Bronchial Emphysema and COPD using NI-Multisim - eeecos-2016
advertisement

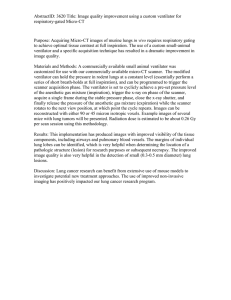
3rd International Conference on Electrical, Electronics, Engineering Trends, Communication, Optimization and Sciences (EEECOS)-2016 Simulation of lung representing the diseases – Bronchial Emphysema and COPD using NI-Multisim and LabVIEW Madhan Djearadjane [1], Soundarya Rangarajan [2], Aditya L. Kashyap [3], Manoj Kiran [4], T Jayanthi [5] [1] [2] [3] [4] [5]Department of Bio-Medical Engineering, SRM University,Kattankulathur, Chennai, India madhand8@gmail.com, jamunasow@gmail.com, adiketchup@gmail.com, jayanthi.t@ktr.srmuniv.ac.in Keywords: Medical simulation, Bronchial Emphysema, COPD, Multisim, LabVIEW. Abstract The purpose of our work is to develop a medical simulation system by an unconventional approach, to reduce the likelihood of a patient succumbing to a Ventilator Induced Lung Injury (VILI) or Ventilator Associated Lung Injury (VALI). Ventilator despite being a saviour for patients whose respiratory systems are compromised is also capable of aggravating the pre-existing anomaly if not used properly. In our work, we have used analogies to remodel and represent the respective first approximation electrical circuit equivalent of the pathological lung, which mimic the pathophysiology of Bronchial Emphysema and Chronic Obstructive Pulmonary Disease (COPD). The idea is to simulate the virtual lung using real time ventilator-parameters and check the responses of the lung, to arrive at model based inferences and extrapolate the physiological lung's conditions to the current ventilator patterns so as to reduce the likelihood of ventilator related hazards. We observed typical waveforms of the compliance of the lung which by our analogy depicts the functionality of the pathophysiological lung. Through real time simulation and circuit response analysis, the ventilator parameters can be adjusted to suit the needs of the patient thereby reducing any unintended damage to the lung. 1 Introduction Respiration as we know is the movement of air from outside the body to the cells inside tissue resulting in the simultaneous expulsion of carbon dioxide and any anomaly that prevents this exchange from happening is called a pathology. Lung diseases are basically of two types: Obstructive and Restrictive [1]. The primary symptoms of obstructive and restrictive lung diseases are similar except the fact that the diseases involving obstruction cause narrowing of the airway causing an abnormally high volume of air to linger in the lungs even after forceful exhalation. The diseases we have considered for our work are of the former type. Chronic Obstructive Pulmonary Disease (COPD) is a long term lung disease presenting with a cluster of conditions, referred to by different names based on the severity and the parts of the lung affected [2]. The typical clinical symptoms of COPD are: shortness of breath, tightness in chest, accumulation of mucus and coughing up of mucus. Bronchial Emphysema is not a severe condition by itself but is a hyponym of the condition COPD. Chronic bronchitis as the name suggests, is an inflammation of the bronchus and accumulation of mucus in the airways. At the tissue level, Bronchial Emphysema affects the deeper bronchioles and the alveoli and COPD affects the left and the right bronchus, bronchioles and the alveoli. Lungs are spongy tissues that help in respiration. When the lungs lose their ability to perform their destined function with spontaneity, the patient finds it difficult to breathe. When such a situation arises, there is a need for an external support. Mechanical ventilation is a method of artificially providing oxygen to an incompetent respiratory system either because of an ailment or a trauma [3, 4]. The problem gets complicated when the mechanical device intended to provide respiratory assistance, causes unintended harm to the patient. According to the National Trauma Institute, 40-50% of the cases admitted in the ICU succumb to VALI [5]. In India, the possibility of a patient succumbing to some form of ventilator related injury is far more likely and has been found to vary between 50 and 60 percent [6, 7]. We have used this superficial knowledge of lung physiology and existing clinical problems to come up with a ventilation assessment unit that virtually analyses the ventilation parameters by checking the response of an electrical analogous lung and provide insight as to how the parameters can be changed to effectively ventilate a lung and reduce the negative effects caused therein. 501 3rd International Conference on Electrical, Electronics, Engineering Trends, Communication, Optimization and Sciences (EEECOS)-2016 2 Previous Work The need to come up with a safe ventilation strategy has been considered carefully and solutions have been provided from a clinical point of view. All the work to reduce the negative effects of ventilation has been through the careful monitoring and manipulation of tidal volume (Tv) and PEEP components of ventilation [8]. The base reference for our work is Tinku Biswas et al’s [9] concept that represents the physiological lung in its electrical equivalent to study the step and ramp responses of the lung and compare the decay time for the respective transfer function. The conclusion was that, the alveolar compliance is directly proportional to the stability of the lung. Figure 2: Remodelled electrical analogue of COPD Zhongai He et al’s [10] technique to recreate the clinical conditions of a patient-ventilator using LabVIEW and Simulink, used a muscle driven pressure system virtually to study the response of the respiratory system during manual control of ventilator output, was also considered to model our system. Much of the existing work concentrates on building virtual patient-ventilator systems and very less work exists on assessing a ventilation system prior to its prescription to a patient. 3 Project Overview Figure 3: Transient analysis output for the remodelled circuit We have used three familiar software to devise the model and experiment with. The software is enlisted below: • NI-Multisim • MathWorks MATLAB • NI-LabVIEW 3.1.2 MathWorks MATLAB 3.1.1 NI-Multisim Mutisim is a powerful electronic schematic capture and simulation program that we used to construct and remodel our virtual lung model in [11]. The remodelled circuit of ‘Bronchial emphysema’ and ‘COPD’ are shown in figure 1 and figure 2. The software was also used to perform transient analysis of the modelled circuit to arrive at inference of dynamic stability of system. Figure 3, shows the transient analysis for different values of R, L, C is shown in the following figure. MathWorks MATLAB was used as a coding platform to simulate step and ramp responses to arrive at an interpretation of decay times of the circuit [12]. We exploited the concept that, the airway resistance and compliance of the alveoli of the physiological lung are analogous with electrical component properties of resistance and capacitance respectively. The proof of concept has been provided by step & ramp response simulation in MATLAB. Figure 4: Step response for a set of values of R, L, C Figure 1: Remodelled electrical analogue of Bronchial Emphysema 502 3rd International Conference on Electrical, Electronics, Engineering Trends, Communication, Optimization and Sciences (EEECOS)-2016 4 Results Table 1 shows the step and ramp response simulations for the circuits remodelled which is a proof of concept that the analogy actually exists. The decay time of the step and ramp responses is almost the same which indicates the stability and response of systems for different inputs. Figure 5: Ramp response for the same set of values as in figure 4 R L C 0.001 Step Response Decay Time(s) 0.25 Ramp Response Decay Time(s) 0.3 1 0.17 10 0.17 0.0001 0.50 0.50 50 17 0.0001 60 65 3.1.3 LabVIEW LabVIEW is a user controllable interface that was used in our work to simulate the modelled circuit in real time. The circuit constructed in Multisim was imported into LabVIEW and the “control and simulation module” was used to simulate the circuit. Table 1: Step & Ramp response decay times for different values of R, L, and C Figure 6: Front panel of LabVIEW simulation Figure 7: Block Diagram of LabVIEW simulation Figure 8: Step Reponse for case 2 Figure 6, 7 represent the LabVIEW based user controllable screen. The Front panel is an operational unit for the user to control and simulate the medical condition. Since the ultimate aim is to develop a virtual ventilation assessment system, we went on to import the remodelled circuit into LabVIEW and control the analogous circuit from LabVIEW’s front panel. Figure 9: Ramp response for case 2 503 3rd International Conference on Electrical, Electronics, Engineering Trends, Communication, Optimization and Sciences (EEECOS)-2016 Figure 13: Block diagram for pressure cycle loop Figure 10: Step response for case 3 Figure 14: Block diagram for volume cycled loop Figures 13, 14 represent the corresponding block diagram of figure 12. Conclusion & Future Work Figure 11: Ramp response for case 3 Figures 9, 10, 11 represent the step and ramp response curves for different stages of severity of the diseases considered. Figure 12: Front panel of the intended simulation screen Figure 12 represents the user controllable screen of our intended model. The user can select the disease he wants to simulate, can select the mode of ventilation for respiratory support and control the tidal volume (T v) / pressure of air delivered to the patient by controlling the analogous voltage input to the circuit. The system is a ventilation assessment module which can be used for real time simulation, for clinicians and professionals to learn and visualize the behaviour of a physiological system to a crude input before dealing with the reality, which we believe would help them to take appropriate decisions not only to support the life of the patient but also to minimize the negative effects of the procedure itself and decrease the postoperative care required and speed up recovery. Currently, the project has covered only 2 diseases at a superficial level. The physiology of the lung is to be studied extensively to get a detailed approximation of each of the components of the lung. Once the model is ready, the electrical analogous concepts can be used to exploit the physiological functioning of a lung, purely in electrical terms, thereby creating a completely user definable virtual model of a lung. The scope of the project can be extended to simulation of other major diseases that require a ventilator support and are susceptible to ventilator associated injuries. Trainees can use the software to simulate and safely analyze a lungs condition to ventilator settings. The software is user friendly, user designable, user definable and user controllable. The software could also be used by medical trainees for simulation purposes for medical training. It could give us a quick real time analysis before the patient is subjected to a ventilator. 504 3rd International Conference on Electrical, Electronics, Engineering Trends, Communication, Optimization and Sciences (EEECOS)-2016 References [1] "Lung Diseases Overview", WebMD, 2016. [Online]. Available: http://www.webmd.com/lung/lung-diseasesoverview. [2] C. Disease and A. Medicine, "Chronic Bronchitis and Chronic Obstructive Pulmonary Disease (ATS Journals)", American Journal of Respiratory and Critical Care Medicine, 2016. Journal of Physiology-Lung Cellular and Molecular Physiology 282.5 (2002): L892-L896. [9] Biswas, Tinku, et al. “An Electrical Model for Bronchitis and Emphysema of Human Respiratory System”, IJMER Volume-2 Issue-5, Sep-Oct 2005. [10] He, Zhonghai, and Yuqian Zhao. “Modeling in [3] "Ventilator Management: Introduction to Ventilator Respiratory Movement Using LabVIEW and Simulink. Management, Modes of Mechanical Ventilation, Methods of Modeling”. Software: 137-160. Ventilatory Support", Emedicine.medscape.com, 2016. [11] Borrello, Mike.” Biomedical systems: modeling and [Online]. Available: http://emedicine.medscape.com/article/810126-overview. simulation of lung mechanics and ventilator controls design. VisSim tutorial series”. Boston(1997). [4] Ventilation Options for COPD-Topic Overview, WebMD, [12] Mathworks - Makers Of MATLAB And Simulink. 2016. [Online]. In.mathworks.com. N.p.,2016. Web. 15 Apr. 2016. [5] "National Trauma Institute", Nationaltraumainstitute.org, [13] Downham, Mechanical Ventilation Series2016. [Online]. Available: Pressure/Volume loop. - Critical Care Practitioner, Critical http://www.nationaltraumainstitute.org/home/ventilatorinduced-lung-injury.html. Care Practitioner, 2016. http://www.jonathandownham.com/mechanical-ventilation- [6] A. Vasudevan, R. Lodha and S. Kabra, "Acute lung injury series-pressurevolume-loop/. and acute respiratory distress syndrome",Indian J Pediatr, vol. 71, no. 8, pp. 743-750, 2004. [14] Hall, John E. Guyton and Hall textbook of medical physiology. Elsevier Health Sciences, 2015. [7] N. de Prost, J. Ricard, G. Saumon and D. Dreyfuss, Ventilator-induced lung injury: historical perspectives and clinical implications, Ann Intensive Care, vol. 1,no. 1, p. 28, 2011. [8] Gahlot, Luxmi, Eric B. Milbrandt, and James Snyder. Higher initial tidal volumes associated with the subsequent development of acute lung injury in dose-response. American [15] Ganong, William F., and Kim E. Barrett. Review of medical physiology. Norwalk, CT: Appleton & Lange, 1995. [16] Pilbeam, Susan P., and Jimmy M. Cairo. Mechanical ventilation: physiological and clinical applications. Mosby, 2006. 505 3rd International Conference on Electrical, Electronics, Engineering Trends, Communication, Optimization and Sciences (EEECOS)-2016 [17] Tobin, Martin J. Principles and practice of mechanical ventilation. (2006): 426. 506