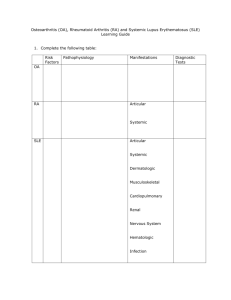
SYSTEMIC AND DISSEMINATED LUPUS ERYTHEMATOSUS HAEMATOLOGY PRESENTATION PRESENTED BY: S. MA. LYDIA YAA SARPONG,RVM REFERENCES: Haematology by: Rodak et Al : Henry's Clinical Diagnostics : Center For Disease Control Journal : Google Images MARCH 17, 2022 Clinical Presentation SYSTEMIC AND DISSEMINATED LUPUS ERYTHEMATOSUS OBJECTIVES At the end of the Presentation: We will be able to;1. Describe the etiology, pathogenesis and pathophysiology of SLE. 2. Correlate Laboratory Diagnosis with Clinical Symptoms. 3. Analyze the impact of SLE on an Individual, Environment and System. …… Cognitively, affectively and Practically…. SYSTEMIC LUPUS ERYTHEMATOSUS (SLE) DISSEMINATED LUPUS ERYTHEMATOSUS (DLE) AUTOIMMUNE DISEASE AUTOIMMUNE DISEASE …Immune System Attacks its own tissues… 1. Inflammation 2. Tissue damage in organs …… NOTE: There is no cure, only medical interventions…… SYSTEMIC LUPUS ERYTHEMATOSUS (SLE) Chronic autoimmune inflammatory disease manifested by severe vasculitis, renal involvement, and lesions of the skin and nervous system. …… NOTE: There is no cure, only medical interventions…… DISSEMINATED LUPUS ERYTHEMATOSUS (DLE) Is a distinctive cutaneous eruption forming part of a systemic disorder that usually includes also characteristic clinical and anatomic evidence of visceral damage. ETIOLOGY (CAUSES )- UNKNOWN PATHOGENESIS PATHOPHYSIOLOGY OF SIGNS AND SYMPTOMS ●FLARE ●REMISSION SIGNS AND SYMPTOMS (Malar rash) COMPLICATIONS ● Poor access to care ● Late diagnosis ● Less effective treatments ● Poor adherence to therapeutic regimes (eg.Pregnancy= "HIGH RISK PREGNANCY") DIAGNOSIS ● Symptoms assessments ● Physical Examination ● X-rays ● Laboratory Tests *****Rheumatologist ***** LABORATORY ASSESSMENT ● Hematology assessments A. Hemolytic Anemia with reticulocytosis. B. Leukopenia,Lymphopenia,Thrombocytopenia . LABORATORY ASSESSMENT ● Hematology assessments ● Thrombocytopenia also is noted in 14% to 26% of patients with systemic lupus erythematosus. ● NOTE:- (The diagnosis of ITP or systemic lupus erythematosus in the mother is a prerequisite for the diagnosis of neonatal autoimmune thrombocytopenia. Neonatal autoimmune thrombocytopenia is due to passive transplacental transfer of antibodies from a mother with ITP or, occasionally, systemic lupus erythematosus). LABORATORY ASSESSMENT ● Hematology assessments A. Presence of LE cells in serous fluids. LABORATORY ASSESSMENT ● Renal Disorder • Persistent Proeteinurea • Cellular Casts (Red cell, hemoglobin, granular, tubular or mixed) FINE CASTS IN THE URINE COARSE LABORATORY ASSESSMENT ● Immunologic • Anti-DNA • Anti-Sm • Positive Antiphospholipid antibodies (IgG or IgM anticardiolipin antibodies, Positive test for Lupus anticoagulant, false positive Treponemal antibody test. • Positive ANA(antinuclear antibody) LABORATORY ASSESSMENT ● 50% of patients with systemic lupus erythematosus have autoimmune APL antibodies. LABORATORY ASSESSMENT Immunologic ● Lupus anticoagulant • The two most commonly recommended test systems are the dilute Russell viper venom time (DRVVT) and the silica-based partial thromboplastin time (PTT) • Two older systems:- kaolin clotting time (KCT) and the dilute thromboplastin time (DTT, also named tissue thromboplastin inhibitor test, TTI) LABORATORY ASSESSMENT Immunologic ● Lupus anticoagulant • Lupus anticoagulant (LA, LAC) Autoantibody to phospholipidbinding proteins such as b2-glycoprotein I, annexin, and prothrombin. May be present as a primary condition or secondary to a collagen disorder such as systemic lupus erythematosus, Sjögren syndrome, or rheumatoid arthritis. • Chronic lupus anticoagulant is associated with venous and arterial thrombosis and spontaneous abortion. ● Women Risk ● Africans /African Americans ● Asians ● Hispanics ● Indians Societal concern ● Women ● Pregnant women ● Weakness ● Other painful episodes ● Laboratory worker SUMMARY CBC • Finding leukopenia and/or thrombocytopenia in idiopathic vasculitides is rare and suggests alternative diagnoses such as systemic lupus erythematosus (SLE), neoplasm, bone marrow disorders, lympho- matoid granulomatosis, or hypersplenism (Mandell, 1994). • Leukocyte counts greater than 10,000/μL, and often greater than 50,000/μL, are characteristic of crystalinduced arthritis (e.g., gout, pseu dogout), chronic in ammatory arthritis (e.g., rheumatoid arthritis, sys temic lupus erythematosus, ankylosing spondylitis), and septic arthritis (Kjeldsberg, 1993) RESEARCH JOURNALS TIP-BITS DIAGNOSTICALLY • The 1982 revised criteria for classification of SLE included 11 categories, adding (1) abnormal titer of antinuclear antibody by immunofluorescence or an equivalent assay, and (2) antibody to native DNA and/or Sm antigen. In contrast to the 1971 criteria, the 1982 criteria removed Raynaud’s phenomenon and alopecia because of their lack of sensitivity and specificity. • The presence of antinuclear antibodies was detected in female laboratory workers with varying degrees of exposure to blood SUMMARY • An autoimmune disease of concern since etiology is not known. • Proper Laboratory investigations ought to be done to help with early diagnosis to avoid complications especially in pregnant women. • Laboratory professionals among many others are at risk.