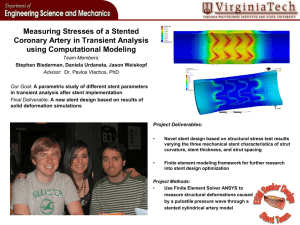
TCTAP C-047 Complete Percutaneous Revascularization in Three
advertisement

19th CardioVascular Summit: TCTAP 2014 TCTAP C-046 Stent the LAD Kiss the Circumflex [Clinical Information] Patient initials or identifier number: Mr SRK Relevant clinical history and physical exam: 60 years old male was admitted in an outside hospital with extensive anterior wall MI. He was thrombolysed with Streptokinase. He was referred to our hospital in view of post infarction angina. Pulse rate - 102/ minute BP was 100/70 mmHg Killip Class II on presentation Relevant test results prior to catheterization: Hb- 12 gm%, TC 6700/mm3 S.creatinine -1.3 mg%, Potassium -3.6 meq/L ,Sodium - 138 meq/L HIV ,HBSag, HCV screening negative. ECG - Persistent ST elevation in Anterior leads with RBBB Relevant catheterization findings: LMCA - Distal 70% stenosis with thrombus. LAD -Type 3 Vessel, proximal 90% stenosis. Distal mild disease. LCX - Ostial mild disease. RCA - Proximal 70 - 80% stenosis [Interventional Management] Procedural step: 7F Right Femoral Artery Access. The LMCA was cannulated with a 7F EBU 3.5 catheter. A Fielder FC wire was used to cross the lession in LAD. The lesion was pre dilated multiple times with 2x10 Pantera PTCA balloon A 2.75x23 DES was deployed from LMCA to LAD at 10 Atmospheres. The distal part of the stent was post dilated with a 3x8 followed by 3x15 Pantera Leo PTCA balloon and proximal part of the stent was post dilated with 3.5 x8 PTCA Pantera Leo Balloon .Check angiogram showed TIMI III flow in LAD but pinching of LCX ostium. Another Fielder FC wire was used to enter the LCX. A kissing balloon inflation was done with 3.5x8 Pantera Leo balloon in LAD and 2.5x8 Pantera in the LCX. Final angiogram done showed well deployed LAD stent with TIMI III flow in both LAD and LCX and no pinching of LCX ostium. TCTAP C-047 Complete Percutaneous Revascularization in Three Vessels CAD Using Drug Eluting Bifurcational Stent Axxess and Closing of Pseudoaneurysm with Double Approach Farhat Fouladvand Holy Family Hospital (Ospedale Sacra Famiglia)- Hospitaller Order of St. John of God, Italy [Clinical Information] Patient initials or identifier number: LA Relevant clinical history and physical exam: Our case presents a clinical and interventional management of a 50 years old man that have had a craniological visit for am atypical chest pain. His clinical history was almost silent, but his risk factors were plurals, like diabetes, hypertension, dyslipidaemia, obesity and smoking. Relevant test results prior to catheterization: According to the most popular risk stratification schemes the patient enters in the high risk group, so the colleague decided to perform a stress test, that was positive for ECG criteria in inferior and lateral leads. Relevant catheterization findings: Thus the patient was admitted in our hospital for elective coronary angiography that was performed by radial approach and revealed a three vessel CAD in left coronary dominance. We had a tight lesion on the bifurcation LAD/D1 (Medina 1.0.0) with another significant lesion on the mid part of LAD. The circumflex artery (Fig. 1) presented a significant lesion at the bifurcation with the first marginal branch (Medina 1.1.0) and the non dominant right coronary had lesions at its proximal and mid part. Now the difficulties in taking the decision were what type of revascularization to choose. The patient EuroSCORE was zero, so his logistic score talks about something like 0,88% perioperative mortality. On the other hand his SYNTAX SCORE was 19 considering the stenosis on his non dominant coronary artery, so hi enters in the low risk for PTCA group. Same his Global Risk Score was very low. So we decided to treat the patient by percutaneous approach. [Interventional Management] Procedural step: During the same catheterisation session we performed direct stenting of the mid (Biomatrix 2.5 x 12 mm at 18 Atm) and proximal (Biomatrix 2.75 x 14 mm at 18 Atm) lesions of his right coronary artery. We had to use a long sheath as the patient has an important tortuosity of the brachial artery. Once completing the PTCA on the RCA we shift the catheter from HS to EBU 3.5 through the long sheath and performed the provisional stenting of the JACC Vol 63/12/Suppl S j April 22–25, 2014 j TCTAP Abstracts/CASE/Bifurcation and Left Main Stenting Downloaded From: https://content.onlinejacc.org/ on 10/02/2016 S95 CASES Suresh Davis, Amit Bhushan Sharma, C. Raghu Almas Hospital, India bifurcation stenosis of LAD (Biomatrix 3.5 x 18 mm at 16 Atm). No kissing balloon was used as the result and flow through the diagonal branch was optimal. Then we placed a second stent after pre-dilatation (Maverick 2.0 x 20 mm at 10 Atm) on the stenosis at the mid LAD (Biomatrix 3.0 x 18 mm at 16 Atm). Both stents were post-dilated at high pressure with non-compliant balloon (NC Apex 3.5 x 15 mm at 20 Atm). As the patient was relatively tired, and we have used about 200 ml of contrast media and as the choice for treatment of the circumflex artery was Axxess stent that need a 7F catheter we postponed the procedure on CX for the next day. On the next day we used the right femoral access. As a practice in our Cath lab we always perform an angiographic control of the femoral access site that demonstrates a good puncture level and absents of leakage. The angiographic control of the previous day PTCA on RCA and LAD demonstrated a good result. Once placed a 7F EBU 3.5, two BMW wires were positioned in the distal part of CX and first marginal branches. Predilatation of the lesions were done (Maverick 2.0 x 20 mm at 10 Atm), and then a dedicated drug eluting biforcational self expandable stent (Axxess 3.5/14 mm) was released at the carina. Once in position the Axxess stent we placed a second drug eluting stent (Biomatrix 2.25 x 18 mm at 16 Atm) on the distal CX in overlapping with the Axxess stent. The final angiographic result was optimal (Fig. 2). Unfortunately, on the next day we noticed a presence of false aneurysm at the site of femoral puncture as well demonstrated by vascular ultrasound. In our hospital we had once a case of dramatic occlusion of the femoral artery by the injection of thrombin, we adopted a method of occlusion of pseudoaneurysm with double approach using a radial access site for placing a balloon in the femoral artery and eco guided injection of thrombin. So we access the femoral artery using the radial artery and we performed the angiography control that confirmed the presence of pseudoaneurysm. Then we placed a 6 mm peripheral balloon in the femoral artery. Once inflated the balloon at pressure just to stopped the flow, under the eco guidance we injected in the pseudoaneurysm sac the thrombin (Fig. 3). The control angiography and vascular ultrasound confirmed a complete closure of the pseudoaneurysm. At the end of the procedure the patient demonstrated a neurologic deficit. Immediately we administered to him 5000 IU of UFH and 500 mg ev of aspirin. After 12 hours the patient was completely asymptomatic. And the ST scan at 48 and 72 hours were negative for ischemic lesions. The patient was discharged in perfect conditions with the standard double antiagregation (acetylsalicylic acid and clopidogrel). This case demonstrates that in multi vessels CAD it’s mandatory to adopt the calculation of EuroSCORE and SYTNAXSCORE to weight the risk and benefit of the different type of revascularization. Moreover it’s a good practice to perform a complete revascularization during the same hospital stay. Obviously the chose of the access site must prefer the less invasive as it is for the radial. According to our experience and the available data the first choice for treatment of a bifurcation should be one stent strategy (provisional stenting), but if the lesion requires different technic the new dedicated for the bifurcation drug eluting stent Axxess can be a good solution. And last but not least the complication must be treated with the competence adopting innovative strategy and done by experienced operators. 19th CardioVascular Summit: TCTAP 2014 CASES Relevant catheterization findings: Coronary angiography showed occlusion of proximal right coronary artery (Figure 1) and severe stenosis of ostial Left Main (Figure 2). [Interventional Management] Procedural step: A second degree AV block appeared with subsequent cardiac arrest due to pulseless electric activity. The patient was immediately assisted with cardiopulmonary resuscitation, orotracheal intubation and intraaortic balloon pump. Percutaneous coronary intervention with stent implantation (DRIVER 3.5x9 mm, Medtronic) was performed on left main (Figure 3) and then on the right coronary artery (XIENCE PRIME LL 3X38 mm) (Figure 4). Intravascular ultrasound (Eagle Eye, Volcano Corporation), performed after ballon angioplasty before stent implantation revealed severe post-irradiation ostial stenosis of both coronary arteries and ulcerative plaque in the proximal segment of RCA (Figure 5). The echocardiogram showed a severe dysfunction of left ventricle because of global hypokinesia and akinesia of inferior wall. The patient was supported with adrenaline, noradrenaline and dopamine and monitored invasively. After 24 hours the lactate trend was lowering and all parameters were stable and improving. Case Summary: We describe a case of 50 years old man with 3 vessels CAD (two stenosis on RCA, one bifurcation stenosis on LAD/D1 and another bifurcation on CX/OM1) in left dominance. After the diagnostic catheterization we performed PTCA with DES on RCA and LAD by radial approach, and the next day we treated the CX/OM1 from femoral approach with placing a bifurcation dedicated drug-eluting self-expandable stent Axxess. After that he developed a pseudoaneurisma at the femoral site, that we treated by double approach: inflated balloon in the femoral artery and under echo guidance injection of thrombin with success. The patient was discharged without any symptoms. TCTAP C-048 PCI in Acute Myocardial Infarction Evolving in Cardiogenic Shock Due to Uncommon Cause Gabriele Gabrielli Azienda Ospedali Riuniti, Italy [Clinical Information] Patient initials or identifier number: M.T. Relevant clinical history and physical exam: A 38-years-old man, with a history of Non-Hodgkin lymphoma treated with mediastinal irradiation 15 years before and mild hypercholesterolemia, was urgently admitted to our hospital with an acute inferior myocardial infarction within 60 minutes from symptoms onset. The patient was stable (Killip class 1). Relevant test results prior to catheterization: The ECG showed ST segment elevation in inferior leads. S96 JACC Vol 63/12/Suppl S Downloaded From: https://content.onlinejacc.org/ on 10/02/2016 j April 22–25, 2014 j TCTAP Abstracts/CASE/Bifurcation and Left Main Stenting