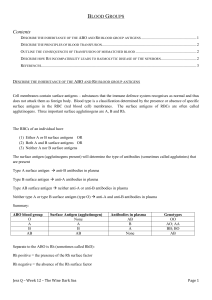
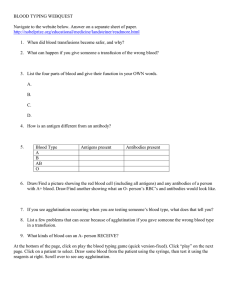
BLOOD GROUPS - II Ms Veena Shriram The Rh(D) Antigen: Rh is the most complex system, with over 45 antigens Discovered in 1940 after work on Rhesus monkeys by Landsteiner & Wiener. Subsequently discovered to be unrelated to monkeys. 85% percent of whites are Dpositive and 15% are D negative; over 99% of Asians are D-positive. Rh gene located on short arm of chromosome 1 This is another imp. group to be matched before transfusion. Thus there are two major groups of antigens causing major mismatched blood transfusion reactions 1) ABO system discovered by Landsteiner in 1900. 2) Rh system discovered by Landsteiner in 1940. Unlike the antibodies of the ABO system, anti-D antibodies do not develop without exposure of a D-negative individual to D-positive red cells by transfusion or entrance of fetal blood into the RH AGGLUTINOGENS: There are 6 known agglutinogens which are called Rh factors present on the R.B.C membrane: C,D,E and c,d,e. They are not detected in any other tissues other than RBC. Inheritance: Each person inherits at least 3 of the above factors from both groups in various combinations from both parents. e.g. CDE, cDe, cDE,----- Agglutinogen D is highly antigenic. Person having D will be called Rh+ve. irrespective of the fact whether C,E is present or not as C,E are poor agglutinogens. Cde, CdE, cde.------Ag D is absent: hence even if C,E are present, person will be labeled Rh-ve. RH BLOOD GROUP SYSTEM: In the Rh system the most imp. antigen is the type D. This occurs on surface of blood cells. The 5 most imp. genes are present on 3 diff. chromosomes - gene ‘D’ is on first chromosome - genes ‘C’ and ‘c’ are on the second chromosome - genes ‘E’ and ‘e’ are on the third chromosome Rh antigens are present only on the surface of blood cells. Production of anti-Rh agglutinins in Rh - ve starts if Rh +ve antigen gets into his blood 1. Rh -ve mother – Rh +ve baby 2. Rh -person – Rh +ve transfusion. (malpractice!!!) Rh agglutinins belong to the IgG type of antibodies – they diffuse through the placenta – so they cause agglutination in the foetal blood - erythroblastosis foetalis To prevent this we must give to the mother anti- Rh IgG antiserum ( D antigen is the strongest antigen) RH AGGLUTININS Person who has Ag D i.e. Rh+ve has no naturally occurring agglutinins in the plasma. Hence Rh system follows first part of LANDSTEINERS LAW. However if a PERSON is Rh -ve and has no agglutinogen D yet has no agglutinins in his plasma. Hence Rh system fails to obey the second part of Landsteiner Law. RH IMMUNE RESPONSE: Rh-ve blood can be given to a person who is Rh+ve as it has no agglutinins against D antigen. However if Rh+ve blood is given to a person who is Rh-ve, an immune response is seen as the D antigen is foreign to the recipient. Hence the recipient develops immune antibodies to it. Anti Rh agglutinins develop slowly within few hours. Maximum conc. of the antibodies is seen 2-4 months later. Hence no agglutination is seen as by the time agglutinins are formed, the donor cells are already destroyed. However, a 2nd exposure of Rh-ve person to Rh+ve blood, severe transfusion reaction is seen due to agglutination of donor erythrocytes with anti Rh antibodies which had been formed in the plasma previously. On multiple exposures to Rh factor, Rh-ve person gets so sensitized, that transfusion reactions can be massive similar to ABO incompatibility. ERYTHROBLASTOSIS FETALIS: Also called Hemolytic Disease of the Newborn (HDN) or Icterus Gravis neonatorum. Cause: It is due to Rh incompatibility when the mother is Rh-ve and the fetus is Rh+ve. This is possible if the father is Rh+ve DD/Dd. If the father is DD all the children are Rh+ve as D is dominant in nature. However if the father is Dd, & the mother dd, then there is 50% chance that the baby will be Rh negative (dd). Also if both parents are Rh+ve but heterozygous Dd, there is one in four chance that the baby will be Rh-ve. ERYTHROBLASTOSIS FETALIS SENSITIZATION: Initially the mother gets sensitized to the fetal blood carrying Rh antigens. Fetal cells enter mother’s blood at the time of separation of placenta, when the maternal sinuses are open. These fetal cells stimulate production of antibodies in the mother. However, these antibodies cannot harm the first baby as separation of placenta takes place after birth of the first baby. The first baby thus escapes from the incompatibility. CONTINUED….. In the second pregnancy, these antibodies which have been formed in the earlier pregnancy can diffuse through the placental barrier (IgG) and and cause agglutination of the fetal R.B.C’s provided the second baby is Rh+ve. In reality 3% of the second baby suffers. While in the third pregnancy, 10% babies suffer. Incidence rises with each successive pregnancy. First born baby may be affected if Mixing of blood in abortions, any intrauterine manipulations-fetomaternal bleed. If mother has been sensitized by previous Rh+ve blood transfusion. Hence never give Rh+ve blood to a young Rh-ve female in the reproductive age group as far as possible Clinical picture: Disease is called Hemolytic Disease of the Newborn because the newborn shows haemolysis due to maternal antibodies. Baby looks pale and anaemic. Haemolysed blood then releases Hb into the circulation which is then converted into bilirubin by macrophages. Icterus Gravis Neonatorum. Rh antibodies remain in the babies blood for 1-2 months during which more haemolyis takes place. To make up for this loss, liver and spleen enlarge to increase rate of erythropoiesis. However due to rapid rate of production, immature nucleated R.B.Cs enter circulation and the peripheral blood shows large nucleated R.B.C. Hence called Erythroblastosis Fetalis. Unconjugated bilirubin then gets deposited in the basal ganglia and cause destruction of the neuronal cells as the blood brain barrier is not yet developed. Baby then shows permanent damage to the motor areas and is mentally retarded. Conjugation of bilirubin does not take place as liver is not yet mature. This condition is called Kernicterus. If the baby does survive above, then the last stage is of generalized edema due to damage to liver & hypoprotenemia.- Hydrops Fetalis. TREATMENT : EXCHANGE TRANSFUSION Carried out soon after birth 400 ml of Rh negative - ABO compatible blood is transfused into Rh+ve baby over a period of few hours. Simultaneously Rh+ve blood is removed from the other hand. This procedure is repeated several times in the first few weeks of life. Principle: Rh-ve blood is not agglutinated by antibodies present in the fetus and hence can tide over the period in which antibodies are c i r c u l a t i n g . Baby's blood containing antibodies and bilirubin is removed hence the baby is saved f r o m c o m p l i c a t i o n s . After a few weeks when almost no antibodies are present, baby's own marrow produces Rh+ve blood which is now safe. PREVENTION: Avoid giving Rh+ve blood to a young Rh-ve female in the reproductive age group. Single dose Injection Anti D is given to the mother within 72 hours of delivery so that these antibodies will agglutinate the fetal cells circulating in the maternal blood & they are removed before they can sensitize the mother. Gap between 2 pregnancies so that antibody titers are low. IMPORTANCE OF BLOOD GROUPS: Blood transfusions Rh blood typing to avoid Erythroblastosis Fetalis. Paternity Tests. Can rule out paternity not confirm it Forensic Medicine to identify criminals Anthropological studies to understand the racial differences and the evolution of blood Groups. Correlation between blood groups and disease: e.g. Blood group O is prone to duodenal ulcer, Blood Group A is prone to gastric malignancy, pernicious anemia. BLOOD TRANSFUSION: Indications: Severe anemia, hemorrhagic shock due to wounds, accidents, maternal hemorrhage. Procedure: Blood is collected from a healthy Donor. It is then stored at 40C in a bag containing ACD (Acid Citrate Dextrose) / CPD (Citrate Phosphate Dextrose) which act as anticoagulants & can be HAZARDS OF BLOOD TRANSFUSION: Due to immune transfusion reactions: A) Hemolytic transfusion reaction: Major mismatch leads to agglutination of Donor RBC’s. Activation of complement system leads to sudden haemolysis and release of Hb into circulation. Acute renal shutdown (causes): 1) Release of toxic substances during hemolytic reaction causes powerful renal vasoconstriction . 2) Toxic substances and the loss of RBC’s makes a person go into circulatory shock. Blood pressure falls with reduced renal blood flow and urine output. 3) Also free Hb which is not bound to haptoglobulin blocks renal tubules causing acute renal shutdown.-fatal 1. Nonhaemolytic immune reaction: Fever with chills due to allergic reaction to donors plasma or ACD bag 2. Anaphylactic reaction due to release of histamine from donors basophils Nonimmune transfusion reaction: 1. circulatory overload & cardiac failure due to rapid transfusion stored blood transfusion reaction 2. a) ACD causes chelation of Calcium leading to tetany. b) Haemolysed RBC release K+ and increased plasma levels i.e. hyperkalemia is seen especially if the blood is more than 14 days old. mild thrombocytopenia because platelets and clotting factors do not survive in stored blood Last but not the least, infections transmitted via blood are viral hepatitis, HIV, malaria etc. TRANSPLANTATION OF TISSUES AND ORGANS Antigens of red blood cells that cause transfusion reactions are also present in other cells of the body, and each bodily tissue has its own additional complement of antigens. Consequently, foreign cells transplanted anywhere into the body of a recipient can produce immune reactions. AUTOGRAFTS, ISOGRAFTS, ALLOGRAFTS, AND XENOGRAFTS. A transplant of a tissue or whole organ from one part of the same animal to another part is called an autograft; from one identical twin to another, an isograft; from one human being to another or from any animal to another animal of the same species, an allograft; And from a lower animal to a human being or from an animal of one species to one of another species, a xenograft. TRANSPLANTATION OF CELLULAR TISSUES. In the case of autografts and isografts, cells in the transplant contain virtually the same types of antigens to live normally and indefinitely if an adequate blood supply is provided. At the other extreme, in the case of xenografts, immune reactions almost always occur, causing death of the cells in the graft within 1 day to 5 weeks after transplantation unless some specific therapy is used to prevent the immune reactions. Different cellular tissues and organs that have been transplanted as allografts: are skin, kidney, heart, liver, glandular tissue, bone marrow, and lung. With proper "matching" of tissues between persons, many kidney allografts have been successful for at least 5 to 15 years, and allograft liver and heart transplants for 1 to 15 years. Describe the molecular basis of blood groups and the reasons for transfusion reactions. Short Notes: 1. Classify blood group 2. ABO blood group system 3. Rh factor 4. Indication of blood transfusion 5. Mismatched blood transfusion