A 63 year old male patient presented with chest pain
advertisement

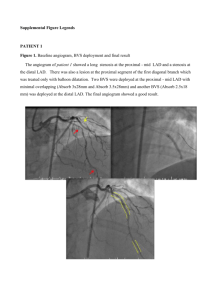
[ □Coronary □Non Coronary ] A case of repetitive subacute thrombosis Presenter: OOO /영문 Operator: OOO /영문 Institution: OOO/영문 Case summary: A 55 year-old male patient was transferred from local hospital. He had no specific cardiovascular risk factors except diabetes. He suffered severe chest pain 2 weeks ago and visited local hospital. Coronary angiography showed tight stenosis of proximal LAD and distal LCX. An unknown stent was implanted in the proximal LAD and distal LCX was dilated with a balloon. Four days later, he suffered severe chest pain again. Follow-up coronary angiography revealed subacute thrombosis in the proximal LAD and proximal LCX. After aspiration of thrombi from both coronary arteries, additional stents were implanted in the proximal LAD and proximal LCX. Despite of maximal medical treatment, severe chest pain was developed again 7 days later, and he was transferred to our hospital. Coronary angiography revealed focal moderate in-stent stenosis (50%) of proximal LAD with luminal haziness. The ostium of first diagonal branch (D1) was severely narrowed (90%). Distal LCX was occluded with anterograde TIMI I flow. There was also significant stenosis (75%) in the proximal RCA and distal RCA. The patient’s ECG showed Q wave in precordial leads, from lead V2 to V6. Because left ventricular end diastolic pressure was high (36 mmHg), PCI was deferred and patients received medication including heparin, tirofiban, aspirin, clopidogrel, and cilostazol. However, the patient complained of severe chest pain 5 days later. So the fourth coronary angiography was performed and revealed totally occluded stent in the mid LAD and small thrombi in the ostium of D1. A 6 Fr sheath was inserted through right radial artery and the left coronary artery was engaged with a 6Fr XB guiding catheter (Cordis). Coronary guidewires (Runthrough, Terumo) were inserted into LAD and diagonal branch, respectively. Thrombectomy was done using Thrombuster (Kaneka Medics) and red colored thrombi were aspirated. IVUS (40MHz Atlantis Pro, BSC) study revealed that stent in the proximal LAD is not fully expanded. The mid LAD lesion and D1 lesion were dilated with a 3.5x20mm balloon (16 atm, Maverick, BSC) and 2.0x14 mm balloon (16 atm, Mercury, Abott), respectively. Then lesions were dilated again using kissing technique (simultaneous inflation at 12 atm). There was residual thrombus in the distal segment of LAD stent, so 3.5x20mm balloon was dilated within distal segment of stent again. Full expansion of stent was confirmed by IVUS study. Follow-up angiography performed 4 days later showed no residual thrombi. After discharge, triple antiplatelet agents were continued and the patient is asymptomatic for 4 months. Discussion: What is the best strategy for repetitive subacute thrombosis? Key pictures: Fig. 1. Baseline CAG Key Words: Fig. 2. Kissing balloon