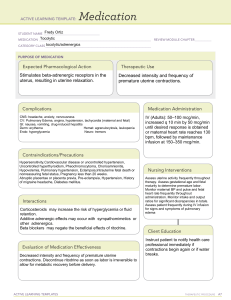
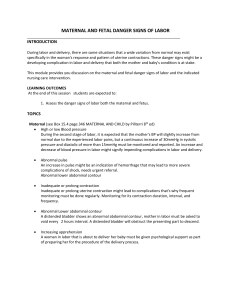
Chapter 19 09-15-2021 Nursing Care During Labor and Birth Learning Objectives Differentiate between the different stages and phases of labor. The first stage of labor begins with the onset of regular uterine contractions and ends with complete cervical effacement and dilation. The latent phase extends from the onset of labor— characterized by regular, painful uterine contractions that cause cervical change—to the beginning of the active phase, when cervical dilation occurs more rapidly. The active phase is defined as the period during which the greatest rate of cervical dilation occurs, which begins at 6 cm and ends with complete cervical dilation at 10 cm The second stage of labor is the stage at which the infant is born. It begins with full cervical dilation (10 cm) and complete effacement (100%) and ends with the baby’s birth The second stage of labor comprises two phases: the latent phase and the active pushing phase. The latent phase, sometimes referred to as delayed pushing, laboring down, or passive descent, is a period of rest and relative calm. During the active pushing (descent) phase the woman has strong urges to bear down, as the Ferguson reflex is activated when the presenting part presses on the stretch receptors of the pelvic floor. Define the physical findings indicative of each stage and phase of labor. First Stage: Early Phase First Stage: onset of regular contractions to full dilation and effacement. Length varies. Early Phase: Duration: nulliparous (first time mom) and multiparous (having borne more than one child) women progress at similar rates. Cervical Dilation: 0-5 cm. Contractions: Mild: mild to moderate by palpation, 2-30 minutes with irregular frequency, and 30-40 seconds long. Patient is typically excited, talkative, with low anxiety. The purpose of this phase is effacement and dilation of cervix. Early Phase: Nursing Care Ambulation as tolerated. Nothing by mouth except ice chips. Pain medication as ordered. 1000 ml. D5W I.V. when active to maintain hydration and emergency access. Catheterize prn because a full bladder can interfere with fetal descent. Monitor fetal heart rate with external fetal monitor. Is it intermittent or continuous? Assess maternal vital signs, fetal heart rate, & contraction pattern every 30-60 minutes and temp every 2-4 hours. Perform vaginal exam as needed. Encourage relaxation measures for pain relief. Teach or review breathing techniques. Encourage woman to ambulate and change position frequently. Encourage woman to void every 2 hours. Support Person: Nurse needs to support the support person also. Let them know: Don’t panic. Know that their presence is helpful. Keep the support person informed of progress. Don’t take woman’s comments/behaviors personally. Assist woman to ambulate in the hall. Encourage woman that she is doing a good job. Provide comfort measures and stay involved. Keep woman informed of her progress. First Stage: Active Phase Duration: multiparous women progress more rapidly than nulliparous women. Dilation: period where greatest rate of cervical dilation occurs; begins at 6 cm and ends with complete cervical dilation at 10 cm. Contractions: Moderate: strong, 1.5-5 minutes apart, 40-90 seconds long. Patient becomes more serious, less extroverted, more restless. Difficulty following directions. Bloody show increases. Active Phase: Nursing Care: Stay in bed? If so, encourage position changes. Support person can help with relaxation techniques. Teach her to move to a faster rate of breathing. Start I.V. fluids. Continue to assess maternal vital signs, contraction pattern and fetal heart rate. Obtain maternal vital signs every 1530 minutes. Obtain temperature every 2-4 hours. Temperature varies if membranes are intact or ruptured. Assess contraction pattern every 15-30 minutes. Assess fetal heart rate every 15-30 minutes. Perform vaginal exam as needed. Administer pain medications as ordered. Active Phase She experiences urge to push. She becomes frustrated, irritable, and doubts her ability to continue. She may experience nausea and vomiting. She may hyperventilate. THIS is the most difficult phase of labor. Active Phase: Nursing Care: Assist with nonpharmacologic pain relief measures or administer pain medication as ordered. Assure her that what she feels is the fetal head. Continue to assess maternal vital signs, fetal heart rate and contractions every 15-30 minutes. Teach the couple that what she is experiencing is normal. Assist her with position changes. Encourage her to void every 2 hours. Provide emotional support and encouragement. Provide positive reinforcement of her efforts. Second Stage of Labor: Active Pushing Phase Duration: Begins with complete dilation and effacement of the cervix and ends with delivery of the infant; average length of time varies. Contractions: Intensity: Significant increase becoming overwhelmingly strong and expulsive; strong by palpation. Frequency: every 2-3 minutes progressing to every 1-2 minutes. Duration: 90 seconds. Purpose is to deliver the infant. She may experience an increased urge to bear down. She may describe pain as a ring of fire (burning sensation of acute pain as vagina stretches and fetal head crowns). Expresses feeling of powerlessness. She may have difficulty following directions. Alters respiratory pattern: has short 4- to 5-sec breath holds with regular breaths in between 5 and 7 times per contraction. Frequent repositioning. Often shows excitement immediately after birth of head. Second Stage: Nursing Care: Monitor maternal vital signs every 5-30 minutes. Assess fetal heart rate every 5-15 minutes. Encourage her to push when she feels like pushing. When pushing, have her do open-glottis pushing and teach her to take 1 cleansing breath before pushing. Provide a calm environment. Assist her in changing positions. Keep couple informed about progress. Offer mirror to watch the birth. Describe maternal behavior and appearance during each stage and phase of labor. First Stage – Early Phase: Patient is typically excited, talkative, with low anxiety. First Stage – Active Phase: Patient becomes more serious, less extroverted, more restless. Difficulty following directions. Bloody show increases. Active Phase: She may experience an increased urge to bear down. She becomes frustrated, irritable, and doubts her ability to continue. She may experience nausea and vomiting. She may hyperventilate. THIS is the most difficult phase of labor. Second Stage – Active Pushing Phase: She may experience an increased urge to bear down. She may describe pain as a ring of fire (burning sensation of acute pain as vagina stretches and fetal head crowns). Expresses feeling of powerlessness. She may have difficulty following directions. Alters respiratory pattern: has short 4- to 5-sec breath holds with regular breaths in between 5 and 7 times per contraction. Frequent repositioning. Often shows excitement immediately after birth of head. She experiences urge to push. Differentiate between true and false labor. True or False Labor? True Labor: regular frequency, becomes stronger and longer occurring closer together, felt in lower abdomen and lower back, becomes more intense with walking, and bloody show present. False Labor: Braxton-Hicks are painless and intermittent and can occur after 4 months gestation. False labor: irregular frequency, felt in upper abdomen and upper back, stops with walking, and no bloody show present. Explain how to measure frequency, duration, and intensity of contractions. Nurse measures, palpates, and times contractions: Frequency: How often uterine contractions occur; the time that passes from the beginning of one contraction to the beginning of the next contraction. Intensity: The strength of a contraction at its peak. Duration: The time that passes between the onset and the end of a contraction. Resting tone: The tension in the uterine muscle between contractions; relaxation of the uterus. Palpation: Mild: Slightly tense fundus that is easy to indent with the fingertips (feels like pressing a finger to the tip of the nose). Moderate: Firm fundus that is difficult to indent with the fingertips (feels like pressing a finger to the chin). Strong: Rigid, board-like fundus that is almost impossible to indent with the fingertips (feels like pressing a finger to the forehead). Carry out appropriate nursing assessments during the progress of labor. Admission Obtain a pregnancy history--this pregnancy, past pregnancies, and births. Cultural Assessment Perform a vaginal exam. It is a sterile procedure and assesses the cervical effacement (percent), dilation (centimeters), fetal presentation and position (feeling a hard head or a squishy bum), and status of membranes (bag of water). When to perform during labor? Do it whenever it is needed. Do not want to do it unless it is necessary especially if her membranes have ruptured (water has broken) due to risk of infection. Perform Leopold maneuvers by palpation of abdomen and assess fetal presentation and lie. Obtain baseline maternal vital signs and fetal heart rate. 20–30-minute baseline fetal heart rate. Ask if she has noticed any vaginal bleeding or mucus drainage. Ask when she last ate? Are membranes (bag of water) ruptured? Spontaneous rupture of membranes (SROM)—has she felt trickle or gush of fluid? Test amniotic fluid with nitrazine (pH) paper. If there is amniotic fluid the paper will turn blue. If there is none present, the paper will stay yellow. What time did membranes rupture? Active red vaginal bleeding is NOT a normal, expected finding. A pinkishreddish mucus is normal and expected. Assessing Contractions Contractions on the monitor will look like waves or hills. Assess before contraction and during contraction. Assess uterine activity regarding its effect on cervical effacement and dilation and on the degree of descent of the presenting part. Consider the effect of uterine activity on the fetus. Maternal vital signs, FHR, and uterine activity. Obtain 20–30-minute baseline assessment. Wave-like pattern, frequency (how often is she having a contraction), duration (how long is each contraction), intensity (how strong are the contractions)—MUST palpate abdomen (fundus) during contraction to determine whether the contraction is mild (feels like your nose, can wiggle a little), moderate (feels like your chin, harder but still wiggles a little), or severe (feels like your forehead, hard with no wiggle). Mild: slightly tense fundus that is easy to indent with the fingertips (feels like pressing a finger to the tip of the nose). Moderate: Firm fundus that is difficult to indent with the fingertips (feels like pressing a finger to the chin). Strong: Rigid, board-like fundus that is almost impossible to indent with the fingertips (feels like pressing a finger to the forehead). Rupture of Membranes TACO Nursing Interventions T= Time: What time did they rupture? A = Amount: Was it a gush or a trickle. C = Color: The color of a fluid, clear-ish cloudy with white specks in it. Cloudiness does not indicate infection; it is supposed to be cloudy. We do not want green color. O = Odor: Cannot describe it but has its own smell. Foul odor indicates infection. Check fetal heart rate immediately. Perform sterile vaginal exam. IF you assess her and you can feel the cord, you are going to push the baby’s head off the cord, calmly call for help, and STAY there with fingers in place to hold the baby up off the cord. You will get on the bed and the team will wheel you and mom to the OR to deliver via c-section. You will stay in position through the preparation process, draping process, and all the way until the surgeon gets the baby out. Then you can get out from under the draping and leave. Note time of rupture. Inspect the color of amniotic fluid. Continue to check woman’s temp every 2 hours until delivery. First Stage: Early Phase: Nursing Assessment: Monitor fetal heart rate with external fetal monitor. Is it intermittent or continuous? Assess maternal vital signs, fetal heart rate, & contraction pattern every 30-60 minutes and temp every 2-4 hours. Perform vaginal exam as needed. First Stage: Active Phase: Nursing Assessment: Continue to assess maternal vital signs, contraction pattern and fetal heart rate. Obtain maternal vital signs every 15-30 minutes. Obtain temperature every 2-4 hours. Temperature varies if membranes are intact or ruptured. Assess contraction pattern every 15-30 minutes. Assess fetal heart rate every 15-30 minutes. Active Phase: Nursing Assessment: Continue to assess maternal vital signs, fetal heart rate and contractions every 15-30 minutes. Second Stage: Nursing Assessment: Monitor maternal vital signs every 5-30 minutes. Assess fetal heart rate every 5-15 minutes. Third Stage: Nursing Assessment: Obtain APGAR scores and perform brief assessment of infant. Assess maternal vital signs every 15 minutes. Fourth Stage of Labor: Nursing Assessment: Assess maternal vital signs, fundus, and lochia every 15 minutes during the first hour. Massage fundus if boggy. Assess perineum for swelling or bruising. Assess bladder for distention and encourage voiding. Implement appropriate nursing interventions during all stages of labor. First Stage: Early Phase: Nursing Care Ambulation as tolerated. Nothing by mouth except ice chips. Pain medication as ordered. 1000 ml. D5W I.V. when active to maintain hydration and emergency access. Catheterize prn because a full bladder can interfere with fetal descent. Encourage relaxation measures for pain relief. Teach or review breathing techniques. Encourage woman to ambulate and change position frequently. Encourage woman to void every 2 hours. Support Person: Nurse needs to support the support person also. Let them know: Don’t panic. Know that their presence is helpful. Keep the support person informed of progress. Don’t take woman’s comments/behaviors personally. Assist woman to ambulate in the hall. Encourage woman that she is doing a good job. Provide comfort measures and stay involved. Keep woman informed of her progress. First Stage: Active Phase: Nursing Care: Stay in bed? If so, encourage position changes. Support person can help with relaxation techniques. Teach her to move to a faster rate of breathing. Start I.V. fluids. Perform vaginal exam as needed. Administer pain medications as ordered. Active Phase: Nursing Care: Assist with nonpharmacologic pain relief measures or administer pain medication as ordered. Assure her that what she feels is the fetal head. Teach the couple that what she is experiencing is normal. Assist her with position changes. Encourage her to void every 2 hours. Provide emotional support and encouragement. Provide positive reinforcement of her efforts. Second Stage: Nursing Care: Encourage her to push when she feels like pushing. When pushing, have her do open-glottis pushing and teach her to take 1 cleansing breath before pushing. Provide a calm environment. Assist her in changing positions. Keep couple informed about progress. Offer mirror to watch the birth. Third Stage: Nursing Care Encourage woman to bear down to deliver placenta. Place infant on woman’s chest and cover with warm blanket. Administer oxytoxic drugs as ordered. Oxytocin Place ID bands on infant, mom & support person. Initiate breastfeeding. Fourth Stage of Labor: Nursing Care Assist with breastfeeding if appropriate. Reassure her that her behavior during labor and delivery was acceptable. Offer something to drink or eat. Chapter 18 09-22-2021 Fetal Assessment During Labor Objectives Differentiate between external and internal fetal monitoring. External Monitoring Ultrasound transducer: High-frequency sound waves reflect mechanical action of the fetal heart. Noninvasive. Does not require rupture of membranes or cervical dilation. Used during both the antepartum and intrapartum periods. Fetal Heart Tones. Toco-transducer: Monitors frequency and duration of contractions by means of a pressuresensing device applied to the maternal abdomen. Used during both the antepartum and intrapartum periods. Contractions. Internal Monitoring Spiral Electrode: Converts the fetal electrocardiogram as obtained from the presenting part to the fetal heart rate via a cardiotachometer. Can be used only when membranes are ruptured, and the cervix is sufficiently dilated during the intrapartum period. Electrode penetrates into the fetal presenting part by 1.5 mm and must be attached securely to ensure a good signal. Measures fetal heart tones (FHTs). Intrauterine Pressure catheter (IUPC): Monitors the frequency, duration, and intensity of contractions. The two types of IUPCs are a fluid-filled system and a solid catheter. Both measure intrauterine pressure at the catheter tip and convert the pressure into millimeters of mercury on the uterine activity panel of the strip chart. Both types can be used only when membranes are ruptured, and the cervix is sufficiently dilated during the intrapartum period. Measures intensity of contractions. Identify ranges for normal fetal heart rate, tachycardia, and bradycardia. Normal Parameters Fetal Heartrate: Normal Range: 110-160 beats/minute. Average rate during a 10-minute period: Round to the nearest 5. Tachycardia: greater than 160 beats/minute lasting longer than 10 minutes. Bradycardia: less than 110 beats/minute lasting longer 10 minutes. Define the four categories of variability. Variability: beat to beat irregular waves or fluctuations in baseline fetal heart rate of 2 cycles per minute or greater. Does not include accelerations or decelerations of FHR. Measure of fetal wellbeing. The four categories of variability are absent, minimal, moderate, and marked. Absent variability is defined as an amplitude range of the FHR fluctuations that is not detectable to the unaided eye. Minimal variability has an amplitude range that is detectable to the unaided eye but is less than 5 beats/min. Depending on other characteristics of the FHR tracing, absent or minimal variability is classified as either abnormal or indeterminate. It can result from fetal hypoxemia and metabolic acidemia. Other possible causes of absent or minimal variability include fetal sleep cycles, fetal tachycardia, extreme prematurity, medications that cause CNS depression, congenital anomalies, and preexisting neurologic injury. Moderate variability, with an amplitude range of 6 to 25 bpm, is considered normal. Its presence reliably predicts a normal fetal acid–base balance (absence of fetal metabolic acidemia). Moderate variability indicates that FHR regulation is not significantly affected by fetal sleep cycles, tachycardia, prematurity, congenital anomalies, preexisting neurologic injury, or CNS depressant medications. The significance of marked variability, with an amplitude range ≥ 25 bpm, is unclear. In many cases, it likely represents a normal variant. Differentiate between Category I and Category III Fetal Heart Rate in the Three-Tier System. Category I: Baseline rate: 110-160 bpm, Baseline FHR variability: moderate, Accelerations: present or absent, Early decelerations: present or absent, No late or variable decelerations. Category III: Absent baseline variability and any of the following: Recurrent late decelerations, Recurrent variable decelerations, Bradycardia. Sinusoidal pattern: (i.e., a regular smooth, undulating wavelike pattern) is not included in the definition of FHR variability. This uncommon pattern classically occurs with severe fetal anemia. Variations of the sinusoidal pattern have been described in association with chorioamnionitis, fetal sepsis, and administration of opioid analgesics. Compare and contrast cause, pattern, and nursing interventions for accelerations, early, late, and variable decelerations. Acceleration Abrupt increase in FHR above baseline. 15 bpm above baseline that lasts greater than 15 seconds. Fetus less than 32 weeks gestation – 10 bpm increase lasting greater than 10 seconds. Can be periodic or episodic and may occur in association with fetal movement or spontaneously. Reassuring Sign: Fetal Well-being. Causes: Fetal movement, Sterile vaginal exam, Fundal pressure: transient compression of the umbilical vein, resulting in decreased fetal venous return and a reflex rise in heart rate. Early Deceleration Gradual decrease in FHR in response to head compression. Sterile vaginal exam, Contractions & fundal pressure, or Second stage of labor. Benign finding. “Mirror image” of the contraction. Nursing Interventions: None. Late Deceleration Gradual decrease in FHR in response to uteroplacental insufficiency. Deceleration begins after contraction has started and return to baseline after contraction ends. Nursing Interventions: Discontinue oxytocin, Place woman in lateral position, Start O2 at 8-10 L/min by nonrebreather face mask, and Increase IV fluids. Variable Deceleration Abrupt decrease in FHR of greater than 15 bpm lasting at least 15 seconds caused by compression of umbilical cord. Can occur anytime during contraction. Transition phase and Second Stage of labor. Shape: U, V, W Nursing Interventions: Discontinue oxytocin, Change maternal position, O2 at 8-10 L/min, Assess for prolapsed cord, and Assist with amnioinfusion. Implement nursing interventions in the management of fetal distress. Management of Abnormal FHR Patterns Basic: Oxygen per facemask 8 – 10 L/min, Side-lying position, Increase IV fluids. Maternal hypotension: Increase IV fluids, Lateral position. Uterine Hyperstimulation (Tachysystole): Decrease or discontinue oxytocin. During second stage of labor: Decrease pushing, Open glottis pushing. Fetal Assessment and Interventions Interventions for Fetal Distress: Amnioinfusion: infusion of room temperature isotonic fluid into the uterine cavity. Relieve pressure on the umbilical cord. Tocolytic therapy: Medications that relax the uterine muscle and inhibit uterine contractions. Chapter 17 09-24-2021 Nonpharmacologic Pain Management Objectives Explain factors that affect an individual’s perception of and response to pain. What the woman chooses or how she chooses to manage her pain is completely up to her. Everybody is very individualized and has a different way. Some women want to feel every contraction, know that they worked through that labor, and had their baby naturally. Other women are not interested in feeling any of the pain or contractions and get an epidural as soon as they can get one. And that is fine. It is their personal choice. Pain During Labor and Birth Everyone perceives and reacts to pain differently. Perception of pain is subjective defined completely by the person who is experiencing it. Women vary in how they perceive and cope with labor pain. It is very individualized. How a woman expresses her pain is very different. Perception of pain is influenced by her culture, age, previous personal experience with pain, similarity of pain associated with labor and birth process, desire for natural childbirth, childbirth preparations, and the physical, psychologic, and emotional support available to her. Different cultures express pain differently. Some cultures are very stoic (indifferent or passive) and won’t express if they are in pain or not. They won’t ask for pain assistance. Other individuals are very vocal about their pain. If the woman want to have a natural childbirth or not is a big desire whether to use pain management or use natural, nonpharmacological pain management. Childbirth preparations, such as birthing classes can make a difference. The woman and support person go to a class and receive information about labor and information about how to breathe during their contractions and how to stay relaxed. This works very well for some women. Some women do not find it helpful. Of late, if a woman has already decided she is having an epidural, she will not attend childbirth classes because she will not experience the pain. The women’s support system or support person is very beneficial and important during the labor process. This could be their significant other, a friend, sister, or mother, or a doula. There are many different persons she may want as her support system/person. Expression of pain: vital sign changes (pulse rate, blood pressure, and respiratory rate might increase during pain), pallor (she may have a change in color due to the pain. Some people get pale, and some people turn red, and some people do not change color at all when experiencing pain), diaphoresis (sweating), nausea and vomiting because of pain at times, anxiety (some women become very anxious because they just do not know how to handle the pain), some women become verbal during pain (crying, yelling, screaming, or groaning), writhing (moving around), gesturing, excessive muscular excitability. Even though some women may not tell you they are in pain, there are subjective ways for you to assess if she is in pain. Ask her how you can help her better manage her pain. Factors influencing the pain response: Physiologic factors: how long she is in labor sometimes will affect how she reacts to her pain. The longer she is in labor, the more tired she becomes, and is less tolerant resulting in fatigue, interval and duration contractions (how strong are her contractions and how close together are the contractions), fetal size and position (what position is the baby in-example: if baby is in an occiput posterior position and the back of the baby’s head is pushing on her sacrum with each contraction, she may be in more pain), and release of endorphins (this happens to everyone and is the body’s natural response to pain but sometimes is not enough to handle the pain). Anxiety: commonly associated with increased pain. Mild anxiety is considered normal during labor and birth. As anxiety and fear heighten, muscle tension increases, the effectiveness of uterine contractions decreases, the experience of discomfort increases, and a cycle of increased fear and anxiety begins. This will slow the progress of labor. NOTE: anxiety does NOT increase pain. It just affects how the woman perceives the pain and reacts to it. Previous experience: A first time mother may not have developed effective strategies for coping with the significant pain of labor and birth. An experienced mother may have had difficult and painful births previously and that anxiety and fear may lead to increased pain perception. If a woman had a good experience during labor and birth, she would bring that experience with her and most likely be more relaxed. Discuss the impact of culture on a woman’s response to pain during labor and birth. Culture: women of different cultural backgrounds may react to pain differently. Chinese women may not exhibit reactions to pain, although exhibiting pain during labor and birth is acceptable. They consider accepting something when it is first offered as impolite; therefore, pain interventions must be offered more than once. Acupuncture may be used for pain relief. Arab or Middle Eastern women may be vocal in response to labor pain. They may prefer medication for pain relief. Japanese women may be stoic in response to labor pain, but they may request medication when pain becomes severe. Southeast Asian women may endure severe pain before requesting relief. Hispanic women may be stoic until late in labor, when they may become vocal and request pain relief. African American women may express pain openly. Their response to being offered medication for pain relief varies. Describe nonpharmacologic strategies to enhance relaxation and comfort during labor and birth. Nonpharmacologic Pain Management Factors influencing pain response: Gate-control theory of pain: if you create another stimulus, it interferes with the pain stimulus. Examples include massage, music, imagery. Environment includes setting, stimuli, and equipment. The environment for laboring mothers nowadays is relaxing and welcoming. Equipment is in cabinets and does not remind the mother that something could possibly go wrong during childbirth. Support can include nurse, doula, family member, friend, spouse or partner, etc. In the normal world, i.e., pre-COVID, women were allowed more than one person in the labor and delivery room with them during the childbirth process. A doula is a person who is trained to help a laboring woman manage her pain. They do not have to be a nurse or a healthcare person at all. They have gone through training, and their only focus is helping the laboring mother deal with her pain. They are not a staff member of a hospital. The woman finds the doula on her own; however, some hospitals do have doula systems. So, if a woman comes into the hospital, they may ask, “Would you like a doula?” Sometimes they have an on-call system, and the doula on-call gets called in. They DO NOT provide nursing care; they ONLY help the woman manage her pain naturally. They can be very beneficial. If the woman does not have anyone with her when she comes in, you, as the nurse, becomes her support person. You help her get through her labor. Application of heat and cold: Sometimes women get very hot during labor and like cold packs, or cold wash clothes on their foreheads, the back of their necks, and/or their chests. Other times they may get cold, either during the labor process or from having cold packs on them. A warm blanket may then be applied. Heat: warmed blankets, warm compresses, heated rice bags, a warm bath or shower, or a moist heating pad can enhance relaxation and reduce pain during labor; relieves muscle ischemia (inadequate blood supply) and effective in reducing back pain caused by a posterior presentation or general backache from fatigue. In second-stage labor, application of warm, moist compresses to perineum relieves burning sensation women often feel when fetal head crowns. Cold: cold cloths, frozen gel packs, or ice packs applied to the back, the chest, and/or the face during labor may be effective in increasing comfort when the woman feels warm. May be applied to areas of musculoskeletal pain, reducing the muscle temperature and relieving muscle spasms. Touch and massage: Effleurage: light stroking of abdomen during contraction. Helps distract the woman through her contraction. Typically, it is better for another person to do this because the woman is focused on her contractions and her breathing. Counter Pressure: use a ball or fist. This is very beneficial for the woman whose baby is in an occiput posterior position and the back of the baby’s head is pushing on her sacrum during each contraction, also known as “back labor.” This is very painful for the woman. Another person applies counter pressure during the contraction, and it helps relieve some of that extra pain she is experiencing due to the baby’s position. Water therapy (hydrotherapy): stimulate release of endorphins by a bath or shower. Water can be very calming for some women and help alleviate some of their pain. They may just stand in the shower during the laboring process. Some hospitals have tubs, and the woman can actually submerge in the water during her labor. Some healthcare providers will even let a woman deliver her baby while in the bathtub because water is just that calming. It is okay for the baby because the baby has been floating around for the last several months in fluid. When the baby is in utero, they are not actually breathing with their lungs, everything is provided to the baby through profusion. When the baby is born in the tub, they go from one bag of water to another water, they do not take a breath yet. They don’t take a breath until they are brought up out of the water. So, it can be calming for both baby and mother. Music: can be very calming and relaxing. Very effective during labor. The music that is calming to the person can be VERY different. For some people it may be waves or raindrops but for other people it may be heavy metal music. We all have our different tastes and preferences. Relaxation techniques Focusing and relaxation using distraction and imagery. Distraction: focus on an object. They can bring something with them, they can focus on the thing that means something to them. We are attempting to replace the pain with a different focus. Imagery: think about another place. Imagery is the same as distraction except we are creating a picture in our mind. When she has a contraction, have her close her eyes and imagine a place or think of something that is calming to her. Box 17.2 – Nonpharmacologic Strategies to Promote Relaxation and Reduce Pain: Cutaneous Stimulation Strategies: Counterpressure, Effleurage (light massage), Therapeutic touch and massage, Walking, Rocking, Changing positions, Application of heat or cold, Transcutaneous electrical nerve stimulation (TENS), Acupressure, Water therapy (showers, baths, whirlpool baths), Intradermal water block. Sensory Stimulation Strategies: Aromatherapy, Breathing techniques, Music, Imagery, Use of focal points. Cognitive Strategies: Childbirth education and hypnosis. Implement non-pharmacologic strategies for a woman in labor. Breathing techniques Key Points about breathing: start and end with a cleansing breath. Kind of like yoga. When she feels the contraction start, she takes a nice, deep breath in, and then breathes according to how her contractions are. The key to breathing is, when her labor is mild, her needs to be slow and should kind of match the contraction. As her labor gets more intense, her breathing may become faster. Paced Breathing Techniques Cleansing Breath: relaxed breath in through nose and out through mouth. Used at the beginning and end of each contraction. Slow Breathing: for mild to moderate contractions. Breaths become deeper and longer as intensity of contractions increase, peak, and go away. Slow-Paced Breathing: can be used when contractions are becoming a little more painful. Deep breaths from belly, abdomen rises and falls with each breath, start with a cleansing breath, as contractions peak; short, light breaths in and out of mouth, 6 to 8 breaths per minute: IN-2-34/OUT-2-3-4/IN-2-3-4/OUT-2-3-4, and end with a cleansing breath. Modified-Paced Breathing: 32 to 40 breaths per minute. IN-OUT/IN-OUT/IN-OUT/IN-OUT … Patterned-Paced or Pant-Blow Breathing: Can be used when contractions are more painful and same rate as modified breathing; enhances concentration. Start with a cleansing breath, light, short breaths through mouth; after a few breaths, let out a longer breath. Repeat pattern until contraction is over and end with a cleansing breath. 3:1 Patterned breathing: IN-OUT/IN-OUT/IN-OUT/IN-BLOW 4:1 Patterned breathing: IN-OUT, IN-OUT, IN-OUT, IN-OUT, IN-BLOW Breathe from Rib Cage: Upper Chest Breathing: quick, short breath through nose, when rib cage expands; short breath through mouth. Can add light panting at peak of contraction. Practice breathing before labor. Begin and end contraction with cleansing breath. Start slow and increase pace of breathing as contractions intensify. Assess for hyperventilation. Benefits of Deep Breathing: brings oxygen to muscles and uterus, relieves tension and stress, makes contractions more productive and comfortable, takes your mind off pain and discomfort, and makes time go by faster. Vocalization can be helpful. Inhales are quiet and exhales are vocal. Hyperventilation One problem with the breathing techniques is sometimes the woman gets very caught up in her contractions and she starts breathing faster than she should, resulting in hyperventilation. This is not good because it affects the oxygenation for both mother and baby. We need to know when this is happening. Symptoms include lightheadedness, dizziness, tingling fingers, and numbness around mouth. Intervention: we need them to slow down and rebreathe their CO2 to equalize their respiratory system. Have her breathe into paper bag (do not often have this in the labor room thought) but cupping hands over mouth works just as effectively. Slow breathing rate to regain focus. She needs to breathe from her belly. Shortening her breath leads to hyperventilation. Box 17.1 – Supporting a Woman in Labor: Provide companionship and reassurance. Offer positive reinforcement and praise for her efforts. Encourage participation in distracting activities and nonpharmacologic measures for comfort. Give nourishment (if allowed by obstetric health care provider). Assist with personal hygiene. Offer information and advice. Involve the woman in decision making regarding her care. Interpret the woman’s wishes to other health care providers and to her support group. Create a relaxing environment. Use a calm and confident approach. Support and encourage the woman’s support people by role-modeling labor support measures and providing time for breaks. Chapter 33 & 31 09-27_29-2021 Postpartum Complications Objectives Perineal Trauma, Hemorrhage, Infection, and Postpartum Depression Differentiate between the causes and signs/symptoms of postpartum hemorrhage. Postpartum Hemorrhage (PPH) Definition: Loss of 500 ml of blood after vaginal birth. Loss of 1000 ml after cesarean birth. Leading cause of maternal morbidity and mortality. Often unrecognized until woman has profound symptoms. Postpartum Hemorrhage: Causes Uterine atony: Loss of uterine tone. Excessive bleeding with a boggy uterus. Associated with High parity, Hydramnios, Macrosomic fetus, Multifetal gestation, or Retained placenta. Lacerations of genital tract: Cervix, vagina, perineum. Caused by trauma during labor and delivery. Bleeding with a firm, contracted uterus. Slow trickle to a steady stream of bleeding. Hematoma: Trauma that caused collection of blood in the vaginal canal. Complaint of vaginal pressure and pain. No excessive bleeding noted. Firm uterus. Inversion of the uterus: The uterus turns inside out and protrudes through the cervical opening Postpartum Hemorrhage Early recognition of PPH. PPH is a medical emergency. Differentiate cause of bleeding through assessment questions. 1. Uterus firm or boggy? 2. Distended bladder? 3. Active visual bleeding? 4. Vaginal pressure and pain? Recognize symptoms of hypovolemic shock. Hemorrhagic (Hypovolemic) Shock Emergency situation in which perfusion of organs may become severely compromised and death may occur. Symptoms: increased pulse rate, increased respiratory rate, decreased blood pressure, decreased urinary output, cool, clammy, pale skin, decreased level of consciousness, mood can be anxious or confused. Implement care for a woman experiencing postpartum hemorrhage and hypovolemic shock. Postpartum Hemorrhage Interventions and Treatment: Uterine atony: Massage fundus, Empty bladder, Medications - Oxytocin (Pitocin) 10-20 units IM, Oxytocin (Pitocin) IV infusion: 10-40 units in a Liter of LR or NS, Methylergonovine (Methergine) 0.2 mg IM every 2-4 hours up to 5 doses, 15-methylprostaglandin (Hemabate) 0.25 mg IM every 15-90 minutes up to 8 doses, or Surgery for Retained placenta. Laceration: Suture laceration. Hematoma: Observation. Evacuation & ligation of bleeding vessel. Uterine inversion: Emergency. Reposition uterus into pelvic cavity. If unsuccessful may require hysterectomy. Hypovolemic Shock Interventions and Treatment: Medical Management: Fluid or blood replacement therapy, IV bolus of Lactated Ringers or Normal Saline or Packed RBC, Platelets. Follow Protocol: Monitor pulse and blood pressure. Vital signs every 5 minutes. Foley catheter to monitor output. Oxygen at 10-12 L/min. Pulse oximetry. Identify predisposing factors, symptoms most common causes and implementation of nursing interventions for postpartum infection. Postpartum Infection Clinical infection of the genital tract that occurs after miscarriage, elective abortion, or childbirth. Definition: Fever (38°C/100.4°F) on 2 days during the first 10 postpartum days. 2 consecutive days Not the first postpartum day. Risk factors: Medical conditions that affect healing. Procedures performed that increase risk of infections. Infection: Endometritis Infection of the uterine lining (endometrium). Occurs more often after cesarean birth. Symptoms: Generalized infection symptoms, Pelvic pain *, Foul-smelling, profuse lochia *, Uterine tenderness *. Treatment: IV antibiotics, Pain relief medications, and Rest. Infection: Wound Infection of cesarean incision or episiotomy. Often develops after discharge. Assessment: R: Redness, E: Ecchymosis, E: Edema, D: Drainage, A: Approximation, Patient education. Signs and Symptoms of Infection: Treatment and Antibiotics. Infection: Mastitis Infection in the breast, Unilateral: usually occurs in one breast, Appears in the first 6 weeks postpartum. Symptoms: Generalized infection symptoms, Local breast tenderness*, Redness to breast*. Treatment: Antibiotics, Antipyretics, Rest, Pump frequently. Infection: General Management Prevention: Hand washing. Perineal hygiene: Change peri-pad frequently. Only touch outside surface of peri-pad. Apply peri-pad front to back. Wipe front to back. Breastfeeding Assessment: Proper latch on, position, and removal from breast. Assessments: Lochia, Vital signs, and wound. Teach patient signs & symptoms of infections. Differentiate between postpartum mood disorders. “Baby Blues.” Postpartum Depression without psychotic features. Postpartum Depression with Psychotic features. Onset within 4 weeks of birth. “Baby Blues” Mild depression. Does not interfere with daily functioning. Typically resolve without any interventions. Overwhelmed by parenthood. Mood swings, Periods of sadness, Tearful/crying, No sleep. Postpartum Depression without Psychotic Features: Postpartum Depression (PPD). Intense sadness with severe mood swings. Irritability is a distinguishing symptom. Symptoms: Fear, Anger, Anxiety, Despondency. Sleeping Difficulties. Guilt and feelings of inadequacy. Rejection of infant – May have thoughts of harming infant. Persists past the first few postpartum weeks. Requires medical intervention. Symptoms of Psychosis: Auditory and Visual hallucinations. Paranoid and/or Grandiose delusions. Delirium or disorientation. Extreme deficits in judgment. Disorganized behavior. Risk of suicide or infanticide (Harm themselves or infant). Identify risk factors and symptoms for postpartum mood disorders. History of depression. Before pregnancy or Prenatal depression. Stress of childcare: “Difficult” infant temperament. Unplanned/unwanted pregnancy. Life stress: Lack of social support, Single, Low socioeconomic status, Low self-esteem. Implement a postpartum depression screening tool. Observe interaction between mother and infant. 2 questions to identify women at risk for PPD. “Over the past 2 weeks have you ever felt down, depressed or hopeless?” “Over the past 2 weeks have you felt little interest or pleasure in doing things?” Formal screening tools: Edinburgh Postnatal Depression Scale (EPDS) and Postpartum Depression Screening Scale (PDSS). Outline a plan of care for the client with postpartum depression. Early identification: Observe woman’s behavior for signs of depression. Observe interaction between mom and infant. Discuss PPD with patient and family. Recognize symptoms: Activities to prevent PPD Share knowledge about postpartum emotional problems with close family and friends. At least once each day or every other day, purposely relax for 15 min by deep breathing, meditating, or taking a hot bath. Take care of yourself: eat a balanced diet. Exercise on a regular basis, at least 30 min a day. Sleep as much as possible; make a promise to yourself to try to sleep when the baby sleeps. Get out of the house: try to leave home for 30 min a day; take a walk outdoors or walk at the mall. Share your feelings with someone close to you; don’t isolate yourself at home with the television. Don’t overcommit yourself or feel like you need to be a superwoman. Ask for help from family and friends. Don’t place unrealistic expectations on yourself; no mother is perfect! Be flexible with your daily activities. Go to a new mothers’ support group: for example, take a postpartum exercise class or attend a breastfeeding support group. Nursing Care: Home & Community Follow up assessment: Home visit or follow up phone call. Nurses in pediatrician’s office need to know signs of PPD and assess for them. Family assistance: Childcare, Maid services, Meals on Wheels. Support groups: Postpartum Support International, Depression after Delivery. Referral to Mental Health Therapist: May need to be hospitalized. Medications: Antidepressants and/or Antipsychotics. Assess safety of infant and mother: “Have you thought about hurting your baby?” “Have you thought about hurting yourself?” Suicide Plan in place?