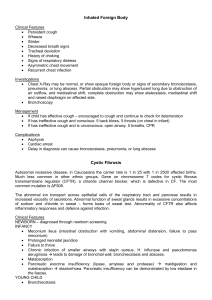
[ Critical Care Research Letters ] Paradoxical Effect of Chest Wall Compression on Respiratory System Compliance A Multicenter Case Series of Patients With ARDS, With Multimodal Assessment Methods Different modalities were used to detect the effect of chest wall compression on changes in: (1) partitioned respiratory mechanics Results Case 1 During patient positioning of a 63-year-old woman (BMI, 28 kg/m2) with severe ARDS on veno-venous extracorporeal membrane oxygenation (San Gerardo Hospital) from semi-recumbent to horizontal, we observed a “paradoxical” (at least toward common expectations) decrease of the driving pressure of the respiratory system (DP,rs) leading to a higher Cpl,rs. Three positions were formally tested: (1) supine (0 ); (2) Trendelenburg (–30 ); and (3) reverse Trendelenburg (30 ). Increased abdominal compression on the lungs in the Trendelenburg position decreased plateau pressure and led to higher Cpl,rs, with a decreased stress index (Fig 1, panel 1). The EIT analysis suggested decreased lung overdistension in the nondependent areas in the Trendelenburg position and greater overdistension in the reverse Trendelenburg position (Fig 1, panel 2). Changes in respiratory mechanics observed during postural changes are described in the Video 1, part 1. Case 2 Chest compression with a 5-kg weight is sometimes used in patients with ARDS to assess respiratory mechanics despite lack of evidence on its benefit.4 chestjournal.org To the Editor: The lungs of patients with ARDS are characterized by marked heterogeneity, resulting in the coexistence of collapsed and hyperinflated tissue.1 Gravitational forces and chest wall geometry help govern the balance between these components.2 In this research letter, we present four cases in which chest wall compression caused an apparently “paradoxical” increase in the compliance of the respiratory system (Cpl,rs), likely explained by reduction of overdistension. using static respiratory maneuvers and an esophageal balloon; (2) distribution of the tidal ventilation and end-expiratory lung volume (EELV) by electrical impedance tomography (EIT)3; and (3) lung aeration by lung CT analysis. We report the effect of a 5-kg bag applied on the chest of a 69-year-old man (BMI, 22.5 kg/m2) admitted to the Neuro-ICU (Niguarda Hospital) with legionellosis causing severe ARDS. We hypothesized that a continuous external weight on the chest might change the mechanical properties of the respiratory system, reducing overdistension of the nondependent lung areas and, in contrast, recruiting the dependent lung areas. We explored this mechanism by EIT.5 We tested three steps, each lasting 10 min: step A, baseline; step B, 5-kg bag continuous compression; and step C, no compression. Compared with baseline, chest weight application led to a sudden improvement of Cpl,rs by reduced DP,rs and reduced end-expiratory lung impedance (EELI), a surrogate of EELV (Fig 2, panel 1). The EELI reduction was localized mainly in the ventral regions (Fig 2, panel 2, solid lines). At the same time, we observed a change in regional tidal volume (TV) distribution from dorsal to ventral lungs, suggesting an increased regional Cpl,rs in nondependent areas (Fig 2, panel 2, dashed lines). In the nondependent lung, we observed an apparently paradoxical behavior: an increased Cpl,rs with a reduction of EELV, which we might interpret as a reduction of regional hyperinflation. In the dependent lung, we observed a decrease in both EELI and regional 1335 1 Paw = 22.8 cmH2O Paw = 26.7 cmH2O Paw = 24.8 cmH2O Stress index < 1 Stress index = 1 Stress index > 1 Reference 2 CW [%] 21 0 7 6 0 12 0 CL [%] 3 LUNGS VOLUME, mL CHEST WALL LUNGS TOTAL VOLUME, mL LUNGS CHEST WALL VOLUME, mL TOTAL Tidal Volume = 180 Tidal Volume = 180 Tidal Volume = 180 CHEST WALL TOTAL a a’ PEEP Pplat PRESSURE, cmH2O Driving Pressure = 12.8 PEEP Pplat PRESSURE, cmH2O PEEP Pplat PRESSURE, cmH2O Driving Pressure = 16.7 Driving Pressure = 14.8 Figure 1 – Case 1. Body positional changes. We positioned the patient as follows: (1) Trendelenburg position (–30 ), left side; (2) supine (0 ), center; and (3) reverse Trendelenburg position (30 ), right side. The ventilator was set as follows: volume-controlled mode with a tidal volume of 180 mL, respiratory rate of 10 breaths/min, FIO2 of 0.65, PEEP of 10 cm H2O, and a Pplat of 25 cm H2O. In the supine position, Pplat was 24.8 cm H2O, leading to a driving pressure of 14.8 cm H2O. The tidal volume was 178 mL, leading to a compliance of the respiratory system (Cpl,rs) of 12 mL/cm H2O. In the Trendelenburg position, driving pressure decreased to 12.8 cm H2O, leading to a Cpl,rs of 14.1 mL/cm H2O. Finally, in a reverse Trendelenburg position, driving pressure increased to 16.7 cm H2O (Cpl,rs ¼ 10.7 mL/cm H2O). Interestingly, the stress index of the airway pressure changed from < 1 to 1 to > 1, moving from the Trendelenburg to 0 to the reverse Trendelenburg position, respectively (panel 1). At electrical impedance tomography evaluation, we observed, compared with the reference (supine positioning [0 ]), a significant improvement of Cpl,rs (CW) in the Trendelenburg position (–30 ), accounting for 21% of decrease of overdistension, with a minimal decrease of Cpl,rs (CL), which suggested 6% of lung de-recruitment. In contrast, in the reverse Trendelenburg position (30 ), we reported a low CW with 7% of lung recruitment, in the presence of a significant CL, which suggested 12% of lung overdistension (panel 2). The change in the mechanical properties of the respiratory system from horizontal to the Trendelenburg position may be suggested by a right-shifting of the pressure-volume curve of the chest wall and, consequently, of the entire respiratory system. Although the global end-expiratory lung volume decreases (from a to a0 , center to the left side), tidal ventilation occurs in a steeper (ie, more compliant) part of the pressure-volume curve, leading to a decreased driving pressure, for the same tidal volume. The opposite happens in the reverse Trendelenburg position, right side (panel 3). CL ¼ compliance “loss”; CW ¼ compliance “win”; Paw ¼ airway pressure; PEEP ¼ positive end-expiratory pressure; Pplat ¼ plateau pressure. TV, suggesting a loss of Cpl,rs likely caused by a certain degree of de-recruitment. Time seems to be a meaningful factor, as the global EELI trend during Step B shows a progressive reduction over time (Fig 2, panel 1). In summary, this case suggests that external chest compression might improve the Cpl,rs by reducing EELV. Although this seems to lead to reduced alveolar overdistension in the nondependent areas, it might also favor dorsal de-recruitment. Case 3 A 64-year-old man (21.5 kg/m2), with a medical history of Hodgkin’s lymphoma and bilateral pneumonia caused by Pneumocystis jirovecii, was admitted to the general 1336 Research Letters ICU (Ospedale Maggiore Policlinico) for ARDS. To reduce tidal overdistension, 3 cm H2O of positive endexpiratory pressure (PEEP) and 6 mL/kg predicted body weight TV were used. However, ventilation was not protective (DP,rs ¼ 25 cm H2O). A weight was therefore placed on the patient’s chest, with an immediate improvement in respiratory mechanics (Fig 2). A chest CT scan was acquired at end-inspiration and endexpiration, both with and without the weight on the chest, to optimize ventilator settings. Figure 2 (panel 3) shows a representative slice with color-mapped qualitative density analysis.6 Application of the weight reduced EELV, with an end-expiratory reduction and increase of hyperinflated and poorly aerated lung tissue, respectively. [ 160#4 CHEST OCTOBER 2021 ] Impedance 1 3 Without Weight 2,000 20 0 0 –2,000 –20 –4,000 –40 A START END Lung density (HU): –1,000 –900 –800 –700 –600 End-inspiration 40 Delta Regional TV (mL) Delta End-Expiratory Lung Impedance 2 4,000 B End-expiration A With Weight C D –500 –400 –300 –200 –100 0 C B Nondependent Delta impedance Dependent Delta impedance Nondependent Delta TV Dependent Delta TV Figure 2 – Chest compression. Case 2. Lung mechanics and electrical impedance tomography behavior during baseline (step A), chest compression (step B), and following removal of the chest weight (step C). Ventilatory settings were as follows: volume-controlled mode, tidal volume of 400 mL, respiratory rate of 25 breaths/min, and positive end-expiratory pressure of 8 cm H2O with an FIO2 of 0.50. The chest compression led to a global end-expiratory lung impedance (EELI) decrease (step B, panel 1) compared with baseline (step A, panel 1); once the compression is discontinued, the EELI increased without returning to baseline values (step C, panel 1). We observed two effects on the regional ventilation: in the dependent lung (dorsal), the chest compression decreased both EELI and regional ventilation (step B, panel 2, solid and dashed black lines); in the nondependent lung (ventral), the compression led to a decrease in EELI (to a greater extent compared with dorsal) and an increase in tidal volume (step B, panel 2, solid and dashed red lines). We also analyzed these regional effects at the beginning and at the end of step B (step B, panel 1, dashed yellow lines, and panel 2); no difference was observed in the dependent lung, whereas a further reduction in EELI was observed in the nondependent lung region. These effects in regional ventilation and EELI disappeared once the chest weight was removed, without a return to baseline values (step C, panel 2). Compliance of the respiratory system was increased during chest compression (from 30 to 36 mL/cm H2O), and driving pressure of the respiratory system was reduced from 13 to 11 cm H2O. These effects immediately reverted following removal of the chest weight. We observed a reduction of the following parameters from baseline to step B: blood oxygen saturation, 98% to 96%; PaO2, 81 to 70 mm Hg; end tidal CO2, 41 to 38 mm Hg; PaCO2, 56 to 50 mm Hg; and alveolar dead space, 26% to 24%. After removal of the chest weight, blood oxygen saturation and end tidal CO2 were 96% and 40 mm Hg, respectively. Case 3. Color-mapped CT scan. Representative CT slices of the lung obtained without (left) and with (right) application of a chest weight. Images were acquired during an end-expiratory (boxes A and B) or end-inspiratory (boxes C and D) hold. The images are visualized by using a color map; color maps represent different ranges of HU, which are reported on the right side of the graphic. Of note, images acquired with a lung weight have lower quality because they were acquired using a low-dose radiation protocol. This, however, does not significantly affect the quantitative results. Following are the respiratory mechanics and lung CT data at baseline and following the application of a chest weight during an end-expiratory hold with a positive endexpiratory pressure of 3 cm H2O: plateau pressure, 28 to 23 cm H2O; driving pressure of the respiratory system, 25 to 20 cm H2O; compliance of the respiratory system, 15 to 19 mL/cm H2O; compliance of the lung, 19 to 24 mL/cm H2O; compliance of the chest wall, 80 to 93 mL/cm H2O; endexpiratory lung volume, 614 to 469 mL; mean CT number, –270 to –220 HU; lung weight, 1,661 to 1,659 g; hyperinflated lung tissue, 0 to 0%; normally aerated lung tissue, 13% to 10%; poorly aerated lung tissue, 27% to 29%; and nonaerated lung tissue, 60% to 61%. HU ¼ Hounsfield units; TV ¼ tidal volume. Case 4 A 62-year-old man (BMI, 28 kg/m2) with severe COVID-19 ARDS was in the ICU (Milan Fair)7 on volume-controlled ventilation with the following settings: TV, 400 mL; respiratory rate, 35 beats/min; PEEP, 8 cm H2O; FIO2, 0.9; and peak inspiratory pressure (PIP), 42 cm H2O. The patient experienced decreased PIP when the head of the bed was lowered to 0 for nursing. To test whether this observation was related to an increased transmission of the abdominal pressure to the chest wall, we performed a transient abdominal compression in semi-recumbent chestjournal.org position (~15 s). A sudden decrease of PIP to 26 cm H2O was observed. After releasing the abdominal compression, PIP immediately increased to 38 cm H2O. Blood oxygen saturation and hemodynamics were unaffected by the transient change in PIP (Video 1, part 2). To further investigate this mechanism, we performed a formal test applying a 5-kg saline bag to the abdomen for 10 min while recording airway and esophageal pressures during end-inspiratory and end-expiratory holds. The following was noted after application of the abdominal weight: DP,rs decreased (28 to 17 cm 1337 H2O); driving pressure of the chest wall increased (1 to 3 cm H2O); and driving pressure of the lung decreased by 13 cm H2O. Consequently, compliance of the lung doubled (15 to 29 mL/cm H2O), whereas compliance of the chest wall worsened (400 to 133 mL/cm H2O). During this test, PaO2/FIO2 and PaCO2 remained unchanged. This finding suggests that the improvement of the lung mechanical properties is unlikely determined by lung recruitment, and more likely the consequence of a decreased lung resting volume preventing endinspiratory overdistention. Discussion The presented cases show that, in some patients with ARDS, compression on the chest wall decreases the amount of hyperinflation, improving respiratory mechanics without causing alveolar recruitment. Our explanation resides in a right shift of the chest wall pressure-volume loop, which decreases lung volume, causing ventilation to occur in a more compliant region of the lung pressure-volume loop (Fig 1, panel 3). The measurement of partitioned respiratory mechanics suggests that an extrinsic weight does not worsen the compliance of the chest wall in a clinically relevant way. However, it reduces chest wall and lung volume, similarly to what is observed in obese patients.8 This might be an additional explanation for the protective effects determined by prone position9 and for the obesity paradox.10 Chest wall compression does not seem to favor alveolar recruitment, which is also unlikely given the decreased airway pressure during weight placement. Our work suggests that an increase of respiratory system compliance during chest or abdominal compression should be regarded as a sign of tidal overinflation and should be taken into account to optimize mechanical ventilation. It remains unknown if improvement of lung mechanics due to patient positioning or chest wall compression has an impact on gas exchange and, ultimately, on patient outcome. Emanuele Rezoagli, MD, PhD Luca Bastia, MD Alice Grassi, MD Arturo Chieregato, MD Thomas Langer, MD Giacomo Grasselli, MD Pietro Caironi, MD Andrea Pradella, MD Alessandro Santini, MD 1338 Research Letters Alessandro Protti, MD Roberto Fumagalli, MD Giuseppe Foti, MD Giacomo Bellani, MD, PhD AFFILIATIONS: From the Department of Medicine and Surgery (E. Rezoagli, A. Grassi, T. Langer, R. Fumagalli, G. Foti, and G. Bellani), University of Milan-Bicocca, Monza, Italy; ASST Monza (E. Rezoagli, G. Foti, and G. Bellani), San Gerardo Hospital, Monza, Italy; Neurointensive Care Unit (L. Bastia and A. Chieregato), ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy; Department of Anesthesiology and Pain Medicine (A. Grassi), University of Toronto, Toronto, ON, Canada; Department of Anaesthesia and Intensive Care Medicine (T. Langer and R. Fumagalli), Niguarda Ca’ Granda, Milan, Italy; Department of Anesthesia, Critical Care and Emergency (G. Grasselli) and Surgery and Liver Transplant Center (G. Grasselli), Fondazione IRCCS Ca’ Granda-Ospedale Maggiore Policlinico, Milan, Italy; Department of Anesthesia and Critical Care (P. Caironi), Azienda Ospedaliero-Universitara S. Luigi Gonzaga, Orbassano, Italy; Department of Oncology (P. Caironi), University of Turin, Turin, Italy; IRCCS Humanitas Research Hospital (A. Pradella, A. Santini, and A. Protti), Rozzano-Milan, Italy; and the Department of Biomedical Sciences (A. Protti), Humanitas University, Pieve Emanuele-Milan, Italy. Drs Rezoagli and Bastia contributed equally to the manuscript. FUNDING/SUPPORT: The authors have reported to CHEST that no funding was received for this study. FINANCIAL/NONFINANCIAL DISCLOSURES: The authors have reported to CHEST the following: G. B. and G. F. received fees from Draeger Medical for lectures also on EIT. None declared (E. R., L. B., A. G., A. C., T. L., G. G., P. C., A. P., A. S., A. P., R. F.). CORRESPONDENCE TO: Giacomo Bellani, MD, PhD; email: giacomo. bellani1@unimib.it, emanuele.rezoagli@unimib.it Copyright Ó 2021 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved. DOI: https://doi.org/10.1016/j.chest.2021.05.057 Acknowledgments Other contributions: The authors are highly grateful to Laurent Brochard, MD, for helpful discussions and his constructive feedback in regard to this work. The authors are indebted to Dario Manzolini, MD, and Manuela Marotta, MD, Department of Medicine and Surgery of the University of Milano-Bicocca, Monza, Italy, for their valuable support with the making of the Video about case 1; to Serena Brusatori, MD, Department of Pathophysiology and Transplantation of the University of Milan, for her valuable support with qualitative colormapped analysis of Figure 2, panel 3; and to Manuela Chiodi, MD, Department of Pathophysiology and Transplantation of the University of Milan, for her valuable support with quantitative CT analysis of Figure 2, panel 3. Additional information: The Video can be found in the Supplemental Materials section of the online article. References 1. Rezoagli E, Fumagalli R, Bellani G. Definition and epidemiology of acute respiratory distress syndrome. Ann Transl Med. 2017;5(14): 282. 2. Gattinoni L, Taccone P, Carlesso E, Marini JJ. Prone position in acute respiratory distress syndrome. Rationale, indications, and limits. Am J Respir Crit Care Med. 2013;188(11):12861293. 3. Rezoagli E, Bellani G. How I set up positive end-expiratory pressure: evidence- and physiology-based! Crit Care. 2019;23(1):412. 4. Bottino N, Panigada M, Chiumello D, Pelosi P, Gattinoni L. Effects of artificial changes in chest wall compliance on respiratory mechanics and gas exchange in patients with acute lung injury (ALI). Crit Care. 2000;4(suppl 1):P117. [ 160#4 CHEST OCTOBER 2021 ] 5. Frerichs I, Amato MBP, Van Kaam AH, et al; TREND study group. Chest electrical impedance tomography examination, data analysis, terminology, clinical use and recommendations: consensus statement of the TRanslational EIT developmeNt stuDy group. Thorax. 2017;72(1):83-93. 6. Langer T, Castagna V, Brusatori S, et al. Short-term physiologic consequences of regional pulmonary vascular occlusion in pigs. Anesthesiology. 2019;131(2):336-343. 7. Rezoagli E, Magliocca A, Bellani G, Pesenti A, Grasselli G. Development of a critical care response—experiences from Italy during the Covid19 pandemic. Anesthesiol Clin. 2021;39(2):265284. chestjournal.org 8. Behazin N, Jones SB, Cohen RI, Loring SH. Respiratory restriction and elevated pleural and esophageal pressures in morbid obesity. J Appl Physiol. 2010;108(1):212-218. 9. Katira BH, Osada K, Engelberts D, et al. Positive end-expiratory pressure, pleural pressure, and regional compliance during pronation: an experimental study. Am J Respir Crit Care Med. 2021;203(10): 1266-1274. 10. Ni Y-N, Luo J, Yu H, et al. Can body mass index predict clinical outcomes for patients with acute lung injury/acute respiratory distress syndrome? A meta-analysis. Crit Care. 2017;21(1):36. 1339