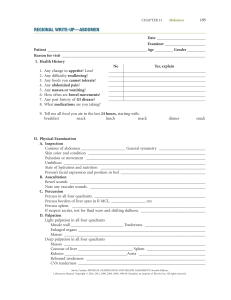
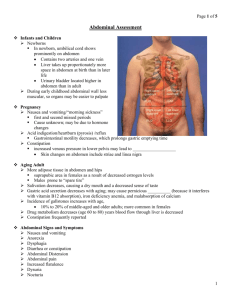
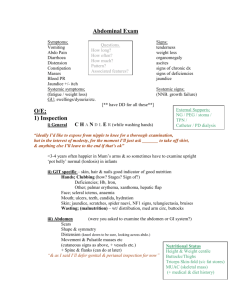
ABDOMINAL ASSESSMENT Abdomen Preps the Patient for Abdominal Exam Patient lying supine, no higher than HOB up 30 degrees Expose the abdomen area without exposing breasts or genital area Stands on right side of patient during exam Completes auscultation before percussion & palpation Completes light palpation of all 4 quadrants before completing deep palpation. Inspection Skin Contour Surface should be smooth and even with homogenous color. Skin can have redness from inflammation, jaundice, skin glistening and taut with ascites. Also, can have striae (linear jagged marks from excessive weight gain/pregnancy) Stand on the person's right side and look down on the abdomen. Then stoop or sit to gaze across the abdomen. Your head should be slightly higher than the abdomen. Determine the profile from the rib margin to the pubic bone. The contour describes the nutritional state and normally ranges from flat to rounded Movement Hernias The abdomen shows respiratory movement. The only other abdominal movement you should note is occasional peristalsis, which may be visible because of the thin musculature. Ask patient to bear down to induce the intestines pushing through abdominal wall. Skin is smooth and even in color with no lesions Contour can be flat, rounded, scaphoid (caved in), and protuberant (distended) Bulges indicate an abdominal hernia: ventral, umbilical, inguinal, or femoral. Auscultate for Bowel sounds Normal bowel sounds are high-pitched, gurgling, cascading sounds, occurring irregularly anywhere from 5 to 30 times per minute. Judge if sounds are present, hypoactive (absent like), or hyperactive (loud, high pitched). One type of hyperactive sound is borborygmus. Percuss to identify Organ size/ enlargement Masses Percuss using indirect method; begin RLQ and precede clockwise, percussing about 3 areas in each quadrant to cover entire abdomen. Note sounds/tone (tympany and dullness) & where heard. What would you normally expect, where? How would you know if your patient has a mass or organ enlargement? Tympany is heard over the stomach, dullness occurs over a distended bladder, adipose tissue, fluid, or a mass, and Hyperresonance is present with gaseous distention Palpate Light Palpation (1 cm) Tenderness Muscle guarding and rigidity Mild tenderness normally is present when With the first four fingers close together, palpating the sigmoid colon in the left lower depress the skin about 1 cm and assess if quadrant patient has tenderness or not. Tenderness occurs with local inflammation Voluntary guarding occurs when the person is cold, tense, or ticklish. It is bilateral, and you will feel the muscles relax slightly during exhalation (use relaxation measures). Involuntary rigidity is a constant, board like hardness of the muscles. It is a protective mechanism accompanying acute inflammation of the peritoneum. Can be unilateral and hurts to sit up. Masses By making a gentle rotary motion, assess if there are bulging spots or masses in the 4 quadrants of the abdomen. Note location, size, shape, consistency, surface, mobility, pulsatility and tenderness. Deep Palpation (5 – 8 cm) Masses Using the first 4 fingers, depress skin 5-8cm. If you identify a mass, first distinguish it from a normally palpable structure or an enlarged organ. Then note location, size, shape, consistency, surface, mobility, pulsatility and tenderness. Liver or organ Begin with liver in RUQ by placing your left enlargement hand under the person's back parallel to the 11th and 12th ribs and lift to support the abdominal contents. Place your right hand on the RUQ, with fingers parallel to the midline. Push deeply down and under the right costal margin. Ask the person to breathe slowly. Bladder distention Femoral Pulses May go over patient’s cloths for this performance exam purposes but must identify correct landmark. Any distention? Grade pulses on 0 – 3 + scale; May go over patient’s shorts for performance exam but must identify correct landmark. Often, the liver is not palpable nor firm.