Page 1 of 5
Abdominal Assessment
Infants and Children
Newborns
In newborn, umbilical cord shows
prominently on abdomen
Contains two arteries and one vein
Liver takes up proportionately more
space in abdomen at birth than in later
life
Urinary bladder located higher in
abdomen than in adult
During early childhood abdominal wall less
muscular, so organs may be easier to palpate
Pregnancy
Nausea and vomiting/“morning sickness”
first and second missed periods
Cause unknown; may be due to hormone
changes
Acid indigestion/heartburn (pyrosis) /reflux
Gastrointestinal motility decreases, which prolongs gastric emptying time
Constipation
increased venous pressure in lower pelvis may lead to ___________________
Skin changes on abdomen include striae and linea nigra
Aging Adult
More adipose tissue in abdomen and hips
suprapubic area in females as a result of decreased estrogen levels
Males prone to “spare tire”
Salivation decreases, causing a dry mouth and a decreased sense of taste
Gastric acid secretion decreases with aging; may cause pernicious __________ (because it interferes
with vitamin B12 absorption), iron deficiency anemia, and malabsorption of calcium
Incidence of gallstones increases with age,
10% to 20% of middle-aged and older adults; more common in females
Drug metabolism decreases (age 60 to 80) years blood flow through liver is decreased
Constipation frequently reported
Abdominal Signs and Symptoms
Nausea and vomiting
Anorexia
Dysphagia
Diarrhea or constipation
Abdominal Distension
Abdominal pain
Increased flatulence
Dysuria
Nocturia
1
Page 2 of 5
Dysguesia
Lactose Intolerance
Lactase is digestive enzyme necessary for absorption of carbohydrate lactose (milk sugar)
abdominal pain, bloating, and flatulence when milk products are consumed
Incidence of lactose intolerance is
70% to 90% in African Americans, American Indians, Asians, and Mediterranean groups
15% in Europeans and Americans
Referred Pain
Upper GI
Patient may complain of “ heart pain” or “chest pain”
May point to or describe substernal area
Lower GI
Intestinal blockage – constipation
Appendicitis – radiating pain from RLQ to umbilicus
Liver
Upper right quadrant and right shoulder
Subjective Questioning and ROS
GI
nausea, vomiting, diarrhea, hepatitis, peptic ulcers, gallstones, gastroesphageal reflux, or loss of
appetite
GU
changes in color, dysuria, hesitancy, urgency, frequency, nocturia, incontinence, polyuria, dribbling,
loose of force of stream, kidney stones, flank pain, testicular and penile pain, penile discharge,
enlarged prostate, emissions, and hernias.
GYN
pain during intercourse, vaginal drainage, odor
Medical History
Abdomen specific
acute or chronic disease processes of the stomach, intestines, kidneys, liver, spleen, uterus, prostate,
etc.
Nonabdomen specific
CHF (ascites), cancer (possible metastases), fibromyalgia (possible IBS), pituitary disorders
(adrenal, polycystic ovaries), alcoholism (hepatitis), spinal cord damage (constipation, dysphagia),
diabetes (kidney dysfunction).
Surgical
GI, reproductive, urinary procedures
N/V,D/C due to medication sensitivities
GI procedures
Injuries/accidents
Trauma, PID, peritonitis, ruptured appendix
Family health history
Cancers (stomach, pancreas, liver, kidney, colon), PUD, DM, polyps, IBS, colitis, malabsorption
(celiac)
Social history
alcohol (malabsorption), cirrhosis, upper/lower GI bleeding
2
Page 3 of 5
Allergies
Health maintenance activities
Medications:
Histamine: two antagonists
Antibiotics
Lactulose
Antacids
Antiemetics, Antidiarrheals
Laxatives or stool softeners
Pancreatic enzymes
Steroids
Chemotherapeutics
Antiflatulents
Alcohol use
Drug use
Travel history
Work environment
Stress
Physical Assessment
Sequence of Steps
Inspection
__________________
Percussion
___________________
Empty Bladder
Supine
Arms at side
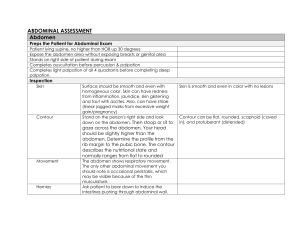
Characteristics Determined by Inspection
Contour
Flat
Round
Scaphoid
Protuberant
Symmetry
Rectus abdominis muscles
Pigmentation and color
Scars
_____________________
Respiratory movement
Masses or nodules
Visible peristalsis
Pulsation
Umbilicus
Inspection: 7 F’s of Abdominal Distension
1. Fat
2. Fluid (______________)
3
Page 4 of 5
3.
4.
5.
6.
7.
Flatus
Feces
Fetus
Fatal growth (malignancy)
Fibroid tumor
Auscultation
Assess all four quadrants
Listen for at least ____________ before concluding bowel sounds are absent
Hypoactive
Hyperactive
Normal findings
Bowel sounds are heard in all quadrants
Usually sounds are high pitched
Occur 5 to 30 times per minute
Bell
Low pitch
Vascular Sounds
Diaphragm
Hi pitch
Gastric Sounds
Palpation- Normal Findings
Light vs. Deep
Light: ½ inch
Deep: 1-3 inches
Palpate all quadrants
One-handed method
Bimanual method
Do not palpate a rigid abdomen
Normal findings
No tenderness
Abdomen feels soft
No muscle guarding
No masses or organomegaly
No bladder distension
Aorta <3 cm, if palpated
Palpation – Abnormal Findings
Rigidity
Tenderness on palpation
Muscle guarding on expiration
Presence of masses, bulges, or swelling
__________________________
At a site away from tenderness, press down perpendicular to abdomen. Push down slow, lift up fast.
Causes structures to rebound. Negative = no pain
Peritoneal inflammation, appendicitis
4
Page 5 of 5
Documentation Example
Abdomen symmetrical and rounded. Color pink with even distribution of pigmentation. No, masses,
pulsations, peristalsis, retractions, or rectus abdominis muscles visible. Positive bowel sounds heard in
all quadrants. No masses, muscle guarding, tenderness upon light palpation. No complaints of pain. --------------------------------------------------------------Sam Smith ADNS Chippewa Valley Technical College
5
 0
0