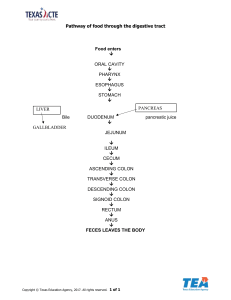
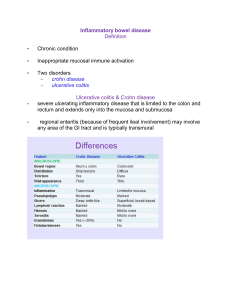
Inflammatory Bowel Disease IBD: ch. condition resulting from inappropriate mucosal immune activation. 2 disorders: Crohn disease & ulcerative colitis. Commensal bacteria normally present in intestinal lumen probably involved in IBD pathogenesis, distinction is based on distribution of affected sites & morphologic expression of disease at those sites. UC: severe ulcerating inflam. disease limited to colon & rectum, extends only into mucosa & submucosa. CD, referred to as regional enteritis (frequent ileal involvement) may involve any area of GI tract & is typically transmural. Pathogenesis Most investigators believe the 2 diseases result from combination of defects in host interactions with intestinal microbiota, intestinal epithelial dysfunction, aberrant mucosal immune responses. This supported by epidemiologic, genetic, clinical studies & data from laboratory models of IBD I- Genetics: Risk of disease increased when there is an affected family member & in CD,concordance rate for monozygotic twins is 50%, UC only 16% Molecular linkage analyses of affected families have identified NOD2 (nucleotide oligomerization binding domain 2) as a susceptibility gene in CD. NOD2 encodes a protein binds to intracellular bacterial peptidoglycans & activates NF-κB. It has been postulated that disease-associated NOD2 variants are less effective at recognizing & combating luminal microbes, which enter lamina propria & trigger inflam. reactions II- Mucosal immune responses: immunosuppression remains mainstay of IBD therapy. Polarization of helper T cells to e TH1 type in CD & emerging data suggest TH17 T cells. Certain polymorphisms of IL-23 receptor confer protection from CD & UC IL-23 is involved in development & maintenance of TH17 cells Epithelial defects: variety of epithileal defects described in both CD & UC. Ex, defects in intestinal epith. tight junction barrier function present in CD pt.s & subset of their healthy first-degree relatives. Microbiota: abundance of microbiota in GI lumen is overwhelming, amounting 1012 organisms / ml in colon & 50% of fecal mass. Antibodies against bacterial protein flagellin are associated with NOD2 polymorphisms, stricture formation, perforation, small-bowel involvement in pt.s with CD, but uncommon in UC Some antibiotics, e.g. metronidazole, can be helpful in management of CD CROHN DISEASE Eponym based on 1932 description by Crohn, Ginzburg, Oppenheimer, has existed for centuries. Louis XIII of France (1601–1643) suffered relapsing bloody diarrhea, fever, rectal abscess, small intestinal and colonic ulcers and fistulae beginning at age 20 years, most likely due to Crohn disease. Morphology CD may occur in any area of GIT, but the most common sites involved at presentation: terminal ileum, ileocecal valve, cecum. Disease is limited to small intestine alone in 40% of cases; small intestine & colon both involved in 30% of pts; remainder have only colonic involvement. Presence of multiple, separate, sharply delineated areas of disease, resulting in skip lesions characteristic of CD & may help diff. from UC Strictures are common Earliest lesion “aphthous ulcer” may progress & multiple lesions often coalesce into elongated, serpentine ulcers oriented along axis of bowel. Edema & loss of normal mucosal texture Sparing of interspersed mucosa Patchy distribution results in a coarsely textured, cobblestone appearance in which diseased tissue is depressed below level of normal mucosa. Fissures develop between mucosal folds extend deeply to become fistula tracts or sites of perforation. Intestinal wall is thickened & rubbery as consequence of transmural edema, inflam., submucosal fibrosis, hypertrophy of muscularis propria, all of which contribute to stricture formation. With extensive transmural disease, mesenteric fat frequently extends around serosal surface (creeping fat) Microscopic Active CD: abundant neutrophils infiltrate & damage crypt epithelium. Clusters of neutrophils within a crypt are referred to as crypt abscesses & ass. with crypt destruction. Ulceration is common in CD & there may be abrupt transition between ulcerated & adjacent normal mucosa. Repeated cycles of crypt destruction & regeneration lead to distortion of mucosal architecture Epith. metaplasia takes form of gastric antralappearing glands “pseudopyloric metaplasia”. Paneth cell metaplasia may also occur in Ltcolon, where Paneth cells are normally absent Architectural & metaplastic changes may persist even when active inflam. has resolved. Mucosal atrophy, with loss of crypts, may occur after years of disease. Non-caseating granulomas, hallmark of CD, found in 35% of cases & may occur in areas of active disease or uninvolved regions in any layer of intestinal wall . Granulomas may also be present in mesenteric LNs. Cutaneous granulomas form nodules that are referred to as metastatic Crohn disease. The absence of granulomas does not preclude a diagnosis of Crohn disease. Clinical Features Extremely variable. Disease begins with intermittent attacks of relatively mild diarrhea, fever, abd pain. 20% of pt.s present acutely with Rt. lower quadrant pain, fever, bloody diarrhea that mimic acute appendicitis or bowel perforation. Periods of active disease are typically interrupted by asymptomatic periods last for weeks to many months. Disease re-activation can be ass. with variety of external triggers “physical or emotional stress, specific dietary items, cigarette smoking”. The latter is a strong exogenous risk factor for development of CD, in some cases, disease onset is associated with initiation of smoking. Unfortunately, smoking cessation does not result in disease remission. ULCERATIVE COLITIS Closely related to CD but intestinal disease in UC is limited to colon & rectum. Common extra-intestinal manifestations of UC overlap with those of CD & include migratory polyarthritis, sacroiliitis, ankylosing spondylitis, uveitis, skin lesions, pericholangitis, primary sclerosing cholangitis. Long-term for UC pt.s depends on severity of active disease & disease duration Morphology Always involves rectum & extends proximally in continuous fashion to involve part or all of colon. Skip lesions are not seen Disease of entire colon is termed “pancolitis” while Lt-sided disease extends to only transverse colon Limited distal disease “ulcerative proctitis” or “ulcerative proctosigmoiditis” Small intestine: normal, although mild mucosal inflam. of distal ileum, backwash ileitis, may be present in severe cases of pancolitis. Involved colonic mucosa: red & granular or have extensive, broad-based ulcers There can be abrupt transition between diseased & uninvolved colon Ulcers are aligned along long axis of colon but do not typically replicate the serpentine ulcers of CD Isolated islands of regenerating mucosa often bulge into lumen to create pseudopolyps & tips of polyps may fuse to create mucosal bridges Ch. disease may lead to mucosal atrophy with flat & smooth mucosal surface that lacks normal folds. Unlike CD, mural thickening is not present, serosal surface is normal, no strictures. Inflammation & inflam. mediators can damage muscularis propria & disturb neuromuscular function leading to colonic dilation & toxic megacolon, which carries significant risk of perforation Microscopically Mucosal disease in UC are similar to colonic CD Include inflam. infiltrates, crypt abscesses, architectural crypt distortion, epith. metaplasia Inflam. process is diffuse & limited to mucosa & superficial submucosa Severe cases: extensive mucosal destruction may be accompanied by ulcers that extend more deeply into submucosa Submucosal fibrosis, mucosal atrophy, distorted mucosal architecture remain as residua of healed disease but histology may also revert to near normal after prolonged remission. Granulomas are not present in UC Clinical Features Is relapsing disorder characterized by attacks of bloody diarrhea with stringy, mucoid material, lower abd. pain, cramps that are temporarily relieved by defecation. Symptoms may persist for days, weeks or months before they subside Colectomy effectively cures intestinal disease in UC but extra-intestinal manifestations may persist Trigger may be infectious, psychologic stress, shortly after smoking cessation in some pt.s Feature Crohn Disease Ulcerative Colitis MACROSCOPIC Bowel region Ileum ± colon Colon only Distribution Skip lesions Diffuse Stricture Yes Rare Wall appearance Thick Thin MICROSCOPIC Crohn Disease Ulcerative Colitis Inflammation Transmural Limited to mucosa Pseudopolyps Moderate Marked Ulcers Deep, knife-like Lymphoid reaction Marked Superficial, broadbased Moderate Fibrosis Marked Mild to none Serositis Marked Mild to none Granulomas Yes (∼35%) No Fistulae/sinuses Yes No CLINICAL Crohn Disease Perianal fistula Yes (in colonic disease) Yes Fat/vitamin malabsorption Malignant potential Recurrence after surgery Toxic megacolon Ulcerative Colitis No No With colonic involvement Common Yes No Yes No Note: All features may not be present in a single case Idiopathic inflammatory bowel disease Crohn disease Small bowel and colon (mostly right side) Patchy involvement Transmural inflammation, fistulas, strictures, serositis Non-caseating granulomas Poor response to surgery Increased risk for cancer Ulcerative colitis Colon only Continuous involvement Superficial inflammation No granulomas Good response to surgery Increased risk for cancer IBD DIFFERENCES CROHN – – – – – – – TRANSMURAL, THICK WALL NOT LIMITED to COLON GRANULOMAS FISTULAE COMMON TERMINAL ILEUM OFTEN SKIP AREAS “CRYPT” ABSCESSES NOT COMMON – NO PSEUDOPOLYPS – MALABSORPTION ULCERATIVE – – – – – – – – – MUCOSAL, THICK MUCOSA LIMITED to COLON NO GRANULOMAS FISTULAE RARE TERMINAL ILEUM NEVER NO SKIP AREAS “CRYPT” ABSCESSES COMMON PSEUDOPOLYPS NO MALABSORPTION