Anxiolytics and Hypnotics: Mechanisms, Effects, and Agents
advertisement

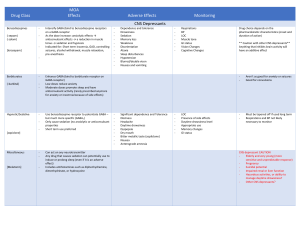
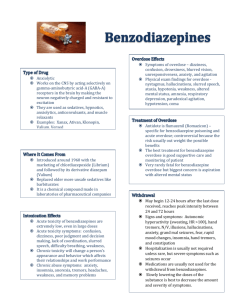
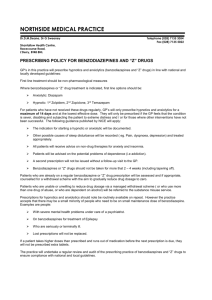
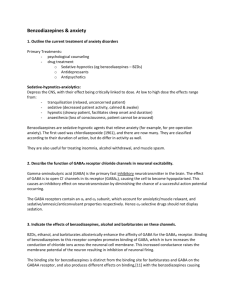
Anxiolytics and Hypnotics : Anxiety • It is an unpleasant state of tension, apprehension or uneasiness-a fear that seems to arise from an unknown source. • The symptoms of severe anxiety are similar to those of fear such as: • Tachycardia • Sweating • Trembling • Palpitation. • Symptoms of severe and chronic anxiety , may be treated with anti-anxiety drugs sometimes called anxiolytics. Classification of Hypnotics, Anxiolytics •Benzodiazepines: Alprazolam Clonazepam Lorazepam Diazepam Flurazepam Benzodiazepine antagonists Flumazenil Other Anxiolitic drugs: Buspirone Antidepressants Barbiturates Amobarbital Phenobarbital Pentobarbital Thiopental Non-barbiturate Anti-histamines Doxepin General Definitions •Sedative: Calm down, treat agitation •Hypnotic: Induce sleep –go to sleep fast, feel refreshed tomorrow !!! •Anxiolytic: Reduce anxiety – physical, emotional, cognitive Benzodiazepines (BZD): • Benzodiazepines are the most widely used anxiolytic drugs. They have largely replaced barbiturates in the treatment of anxiety, because benzodiazepines are safer and more effective. Mechanism of Action • The targets for benzodiazepine actions are the γaminobutyric acid (GABAA ) receptors. [Note: GABA is the major inhibitory neurotransmitter in the central nervous system (CNS).] These receptors are primarily composed of α, β, and γ subunit .Benzodiazepines modulate GABA effects by binding to a specific, high-affinity site located at the interface of the α subunit and the γ2 subunit. • The benzodiazepine receptor locations in the CNS parallel those of the GABA neurons. Binding of GABA to its receptor triggers an opening of a chloride channel, which leads to an increase in chloride conductance. Benzodiazepines increase the frequency of channel openings produced by GABA. The influx of chloride ions causes a small hyperpolarization that moves the postsynaptic potential away from its firing threshold and, thus, inhibits the formation of action potentials. Therapeutic Effects Sedative, Hypnotic, Anticonvulsant, Muscle-Relaxant. Anxiety disorder. Adverse Effects • Sedation, • CNS Depression • Behavioral Disturbance – – – – – Irritability, excitement, aggression coordination, attention (driving) poor visual-spatial ability Ataxia, confusion Drowziness • Overdose: Rare fatalities if BZD alone • Severe CNS & Respiratory Depression if combined with: – – – – alcohol barbiturates narcotics tricyclic antidepressants BENZODIAZEPINE ANTAGONIST • Flumazenil is a GABA-receptor antagonist that can rapidly reverse the effects of benzodiazepines. The drug is available for intravenous (IV) administration only. Onset is rapid, but duration is short, with a half life of about 1 hour. Frequent administration may be necessary to maintain reversal of a long-acting benzodiazepine. Administration of flumazenil may precipitate withdrawal . • Dizziness, nausea, vomiting, and agitation are the most common side effects. OTHER ANXIOLYTIC AGENTS • 1) Antidepressants • Selective serotonin reuptake inhibitors may be used alone, or prescribed in combination with a low dose of a benzodiazepine during the first weeks of treatment. After four to six weeks, when the antidepressant begins to produce an anxiolytic effect, the benzodiazepine dose can be tapered. SSRIs have a lower potential for physical dependence than the benzodiazepines, and have become first-line treatment for GAD. While only certain SSRIs have been approved by the FDA for the treatment of GAD, the efficacy of these drugs for GAD is most likely a class effect. Thus, the choice among these antidepressants can be based upon side effects and cost. Long-term use of antidepressants and benzodiazepines for anxiety disorders is often required to maintain ongoing benefit and prevent relapse. • 2) Buspirone • Buspirone is useful for the chronic treatment of GAD and has an efficacy comparable to that of the benzodiazepines. This agent is not effective for short-term or “as-needed” treatment of acute anxiety states. The actions of buspirone appear to be mediated by serotonin (5-HT1A) receptors, although other receptors could be involved, because buspirone displays some affinity for DA2 dopamine receptors and 5-HT2A serotonin receptors. Thus, its mode of action differs from that of the benzodiazepines. • The frequency of adverse effects is low, with the most common effects being headaches, dizziness, nervousness, and light-headedness. Barbiturates •All derivatives of Barbituric acid •Depressants of the central nervous system (CNS) that impair or reduce the activity of the brain by acting as a Gamma Amino Butyric Acid (GABA) potentiators •Categorized as hypnotics and also called “downers” •Produce alcohol like symptoms such as impaired motor control (ataxia), dizziness, and slower breathing and heart rate Barbiturates • • • • • Amobarbital Pentobarbital Secobarbital Phenobarbitol Thiopental Mechanism of Action Barbiturates potentiate the effect of GABA at the GABA-A receptor. The GABA-A receptor is a ligand gated ion channel membrane receptor that allows for the flow of Cl through the membrane in neurons. GABA is the principle neurotransmitter for this receptor which upon binding causes the channel to open and creates a negative change in the transmembrane potential. This makes it an Inhibitory neurotransmitter GABA binding site Barbiturate binding site Mechanism of Action Facilitation of GABA action on the brain. increase the duration of the GABA gated channel opening but in large dose, they can directly activating chloride channels. Pharmacological Actions: • Depression of CNS At low doses produce sedation At high doses drugs causes hypnosis, followed by anesthesia and finally coma and death. • Respiratory depression • Enzyme induction: induce P450 microsomal enzyme in liver. Adverse effects •Drowsiness •Impaired concentration •Mental and physical sluggishness •Hypnotic doses produces feeling of tiredness after wake. •Impaired ability to function normally •Nausea •Dizziness Non- barbiturate sedatives ANTIHISTAMINES antihistamine with sedating properties such as diphenhydramine and doxylamine are effective in treating mild type of insomnia. They have numerous undesirable side effects make them less useful. Zolpidem: • This hypnotic drug is not structurally related to benzodiazepine but it selectively bind to the benzodiazepine receptor . • It is rapidly absorbed from the GIT & its onset of action is rapid & short elimination half life. • Adverse effects: nightmares, agitation, headache, GI upset, dizziness