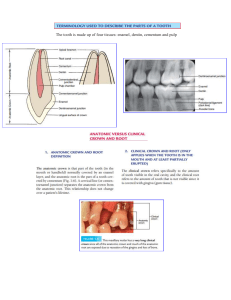
METABOLIC DISEASES OF BONE By Syeda Batul Fatima Outline RICKETS SCURVY HYPERPARATHYROIDISM GIGANTISM & ACROMEGALY FLUOROSIS Metabolic bone diseases describes a group of disorders due to abnormalities of formation (bone morphology) and metabolism of bone (functions) . INTRODUCTION OR Any systemic condition that results in reduced bone strength, altered mineralization or composition. Rickets Rickets is the softening and weakening of bones in children, usually because of an extreme and prolonged vitamin D deficiency. Rickets Causes defective calcification & development of the skeleton Onset usually in infancy Its adult counterpart is osteomalacia The main defects are broadening of the growing ends of bones & prominent costochondral junctions due to the epiphyseal defects. Overgrowth of cartilage (as shown) causes the epiphyseal plate to be broad, thick and irregular, and the ends of the bone become splayed. The growing end of the bone is ill-defined and calcification defective. Rickets Typical changes in the skull are ● ● ● wide fontanelles bossing of the frontal and parietal eminences thinning of the back of the skull Dental effects/Oral manifestations ● ● ● ● Occur in the most severe cases Hypocalcification of dentine, with a wide band of predentine & excessive interglobular spaces Enamel hypoplasia Eruption of teeth may also be delayed in such cases Rickets Causes ● In developing countries is usually due to deficiency of dietary calcium ○ ● ● Cereal & wholemeal grains containing phytates which impairs calcium absorption Rare in developed countries; caused by deficiency of vitamin D, either in the diet or through lack of exposure to sunlight Renal rickets; excess mineral excretion in chronic renal diseases; include renal tubular acidosis, hypophosphatemic rickets & defects in vitamin D metabolism in the kidney Rickets Treatment ● ● ● ● ● Vitamin D. Adequate dietary Calcium & phosphorus provided by milk, formula & other dairy products; or added to vitamin D prescriptions Symptomatic hypocalcemia need IV CaCl as 20mg/kg or Ca gluconate as 100 mg/kg as a bolus, followed by oral calcium tapered over 2-6 weeks. Health education Treatment of the cause if possible Rickets Vitamin D resistant rickets This condition caused by genetic failure of reabsorption of phosphate in the kidney is associated with characteristic dental defects Scurvy Prolonged deficiency of vitamin C may result in scurvy. Scurvy It is characterized by: ➔ ➔ ➔ Weakened blood vessels particularly microvessels having least muscular supports. Defective synthesis of osteoid which is derivative of collagen. Impaired wound healing. Pathogenesis of Scurvy There is defective formation of collagen in connective tissues because of failure of hydroxylation of proline to hydroxyproline which is a characteristic amino acid of collagen. There is also: ➔ ➔ Increase permeability of capillary (hemorrhage). Anemia due to erythropoiesis and defective collagen formation. Oral manifestations of scurvy & Management It occurs chiefly in gingival and periodontal region. Interdental and marginal gingiva is bright red, swollen, smooth, shiny surface producing an appearance known as scurvy bud. In fully developed scurvy, the gingiva becomes boggy, ulcerated and bleeds easily. These types of gingival lesion are termed as scorbutic gingivitis. Color changes to violaceous red. Typical fetid breath of the patient with fusospirochetal stomatitis. In severe cases, hemorrhage and swelling of periodontal ligament membrane occurs followed by loss of bone and loosening of teeth which are exfoliated. Management; Vitamin C 250 mg 3 times daily can be given. Hyperparathyroidism It is an endocrine disorder in which there is an excess of circulating parathyroid hormone. Excess PTH stimulates osteoclast to mobilize calcium from skeleton leading to hypercalcemia in addition to PTH increased renal tubular reabsorption of calcium. Clinical features of hyperparathyroidism Age and sex distribution: Female to male ratio is 3:1. Mainly in 30 to 60 years of age. Classic triad: It has classic triad of stones, bones and abdominal organs. 1) 2) 3) Stones: Renal calculi are common due to elevated level of serum calcium. Metastatic calcification is seen. Bones: There are variety of osseous changes seen in bones. There is also bone and joint pain. Abdominal organs: There is tendency for the development of duodenal ulcers. There is gradual loosening drifting and loss of teeth, malocclusion. There is pathological fracture of bone. Cystic lesion involving jaws are seen over 10 percent of cases. Oral manifestations of Hyperparathyroidism Brown tumor is present intraorally. ● ● ● Dental Radiograph in hyperparathyroidism ● ● ● Reduced bone density, Loss of trabecular pattern and lamina dura around the teeth. In severe disease there is development of one or More brown tumours in the jaws which appear as unilocular or multilocular cysts There is diffuse mandibular enlargement in hyperparathyroidism secondary to renal disease Pathological fractures There is loss of lamina dura around the roots, loss of trabeculae centrally and coarsening of the trabecular pattern elsewhere. Serum alkaline phosphatase and serum calcium level is increased. Decreased blood phosphorus level. Increase in circulating hormone demonstrated by radioisotope studies. Diagnosis & Treatment Cinacalcet is now a day use in management of overproduction of parathormone associated with secondary hyperparathyroidism. This is calcimimetic agent that sensitize the calcium receptor of the parathyroid cells to extracellular calcium causing the cell to reduce output of parathormone. Gigantism: If the increase occurs before the epiphysis of the long bone are closed. Acromegaly: If the increase occurs later in life after epiphysis closure. Gigantism & Acromegaly Gigantism Generalized overgrowth of most tissue in childhood occurs. Most of the soft tissue and bones respond to the excess hormone by enlarging. Symptoms: ● ● ● ● Height 7 to 8 feet Later in life, may show genital underdevelopment Excessive perspiration & complain of headache, lassitude, fatigue, muscle & joints pain and hot flashes Increase in size of calvarium Gigantism Signs: Pituitary tumors may also induce deficiency of other pituitary hormones causing signs of hypogonadism including decreased libido and menstrual problems in women. This disease is caused by prolonged and excessive secretion of growth hormone, usually due to a secreting adenoma of the anterior lobe of the pituitary developing after the epiphyses have closed. Acromegaly Bone overgrowth and thickening of the soft tissue cause a characteristic coarsening of facial features termed acromegaly. It is more common in males and occurs most frequently in 3rd decade. Acromegaly Symptoms Hand and feet become large, with clubbing of the toes and fingers due to enlargement of the tufts of the terminal phalanges. There is temporal headache, photophobia & reduction in vision. Ribs also increase in size. Hypertrophy of soft palatal tissue may cause or accentuate sleep apnea. Acromegaly Oral Manifestations The palatal vault is usually flattened and the tongue increase in size and may cause crenation on its lateral border. Teeth are proportional to the size of jaw & the rest of the body and root may be longer than normal The teeth become spaced Class III malocclusion Acromegaly Diagnosis Laboratory Findings It can be made from the characteristic clinical and radiographic findings. Growth hormone concentration can be measured by radioimmunoassay technique. Measurement of serum growth hormone level should be done. This should be done after giving patient a measured quantity of glucose. Normally, this glucose challenge will reduce the production of growth hormone. Radiological Features It shows enlarge sella as a results presence of pituitary adenoma. MRI will diagnose pituitary adenoma. Management Trans-sphenoidal surgery may result in cure of GH excess Octreotide, pegvisomant & dopamine antagonists. Fluorosis It is a cosmetic condition that occurs during first eight years of life. Also termed as mottled enamel is an extremely common disorder, characterized by hypomineralization of tooth enamel caused by ingestion of excessive fluoride during enamel formation. Causes of fluorosis ● ● ● ● Excess fluoridation of drinking water Ingestion of fluoride toothpaste Overuse of Fluoride tablets Consumption of processed food made with fluoridated water Mechanism of action in fluorosis ● ● ● Structurally, an increase in fluoride intake results in an increase in degree & extent of porosity of enamel. Enamel changes described may be a result of fluoride damage of secretory ameloblast. There can either be due to fluoride induce change in compositon of enamel matrix or be a result of disturbance of the cellular processes during enamel maturation. Signs & Symptoms of fluorosis ● Chalk like discoloration of teeth with white spot or lines on tooth enamel ● In more severe cases, the affected area have yellow or brown discoloration. ● In extreme forms, fluorosis may result in pitted tooth surface Classification of fluorosis 1. 2. 3. 4. 5. 6. Normal Questionable Very mild Mild Moderate Severe 1. ● ● ● ● Normal Smooth Glossy Pale Creamy white translucent surface 1. ● Questionable Ranging from few white flecks to occassional white spot Very mild ● Small opaque paper white area scattered over the tooth but not involving as much as 25 % of tooth surface Mild ● The white opaque areas in the enamel of the tooth are more extensive but do not involve as much as 50% of the tooth Moderate ● ● All enamel surface of teeth are affected and the surface subject to attrition show wear. Brown stain is frequently a disfiguring feature Severe ● All enamel surfaces are affected discrete or confluent pitting . Brown stains are widespread and teeth often present a corroded like appearance. Prevention of fluorosis ● ● ● ● To prevent fluorosis , fluoridation of drinking water should not exceed normal range (Normal range : 0.7 to 1.2 ppm) Fluoride supplement should only be prescribed for children living in non fluoridated water supply areas Use only acceptable amount of toothpaste for children under 6 year (pea size) It is important to teach the child to spit out the toothpaste after brushing instead of swallowing Treatment of fluorosis ● ● ● Microabrasion : (Conservative removal of outer layer of enamel) Followed by tooth whitening can make the brown discoloration less apparent Bonding: coats the teeth with hard resin that bonds to the enamel. Veneers: These are the customized shells that cover the front of teeth to improve the appearance. References 1. Textbook of Oral Pathology 2. Soames’ Southam’s Oral Pathology