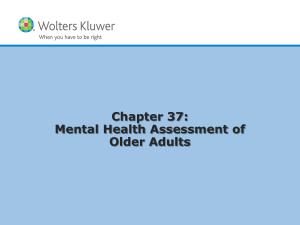
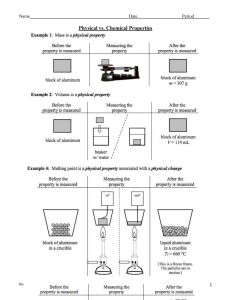
Management of Patients With Cerebrovascular Disorders Edited M. Leavitt Cerebrovascular Disorders Functional abnormality of the CNS that occurs when the blood supply to the brain is disrupted o Ischemic stroke: inadequate blood flow o Hemorrhagic stroke: bleeding Stroke (“brain attack”) is the primary cerebrovascular disorder and the fifth leading cause of death in the United States Stroke is the leading cause of serious long-term disability in the United States Financial impact is profound Copyright © 2018 Wolters Kluwer · All Rights Reserved Question What is agnosia? A. Failure to recognize familiar objects perceived by the senses B. Inability to express oneself or to understand language C. Inability to perform previously learned purposeful motor acts on a voluntary basis D. Impaired ability to coordinate movement, often seen as a staggering gait or postural imbalance Copyright © 2018 Wolters Kluwer · All Rights Reserved Answer to Question A. Failure to recognize familiar objects perceived by the senses Agnosia is failure to recognize familiar objects perceived by the senses. Aphasia is an inability to express oneself or to understand language. Apraxia is an inability to perform previously learned purposeful motor acts on a voluntary basis. Ataxia is an impaired ability to coordinate movement, often seen as a staggering gait or postural imbalance Copyright © 2018 Wolters Kluwer · All Rights Reserved Question Which of the following patients has the highest risk of stroke? o A. Obese 45-y/o Native American o B. 35 y/o Asian American woman who smokes o C. 32 y/o white woman taking oral contraceptives o D. 65 y/o African American man with hypertension Copyright © 2018 Wolters Kluwer · All Rights Reserved Prevention Non-modifiable risk factors o Age (older than 55 years), male gender, African Americans (see Health Disparities p. 1347) Modifiable risk factors o Hypertension is the primary risk factor o Cardiovascular disease o Elevated cholesterol or elevated hematocrit o Obesity o Diabetes o Oral contraceptive use o Smoking and drug and alcohol abuse o Women w/ migraine aura Copyright © 2018 Wolters Kluwer · All Rights Reserved Question Is the following statement true or false? Ischemic stroke account for 85% to 87% of strokes, and hemorrhagic stroke accounts for 13% to 15% A. True B. False Copyright © 2018 Wolters Kluwer · All Rights Reserved Answer to Question A. True Ischemic stroke account for 85%-87% of strokes, while hemorrhagic stroke accounts for 13%-15% Copyright © 2018 Wolters Kluwer · All Rights Reserved Transient Ischemic Attack (TIA) Temporary neurologic deficit resulting from a temporary impairment of blood flow May be due to microembolii Typically lasts less than 60 minutes “Warning of an impending stroke” Diagnostic workup is required to treat and prevent irreversible deficits Treat as a medical emergency TIA Copyright © 2018 Wolters Kluwer · All Rights Reserved Preventive Treatment and Secondary Prevention Health maintenance measures including a healthy lifestyle, not smoking, exercise, healthy diet and weight Carotid endarterectomy for carotid stenosis o Removes plaques that block cerebral blood flow Anticoagulant therapy for atrial fibrillation Antiplatelet therapy “Statins” Antihypertensive medications Copyright © 2018 Wolters Kluwer · All Rights Reserved Carotid Endarterectomy Copyright © 2018 Wolters Kluwer · All Rights Reserved Stroke “Brain attack” Urgent issue similar to “heart attack” TIME = BRAIN Older name CVA (cerebrovascular accident) Sudden loss of function resulting from a disruption of the blood supply to a part of the brain Types of stroke: o Ischemic (85% - 87%) Thrombotic: injury to vessel wall -> clot in lumen Embolic: embolism lodges in vessel wall o Hemorrhagic (13% - 15%) Intracerebral vessel rupture Subarachnoid aneurysm rupture Copyright © 2018 Wolters Kluwer · All Rights Reserved Stroke: Ischemic vs Hemorrhagic Copyright © 2018 Wolters Kluwer · All Rights Reserved Ischemic Stroke Disruption of the blood supply caused by an obstruction, usually a thrombus or embolism, that causes infarction of brain tissue Types o Large artery thrombosis: plaques in large vessels o Small penetrating artery thrombosis: common type AKA Lacunar Stroke (infarcted tissue leaves a cavity) o Cardiogenic embolism: A fib, LV thrombus, Patent Foramen Ovale (PFO). Most common site is Left Middle Cerebral Artery o Cryptogenic: no known cause, might be PFO o Other: cocaine, coagulopathies, vasospasm, dissection of carotid or vertebral arteries Copyright © 2018 Wolters Kluwer · All Rights Reserved Left atrial appendage Copyright © 2018 Wolters Kluwer · All Rights Reserved Patent foramen ovale and closure Copyright © 2018 Wolters Kluwer · All Rights Reserved Pathophysiology The Ischemic Cascade Copyright © 2018 Wolters Kluwer · All Rights Reserved Manifestations of Ischemic Stroke Symptoms depend on which blood vessels are obstructed and size of the affected brain area Numbness or weakness of face, arm, or leg, especially on one side Confusion or change in mental status Trouble speaking or understanding speech Difficulty in walking, dizziness, or loss of balance or coordination Sudden, severe headache (more freq hemorrhagic) Perceptual disturbances Copyright © 2018 Wolters Kluwer · All Rights Reserved Terms Hemiplegia: paralysis of one side or part of the body Hemiparesis: weakness of one side or part of the body Dysarthria: difficulty formulating words due to muscle weakness Aphasia: Expressive, receptive, or both (Global) o expressive aphasia: unable to form words o receptive aphasia: unable to comprehend words Hemianopsia: loss of visual field o Homonymous hemianopsia: loss of half visual field Agnosia: failure to recognize familiar objects perceived by the senses. Apraxia: inability to perform a previously learned action Copyright © 2018 Wolters Kluwer · All Rights Reserved Visual Pathways Copyright © 2018 Wolters Kluwer · All Rights Reserved Assessment History: When last seen well? WHY? Airway: loss of gag or cough? altered respiratory pattern? o Bedside dysphagia screening o Fluoroscopic swallow study CV: BP, heart rate & rhythm, carotid bruit? Assessment of stroke: NIHSS assessment tool Neuro deficits: Symptoms depend on which blood vessels are obstructed and size of the affected brain area o o o o o o o Numbness or weakness of face, arm, or leg, especially on one side Confusion or change in mental status Trouble speaking or understanding speech Difficulty in walking, dizziness, or loss of balance or coordination Sudden, severe headache Perceptual disturbances Stroke! Copyright © 2018 Wolters Kluwer · All Rights Reserved National Institutes of Health Stroke Scale (NIHSS) Table 57-10., p. 1368 Copyright © 2018 Wolters Kluwer · All Rights Reserved National Institutes of Health Stroke Scale (NIHSS) Significance of NIHSS (start at 0.30, advance to 2:50) Tips on scoring the NIHSS (go to 0.55, then 7:10) NIHSS Demo Copyright © 2018 Wolters Kluwer · All Rights Reserved Knowledge Check Your patient with a right-sided stroke has left homonymous hemianopsia. Which of the following would you do? o A. Tell patient to look to right side to see objects o B. Place bedside table on right side of bed o C. Explain food on plate using clock method o D. Place wheelchair on patient’s left side Copyright © 2018 Wolters Kluwer · All Rights Reserved Diagnostic Studies Diagnosis: ED Diagnosis o CT scan: non-contrast to direct treatment CT Scan Ischemic stroke Hemorrhagic stroke o Cerebral angiography o Lumbar puncture if CT is negative and ICP is not elevated to confirm subarachnoid hemorrhage Copyright © 2018 Wolters Kluwer · All Rights Reserved Question A patient has trouble finding words and right arm weakness. What area of the brain is likely involved? o A. Brainstem o B. Vertebral artery o C. Left middle cerebral artery o D. Right middle cerebral artery Copyright © 2018 Wolters Kluwer · All Rights Reserved Left vs. Right hemispheric stroke Left hemisphere: language, math, analytics Right hemisphere: visual & special awareness; proprioception Copyright © 2018 Wolters Kluwer · All Rights Reserved Copyright © 2018 Wolters Kluwer · All Rights Reserved Medical Management: Acute Phase of Stroke Prompt diagnosis and treatment Continued assessment of stroke: NIHSS assessment tool Thrombolytic therapy o Criteria for tPA o IV dosage and administration o Patient monitoring o Side effects: potential bleeding Elevate head of bed (HOB) unless contraindicated Maintain airway and ventilation Continuous hemodynamic monitoring and neurologic assessment Copyright © 2018 Wolters Kluwer · All Rights Reserved Ischemic Stroke Treatment tPA screening: o Non-contrast CT to R/O hemorrhagic stroke o Labs: Blood sugar & PT, PTT o History GI Bleed or head trauma last 3 months Active internal bleeding last 3 weeks Major surgery last 2 weeks tPA infusion, systemic IV o Dose is weight-based o Monitor VS & neuro status o Control systolic BP <185 mmHg May also give tPA IA, directly to clot, within 6 hours Copyright © 2018 Wolters Kluwer · All Rights Reserved Ischemic Stroke Treatment tPA o Binds to fibrin, converts plasminogen to plasmin, digests fibrin, breaks down clot. o Give within 3 hrs of sx (sometimes up to 4.5 hrs) o Goal: given within 60 minutes of ED arrival o Door to needle in 5 minutes o Thrombectomy with stent retrievers is standard of care for some acute ischemic strokes o Neurovascular Stent Retriever o Must meet criteria (>18, pre-stroke no deficits, tPA within 4.5 hrs, proximal large vessel occlusion in the anterior circulation (internal carotid or middle cerebral arteries), endovascular tmt within 6 hrs) Copyright © 2018 Wolters Kluwer · All Rights Reserved If tPA contraindicated… Oxygen HOB up to decrease ICP Hemodynamic monitoring o If hypertensive, reduce MAP by 30% o Balance of reducing BP but not reducing cerebral perfusion pressure (CPP) Less than 220/120 o Higher BPs are desired to perfuse brain May need intubation for airway mgmt Mannitol (osmotic diuretic) is controversial. Has not been shown to have statistically significant benefit Copyright © 2018 Wolters Kluwer · All Rights Reserved Find source of embolic stroke Carotid ultrasound CT angiography MRI angiography Transthoracic echo Transesophageal echo Copyright © 2018 Wolters Kluwer · All Rights Reserved Knowledge Check Which of the following findings would you expect in a patient with a left-hemispheric stroke? o A. Poor impulse control o B. Poor judgment o C. Difficulty understanding language o D. Loss of depth perception Copyright © 2018 Wolters Kluwer · All Rights Reserved Hemorrhagic Stroke Caused by bleeding into brain tissue, the ventricles, or subarachnoid space May be caused by o spontaneous rupture of small vessels primarily related to hypertension o subarachnoid hemorrhage (SAH) caused by a ruptured aneurysm: SAH -> SIADH -> what electrolyte problem? 30-55% What IV fluid order should be anticipated? o intracerebral hemorrhage related to amyloid angiopathy o arterial venous malformations (AVMs) o intracranial aneurysms o medications such as anticoagulants Copyright © 2018 Wolters Kluwer · All Rights Reserved Hemorrhagic Stroke Brain metabolism is disrupted by exposure to blood ICP increases caused by blood in the subarachnoid space Compression or secondary ischemia from reduced perfusion and vasoconstriction causes injury to brain tissue Intracerebral hemorrhage from HTN and cerebral atherosclerosis Copyright © 2018 Wolters Kluwer · All Rights Reserved Manifestations Similar to ischemic stroke Severe headache: may be sign of leaking aneurysm or other brain bleed Early and sudden changes in LOC Vomiting Bleeding Copyright © 2018 Wolters Kluwer · All Rights Reserved Aneurysms Dilation of walls of cerebral artery due to weakness in the arterial walls Usually occur at bifurcations of large arteries at Circle of Willis Rupture = Hemorrhagic stroke Copyright © 2018 Wolters Kluwer · All Rights Reserved Copyright © 2018 Wolters Kluwer · All Rights Reserved Aneurysms Copyright © 2018 Wolters Kluwer · All Rights Reserved Aneurysm treatment (Fig. 57-7, p. 1356) Cerebral aneurysms 3 ways to treat cerebral aneurysms Aneurysm coiling and stenting Aneurysm clipping (start at 30 sec) Clipping unruptured middle cerebral artery aneurysm (clip goes on at 5 min) Copyright © 2018 Wolters Kluwer · All Rights Reserved Aneurysm Precautions Provide a nonstimulating environment, prevent increases in ICP, prevent further bleeding: o Absolute bed rest with HOB 30 degrees o Avoid all activity that may increase ICP or BP; Valsalva maneuver, acute flexion or rotation of neck or head o Stool softener and mild laxatives o Nonstimulating, nonstressful environment; dim lighting, no reading, no TV, no radio o Visitors are restricted Copyright © 2018 Wolters Kluwer · All Rights Reserved Arteriovenous Malformations Tangle of arteries and veins in brain that lacks a capillary bed Vessels can dilate and rupture AVM Copyright © 2018 Wolters Kluwer · All Rights Reserved Nursing Process: The Patient With a Hemorrhagic Stroke—Assessment Complete and ongoing neurologic assessment; use neurologic flow chart NIHSS Altered LOC: earliest sign of deterioration o Drowsy, slurred speech, sluggish pupils Sluggish pupillary reaction Motor and sensory dysfunction Cranial nerve deficits Speech difficulties and visual disturbance Headache and nuchal rigidity Other neurologic deficits Copyright © 2018 Wolters Kluwer · All Rights Reserved Nursing Process: The Patient With a Hemorrhagic Stroke—Diagnoses Risk for ineffective tissue perfusion (cerebral) related to bleeding or vasospasm Anxiety related to illness and/or medically imposed restrictions (aneurysm precautions) Copyright © 2018 Wolters Kluwer · All Rights Reserved Collaborative Problems and Potential Complications: Hemorrhagic Stroke Decreased cerebral blood flow Inadequate oxygen delivery to brain Pneumonia Vasospasm Seizures Hydrocephalus Rebleeding Hyponatremia Copyright © 2018 Wolters Kluwer · All Rights Reserved Nursing Process: The Patient With a Hemorrhagic Stroke—Planning Goals may include: o Improved cerebral tissue perfusion o Relief of anxiety o The absence of complications Copyright © 2018 Wolters Kluwer · All Rights Reserved Nursing Process: The Patient Recovering From a Stroke—Assessment Acute phase: o Ongoing, frequent monitoring of all systems, including vital signs and neurologic assessment o LOC o Motor symptoms o Speech o Pupil changes o I&O o Blood pressure maintenance o Bleeding o Oxygen saturation o Collaborative Care: Box on p. 1359 Copyright © 2018 Wolters Kluwer · All Rights Reserved Nursing Care Post Acute Phase After the acute phase: o Mental status o Sensation/perception: Fig. 57-9, p. 1362 o Motor control: Fig. 57-10, p. 1363 o Swallowing ability o Nutritional and hydration status Assistive devices Fig 57-8, p. 1361 o Skin integrity o Activity tolerance o Bowel and bladder function o Neglect Parietal lobe problem Copyright © 2018 Wolters Kluwer · All Rights Reserved Knowledge Check Which of the following findings would you expect in a patient with a right hemispheric stroke? o A. Left hemiplegia and poor impulse control o B. Left hemiplegia and aphasia o C. Right hemiplegia and poor situational awareness o D. Right hemiplegia and poor depth perception Copyright © 2018 Wolters Kluwer · All Rights Reserved Nursing Process: The Patient Recovering From a Stroke—Diagnoses Impaired physical mobility Acute pain Self-care deficits Impaired comfort R/T disturbed sensory perception Impaired swallowing Urinary incontinence Constipation Acute confusion Impaired verbal communication Risk for impaired skin integrity Interrupted family processes Sexual dysfunction Copyright © 2018 Wolters Kluwer · All Rights Reserved Nursing Process: The Patient Recovering From a Stroke—Planning Major goals may include o Improved mobility o Avoidance of shoulder pain o Achievement of self-care o Relief of sensory and perceptual deprivation o Prevention of aspiration o Continence of bowel and bladder o Improved thought processes o Achieving a form of communication o Maintaining skin integrity o Restored family functioning o Improved sexual function o Absence of complications Copyright © 2018 Wolters Kluwer · All Rights Reserved Interventions Focus on the whole person Provide interventions to prevent complications and promote rehabilitation Provide support and encouragement Listen to the patient Therapy for aphasia: board of common words & phrases Nursing Through the Years (J&J) 2020 Podcast interview with Rebecca Koszalenski Copyright © 2018 Wolters Kluwer · All Rights Reserved Improving Mobility and Preventing Joint Deformities Turn and position in correct alignment every 2 hours Use of splints Passive or active ROM four or five times day Positioning of hands and fingers Prevention of flexion contractures Prevention of shoulder abduction Do not lift by flaccid shoulder Measures to prevent and treat shoulder problems Copyright © 2018 Wolters Kluwer · All Rights Reserved Improving Mobility and Preventing Joint Deformities Encourage patient to exercise unaffected side Establish regular exercise routine Quadriceps setting and gluteal exercises Assist patient out of bed as soon as possible; assess and help patient achieve balance; move slowly Ambulation training Copyright © 2018 Wolters Kluwer · All Rights Reserved Interventions Enhancing self-care o Set realistic goals with the patient o Encourage personal hygiene o Ensure that patient does not neglect the affected side If visual field loss, approach from intact side Homonymous hemianopsia (loss of half of visual field): may not recognize one side of body as own. Need to see it o Use of assistive devices and modification of clothing Support and encouragement Strategies to enhance communication Encourage patient to turn head, look to side with visual field loss Copyright © 2018 Wolters Kluwer · All Rights Reserved Interventions Nutrition o Consult with speech therapy or nutritional services – immediate dysphagia screen o Have patient sit upright, preferably out of bed to eat o Chin tuck or swallowing method o Use of thickened liquids or pureed diet Bowel and bladder control o Assessment of voiding and scheduled voiding o Measures to prevent constipation: fiber, fluid, toileting schedule o Bowel and bladder retraining Copyright © 2018 Wolters Kluwer · All Rights Reserved Knowledge Check How should you communicate with a patient who has global (both receptive and expressive) aphasia? o A. Speak louder o B. Speak slower o C. Use a letter board o D. Provide multiple instructions at one time Communication with patient with aphasia: Table 57-11, p. 1361 Copyright © 2018 Wolters Kluwer · All Rights Reserved Interventions Relieving sensory deprivation and anxiety Keep sensory stimulation to a minimum for aneurysm precautions Realty orientation Patient and family education Support and reassurance Seizure precautions Strategies to regain and promote self-care and rehabilitation Copyright © 2018 Wolters Kluwer · All Rights Reserved Home Care and Education for the Patient Recovering from a Stroke Prevention of subsequent strokes, health promotion, and follow-up care; Prevention of and signs and symptoms of complications Medication education Safety measures Adaptive strategies and use of assistive devices for ADLs o Unexpected emotional responses -> Frustration Nutrition: diet, swallowing techniques, tube feeding administration Elimination: bowel and bladder programs, catheter use Exercise and activities, recreation and diversion Socialization, support groups, and community resources Copyright © 2018 Wolters Kluwer · All Rights Reserved Question What intervention would NOT be included in aspiration precautions for a patient in the acute phase of a stroke? A. Referral to speech therapy B. Have patient tuck their chin toward the chest when swallowing C. Thickened fluids or pureed diet D. Raise HOB to 30 degrees when feeding Copyright © 2018 Wolters Kluwer · All Rights Reserved Answer to Question D. Raise HOB to 30 degrees when feeding Interventions to prevent aspiration include a referral to speech therapy for swallowing evaluation; having the patient tuck the chin toward the chest when swallowing to close off the trachea, preventing aspiration into the lungs; providing thickened fluids or a pureed diet; and sitting the patient at a full upright position (90 degrees) when feeding or providing fluids. The patient’s HOB should be elevated to 30 degrees at all times to prevent aspiration of secretions but would not prevent aspiration of food or fluids when feeding Copyright © 2018 Wolters Kluwer · All Rights Reserved Questions? Copyright © 2018 Wolters Kluwer · All Rights Reserved