidus 4. Infraspinatus 5. Teris Major and Minor 6. Latissimus Dorsi 7. Trapezius Lower Fibers 1. Rectus Femoris 2. Vastus Lateralis 3. Vastus Medialis 4. Tibialis Anterior 5. Peroneous Longus 6. Extensor Digitonum Brevvis 7. Peroneous Brevis 8. Extensor Hallucis Longus 9. Extensor Digitorum Brevis 10. Abductor Hallucis Longus 1. Biceps Femoris 2. Semimembranous and Semitendinosus 3. Gastrocnemius Lateral Head 6|Page 4. Gastrocnemius Medial Head 5. Soleus 6. Flexor Digitorum Longus 7. Flexor Hallcis Longus 8. Tibiolis Posterior result in greater depth of penetration than narrower (B). Which Color Wire Should I Use Where? • Left Pic: Electrodes should be positioned over the muscle tissue to be stimulated. Placement of electrodes distal to the muscle fibers (A) results in stimulation over areas without muscle tissue and may be uncomfortable or result in lesser response from the muscle. Placement over more muscular tissue (B) results in a more robust response Right Pic: The interelectrode distance will affect the depth of current penetration. Wider placements (A) will The lead wires of many electrotherapy devices are manufactured with red & black ends. Many clinicians assume this indicates the positive and negative leads, respectively. However, with currents that continually change direction, such as AC and biphasic currents, the polarity is continually changing, so the red and black lead is neither the anode nor the cathode for more than the duration of a single phase of a biphasic pulse (i.e., microseconds). Only when using DC, monophasic pulsed current, or unbalanced asymmetrical pulsed current would the red and black truly indicate an anode and cathode. Name Monopolar Electrode Location Active electrode of single circuit over target area; inactive over nearby nontreatment area Common Use Pain modulation, iontophoresis, tissue healing 7|Page Bipolar Quadripolar Both or all electrodes of single circuit over target tissues Four electrodes of two circuits over target tissues Muscle activation, pain modulation Pain modulation Patient Positioning • JOINT crossed by the stimulated ms must be in MIDRANGE. = allows patient to perform a strong isometric contraction Pulse Duration • • • Innervated ms: 150-350 us to stimulate motor nerves Smaller ms → Shorter p.d. (150-200 us) Larger ms → Longer p.d. (200-350 us) Small people / Children = Shorter p.d. If SHORTENED PULSE DURATION → HIGHER AMPLITUDE current will be required to achieve the same strength of contraction produced by a longer pulse duration On:Off Time • • • Selection of ideal combination of p.d. and current amp should be based on patient’s comfort & achievement of the desired outcome Allows muscle to contract & relax → limits fatigue STRENGTHENING o ON-time = 6 – 10 secs o OFF-time = 50 – 120 secs o Initial ON:OFF ratio = 1:5 o Progressed ratio = 1:4 or 1:3 RELAXATION / RELIEVE SPASM & EDEMA muscle o ON-time: 2-5 secs o OFF-time: 2-5 secs o ON:OFF ratio: 1:1 Ramp Time Frequency: • • • • • Determines type of response or ms contraction As frequency increases, twitches will occur more closely together → will produce smooth tetanic contraction (35-50 pps) Beyond 50-80 pps → greater muscle strengthening → More rapid fatigue during repeated stimulation Recommended Frequency (clinical): 35 – 50 pps Low Frequency: 20-30 pps better tolerated for smaller ms (face, distal UE & all ms in young children) • • • • Allows gradual increase & decrease of force To facilitate repetitive exercise &/ or ON-time is 6-10 secs → RAMP UP/DOWN time = 1-4 secs Activities that require rapid contraction & relaxation of ms, RAMP TIME SHOULD NOT BE USED When contraction of Antagonist to a spastic ms is stimulated in a pt with CVA/stroke → LONG RAMP TIME = 4-8 secs (avoids SPASTICITY) 8|Page Current Amplitude (Intensity) • • • • Where the strength of contraction produced depends the most Ms STRENGTHENING: o until contraction of desired strength o o Uninjured = at least 50% of MVIC strength o Recovery from injury/surgery = ≥ 10% of MVIC of uninjured limb ** stronger contractions are likely to be more effective Motor ReEducation = (BEST) LOWEST Current Amp to produce the desired fxnal mvmt ** Goal: functional mvmt that may not require max strength ** ES can assist c functional recovery by providing sensory input, proprioceptive feedback of (N) motion, & inc ms strength Reduce Ms Spasm / Pump out Edema = Sufficient enough to produce a visible contraction Treatment Time • • Parameters for NMES and FES Muscle Strengthening = 10 – 20 contractions > 10 mins o repeat multiple times a day if patient has device at home done only ONCE each visit Motor ReEducation = at most 20 mins o <20 mins if patient is inattentive or fatigued 9|Page PARAMETERS FOR DENERVATED MUSCLE EMS Parameters Typically Used for Stimulating Denervated Muscle Waveform Pulse Duration Frequency Amplitude Ramp-up time Ramp-down time Duty cycle Treatment time and duration Monophasic or DC 1-450 msec (long) 1-500 pps To obtain contraction but low to prevent burns Not identified Not indentified Highly variable 30 minutes, 8 hours per day 5-7 days per week 4 days to 4 years DOCUMENTATION • • • • • • Area to be treated Patient positioning Specific Stimulation Parameters Electrode Placement Tx Duration Patient response to tx ** Include Current Amplitude NMES on R Biceps x 10 mins Ambulation inside // bars: FES on R Ankle DFs during swing phase x 10:50 secs on:off time x 2 secs Ramp x 5 rounds Bells Palsy: ES on R Facial Motor Points x 30 contractions each x 2 sets 10 | P a g e • • Doesn’t deliver current; Electrical activity generated by ms contraction is detected Not generally considered as an electrotherapeutic agent EMG Biofeedback Criteria of use: 1. 2. 3. 4. No visual problem No comprehension/communication problem Good motor control No profound sensory loss Contraindication: • • Any condition where ms contraction is detrimental Skin irritation at electrode site ELECTROMYOGRAPHIC EMG BIOFEEDBACK • • • • EMG: Record of the electrical activity of muscles using surface or fine wire/needle electrodes • BIOFEEDBACK: Technique of making unconscious or involuntary body processes perceptible to the senses to manipulate them by conscious mental control. Use of appropriate instrumentation to bring covert-physiologic process to the awareness of one or more individual Used to transduce ms potentials into auditory or visual cues for the purpose of increasing / decreasing voluntary activity Clinical Examples of Facilitatory and Inhibitory Biofeedback Facilitatory • • To increase muscle activity after surgery or injury when volitional recruitment is impaired To normalize the balance of muscles acting at a joint where one muscle group may be insufficient 11 | P a g e • • Inhibitory • • • To improve volitional motor control following dysfunction of the CNS To increase volitional control of pelvic floor muscles for rehabilitation of urinary incontinence To help decrease activity in muscle demonstrating spasticity caused by dysfunction of the CNS To help decrease activity in muscle demonstrating increased activity caused by postural stress or anxiety To help decrease muscle activity associated with chronic pain EMG BIOFEEDBACK Electrodes close together = minimize cross talk, yield small signals, more precise signals farther apart = yields large signal, detection from more than 1 muscle 12 | P a g e