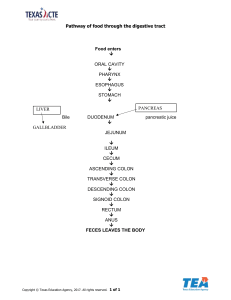
GI review A 52 year old female comes to her physician because of generalized itching, and a recent visit from her sister ended with an embarrassing mention of her eyes looking a little yellow. Laboratory studies show increased direct bilirubin and alkaline phosphatase. A liver biopsy specimen shows granulomatous inflammation centered on on the bile ducts within the portal spaces. Presence of which of the following would best confirm the most likely diagnosis A. B. C. D. E. Antimitochondrial antibioidies Decreased serum ceruloplasmin Elevated liver enzymes Markedly elevated hematocrit PiZZ allele Primary biliary cirrhosis • Autoimmune disease leading to lymphocytic infiltration and formation of granulomas • Destruction of intralobular bile ducts--> can’t excrete conjugated bilirubin • Classically seen in women • Characteristic: antimitochondrial antibodies Contrast with primary sclerosing cholangitis • Primary biliary cirrhosis would appear normal on ERCP imaging PSC would look like beads due to alternating strictures and dilation • While PBC has granulomas, PSC has onion skinning of the bile ducts • PSC is classically in middle aged men • PSC is associated with UC (KNOW. THIS.) • Often p-ANCA positive A 52 year old female comes to her physician because of generalized itching, and a recent visit from her sister ended with an embarrassing mention of her eyes looking a little yellow. Laboratory studies show increased direct bilirubin and alkaline phosphatase. A liver biopsy specimen shows granulomatous inflammation centered on on the bile ducts within the portal spaces. Presence of which of the following would best confirm the most likely diagnosis A. B. C. D. E. Antimitochondrial antibodies Decreased serum ceruloplasmin Elevated liver enzymes Markedly elevated hematocrit PiZZ allele A 52 year old female comes to her physician because of generalized itching, and a recent visit from her sister ended with an embarrassing mention of her eyes looking a little yellow. Laboratory studies show increased direct bilirubin and alkaline phosphatase. A liver biopsy specimen shows granulomatous inflammation centered on on the bile ducts within the portal spaces. Presence of which of the following would best confirm the most likely diagnosis A. B. C. D. E. Antimitochondrial antibodies Decreased serum ceruloplasmin Elevated liver enzymes Markedly elevated hematocrit PiZZ allele B- decrease serum ceruloplasmin: Wilson’s Disease • Mutation in a copper transportation gene on chromosome 13 • Can’t excrete copper into bile properly and incorporate it onto ceruloplasmin (transport protein) • Copper accumulates in liver (cirrhosis), brain (dysarthria, dystonia, tremor) and Descemet membrane of cornea (Kayser Flescher rings) • Classic lab findings: high serum copper (can’t excrete it) and low serum ceruloplasmin • Treat by chelating the copper with pencillamine or trientine D- markedly elevated hematocrit: Hemochromatosis • Recessive mutation in HFE gene which normally sense iron loads and tells the intestine to increase intestinal absorption of iron • Labs: increased ferritin AND iron • Iron accumulates in liver (cirrhosis), pancreas (diabetes), skin (bronze skin), heart (restrictive cardiomyopathy), and joints (arthritis) • Don’t get tripped up and think diabetes classic mimicker on Step. Check if they have weird skin pigmentation or joint pain • Usually doesn’t present until age 40 • Need to treat by repeated phlebotomy E- PiZZ allele: alpha 1 antitrypsin deficiency • Codominant trait that leads to misfolding of antitrypsin protein • Aggregates in liver PAS (pink) globules in liver • Normally should be working in the lungs to inhibit elastase breakdown of the lungs • Dyspnea and liver failure in a younger, previously healthy patient should make you suspicious 34 year old woman comes to the physician because of abdominal fullness and early satiety. She says her bowel habits have not changed recently, but feels she has gotten more constipated over the years. A radiographic series shows a circumferential lesion with associated narrowing of the lumen in her sigmoid colon. A colonoscopy shows over 100 polyps. Mutation in what gene predisposed her to this condition? A. B. C. D. E. 5q21 11p13 13q14 17q11 22q12 34 year old woman comes to the physician because of abdominal fullness and early satiety. She says her bowel habits have not changed recently, but feels she has gotten more constipated over the years. A radiographic series shows a circumferential lesion with associated narrowing of the lumen in her sigmoid colon. A colonoscopy shows over 100 polyps. Mutation in what gene predisposed her to this condition? A. B. C. D. E. 5q21 11p13 13q14 17q11 22q12 34 year old woman comes to the physician because of abdominal fullness and early satiety. She says her bowel habits have not changed recently, but feels she has gotten more constipated over the years. A radiographic series shows a circumferential lesion with associated narrowing of the lumen in her sigmoid colon. A colonoscopy shows over 100 polyps. Mutation in what gene predisposed her to this condition? A. B. C. D. E. 5q21 11p13 13q14 17q11 22q12 Familial adenomatous polyposis • Mutation in APC on chromosome 5 • Autosomal dominant matter • By age 40 nearly all of these patients will develop colon cancer and thus undergo prophylactic colectomy • Colon cancer on left side of colon looks like an “apple core” with constriction and narrowing • Colon cancer on the right side is associated with iron deficiency anemia, and exophytic mass into the lumen • CEA is a good tumor marker to watch for recurrence, NOT good for screening Other polyposis syndromes • Lynch (HNPCC)--> key thing would be early onset of colon cancer without any previous polyps. Mutation in mismatch repair genes. ALWAYS involves proximal colon • Gardner: version of FAP that also has osseous and soft tissue tumors • Turcot: version of FAP that has CNS tumors (sounds like turban) • Peutz-Jeghers: hamartomas throughout the GI tract (mought, lips too) and also on the genitalia • Juvenile polyposis syndrome: hamartomatous polyps, typically younger than 5 years old 54 year old female comes to the physician due to fatigue and difficulty swallowing. Physical exam shows a smooth, red tongue. A CBC shows microcytic, hypochromic anemia with an increased RDW. This patient is at increased risk for developing which of the following conditions? A. B. C. D. E. Esophageal adenocarcinoma Barrett esophagus HSV esophagitis CMV esophagitis Esophageal squamous cell carcinoma 54 year old female comes to the physician due to fatigue and difficulty swallowing. Physical exam shows a smooth, red tongue. A CBC shows microcytic, hypochromic anemia with an increased RDW. This patient is at increased risk for developing which of the following conditions? A. B. C. D. E. Esophageal adenocarcinoma Barrett esophagus HSV esophagitis CMV esophagitis Esophageal squamous cell carcinoma 54 year old female comes to the physician due to fatigue and difficulty swallowing. Physical exam shows a smooth, red tongue. A CBC shows microcytic, hypochromic anemia with an increased RDW. This patient is at increased risk for developing which of the following conditions? A. B. C. D. E. Esophageal adenocarcinoma Barrett esophagus HSV esophagitis CMV esophagitis Esophageal squamous cell carcinoma Plummer Vinson syndrome • Atrophic glossitis with a beefy red tongue, iron deficiency anemia, and esophageal webs • This syndrome affects the proximal part of the esophagus so they are at increased risk of SCC of the esophagus • Remember, SCC of the esophagus involves the upper 2/3 since the epithelium is stratified squamous • Adenocarcinoma of the esophagus involves the lower 1/3 since that is where columnar cells begin to appear B- Barrett esophagus • Metaplasia due to chronic reflux irritating the epithelium • Nonkeratinized stratified squamous changes to nonciliated columnar with goblet cells • Increased risk for adenocarcinoma (lower part of esophagus) C and D –HSV and CMV esophagitis • HSV– punched out • CMV– linear ulcers • Can also get candida esophagitis-– white pseudomembrane • This should only be happening in immunocompromised patients • This should set you off to thinking they are either taking immunosuppressant's or they have HIV • Also know eosinophilic esophagitis– common in patients with food allergies. Symptoms of GERD that don’t resolve with PPI. See esophageal rings and linear furrows SCC vs Adeoncarcinoma of the esophagus • SCC upper 2/3 • Risk factors: alcohol, hot liquids, smoking, achalasia • More common worldwide • Adenocarcinoma lower 1/3 • GERD, Barrett esophagus, obesity, achalasia, smoking • Common in US Achalasia vs Sclerodermal esophageal dysmotility– both cause dysphagia and increased risk of cancer! • Achalasia is due to HIGH LES pressure (loss of inhibitory neurons with VIP and no) and ABSENT peristalsis • Bird’s beak on barium swallow • Sclerodermal involvement– smooth muscle atrophy leading to LOW LES pressure • Also have acid reflux symptoms 62 year old female with rheumatoid arthritis and no other PMHx comes to the office complaining of severe epigastric pain and vomiting of bright red blood. An endoscopy is planned for tomorrow morning. What is the most likely cause of this patients symptoms? A. B. C. D. E. Alcohol NSAIDS Brain injury Burn injury Uremia 62 year old female with rheumatoid arthritis and no other PMHx comes to the office complaining of severe epigastric pain and vomiting of bright red blood. An endoscopy is planned for tomorrow morning. What is the most likely cause of this patients symptoms? A. B. C. D. E. Alcohol NSAIDS Brain injury Burn injury Uremia 62 year old female with rheumatoid arthritis and no other PMHx comes to the office complaining of severe epigastric pain and vomiting of bright red blood. An endoscopy is planned for tomorrow morning. What is the most likely cause of this patients symptoms? A. B. C. D. E. Alcohol NSAIDS Brain injury Burn injury Uremia Gastritis/peptic ulcer disease • Acute gastritis • NSAIDS decreased PGE2 production leading to decreased protection of mucosa (can lead to gastric ulcers) • Alcohol exacerbates this • Curling ulcer– burns lead to loss of fluids and decreased perfusion to the stomach and mucosal ischemia • Cushing ulcer– brain injury leads to increased vagal stimulation and increased ACTH secretion which increased acid production • Chronic gastritis • H pylori– antrum first • Mucosal inflammation leading to atrophy • Decrease in HCl release which leads to increase in gastrin release increased risk for gastric cancer • Increased risk peptic ulcers • Autoimmune– body and fundus • Antibodies to parietal cells or intrinsic facto • PERNICIOUS ANEMIA PUD • Gastric ulcer • 70% due to H pylori, but also think of NSAIDS • Pain is GREATER WITH MEAL (acid secretion) • High risk of gastric carcinoma • NEED to do a biopsy of margins • Hemorrhage generally is from bleeding of right gastric artery • Peptic ulcer • 90% due to H pylori, but also consider oversecretion of gastrin with ZE (especially is multiple duodenal ulcers that reach all the way to jejunum) • Usually benign, no need for biopsy • Hemorrhage generally is due to bleeding of gastroduodenal artery 82 year old male with diffuse atherosclerotic disease presents with sudden left lower abdominal pain with guarding. Within 24 hours he passes bright red blood mixed with stool. A colonoscopy shows a diffusely necrotic descending colon. Which of the following is the most probably cause of this presentation? A. B. C. D. E. Acute arterial thrombotic occlusion Arterial embolic occlusion of SMA Bowel obstruction Nonocclusive ischemia Hypotensive ischemia 82 year old male with diffuse atherosclerotic disease presents with sudden left lower abdominal pain with guarding. Within 24 hours he passes bright red blood mixed with stool. A colonoscopy shows a diffusely necrotic descending colon. Which of the following is the most probably cause of this presentation? A. B. C. D. E. Acute arterial thrombotic occlusion Arterial embolic occlusion of SMA Bowel obstruction Nonocclusive ischemia Hypotensive ischemia 82 year old male with diffuse atherosclerotic disease presents with sudden left lower abdominal pain. Within 24 hours he passes bright red blood mixed with stool. A colonoscopy shows a diffusely necrotic descending colon. Which of the following is the most probably cause of this presentation? A. B. C. D. E. Acute arterial thrombotic occlusion Arterial embolic occlusion of SMA Bowel obstruction Chronic atherosclerotic reduction in blood flow Hypotensive ischemia Colonic ischemia vs Acute mesenteric ischemia vs chronic mesenteric ischemia • Colonic ischemia • Reduction in intestinal blood flow from occlusion leads to crampy abdominal pain and hematochezia • Usually happens in watershed areas • Splenic flexure or distal colon • Acute mesenteric ischemia • Chronic mesenteric ischemia • Generally due to embolic occlusion of SMA • Acute abdominal pain OUT OF PROPORTION TO FINDINGS • Red currant stools • Generally due to chronic atherosclerosis of SMA, IMA • Chronic hypoperfusion leads to postprandial epigastric pain and weight loss– why?? A 65 year old male comes ot the physician with a 4 week history of weakness and vague postprandial epigastric pain. He also notes that he has lost 5 kg in the last 4 weeks. He smokes 1 pack of cigarettes daily and drinks alcohol occasionally. FOBT is positive, and gastroduodenoscopy shows an ulcer in the antrum with raised margins. Biopsy of the ulcer is taken and likely to show what pathology? A. B. C. D. E. Mucin filled cells with peripheral nuclei H. pylori infiltration Gastric adenocarcinoma Gastric carcinoid tumor Hypertrophied rugae A 65 year old male comes to the physician with a 4 week history of weakness and vague postprandial epigastric pain. He also notes that he has lost 5 kg in the last 4 weeks. He smokes 1 pack of cigarettes daily and drinks alcohol occasionally. FOBT is positive, and gastroduodenoscopy shows an ulcer in the antrum with raised margins. Biopsy of the ulcer is taken and likely to show what pathology? A. B. C. D. E. Mucin filled cells with peripheral nuclei H. pylori infiltration Gastric adenocarcinoma Gastric carcinoid tumor Hypertrophied rugae A 65 year old male comes to the physician with a 4 week history of weakness and vague postprandial epigastric pain. He also notes that he has lost 5 kg in the last 4 weeks. He smokes 1 pack of cigarettes daily and drinks alcohol occasionally. FOBT is positive, and gastroduodenoscopy shows an ulcer in the antrum with raised margins. Biopsy of the ulcer is taken and likely to show what pathology? A. B. C. D. E. Mucin filled cells with peripheral nuclei H. pylori infiltration Gastric adenocarcinoma Gastric carcinoid tumor Hypertrophied rugae Gastric cancers • Most commonly adenocarcinomas • Intestinal • Associated with H. pylori, tobacco, nitrosamines, chronic gastritis • See what looks like an ulcer with raised margins • Diffuse • Not associated with H pylori • Classic pathology is signet ring cells and stomach wall grossly thickened (linitis plastica) Menetrier disease– rugae look like brain gyri • Protein loss! • Hyperplasia of the gastric mucosa leads to crowding out of the parietal cells with decreased acid production • This is what causes the loss of ability to absorb protein • Precancerous A 15 year old male immigrant comes to the doctor complaining of bowel movements that are pale and oily looking, and have become increasingly foul smelling. He notes that he has recently gotten many bloody noses, and that he remembers his mom telling him as a child he always had sinus infections. What pathological process is most likely associated with his underlying disease process? A. B. C. D. E. Lactase deficiency Villous atrophy seen on duodenoscopy Improvement of villous atrophy with antibiotics Infection with Tropheryma whipplei Misfolded protein leading to decreased chloride secretions A 15 year old male immigrant comes to the doctor complaining of bowel movements that are pale and oily looking, and have become increasingly foul smelling. He notes that he has recently gotten many bloody noses, and that he remembers his mom telling him as a child he always had sinus infections. What pathological process is most likely associated with his underlying disease process? A. B. C. D. E. Lactase deficiency Villous atrophy seen on duodenoscopy Improvement of villous atrophy with antibiotics Infection with Tropheryma whipplei Misfolded protein leading to decreased chloride secretions A 15 year old male immigrant comes to the doctor complaining of bowel movements that are pale and oily looking, and have become increasingly foul smelling. He notes that he has recently gotten many bloody noses, and that he remembers his mom telling him as a child he always had sinus infections. What pathological process is most likely associated with his underlying disease process? A. B. C. D. E. Lactase deficiency Villous atrophy seen on duodenoscopy Transmural inflammation of the ileum Infection with Tropheryma whipplei Misfolded protein leading to decreased chloride secretions Cystic Fibrosis causes pancreatic insufficiency • Malabsorption of fat leading to steatorrhea • Malabsorption of fat soluble vitamins and Vitamin B12 • Lack of vitamin K often leads to increased bleeding • Will complain of chronic sinopulmonary infections A- lactase deficiency • Will not cause steatorrhea • Normal appearing villi on endoscopy • Osmotic diarrhea diarrhea improves when fasting starts B- celiac disease • Autoimmune intolerance of gliadin • Malabsoprtion and steatorrhea • Could also cause deficiency of fat soluble vitamins due to damage to intestine • However would not see chronic pulmonary infections • Lab findings: IgA anti tissue transglutaminase, anti endomysial, anti deamidated gliadin • Endoscopy findings villous atrophy and crypt hyperplasia C- IBD, Crohn’s disease • Transmural inflammation of any part of the GI tract • Usually affects ileum leading to fat malabsorption and absorption of folic acid, iron, or B12 • Cobblestone mucosa, creeping fat, FISSURES • Generally leaves rectum alone • Diarrhea may or may not be bloody, depending on location of lesions • UC always bloody because always affects colon • Treat with immunosuppresants (steroids, azathioprine) and antibodies to TNF (adalimumab, infliximab) D- Whipple disease • Gram positive bug • PAS + FOAMY macrophages in lamina propria leading to poor absorption of fats • Also get cardiac symptoms, arthralgias, and neurologic symptoms IBS v IBD • IBS should never have bloody diarrhea • Key component should be that the pain is surrounding defecation • Can have diarrhea or constipation • Will NOT have other manifestations like in IBD– erythema nodosum, uveitis, etc Volvulus vs Intusseception vs Meckels Diverticulum: all cause bleeding in little kiddos • Volvulus • Usually associated with malrotation--ligament of treitz misplaced • In kids usually in the midgut • Key component would be abdominal distension and bilious vomiting as well • Intestinal ischemia from twisting of vessels would lead to bloody stools • Meckels diverticulum • Embryonic remnant, and if contains ectopic gastric or pancreatic tissue can cause erosion of surrounding mucosa • Usually in kids around 2 years old • Painless bloody stools • Intussusception • Telescoping of one portion of bowel into another • Crampy abdominal pain that is periodic • Bloody stools is a late sign • In children usually associated with recent infection and hypertrophy of Peyer’s patch • Note– if seen in adolescence of older, this is lymphoma until proven otherwise