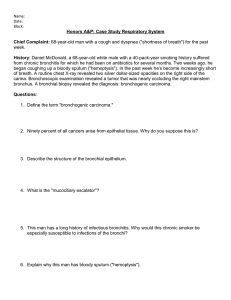
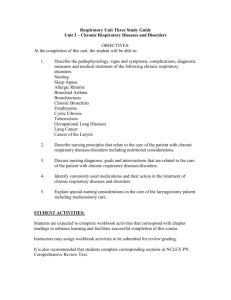
The theme of the lecture: “Bronchial asthma. Chronic obstructive pulmonary disease. The syndrome of bronchial obstruction. Pulmonary emphysema" Ass-prof.N.Bilkevych Respiratory system anatomy Syndromes 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. Respiratory failure Bronchial obstruction Pulmonary emphysema Lung tissue consolidation Mucocilliary insufficiency Intoxicaion syndrome Athelectasis Cavity in the lungs Free air in pleural cavity Liquid in pleural cavity Mucocilliary insufficiency and respiratory failure The syndrome of bronchial obstruction (lat.) – barrier, obstracle. Causes of bronchial obstruction: Obstructio - spasm of bronchial smooth muscles accumulation of fluid in fine bronchi - edema of bronchial mucosa - poor elasticity of lungs Pulmonary emphysema Emphysema is a disease caused by enlargement of the lungs and an increase in their airiness due to overstretching of the alveoli or due to rupture of the alveolar walls. The lungs are enlarged. Exhalation requires greater effort . Gas exchange of oxygen and carbon dioxide in the alveoli due to tissue damage and blockage is markedly reduced. Causes of pulmonary emphysema I. Local A. Congenital abnormalities of bronchi B. Compensatory due to lung collapse, scarring or resection C. Partial bronchial obstruction Neoplasm Foreign body D. MacLeod'syndrome II. Generalized A. Idiopathic B. Senile C. Familial (alpha-1-anti-trypsin deficiency) D. Associated with chronic bronchitis, asthma or pneumoconiosis. Bronchial asthma A chronic recurrent inflammatory disease of the respiratory tract, which is characterized by reverse bronchial obstruction and bronchial hyperreactivity. The bronchial obstruction is produced by a combination of mucosal edema, constriction of the bronchial musculature, excessive secretion of viscid mucus, causing mucous plugs. Essentials of Diagnosis: • Recurrent acute attacks of dyspnea, cough, and mucoid sputum, usually accompanied by wheezing. • Prolonged expiration with generalized wheezing and musical rales. • Bronchial obstruction is reversible by drugs Etiology 40-80% of patients have a hereditary predisposition (allergy, allergic rhinitis and sinusitis, nasal polyps) •Acquired etiological factors • Acquired ethiological factors Domestic allergens Environmental allergens Food allergy drugs bacterial allergens Domestic mites, animal wool, insect allergens, fungal spores, plant pollen Food allergy (milk, wheat flour, fish, food additives, dyes, conservants) Acquired ethiological factors Domestic allergens ( dust, insect allergens, fungi, animal wool, epidermis) Environmental allergens ( fungi, insect allergens, pollen etc) Food allergy ( milk, flour, fish, chemical admixtures to food) drugs ( antibiotics, enzymes, aspirin) bacterial allergens ( neisseria, Staphylococcus aureus, Candida albicans, mycoplasma, helmints) drug allergy (antibiotics, enzymes, aspirin) bacterial allergens] (Neisseria, Staphylococcus aureus, fungi Candida, mycoplasma, roundworms and other infestations, parainfluenza virus) Pathogenesis of BA Immunological mechanisms Due to: - Ig E - basophils - mast cells Reaction mediators: - histamine - prostaglandins - leukotrienes Non-immunological mechanisms Release 1. Pseudoallergic Medications food plant allergens of animal origin biologically active substances and activation of the complement system 2. Theory of β-adrenergic block In norm irritant adren aline α- β- receptors receptors (vascular spasm) β1-miocardium (heart rate ) irritant adrenalinн ннн bronchospasm ATP adenylate cyclase AMP через β2-bronchi (dilatation) βreceptors Formation cyclic AMP In bronchial asthma defect (congenital)β2- adenylate cyclase deficiency рецепторів bronchospasm !!! cAMP 3. Involving neurohumoral and cellular mechanisms (influence of parasympathetic innervation) 4. Reflectory bronchospasm а) rhinobronchial reflex b) cooling of sensitive zones of bronchi c) gastroesophageal reflux 5. Psycho-emotional influences through the autonomic nervous system. 6. Endocrine mechanisms (hormone imbalance). 7. Formation of irreversible bronchial obstruction under the influence of recurrent infection. Сlassification of bronchial asthma Degree of severity Course І Intermittent course ІІ Persistent course ІІІ mild ІV moderate severe Intermittent asthma Attacks are short and mild day <1 time a weak night ≤2 times a month Between attacks symptoms are abcent Persisting asthma mild Symptoms are permanent but short day <1 time a weal but not more than 1 time a day night =1-2 times a month moderate Symptoms are premanent day permanently night > 1 time a weak Limitation of physical activity Night is deranged severe day Permanent long attacks night Limitation of physical activity Exacerbations may be dangerous for patient’s life Diagnosis: Intermittent bronchial asthma, m,ild degree of exacerbation, respiratory insufficiency 0 degree. Clinical pattern: complaints Attacks of expiratory dyspnea Tightness in the chest Dry cough General weakness, dizziness Clinical pattern Inspection Forsed position of a patient – orthopnoe Skin is pale Respiration cyanotic later (10-12 per min) Wheezes Swelling of neck veins Mouth is opened Viscous white transparent sputum Inspection of a chest Inspiratory position Participation of additional respiratory muscles in respiration palpation Intercostal spaces are wide Vocal fremitus is weakened The chest is rigid Percussion Bundbox sound Upper and lower borders of the lungs are diaplaced upward and downward Respiratory mobility of lungs lower borders is markedly limited Appearance of a patient during attack of asthma Auscultation (before expectoration of sputum) Weakened vesicular breathing Prolonged expiration Dry whistling (high-pitched) rales Auscultation (during expectoration of sputum) Amount of Amount of high-pitched rales decreases low-pitched rales increases Appearance of moist rales Laboratory diagnostics in exacerbation Blood: Moderate lymphocytosis eosinophilia Sputum: eosinophils Charkot-Leyden crystals Kurshmann’s spirals Дослідження харкотиння Instrumental diagnostics Investigation of external respiratory function І. Spyrography FEV1 < 80% Tiffneu index ( FEV1 /VLC, %) ІІ. Pneumotachymetry Of expiratory force In tests with bronchodilators, reverse bronchial obstruction is determined. спірограма Instrumental diagnostics Investigation of external respiratory function ІІІ. Peak -fluometry (analysis of peak volumetric velocity of forced expiration) Chest X-ray in asthma X-ray hypertranslucencv of lung fields. Widened intercostal spaces Low fiat diaphragm Increased retrosternal translucency Narxow vertical heart Large hilar shadows Diminished peripheral vascular pattern Chest X-ray in bronchial asthma increased lung transparency horizontal placement of ribs expansion of intercostal spaces low position if the diafragm X-ray shows pulmonary emphysema Endoscopic findings: hyperemia, edema of bronchial mucosa, hypersecretion Allergic tests allow to determine allergens Positive reaction Principles of asthma treatment I. Etiological ІІ. Pathogenetic Etiological 1. Elimination therapy Pathogenetic 1. Influence on the immunological phase specific hyposensitization nonspecific hyposensitization - fasting diet - treatment with histoglobulin - treatment with glucocorticoids - immunomodulatory therapy 2. Influence on the pathochemical phase • mast cell stabilizers (ketotifen) • leuktriene inhibitors (Montelucast) • protease inhibitors • antioxidant therapy Influence on the pathophysiological phase bronchodilators adrenergic receptor stimulants M-cholinoblockers phosphodiesterase inhibitors Ca ++ antagonists Antispasmodics expectorants Usage of inhaler Solotvino (salt caves) Physiotherapeutic treatment • aerosol therapy • electrophoresis (with bronchodilators) • ultrasound • halotherapy • therapeutic massage • barotherapy • breathing exercises • acupuncture Resort treatment Physiotherapy Climatotherapy SOFT WARM DRY CLIMATE WITHOUT SHARPY WEATHER CHANGES MOUNTAIN LOCATION (900 - 1000 m ABOVE SEA LEVEL) COASTAL RESORTS WITH LOW HUMIDITY Chronic obstructive pulmonary disease A primary chronic inflammatory disease with predominant lesions of the distal airways and lung parenchyma, formation of emphysema with development of incompletely reversible or irreversible bronchial obstruction caused by a pathological inflammatory reaction Types of bronchitis Acute bronchitis: This is the more common one. Symptoms last for a few weeks, but it doesn’t usually cause any problems past that. Chronic bronchitis: exacerbations are observed for 2 and more years. Total duration of exacerbation p;eriod is more than 2 weeks annulary Chronic obstructive pulmonary disease (COPD) The common combination of chronic bronchitis and emphysema has been termed chronic obstructive airways disease (COAD) or chronic obstructive pulmonary disease (COPD). This is a morbid condition characterized by irreverseble bronchial obstruction caused by deformation and sclerosis of bronchial tree due to persistent inflammation. Up to 20% of adults worldwide have the disease, and this proportion is higher in heavily industrialized countries. Chronic bronchitis occurs in the majority of heavy smokers (at least 80% of smokers). It is the third most common cause of death in men over 65 years (60 per 100.000), and is more common in men (8%) than women (3%). Risk-factors of COPD External • long-term smoking or passive smoking • industrial and domestic harmful substances • infections • low socio-economic state (food restrictions, overcoolings, harmful habits) Internal Genetical predisposition (inherited deficiency of - α1-antitripsine) Bronchial hyperreactivity Hypoplasia of the lungs Pathological mechanisms Disorders of functional activity of ciliated epithelium Change of sputum viscosity Immunodepression (deranged cellular and humoral defence) Air pollutants inactivate α1-antitripsine and inhibitor of elastase. Clinical pattern Complaints Cough (usually with mucopurulent sputum) Dyspnoe (constant expiratory) General inspection In later stage – diffuse cyanosis, jugular veins swelling Inspection of a chest Emphysematous chest Protrusion of supra- and infraclavicular fossa Participation of additional respiratory muscles Palpation Rigid chest, diffusely weakened vocal fremitus Percussion • Hyperresonant sound • Displacement of the upper border of the lungs up • Shifting the lower border of the lungs down • Expansion of Kroenig’s area Auscultation •Weakened vesicular breathing with prolonged expiratory phase •Dry rales (wheezes) Instrumental examination External respiratory function FEV1 < 80% Tiffneu index < 70% Spyrometry (determination of FEV1, VLC, FVLC) Tests with bronchodilators (Salbutamol test) shows low reversibility of bronchial obstruction. Stages of COPD GOLD 1: Mild GOLD 2: Moderate GOLD 3: Severe GOLD 4: Very severe Group A: Low risk, less symptoms Group B: Low risk, more symptoms Group C: High risk, less symptoms Group D: High risk, more symptoms Stages of COPD 1 – chronic bronchitis, pneumosclerosis (including bronchial walls) Stage 2 – pulmonary emphysema Stage 3 – Chronic right-ventricular failure Stage Stage 1 -- Mild -- FEV-1 ≥80%: You may have no symptoms. You might be short of breath when walking fast on level ground or climbing a slight hill. Stage 2 -- Moderate -- FEV-1 50-79%: If you’re walking on level ground, you might have to stop every few minutes to catch your breath. Stage 3 -- Severe -- FEV-1 30-49%: You may be too short of breath to leave the house. You might get breathless doing something as simple as dressing and undressing. Stage 4 -- Very Severe -- FEV-1 ≤30%: You might have lung or heart failure. This can make it hard to catch your breath even when you’re resting. You might hear this called end-stage COPD. Treatment Smoking cessation. Bronchodilators (Salbutamol) Corticosteroids, NSAIDs Combinations of bronchodilators and corticosteroids (Seretid, Simbicort) Oxygen Antibiotics (amoxivullin, cefaosporines) Expectorants (lasolvan) Sanation bronchosclpy and surgical removal of large bullae may be occasionally helpful. Oxygen therapy Thank you for your attention! Treatment The most important step in management is to persuade the patient to stop smoking. Bronchodilators may achieve some reversal of airways obstruction Corticosteroids have a role in some patients. Surgical removal of large bullae is occasionally helpful. Oxygen is usually given via nasal cannulae. Occasionally transtracheal oxygen therapy (TTOT) via a small polyethylene catheter introduced directly into the trachea. Long-term oxygen therapy from cylinders or an oxygen concentrator may be of value in patients with chronic stable respiratory failure. The flow rate and concentration are adjusted to relieve arterial hypoxaemia while avoiding carbon dioxide narcosis. Infections are frequent, and it is important to educate patients in the early recognition of symptoms and signs, for example change of sputum colour and quality, fever or increasing wheeze. Many patients should be given a supply of antibiotics to keep at home for selfmedication. Bronchoscopy is used if it is necessary ДЯКУЮ ЗА УВАГУ