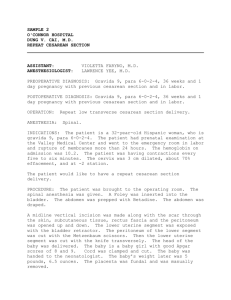
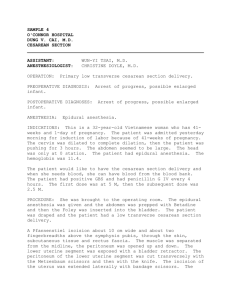
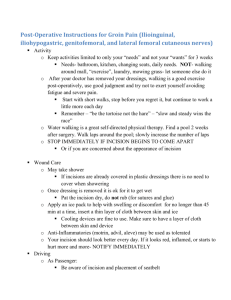
CESAREAN SECTION Name-Vishnu Kumar Bairwa Roll no.-132 DEFINITION It is an operative procedure whereby the fetuses after the end of 28th weeks are delivered through an incision on the abdominal and uterine walls. This excludes delivery through an abdominal incision where the fetus, lying free in the abdominal cavity following uterine rupture or in secondary abdominal pregnancy. INDICATION Time of operation Elective Operation is done at a prearranged time during pregnancy. Emergency When the operation is to be done due to an acute obstetric emergency (fetal distress). A time interval of 30 minutes between the decision and delivery is taken as reasonable Types of operation Lower segment cesarean section(LSCS) In this operation, the extraction of the baby is done through an incision made in the lower segment through a transperitoneal approach. Classical or upper segment CS In this operation, the baby is extracted through an incision made in the upper segment of the uterus. Lower segment cesarean section(LSCS) PREOPERATIVE PREPARATION Informed written permission for the procedure, anesthesia and blood transfusion is obtained. „ • Abdomen is scrubbed with soap and nonorganic iodide lotion. • Premedicative sedative must not be given. „ • Nonparticulate antacid (sodium citrate) is given orally to neutralize the gastric acid. „ • Ranitidine (H2 blocker) 150 mg is given orally night before (elective procedure) and it is repeated (50 mg IM or IV) 1 hour before the surgery to raise the gastric pH. „ • The stomach should be emptied. „ • Metoclopramide (10 mg IV) is given to increase the tone of the lower esophageal sphincter as well as to reduce the stomach contents. • Bladder should be emptied by a Foley catheter. • FHS should be checked once more at this stage. • Cross matching of blood for transfusion. • Prophylactic antibiotics should be given (IV) before making the skin incision • •IV cannula: Sited to administer fluids (Ringer’s solution, 5% dextrose). • • Position of the patient:The patient is placed in the dorsal position. In susceptible cases, to minimize any adverse effects of venacaval compression, a 15° tilt to her left using a wedge till delivery of the baby should be done. • • Anesthesia—may be spinal, epidural or general. • Antiseptic painting:The abdomen is painted with 7.5% povidone-iodine solution or savlon lotion and to be properly draped with sterile towels. I•ncision on the abdomen 1) Vertical incision may be infraumbilical midline or paramedian. 2) Transverse incision, modified Pfannenstiel is made 3 cm above the symphysis pubis. Packing: • The doyen’s retractor is introuced. The peritoneal cavity is now packed off using two taped large swabs. • The tape ends are attached to artery forceps. This will minimize spilling of the uterine contents into the general peritoneal cavity. Uterine incision (A) Lower segments transverse (B) Lower segment vertical (C) “J” incision (D) Classical incision (E) Inverted T incision Steps of LSCS (A) The loose peritoneum on the lower segment is cut transversely (B) A short incision is made in the midline down to the membranes (C) The incision of the lower segment is being enlarged using index fnger of both hands (D) Sagittal section showing insinuation of the fingers between the lower uterine flap and the fetal head until the posterior surface is reached (E) Methods of delivery of the head (F) Placenta is being delivered (G) Inserting the continuous catgut (No. ‘0’) suture taking deeper muscles excluding the decidua (H) Similar method of continuous suture taking superficial muscles and fascia down to the first layer of suture (I) Continuous peritoneal catgut suture • • • • • • • • CLASSICAL CESAREAN SECTION This is relatively easy to perform. Abdominal incision is always longitudinal (paramedian) and about 15 cm (6") in length, 1/3rd of which extends above the umbilicus. A longitudinal incision of about 12.5 cm (5") is made on the midline of the anterior wall of the uterus starting from below the fundus. The incision is deepened along its entire length until the membranes are exposed which are punctured. The baby is delivered commonly as breech extraction. Intravenous oxytocin 5 IU IV (slow) or methergine 0.2 mg is administered following delivery of the baby. The uterus is eventrated. The placenta is extracted by traction on the cord or removed manually Suture of the uterine incision • The uterus is sutured in three layers. ‹ • A continuous suture is placed with chromic catgut No “0” or vicryl taking deep muscles excluding the decidua. ‹ • A second layer of interrupted sutures (1 cm apart) using chromic catgut No. “1” or vicryl taking the entire depth of superficial muscles down to the first layer of suture. ‹ • The third layer of continuous suture taking the peritoneum with the adjacent muscles using chromic catgut No “0” and round-bodied needle. The uterus is returned back into the abdominal cavity. Packings are removed. peritoneal toileting is done and the abdomen is closed in layers. POSTOPERATIVE CARE First 24 hours: (Day 0) „ Observation for the frst 6–8 hours is important. Monitor vitals,amount of vaginal bleeding and behavior of the uterus. Fluid: Sodium chloride (0.9%) or Ringer’s lactate drip is continued until at least 2.0–2.5 L of the solutions are infused. Blood transfusion is helpful in anemic mothers. Oxytocics: Injection oxytocin 5 units IM or IV (slow) or methergine 0.2 mg IM is given and may be repeated. „ Prophylactic antibiotics (cephalosporins, metronidazole) for all cesarean delivery is given for 2–4 doses. Analgesics in the form of pethidine hydrochloride 75–100 mg is administered and may have to be repeated. „ Ambulation:She is encouraged to move her legs and ankles and to breathe deeply to minimize leg vein thrombosis and pulmonary embolism. „ Baby is put to the breast for feeding after 3–4 hours when mother is stable and relieved of pain • Day1: Oral feeding in the form of plain or electrolyte water or raw tea may be given. Active bowel sounds are observed by the end of the day. • Day2: Light solid diet of the patient’s choice is given. Bowel care: 3–4 teaspoons of lactulose is given at bed time, if the bowels do not move spontaneously. Day 5 or day 6: The abdominal skin stitches are to be removed on the D-5 (in transverse) or D-6 (in longitudinal). Discharge • The patient is discharged on the day following removal of the stitches, if otherwise fit. • Usual advices like those following vaginal delivery are given. • Depending on postoperative recovery and availability of care at home, patient may be discharged as early as third to as late as seventh postoperative days. COMPLICATIONS OF CESAREAN SECTION The complications are related either due to the „ operations (inherent hazards)‚ or due to „anesthesia. The complications are grouped into o Maternal • o Fetal The maternal complications may be o Intraoperative „ o Postoperative INTRAOPERATIVE COMPLICATIONS • • Extension of uterine incision involve the uterine vesssel to cause severe hemorrhage, may lead to broad ligament hematoma formation. • • Uterine lacerations at the lower uterine incision—may extend laterally or inferiorly into the vagina. • • Bladder injury • Ureteral injury • Gastrointestinal tract injury • • Hemorrhage may be due to uterine atony or uterine lacerations.• • Morbid adherent placenta (placenta accreta):Total hysterectomy is often needed for such a case to control hemorrhage. POSTOPERATIVE COMPLICATIONS MATERNAL 1) Immediate • 2) Remote IMMEDIATE „ Postpartum hemorrhage Shock Anesthetic hazards Infections Intestinal obstruction Deep vein thrombosis and thromboembolic disorder Wound complications: Abdominal wound sepsis is quite common. i. sanguineous or frank pus ii. hematoma iii. dehiscence (peritoneal coat intact) iv. burst abdomen (involving the peritoneal coat) REMOTE: • Gynecological: Menstrual excess or irregularities, chronic pelvic pain or backache. General surgical: Incisional hernia, intestinal obstruction due to adhesions and bands. Future pregnancy: There is risk of scar rupture FETAL: (1) asphyxia may be preexisting (2) RDS (3) prematurity (4) infection and (5) intracranial hemorrhage