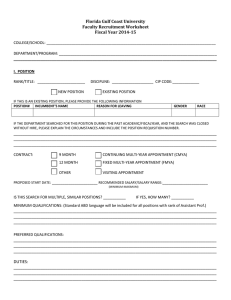
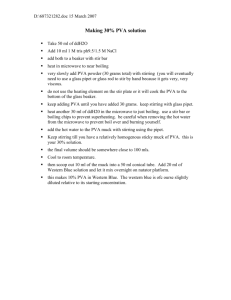
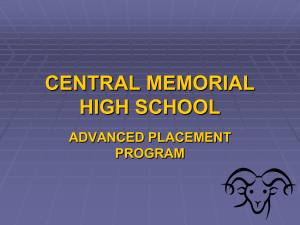
Energy conversion efficiency in human left ventricle. T Kameyama, H Asanoi, S Ishizaka, K Yamanishi, M Fujita and S Sasayama Circulation. 1992;85:988-996 doi: 10.1161/01.CIR.85.3.988 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1992 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/85/3/988 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/ Downloaded from http://circ.ahajournals.org/ by guest on March 2, 2014 988 Energy Conversion Efficiency in Human Left Ventricle Tomoki Kameyama, MD; Hidetsugu Asanoi, MD; Shinji Ishizaka, MD; Kazuto Yamanishi, MD; Masatoshi Fujita, MD; and Shigetake Sasayama, MD Background. Left ventricular mechanical efficiency is one of the most important measures of left ventricular pump performance. Several clinical studies, however, have shown that mechanical efficiency does not fall substantially as the heart fails. To clarify the insensitivity of mechanical efficiency to the change in pump performance, we analyzed human left ventricular mechanical efficiency, applying the concept of left ventricular systolic pressure-volume area (PVA). Methods and Results. PVA correlates linearly with myocardial oxygen consumption per beat (MVo2): MVo2=a * PVA+b, and represents the total mechanical energy of contraction. We determined MVo2-PVA relation and external work in 11 patients with different contractile states. We also calculated the energy transfer from MVo2 to PVA (PVA/MVo2 efficiency), that from PVA to external work (work efficiency), and mechanical efficiency (external work/MVo2). Left ventricular pressure-volume loops were constructed by plotting the instantaneous left ventricular pressure against the left ventricular volume at baseline and during pressure loading. The contractile properties of the ventricle were defined by the slope of the end-systolic pressure-volume relation (Ees). Pressure elevation raised external work by 41.4%, PVA by 71.2%, and MVo2 by 54.5%. These changes were associated with a decrease in work efficiency and an increase in PVA/MVo2 efficiency. The opposite directional changes in these two efficiencies rendered the mechanical efficiency constant. The slope, a, of the relation between MVo2 and PVA was relatively constant (2.46±0.33) over the range of 0.8-8.8 mm Hg/ml of Ees, but the oxygen axis intercept, b, tended to decrease with the reduction in Ees. PVA/MVo2 efficiency correlated inversely (r= -0.66, p <0.05) with Ees, whereas work efficiency correlated linearly with Ees (r=0.91, p<0.01). Conclusions. Mechanical efficiency is not appreciably affected by changes in loading and inotropic conditions as long as the left ventricular contractility is not severely depressed. (Circulation 1992;85:988-996) KEY WoRDs pressure-volume relation * oxygen consumption * pressure-volume area echanical efficiency, one of the most important parameters of the energy transfer system, designates the fraction of total consumed energy that is converted into external work (EW).12 Previous clinical studies,3-5 however, have documented that if the contractile state of the ventricle is not severely depressed, left ventricular mechanical efficiency does not change substantially in patients with cardiac dysfunction. The mechanism for the insensitivity of mechanical efficiency to cardiac function has not been systematically examined in clinical settings because of the lack of a suitable analytical framework. Suga6 and Suga et a17 have shown that ventricular pressure-volume area (PVA) represents the total mechanical energy of contraction (Figure 1), and it correlated linearly with myocardial oxygen consumption per beat (MVo2). The PVA has a great advantage over the previous predictors of mechanical energy utilization in M From The Second Department of Internal Medicine, Toyama Medical and Pharmaceutical University, Toyama, Japan. Presented in part at the 61st Scientific Sessions of the American Heart Association, Washington, D.C., November 14, 1988. Address for correspondence: Hidetsugu Asanoi, MD, The Second Department of Internal Medicine, Faculty of Medicine, Toyama Medical and Pharmaceutical University, 2630 Sugitani, Toyama 930-01, Japan. Received July 3, 1990; revision accepted October 22, 1991. that left ventricular mechanical performance is integrated into the PVA and can be quantitatively related to MVo2 on the same dimensional basis.8 Therefore, the PVA concept provides a useful framework to analyze the relation between the loading and inotropic conditions and mechanical efficiency of the diseased left ventricle. So far, mechanical energy transfer using the PVA concept has been examined only under unphysiological states such as excised hearts or anesthetized animal models.6-9 In the present study, we have extended the analysis of efficiency of energy transfer6'8 for the first time to human left ventricles. To clarify the insensitivity of mechanical efficiency to cardiac deterioration, we have examined, in patients with normal and moderately depressed hearts, how the changes in contractile state and afterload influence the MVo2-PVA relation and mechanical efficiency. Methods Study Patients The study was performed in 11 patients (mean age, 50 years; range, 36-62 years). Six patients had previous myocardial infarction, four had cardiomyopathy (two, idiopathic and two, after myocarditis), and one had atypical chest pain. Patients who showed clinical symp- Downloaded from http://circ.ahajournals.org/ by guest on March 2, 2014 Kameyama et al Energy Conversion Efficiency in Human Ventricle 989 External P-V Loop, C,)~~~~~~~~~~~~~~~~~~(W & Potential End-diastolic VolumeArega EPE Volume Volume FIGURE 1. Schematic ofpressure-volume (P-V) relations of left ventricle (left panel) and P-Varea (PVA) (right panel). Three P-V loops of ejecting contractions are shown in the left paneL The solid circles at the left upper corners of the loops are the end-systolic P-Vpoints. The line through these points is the end-systolic P-V line, and its slope is Ees. Diastolic P-V curve consists of the diastolic segment of these P-V loops. Effective arterial elastance, Ea, is the slope of end-systolic pressure-stroke volume (P-SV) relation. The origin of the relation line, that is, its volume axis intercept, is a given end-diastolic volume. The stroke volume is represented on this ventricular volume axis as a distance to the left of this intercept. When the ventricle is coupled with the arterial system, the equilibrium is determined as the intersection between the arterial end-systolic P-SVline and the ventricular end-systolic P-V line. PVA is the area in the P-V diagram that is circumscribed by the end-systolic P-V line, the end-diastolic P-V relation curve, and the systolic segment of P-V trajectory (E-A-B-C-E, right panel). PVA consists of the external work (EW) performed during systole and the end-systolic elastic potential energy (PE) stored in the ventricular wall at end systole. EW is the area within the P-V loop trajectory (A-B-C-D-A), and PE is the area between end-systolic P-V line and end-diastolic P-V relation curve to the left of EW (E-C-D-E). toms and signs of new myocardial ischemia on treadmill exercise test or exercise 20`T1 myocardial perfusion scans were excluded from the study, as were patients with left ventricular aneurysm or mitral regurgitation. All patients were in normal sinus rhythm, and all medications were withheld 24 hours before the procedure. The study protocol was reviewed and approved by the Ethical Committee of our institute, and informed written consent was obtained from each patient. There were no complications as a result of the study. Catheterization Procedure Cardiac catheterization was performed by the right brachial approach with the patients in a fasting state. After conventional diagnostic right and left heart catheterization, coronary arteriography was performed by the Sones technique. Proximal coronary sinus catheterization was performed with a dual-thermistor thermodilution catheter (Webster Laboratory Inc.).10 A highfidelity micromanometer-tipped catheter (Micro-Tip, Millar Instruments) was then introduced into the left ventricle, which allowed simultaneous high-fidelity pressure measurement during left ventriculography. After sufficient time was allowed after coronary arteriography, coronary sinus blood flow was determined in duplicate by the standard thermodilution method. The position of the catheter was checked frequently during the study by both fluoroscopic appearance and hand injection of small doses of contrast medium to confirm the proximal thermistor placed directly into the ostium of the coronary sinus. Arterial and coronary sinus blood samples were drawn simultaneously for the determination of oxygen saturation and lactate concentration. Left ventricular cineangiography was then performed in the 30° right anterior oblique projection with a Toshiba 9-in. (22.86-cm) image intensification system. Left ventricular opacification was achieved by injecting 35-40 ml of radiopaque nonionic contrast agent (iopamidol) through a Millar angiographic catheter at a rate of 12 ml/sec. Films were exposed at a rate of 60 frames/sec with an Arriflex 35 mm cine camera while the patient was gently holding his breath. During the cineangiographic study, high-fidelity left ventricular pressure, ECG, cineangiographic frame markers, and an injection marker were recorded simultaneously. An adequate recovery time was allowed for the left ventricular pressure to return to baseline level. Phenylephrine (5 mg/100 ml) was started to increase the systolic left ventricular pressure by about 50 mm Hg. In nine patients, the heart rate was kept almost the same as in the control state by coronary sinus pacing. Measurements of coronary sinus flow and samplings of coronary sinus blood were taken again under steady-state conditions during pressure elevation. After these measurements, the second cineventriculogram was obtained in the same manner as in the control state. In seven patients, myocardial lactate uptake was calculated as follows: myocardial lactate uptake=(arterial lactatecoronary sinus lactate) x 100/arterial lactate. There were no signs of pulmonary congestion, appearance of a transient mitral regurgitation, or other side effects during these procedures. Generation ofAngiographic Pressure-Volume Diagrams The boundary of the ventricular silhouette was delineated manually by Oscon cine analyzer. Left ventricular Downloaded from http://circ.ahajournals.org/ by guest on March 2, 2014 Circulation Vol 85, No 3 March 1992 990 Ees -3.5 mmHg/ml 150 I E 100 W 8 50 W 01 00 VOLUME(ml) W- a0F CL A PYA+B 0.3 5 B = 1.1 j /beat MVO2= 1 6.0 phenylephrine N 4.0 control N 0 2.C ni! -0 1.0 2.0 PVA ( j /beat) FIGURE 2. Graphs show left ventricular pressure-volume (P-V) diagram for baseline and a high pressure setting with phenylephrine (upper panel). P-V area (PVA) is the area circumscribed by the end-systolic P-V line, the end-diastolic P-V curve, and the systolic segment ofP-Vtrajectory (shaded area). An end-systolic P-V line was drawn on the left upper corner of the P-V loops. The left ventricular contractile state was defined by the slope (Ees) of this relation. Relation between myocardial oxygen consumption per beat (MVO2) and PVA in the same patient (case 2) as in the upper panel (lower panel). MVO2 was plotted as a function of PVA in basal and high-pressure states. The slope (A) and oxygen axis intercept (B) of this relation was determined from a straight line passed through these two points (MVO2=A. PVA +B). MVO2 and PVA are expressed in joules. volume (V) was calculated by the area-length method using a modified Kennedy's formula1': V=0.687xC3x A2/L+ 1.9, where A is the area of the ventricle calculated from the number of pixels surrounded by the ventricular boundary, L is the longest measured length between the midpoint of the aortic valve and the apex, and C is the linear correction factor for the magnification of a unit of length (one pixel). C was derived from a comparison with the known area of the filmed 1-cm2 grid placed parallel to the tube at the position of the heart. The calculated volume of each frame was synchronized to corresponding pressure by simultaneously recorded exposure marker throughout one cardiac cycle to obtain the pressure-volume loop. Ventricular and Arterial End-Systolic Pressure-Volume Relations An end-systolic pressure-volume line was drawn on the left upper corners of the pressure-volume loops of baseline and pressure loading (Figure 2, upper panel). The left ventricular contractile state was defined by the slope (Ees) of this end-systolic pressure-volume relation.12,13 Given a constant heart rate, arterial end-systolic pressure changes with stroke volume in a roughly linear relation. The slope of this relation is in proportion to the impedance that the arterial tree offers to the stroke flow. Thus, the arterial properties can be represented as a first approximation by the arterial end-systolic pressure-stroke volume relation. Sunagawa et al14 called this slope effective arterial elastance (Ea). We determined Ea as the ratio of end-systolic pressure to stroke volume both at rest and during increased afterload. Left Ventricular Work and Work Efficiency We measured PVA by planimetry at baseline and during increased afterload and defined it as the area within the straight line connecting volume axis intercept (V0) of the end-systolic pressure-volume line and the end-systolic point, end-diastolic pressure-volume relation curve, and systolic segment of the pressure-volume trajectory. PVA in an ejecting contraction consists of two parts (Figure 1, right panel).6 One is the area within the pressure-volume loop trajectory (A-B-C-D-A), which equals left ventricular EW. The other is the area between the end-systolic and end-diastolic pressurevolume relation curves to the left of EW (E-C-D-E). This area is considered equal to end-systolic elastic potential energy built during systole and stored in the ventricular wall. We analyzed the ratio of EW to PVA, which represents the efficiency of energy transfer from the ventricle to the arterial system. This ratio was termed work efficiency in the present article.15 Mechanical Efficiency and MVo2-PVA Relation Oxygen contents of arterial and coronary sinus blood were calculated as the product of the percent oxygen saturation, oxyhemoglobin binding capacity, and hemoglobin concentration. MVo2 was calculated as the product of coronary sinus blood flow and the arteriocoronary sinus oxygen difference and was expressed on a per beat basis. Because the energy units of EW and MVo2 are expressed by mm Hg * ml and ml 02, respectively, these units were converted into a common unit of energy, joules (J), by use of the following conversions: 1 mmHg*ml=1.33x10-4 J and 1 ml 02=20 J.16 Then mechanical efficiency was expressed conventionally by the ratio of EW to MVo2. For each patient, MVo2 was plotted as a function of PVA in the basal and highpressure states. The slope, a, and oxygen axis intercept, b, of the relation between MVo2 and PVA were determined from a straight line connecting these two points (i.e., MVo2=a * PVA+b)6 in the same manner as determined by Burkhoff et al (Figure 2, lower panel).17 Statistical Analysis Data were expressed as mean±SD. Because the patients served as their own controls, the statistical significance of differences in hemodynamic variables was tested by paired t test. Values of p<0.05 were considered to represent a statistical significance. The interrelations between efficiency parameters and basal inotropic state were quantified by linear regression analysis. Results The data for all patients are listed in Table 1. The left ventricular end-systolic pressure increased by 54.6 +20.9 Downloaded from http://circ.ahajournals.org/ by guest on March 2, 2014 Kameyama et al Energy Conversion Efficiency in Human Ventricle 991 TABLE 1. Left Ventricular and Coronary Hemodynamic Data DO2 HR ESP LVP EDV ESV EF Ea Ees CSF (ml/100 MVo2 LU Patient (bpm) (mm Hg) (mm Hg) (ml/m2) (mu/m2) (%) (mm Hg/mi) (mm Hg/ml) (ml/min) ml) (ml/min) (%) 156 156 1c 70 22 57 2.72 61 2.21 135 8.9 13.4 38 70 176 176 1P 64 28 2.99 56 10.3 155 16.0 50 120 79 96 2C 66 25 1.50 63 3.54 132 9.4 12.4 40 142 2P 148 60 84 33 1.80 61 162 9.1 14.7 41 100 60 110 64 21 3C 1.08 67 8.80 152 9.7 14.7 7 165 170 24 76 3P 73 67 1.57 190 9.7 18.4 18 100 95 120 4C 61 1.33 2.65 70 18 163 8.9 14.5 42 175 178 4P 80 35 2.22 245 9.8 24.0 95 56 44 124 124 SC 1.88 92 75 34 54 185 12.0 22.3 5.97 35 5P 152 91 152 37 1.95 57 85 240 11.0 26.4 40 63 116 140 6C 76 42 1.93 98 45 8.4 8.2 5.22 48 67 179 180 6P 40 81 49 3.20 11.9 134 8.9 58 75 92 114 7C 20 1.26 70 68 80 12.7 10.2 5.40 57 75 173 176 7P 67 1.88 91 30 130 13.7 17.8 61 8C 65 78 96 153 107 30 11.3 7.9 0.81 0.96 80 nd 128 8P 60 104 125 28 1.17 175 100 11.3 11.3 nd 9C 60 102 113 26 64 59 1.62 3.17 68 10.2 6.9 nd 9P 62 41 179 179 93 130 10.4 13.7 56 2.11 nd 10 C 86 93 99 46 14.2 39 1.90 75 81 11.5 nd 1.43 144 67 148 108 10 P 75 12.0 19.9 38 2.09 165 nd 11 C 79 98 47 73 88 10.5 35 1.84 100 10.5 nd 3.28 11 P 148 88 148 57 87 11.0 34 3.02 150 16.5 nd Mean C 76 103 117 37 76 10.6 3.86 54 1.64 115 12.1 38 SD -+-13 +22 +17 ±2.31 +26 +26 +1.8 ±16 ±40 ±0.50 ±4.3 ±+14 Mean P 73 158 162 48 93 164 10.7 51 2.18 17.3 45 +-13 +29 +23 SD ±45 +1.4 +14 ±13 +0.64 +4.7 +30 ±+17 NS <0.01 <0.01 <0.01 <0.01 <0.01 <0.05 <0.01 NS <0.01 <0.01 p HR (bpm), heart rate (beats per minute); ESP, LVP, left ventricular end-systolic and peak pressures; EDV, ESV, left ventricular end-diastolic and end-systolic volume; EF, left ventricular ejection fraction; Ea, slope of arterial end-systolic pressure-stroke volume relation; Ees, slope of left ventricular end-systolic pressure-volume relation; CSF, coronary sinus flow; DO2, arteriocoronary sinus oxygen difference; MVo2, myocardial oxygen consumption per minute; LU, lactate uptake; C, control; P, phenylephrine; nd, not determined. - - - - - - Hg with phenylephrine, associated with 35.2± 22.9% increase in Ea. There were significant augmentations of end-diastolic volume and end-systolic volume and reduction in ejection fraction. Coronary sinus blood flow increased by 48.1±26.9%, but there were no significant changes in arteriocoronary sinus 02 difference. Consequently, myocardial oxygen consumption per minute increased by 49.0±25.9%. Myocardial lactate uptake also increased in all seven patients, and there were no signs of myocardial ischemia on the ECG during these interventions. Representative pressure-volume loops are shown in Figure 2. Individual data on the left ventricular work and energy transfer are listed in Table 2. With pressure elevation, left ventricular EW increased by 41.4+34.3%, and end-systolic potential energy was doubled. The PVA (sum of the area of EW and potential energy) increased by 71.2±33.6%. These changes were accompanied by a decrease in work efficiency (EW/PVA) but an increase in PVA/MVo2 efficiency. Consequently, mechanical efficiency (EW/MVo2) did not change appreciably. Ees ranged from 0.81 to 8.8 mm Hg/ml, and left ventricular ejection fraction ranged from 30% to 70%. Only four of the patients had depressed ejection fraction (<50%), which did not necessarily correlate with mm - Ees (r=0.48, p>0.10). Figure 3 shows the scatter diacoefficient, a, and oxygen axis intercept, b, of MVo2-PVA relation against Ees. The reciprocal of the slope, 1/a, reflects the efficiency with which oxygen is utilized to generate mechanical energy. This value was constant, with a mean value of 41% over the wide range of Ees values. The intercept, b, tended to decline with depression of contractile state. Figure 4 shows PVA/MVo2 efficiency and work efficiency plotted as a function of Ees. The former correlated inversely with Ees (r=-0.649, p<0.05) and the latter linearly (r=0.907, p<0.01). Consequently, because of counterbalance of these two efficiencies, mechanical efficiency (EW/MVo2) remained unchanged (22.1±4.2%) within the range of Ees or ejection fraction of the patients studied (Figure 5). gram of slope Discussion The primary determinants of MVo2 are the preload and afterload and the contractile state of the left ventricle. PVA is the first and intermediate form of total mechanical energy, which allows us to relate these parameters of cardiac mechanical performance to MVo2 on the same dimensional basis. Tension-time Downloaded from http://circ.ahajournals.org/ by guest on March 2, 2014 992 Circulation Vol 85, No 3 March 1992 TABLE 2. Left Ventricular Work and Efficiency PVA EW PE (mm Hg ml) (mm Hg ml) (mm Hg ml) Patient 10,676 4,859 1C 5,817 7,424 1P 5,363 12,787 2C 1,733 3,656 5,389 9,940 2P 4,828 5,112 992 9,781 3C 8,789 12,853 3,159 9,694 3P 8,406 4C 2,882 5,524 4P 9,316 6,490 15,806 7,627 2,117 5C 5,510 10,435 3,435 7,000 5P 6,708 6C 1,717 4,991 9,370 6P 4,658 4,712 7C 6,049 1,631 4,428 13,148 4,474 8,670 7P 7,391 8C 3,216 4,175 11,500 8P 5,504 4,996 7,099 9C 1,937 5,167 14,788 6,715 9P 8,073 7,647 3,299 10 C 4,348 7,554 8,316 10 P 15,870 5,190 11 C 1,441 3,749 10,070 11 P 4,026 6,044 7,452 Mean C 2,348 5,105 SD +1,697 +1,115 ±1,423 12,415 Mean P 5,297 7,027 +2,358 SD +1,551 +1,863 <0.01 <0.01 <0.01 p EW/MVo2 (%) PVA/MVo2 (%) 37 37 23 27 27 28 37 42 21 24 34 35 30 37 40 41 41 45 38 40 29 36 33 EW/PVA (%) 54 42 68 51 90 75 66 59 72 67 74 50 73 66 56 52 73 55 57 53 72 60 69 20 16 15 14 24 21 25 25 15 16 26 18 22 24 23 21 30 24 22 21 21 21 22 ±7 +10 +4 36 +7 <0.01 57 +9 <0.01 20 -+4 NS a 1/a (%) b (J/beat) 2.64 38 0.08 2.90 35 1.06 3.00 33 1.00 2.08 48 0.68 2.62 38 2.16 2.68 37 0.20 2.16 46 0.97 2.43 41 0.04 2.08 48 0.33 2.40 42 0.22 2.09 48 0.95 2.46 +0.33 41 +6 0.70 +0.63 EW, left ventricular external work; PE, end-systolic potential energy; PVA, pressure-volume area; PVA/MVo2, PVA/myocardial oxygen consumption efficiency; EW/PVA, work efficiency; EW/MVo2, mechanical efficiency; a, slope of the PVA-MVo2 relation; 1/a, reciprocal of slope a; b, oxygen axis intercept of PVA-MVo2 relation; J, joule; C, control; P, phenylephrine. index, peak pressure, and stroke work, which are proposed as clinical predictors of MVo2, can change considerably despite an absence of change in MVo2.18 Myocardial peak force and contractile state have been viewed as the major predictors of energy consumption.21920 MVo2 for a given peak force increases considerably, however, with shortening and ejection.21 Weber and Janicki21 showed that the time integral of total systolic force correlated linearly with MVo2 for both ejecting and isovolumetric contractions in canine left ventricle. This parameter, however, is not equivalent to the total mechanical energy generated by ventricular contraction, as PVA is. Moreover, Suga et al822 have recently demonstrated that MVo2 remained constant when the force-time integral was greatly changed by reciprocally changing afterloaded pressure and enddiastolic volume while keeping PVA constant in a stable contractile state. The linear muscle version of PVA, which was called force-length area,23 has also been shown to correlate closely with MVo2 in ferret papillary muscles23 and with total heat generated in rabbit papillary muscles.24 All these results support feasibility of PVA as a linear and close correlate of MVo2. As far as we know, this is the first study to quantitatively describe the influence of ventricular contractile state and afterload on efficiency of energy transfer in human left ventricle. The present study showed that, with the depres- sion of contractile state, there arose an increase in energy conversion from MVo2 to PVA and a decrease in that from PVA to EW. Mechanical efficiency (EW/MVo2) remained unchanged over the range of contractile states of the patients studied. An increase in afterload produced similar effects on these energy conversion efficiencies. We used PVA as the total mechanical energy of ejecting contraction, as defined by Suga.6 According to the PVA concept,9 mechanical efficiency can be divided into two steps: the efficiency of energy conversion from MVo2 to PVA as the first step and the efficiency of energy conversion from PVA to EW as the second step. Then PVA can be assumed to reflect an intermediate form of energy between MVO2 and EW. Energy Conversion Efficiency From MVo2 to PVA Suga6 and Suga et a125 have demonstrated a linear relation between MVo2 and PVA with a nonzero positive intercept for PVA=O (MVo2=a* PVA+b, b>O). The intercept, b, the MVo2 required for a mechanically unloaded contraction, represents the sum of the basal energy requirement and the energy required for excitation-contraction coupling.26 They also have shown that when inotropic state is enhanced, the MVo2-PVA relation shifts upward (increase in b), and when inotropic state is depressed, the relation shifts downward (de- Downloaded from http://circ.ahajournals.org/ by guest on March 2, 2014 -~ ~ Kameyama et al Energy Conversion Efficiency in Human Ventricle 50 50 0 401_ eh 0 8 . 0 a * S 0 0 0 8 cc- a - 0 40 - 0~ 20~ NS Y =-2.0 x+40.2 r =-0.66 P <0.05 00~~~ 0 0~~~~~~~~~~~~~4 0~~~~~~~ 0 30 (M N 301_ 993 2010 r =0.59 P<O. a, .0 80[ 0 4- 2.0. 0- en . 90 o0 CD . A , ,a1 * o 1.0 0 1.0 N' ~ 0 0 co~ 0 ^.^.. 2.0 3: 40 .SO 0 . . 80 O V L 0 0 70 t. 0. 0 Ees (mmHg/mI ) FIGURE 3. Scatterplots show the relation between the basal inotropic state (Ees) and the slope coefficient (A) and oxygen axis intercept (B) of myocardial oxygen consumption-pressure volume area relation. The reciprocal of the slope (1/A) reflects the efficiency with which oxygen is utilized to generate mechanical energy. This efficiency was constant with a mean value of 41% over a wide range of Ees (upper panel). Intercept B, non-work-related oxygen consumption, tended to decline with the depression of contractile state (lower panel). crease in b), without significant change in the slope, a, of the relation. The reciprocal of the slope of the linear MVo2-PVA relation has been considered to represent the efficiency of chemomechanical transduction of the contractile machinery of the left ventricle. In excised dog hearts, this efficiency ranged from 30% to 50% regardless of the loading, heart rate, and inotropic conditions.25-27 The present study demonstrated that this efficiency averaged 41% in human left ventricle at any level of contractile state. Under these circumstances, PVA/MVo2 efficiency increases with the depression of contractile state for a given PVA and with an increase in PVA accompanied by an increase in afterload (Figure 6, left panel). Left Ventricular Work Efficiency Work efficiency, EW/PVA, represents the efficiency of mechanical energy transfer from the ventricle to the arterial system.9 This efficiency decreased with the depression of the contractile state or with an increase in afterload. If we assume that the time-averaged ventricular pressure during ejection is close to end-systolic pressure and left ventricular diastolic pressure is negligible compared with the pressure during ejection, EW can be approximated by the product of stroke volume and end- Y = 4.0 60~ WI 0 50 x +53.1 r = 0.91 P<0.01 F 40 . 0 2 4 6 8 10 Ees (mmHg/mI) FIGURE 4. Graphs show relation between PVAIMVO2 efficiency and work efficiency (EWIPVA) and the basal inotropic state (Ees). PVA/MVO2 correlated inversely with Ees, and work efficiency decreased linearly with the reduction in Ees. PVA, pressure-volume area; MVO2, myocardial oxygen consumption per beat; EW, left ventricular external work; Ees, slope of end-systolic pressure-volume relation. systolic pressure. Work efficiency can be formulated28 as EW/PVA=1/[1+(Ea/Ees)/2], where Ea represents the arterial input impedance properties (effective arterial elastance) expressed by the slope of arterial end-systolic pressure-stroke volume relation. This formula implies that work efficiency is a function of basal inotropic state (Ees) and afterload (Ea). In a previous study,15 we have demonstrated that in patients with variably depressed hearts, work efficiency was actually related to the Ea/Ees ratio. This relation is shown schematically in Figure 6 (right panel), which illustrates two different inotropic conditions and two different effective arterial elastances. This conceptual framework shows that a depression of contractile state or an increase in afterload increases the Ea/Ees ratio and end-systolic potential energy and reduces work efficiency. Left Ventricular Mechanical Efficiency According to earlier studies,1-4,29,30 cardiac mechanical efficiency varies between 0 and 45%, with normal functioning values of 10% to 25%. Our present data fell within this range. The mechanical efficiency is affected by ventricular preload, afterload, and contractile state. The influence of these factors on efficiency, however, has been difficult to analyze in quantitative terms. Evans Downloaded from http://circ.ahajournals.org/ by guest on March 2, 2014 Circulation Vol 85, No 3 March 1992 994 40 30 0 2 0 2020 ** * 3: 10 0 2.0 4.0 G.0 Ees (mmHg/mi) 40 30 _^il 20 0o 2 20 * ~ -1 10 o 20 40 60 loading during cineventriculography. According to Baxley et a13 or Nichols et al,4 most of the patients with ejection fraction less than 40% showed a significant reduction in mechanical efficiency. In patients with ** * ejection fraction greater than 40%, however, mechanical efficiency did not always decrease to that extent. In the present study, mechanical efficiency did not correlate with left ventricular ejection fraction. The mechanism for relatively constant mechanical efficiency in moderately depressed hearts can be explained by the o . . . . .PVA concept (Figure 6). In these hearts, the reduction 8.0 10.0 in non-work-related oxygen consumption, b, raises PVA/MVo2 efficiency, which counteracts the reduction in work efficiency so as to maintain mechanical efficiency. When the heart is severely depressed, however, the substantial fall in work efficiency would predominate over the increase in PVA/MVo2 efficiency, resulting in a mismatch in terms of mechanical efficiency. Similar mechanisms could also work in the response of mechanical efficiency to pressure loading. 0 3 * 3The present study included six patients with previous myocardial infarction. In these patients, MVo2 might be augmented in maintaining increased regional systolic wall stress, which could not be expressed within the pressure-volume diagram. Therefore, if wall stress were used instead of pressure, different findings might occur in patients with regional wall motion abnormalities. 80 EF (%) FIGURE 5. Scatterplots show relation between the mechanical efficiency (EW/MVO2) and the basal inotropic state (Ees) (upper panel) or ejection fraction (EF) (lower panel). Mechanical efficiency remained unchanged (mean 22.1%) against different Ees or EF levels. EW, left ventricular external work; MVo2, myocardial oxygen consumption per beat; Ees, slope of end-systolic pressure-volume relation. and Matsuokal first observed in Starling heart-lung preparations that mechanical efficiency decreased as the condition of the heart preparations deteriorated. They also found that cardiac efficiency was greater during volume loading than during pressure loading. Bing et a129 measured left ventricular efficiency in humans. Mean efficiency value for normal subjects was 22%, which compared remarkably well with the average value of 15% for patients with congestive heart failure. Baxley et al3 calculated mechanical efficiency in patients with variably depressed hearts resulting from valvular or myocardial disease. The range of efficiency varied from 4% to 40%, with the smallest value formed in patients with primary myocardial disease. They showed that mechanical efficiency was roughly correlated with ejection fraction. Recently, Nichols et a14 showed a similar relation between ejection phase indexes and left ventricular mechanical efficiency in patients with coronary artery disease. The present study demonstrated that mechanical efficiency was comparable in patients with mildly to moderately depressed hearts. We consider that the differences between our results and those in earlier studies probably result from severity of cardiac depression, because we exclude patients with severe cardiac dysfunction, who may have a risk in pressure or volume Limitations Several methodological problems must be discussed. Because volume data are limited by left ventriculography, we derived the relation between PVA and MVo2 only for two pressure settings in each subject, one baseline pressure and another relatively high pressure. For this analysis, we took advantage of the fact that despite the great difference in heart size, a high correlation of the linear MVo2-PVA relation has been shown both in dog hearts and in rabbit hearts.31 Minor fluctuation of contractility caused by baroreflex-mediated alterations in sympathetic discharge cannot be excluded. In this regard, Suga et a132 reported that the changes in the slope of end-systolic pressure-volume line caused by either carotid sinus or aortic baroreceptor reflexes were only about 13% when arterial pressure was changed between 100 mm Hg and 150 mm Hg. In addition, Vatner et a133 found that in conscious animals, the baroreflex control of cardiac contractility was even weaker than in the anesthetized state. Therefore, the reflex change in the slope of end-systolic pressure-volume relation in our study could be negligible. Pressure loading potentially causes a transient mitral regurgitation, which might modify the increase in MVo234 and the change in mechanical efficiency because mitral regurgitation increases left ventricular flow work but decreases potential energy. The present study, however, confirmed that there were no signs of mitral regurgitation either at rest or during pressure elevation. The thermodilution technique for estimation of coronary blood flow has been used in the past several years. The accuracy of this method greatly depends on the catheter position within the coronary sinus, and only large changes (more than 30%) in coronary blood flow are likely to be qualitatively accurate.35 We paid meticulous attention throughout these studies to proximal positioning of the external thermistor. The change in Downloaded from http://circ.ahajournals.org/ by guest on March 2, 2014 Kameyama et al Energy Conversion Efficiency in Human Ventricle 995 8.0 C m CO EE W a 4.0 or cm 0 0. 0 1.0 2.0 200 100 VOLUME ( PVA ( joule/beat ) ml ) FIGURE 6. Schematic of MVO2-PVA relation line and isoefficiency line (left panel). Family of isoefficiency lines (dashed lines) indicates various efficiencies of energy conversion from MVO2 to PVA. The depression of contractile state shifts MVO2-PVA relation (solid line) downward in parallel and increases PVAIMVO2 efficiency for a given PVA. Given a constant inotropic state, PVA/MVO2 efficiency increases with an increase in PVA. Effects of contractility and afterload on work efficiency of the left ventricle (right panel). Solid pressure-volume loops indicate baseline and a high-pressure state in normal heart. Dashed loops also represent basal and a high-pressure state in depressed heart. A depression of contractile state results in a substantial increase in end-systolic potential energy and reduces work efficiency. For a given rise in afterload, the reduction in work efficiency is more marked in the depressed heart than in the normal heart. MVO2, myocardial oxygen consumption per beat; PVA, pressure-volume area; Ees, slope of end-systolic pressure-volume relation; Ea, slope of end-systolic pressure-stroke volume relation. coronary blood flow in this study was 42.2%. With each patient serving as his own control and with little change in heart rate, data thus collected should reliably reflect changes in coronary sinus flow. Recent evidence indicates that the ionic contrast medium can significantly alter myocardial metabolism by increasing the free fatty acid uptake of the myocardium while decreasing the myocardial uptake of glucose and lactate.36 In the present study, we carried out left ventriculography using nonionic contrast agents, which exhibit considerably less myocardial toxicity. Sufficient time was also allowed between two left ventriculographies. Therefore, the effects of contrast medium on cardiac performance and metabolism would be minimized in this study. Finally, because of the small numbers and heterogeneity of the patients, the data obtained were somewhat scattered and could contain modest quantitative error. However, hemodynamic changes seen in our study were dramatic and relatively uniform during pressure manipulation. Therefore, quantitative factors probably would little affect the present results. In summary, we applied the PVA concept to evaluate energy conversion efficiency in human left ventricles. Our results showed that mechanical efficiency does not change appreciably with depression of contractile state or an increase in afterload as long as the left ventricular pump function is not severely compromised. The decreased sensitivity of mechanical efficiency can be accounted for by the counteraction of PVA/MVo2 efficiency and work efficiency. Thus, the concept of PVAmediated energy transfer would provide us a rational basis to gain insight into the energetic aspects of human left ventricle under normal and pathological conditions. Acknowledgment We thank Professor H. Suga, Okayama University, for his valuable suggestions. References 1. Evans CL, Matsuoka Y: The effect of various mechanical conditions on the gaseous metabolism and efficiency of the mammalian heart. J Physiol (Lond) 1915;49:378-405 2. Gibbs CL: Cardiac energetics. Physiol Rev 1978;58:174-254 3. Baxley WA, Dodge HT, Rackley CE, Sandler H, Pugh D: Left ventricular mechanical efficiency in man with heart disease. Circulation 1977;55:564-568 4. Nichols AB, Pearson MH, Sciacca RR, Cannon PJ: Left ventricular mechanical efficiency in coronary artery disease. J Am Coll Cardiol 1986;7:270-279 5. Hasenfuss G, Holubarsch C, Heiss HW, Meinertz T, Bonzel T, Wais U, Lehmann M, Just H: Myocardial energetics in patients with dilated cardiomyopathy: Influence of nitroprusside and enox- imone. Circulation 1989;80:51-64 6. Suga H: Total mechanical energy of a ventricle model and cardiac oxygen consumption. Am J Physiol 1979;236(Heart Circ Physiol 5):H498-H505 7. Suga H, Hayashi T, Shirahata M, Suehiro S, Hisano R: Regression of cardiac oxygen consumption on ventricular pressure-volume area in dog. Am J Physiol 1981;240(Heart Circ Physiol 9):H320-H325 8. Suga H, Goto Y, Nozawa T, Yasumura Y, Futaki S, Tanaka N: Force-time integral decreases with ejection despite constant oxygen consumption and pressure-volume area in dog left ventricle. Circ Res 1987;60:797-803 9. Nozawa T, Yasumura Y, Futaki S, Tanaka N, Uenishi M, Suga H: Efficiency of energy transfer from pressure-volume area to external mechanical work increases with contractile state and decreases with afterload in the left ventricle of the anesthetized closed chest dog. Circulation 1988;77:1116-1124 10. Ganz W, Tamura K, Marcus HS, Donoso R, Yoshida S, Swan HJC: Measurement of coronary sinus blood flow by continuous thermodilution in man. Circulation 1971;44:181-195 11. Kennedy JW, Trenholme SE, Kasser IS: Left ventricular volume and mass from single plane angiogram: A comparison of anteroposterior and right anterior oblique methods. Am Heart J 1970;80: 343-352 12. Suga H, Sagawa K, Shoukas AA: Load independence of the instantaneous pressure-volume ratio of the canine left ventricle and effects of epinephrine and heart rate on the ratio. Circ Res 1973;32:314-322 13. Suga H, Sagawa K: Instantaneous pressure-volume relationships and their ratio in the excised, supported canine left ventricle. Circ Res 1974;35:117-126 Downloaded from http://circ.ahajournals.org/ by guest on March 2, 2014 996 Circulation Vol 85, No 3 March 1992 14. Sunagawa K, Maughan WL, Burkhoff D, Sagawa K: Left ventricular interaction with arterial load studied in isolated canine heart. Am J Physiol 1983;245(Heart Circ Physiol 14):H773-H780 15. Asanoi H, Sasayama S, Kameyama T: Ventriculoarterial coupling in normal and failing heart in humans. Circ Res 1989;65:483-493 16. Coulson RL: Energetics of isovolumic contractions of the isolated rabbit heart. J Physiol (Lond) 1976;260:43-53 17. Burkhoff D, Yue DT, Oikawa RY, Franz MR, Schaefer J, Sagawa K: Influence of ventricular contractility on non-work related myocardial oxygen consumption. Heart Vessels 1987;3:66-72 18. Suga H, Hayashi T, Suehiro S, Hisano R, Shirahata M: Equal oxygen consumption rates of isovolumic and ejecting contractions with equal systolic pressure volume areas in canine left ventricle. Circ Res 1981;49:1082-1091 19. McDonald RH: Developed tension: A major determinant of myocardial oxygen consumption. Am J Physiol 1966;210:351-356 20. Henry PD, Eckberg D, Gault JH, Ross J: Depressed inotropic state and reduced myocardial oxygen consumption in the human heart. Am J Cardiol 1973;31:300-306 21. Weber KT, Janicki JS: Myocardial oxygen consumption: The role of wall force and shortening. Am J Physiol 1977;233(Heart Circ Physiol 2):H421-H430 22. Suga H, Nozawa T, Yasumura Y, Futaki S, Ohgoshi Y, Yaku H, Goto Y: Force-time integral does not improve predictability of cardiac 02 consumption from pressure-volume area (PVA) in dog left ventricle. Heart Vessels 1990;5:152-158 23. Hisano R, Cooper G: Correlation of force-length area with oxygen consumption in ferret papillary muscle. Circ Res 1987;61:318-328 24. Gibbs CL, Chapman JB: Cardiac energetics, in Ter Keurus HEDJ, Tyberg JV (eds): Mechanics of the Circulation. Dordrecht/Boston/ Lancaster, Martinus Nijhoff Publishing, 1987, pp 69-86 25. Suga H, Hayashi T, Shirahata M: Ventricular systolic pressure volume area as predictor of cardiac oxygen consumption. Am J Physiol 1981;240(Heart Circ Physiol 9):H39-H44 26. Suga H, Hisano R, Goto Y, Yamada 0, Igarashi Y: Effects of positive inotropic agents on the relation between oxygen consump- 27. 28. 29. 30. tion and systolic pressure volume area in canine left ventricle. Circ Res 1983;53:306-318 Suga H, Hisano R, Hirata S, Hayashi T, Yamada 0, Ninomiya I: Heart rate-independent energetics and systolic pressure-volume area in dog heart. Am J Physiol 1983;244(Heart Circ Physiol 13):H206-H214 Burkhoff D, Sagawa K: Ventricular efficiency predicted by an analytical model. Am J Physiol 1986;250(Regulatory Integrative Comp Physiol 19):R1021-R1027 Bing RJ, Hammond MM, Handelsman JC, Powers SR, Spencer FC, Eckenhoff JE, Goodale WT, Hafkenschiel JH, Kety SS: The measurement of coronary blood flow, oxygen consumption and efficiency of the left ventricle in man. Am Heart J 1949;38:1-24 Bing RJ, Michal G: Myocardial efficiency. Ann N Y Acad Sci 1959;72:555-558 31. Goto Y, Slinker B, LeWinter M: Similar normalized Emax and O2 consumption-pressure-volume area relation in rabbit and dog. Am J Physiol 1988;255(Heart Circ Physiol 24):H366-H374 32. Suga H, Goto Y, Yasumura Y, Nozawa T, Futaki S, Tanaka N, Uenishi M: 02 consumption of dog heart under decreased coronary perfusion and propranolol. Am J Physiol 1988;254(Heart Circ Physiol 23):H292-H303 33. Vatner SF, Higgins CB, Franklin D, Braunwald E: Extent of carotid sinus regulation of the myocardial contractile state in conscious dogs. J Clin Invest 1972;51:995-1008 34. Urschel CW, Covell JW, Graham TP, Clancy RL, Ross J, Sonnenblick EH, Braunwald E: Effects of acute valvular regurgitation on the oxygen consumption of the canine heart. Circ Res 1968;23: 33-43 35. Marcus ML, Wilson RF, White CW: Methods of measurement of myocardial blood flow in patients: Critical review. Circulation 1987;76:245-253 36. Wisneski JA, Gertz EW, Neese RA, Morris DL: Absence of myocardial biochemical toxicity with non ionic contrast agent (iopamidol). Am Heart J 1985;110:609-617 Downloaded from http://circ.ahajournals.org/ by guest on March 2, 2014
 0
0

No more boring flashcards learning!
Learn languages, math, history, economics, chemistry and more with free StudyLib Extension!
- Distribute all flashcards reviewing into small sessions
- Get inspired with a daily photo
- Import sets from Anki, Quizlet, etc
- Add Active Recall to your learning and get higher grades!


Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users