Supporting children with speech, language and
advertisement

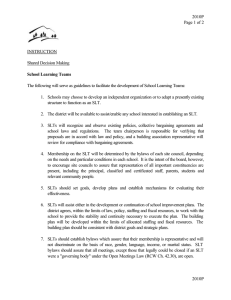
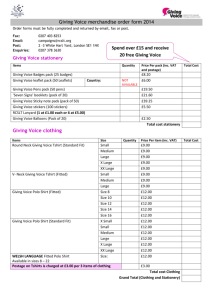
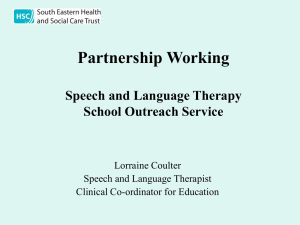
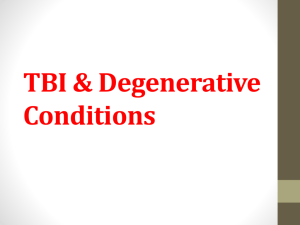
Supporting children with speech, language and communication needs within integrated children’s services Position Paper Marie Gascoigne January 2006 www.rcslt.org Referencing This document should be referenced as follows: Gascoigne M. (2006) “Supporting children with speech, language and communication needs within integrated children’s services” RCSLT Position Paper, RCSLT: London This document is available from the RCSLT website: www.rcslt.org 2 Supporting children with speech, language and communication needs within integrated children’s services Contents 1. Introduction 2. Reviewing the context 2.1 Changing context for children’s services across the UK 2.2 Commissioning integrated services for children 2.3 Delivering integrated children’s services through multi-agency models 2.4 Workforce review 2.5 Theoretical models for speech and language development 2.6 Current professional consensus 2.7 Summary of the context 3. Articulating the vision: focus on impact 3.1 Delivering effective support 3.2 Planning for maximum impact 3.3 Systems for strategy 3.4 Developing the workforce 4. Conclusions and way forward 3 www.rcslt.org Acknowledgements Many have contributed to the final version of this paper and much experience and professional expertise has been shared in debating and refining the key recommendations outlined as well as their underpinning principles. The 100 or so delegates to the Children’s Services event held in September 2004 enabled a representative sample of the professional membership to discuss models of service delivery and explore the professional consensus regarding ‘good practice’ in terms of the contribution of the speech and language therapist to the support of children with speech, language and communication needs. Thanks to all those who attended and to those who commented on drafts of the paper. This event was planned and facilitated by a steering group consisting of members of the RCSLT Education Committee alongside additional representatives from the four UK countries as well as the independent and voluntary sector: Mary Auckland, Pauline Bierne, Kate Davies, Sarah Fisher, Yvette Johnson, Rosie Jones, Maria Luscombe, Nita Madhani, Nigel Miller, Pat Mobley, Jane Oates, Judy Roux, Liz Shaw, Alison Stroud, Shelagh Urwin, Anne Whateley and Fiona Whyte. 4 Thanks also to members of the Professional Development Board and Management Board for helpful comments on drafts of the paper. The practice example boxes sited throughout the paper aim to bring reality to some otherwise abstract concepts. Examples evidence practice across the profession and individual contact details are available throughout the document. It has been particularly helpful to have had the contributions from representatives of the voluntary sector, especially ICAN and SLTs in independent practice. Particular thanks are due to the following individuals who have offered detailed comments and feedback at various stages of the development of this paper. James Law and Nicola Grove provided useful suggestions from an academic perspective, which were extremely helpful and have contributed significantly to the final structure of the paper. Finally, Sue Roulstone and Kamini Gadhok have not only contributed to the paper but have also provided advice and guidance throughout the process of producing this document. Supporting children with speech, language and communication needs within integrated children’s services Executive summary Introduction This paper has been written so that the Royal College of Speech and Language Therapists (RCSLT) can respond to requests from respective UK governments for the profession’s view and position regarding the role of the speech and language therapist (SLT) within the changing context and development of children’s services. The paper will also serve as a reference for speech and language therapy services, commissioners from health and education, and other key stakeholders. The RCSLT is aware of the need to define and develop best practice within the context of national policy frameworks and considers this paper as crucial in informing this work. A number of key policy initiatives over the past three to five years are analysed in section two. There is also a brief summary of theory underpinning intervention for communication disability. Together, these provide a convincing backdrop to the vision of future speech and language therapy services, which is set out in section three: Articulating the vision: focus on impact. The paper sets out 15 recommendations that support four key areas: • • • • Delivering effective support Planning for maximum impact Systems for strategy Developing the workforce As a member-led organisation, the RCSLT recognises the importance of involving the profession in the development of this paper in order to achieve consensus. Consequently, the paper sets out a framework that has been tested by the author with members from across the four UK countries, as well as from key groups, such as practitioners in independent practice, the voluntary sector and higher education institutions (HEIs). The RCSLT envisages that, as well as informing our joint working within each of the home countries, the paper will also provide SLTs with a framework to support local service development and delivery. However, the paper is not a service planning document. The aim of the paper is to capture and disseminate key principles that the RCSLT believes should underpin service commissioning and provision. It will therefore provide a framework that UK service planners and managers can use to develop services that will best meet the needs of children with speech, language and communication needs. The focus of the paper is the role of the SLT. However, the principles outlined could well be applied to other AHPs working with children and to other professional colleagues within integrated children’s services. The pace of policy development and change during the preparation of this paper is a testament to the modernisation agenda in public services. Consequently, the recommendations outlined within the paper are viewed as time-limited and a review will be necessary in 2008 – a significant time in so many of the policy agendas influencing the document. 5 www.rcslt.org Key area 1 Delivering effective support Recommendation 1: Any speech and language therapist (SLT) working with children should: • Identify the speech, language, communication or eating/drinking needs of the child as part of, or with reference to, the appropriate multidisciplinary team (this does not imply a static membership, more the team of relevant professionals for the individual child) • Identify the functional impact of these needs • Consider the most appropriate context for support ie. which settings are most relevant to the child and their family • Identify the contribution of the speech and language therapist as part of the wider team working with the child to meet the child’s needs – including the full range of options from advice to colleagues through setting up programmes to direct intervention where appropriate. Recommendation 2: Services should offer the full range of support for children, including direct intervention where appropriate, while ensuring overall management includes goals relating to activity and participation, managed by those most relevant the child. Recommendation 3: The RCSLT regards trans-disciplinary working as central to work with children. The RCSLT supports the exploration of SLT roles within trans-disciplinary models and the development of new models that maximise the contribution of SLTs while ensuring that the specialist contribution to the system is recognised as essential. Emerging key worker roles and lead professional roles are also central to this model of working if it is to be successfully implemented for the benefit of children and their families. Recommendation 4: Training of others, including parents, should be viewed a central activity for SLTs to maximise impact for the child and their family. Key area 2 Planning for maximum impact Recommendation 5: Service planning for children with speech, language, communication or eating/drinking needs should always be in partnership with other agencies. Recommendation 6: Service planning should take account of the most functionally communicative and socially appropriate environment for effecting change. Recommendation 7: There is a need to define the parameters of an appropriate advisory needs-based and dynamic approach to supporting children which integrates the concept of skill mix both within the profession and across professional boundaries. The term ‘consultative’ model should be replaced by a more accurate description of the service being delivered. The RCSLT supports the need for research to further define and investigate the impact of approaches, which rely on the implementation of speech and language therapy advice by others. Recommendation 8: Service structures should reflect the changing context. Highly specialist, principal and consultant therapists need to use time to train, develop, coach and mentor less experienced therapists, who in turn need to be given the opportunity to work with all caseloads. The most specialist need to focus their skills on the strategic developments within their specialist area. 6 Supporting children with speech, language and communication needs within integrated children’s services Key area 3 Systems for strategy Recommendation 9: The RCSLT recommends that within each local authority area there needs to be an SLT professional lead for children, who can interpret national policy and ensure partnership working occurs in terms of integrated commissioning of speech and language therapy provision, strategic planning and operational delivery. This professional lead should ideally be a member of key strategic multi-agency planning groups and be empowered to make key strategic decisions on behalf of local speech and language therapy services. The role of professional lead should also provide a focal point in terms of professional standards for all speech and language therapy provider services both within statutory and non-statutory provider organisations (including independent practitioners). Recommendation 10: The role of the SLT must be seen within the context of the specialist and wider workforce. Commissioners need to be aware of the unique contribution of SLTs across the population base. Recommendation 11: Managers and service leads should work together with their allied health professional (AHP) colleagues as well as colleagues from education and social care, in the development of new roles, in particular the development of consultants/specialist advisory posts and crossagency posts. Recommendation 12: Management opportunities across agencies and across professional boundaries should be developed. Key area 4 Developing the workforce Recommendation 13: The RCSLT supports the development of placements that offer student therapists a full range of opportunities as part of their practice-based learning and this would include working as part of trans-disciplinary teams. Recommendation 14: Speech and language therapists working with children should undertake continuing professional development (CPD) activities across health, education and social care in order to develop knowledge and skills that will prepare them for cross-agency roles. The RCSLT values CPD activities that are not limited to the health context. Recommendation 15: The challenges of the changing context mean that business and entrepreneurial skills sets will become more relevant for senior managers. Excellent communication and negotiation skills should also be developed by all speech and language therapy service leads as part of a portfolio of leadership competence. 7 www.rcslt.org 1. Introduction This paper has been written so that the Royal College of Speech and Language Therapists (RCSLT) can respond to requests from respective UK governments for the profession’s view and position regarding the role of the speech and language therapist (SLT) within the changing context and development of children’s services. The paper will also serve as a reference for speech and language therapy services, commissioners from health and education, and other key stakeholders. Approximately 70% of the 10,000 SLTs registered in the UK work with children. It is estimated that approximately 6-8% of children aged between 0-11 years have speech, language and communication needs1. The prevalence for children with severe and complex needs may be a further 1%. The RCSLT is aware of the need to define and develop best practice within the context of national policy frameworks and would consider this paper as crucial in informing this work. As a member-led organisation, the RCSLT recognised the importance of involving the profession in the development of this paper in order to achieve consensus. Consequently, the paper sets out a framework that has been tested by the author with members from across the four UK countries, as well as from key groups such as practitioners in independent practice, the voluntary sector and higher education institutions (HEIs). 8 The RCSLT envisages that, as well as informing our joint working within each of the home countries, the paper will also provide SLTs with a framework to support local service development and delivery. However, the paper is not a service planning document. Its aim is to capture and disseminate key principles that the RCSLT believes should underpin service commissioning and provision. It will therefore provide a framework that UK service planners and managers can use to develop services that will best meet the needs of children with speech, language and communication needs. The focus of the paper is the role of the SLT. However, the principles outlined could well be applied to other allied health professionals (AHPs) working with children and to other professional colleagues within integrated children’s services. The pace of policy development and change during the preparation of this paper is a testament to the modernisation agenda in public services. Consequently, the principles outlined within the paper are viewed as time-limited and a review will be necessary in 2008 – a significant time in so many of the policy agendas influencing the document. Supporting children with speech, language and communication needs within integrated children’s services 2. Reviewing the context 2.1 The changing context for children’s services across UK The legislative and policy agendas for children’s services across the four UK countries have moved in the same direction over the past three to five years, albeit with some local variations. A useful summary is available in the 4 Nations Child Policy Network, showing the policy and legislation affecting children2. The common themes that emerge across the UK include: • The need for statutory services to integrate delivery of services around the child and their family. Examples of this include the development of Sure Start (Sure Start Scotland, Sure Start NI, Cymorth in Wales) initiatives such as Children’s Centres 3 4 5 6, the Early Support Programme7 and the development of Children’s Trusts or their equivalent 8 • While terminology may differ from country to country, a recognition that all agencies working with children have a key role to play in all aspects of the child’s development in order for them to achieve the five outcomes to: i. Be healthy ii. Stay safe iii. Enjoy and achieve iv. Make a positive contribution v. Achieve economic well-being 9 • A focus on inclusion of children with special (or additional) needs in mainstream settings and the need for specialist services to be delivered flexibly in order to enable inclusion 10 11 12 13 • Emphasis on targeting services to address inherent inequalities due to disadvantage of whatever sort (Sure Start initiatives, Looked After Children). • The move to developing primary care services and the increasing focus on health promotion14 • Recognition of a changing workforce profile and the need to examine and redesign professional roles focusing on the competences required to deliver new integrated services 15 16 Figure 1 In England, the papers Creating a Patient-led NHS 17 and Commissioning a Patient-led NHS 18 signify far-reaching changes to the mechanisms for service provision. Therapists working in children’s services may in the future be providing care for children whilst being employed by local authority-based children’s trusts, new therapy organisations (including companies limited by guarantee, charitable organisations, independent provider consortia), or possibly as employees of foundation hospitals. The key themes of contestability and plurality in these policy papers will result in the need for services to be offered in ways that offer commissioners (whether from health, education or social care) packages that are clearly understood in terms of positive impact on the relevant population. It will also be critical for SLTs and other colleagues to become involved in commissioning in order to influence the commissioning processes and ensure that the added value of therapists is understood. The challenge for SLTs, along with other AHPs, and colleagues in education and social care, is to respond to this changing context proactively and creatively. In order to respond, it is necessary to have a clear understanding of the key drivers and resistors that are in play and to be able to develop creative solutions. There are capacity issues, both in terms of numbers of individuals needed to deliver the agenda, but also in terms of competences needed. New roles require different skill sets. A change programme as significant as that which we are experiencing for children’s services across the UK will need to address capacity issues at every level, from pre-registration to expert practitioner, and also in terms of management and leadership capacity. Figure 1 (below) represents the key issues as a ‘forcefield’ 19 diagram. This identifies key themes clearly and sets the framework for exploration of these issues in this paper. Force field diagram showing key drivers and resistors within the context of integrated children’s services Legislative and policy framework Challenge of communicating the scope and scale of the proposed change Workforce strategy Professional expectations of the familiar career framework Services built around the child facilitated by new organisational structures Services currently build around historical structures with embedded organisational cultures 9 www.rcslt.org 2.2 Commissioning integrated services for children Commissioners for children will take overarching policy leadership for children’s services across the traditional boundaries of health, education and social care nationally 20 21 22. These posts are established in England, Wales and Northern Ireland, whilst in Scotland the Scottish Executive is evaluating the added value that a single commissioner would give 23. Locally, services will see the appointment of directors of children’s services or lead chief officers for children (Wales 24) whose role will be to ensure redesigned services meet the needs of all children, including those who are vulnerable and/or have additional specialist needs, as locally and flexibly as possible. Vulnerable children and those with additional needs form part of the population of ‘all children’. In an inclusive society, specialist and targeted services for these children should be integral to universal mainstream provision. The integration of education, health and social care for children means they should be able to access all the services they require – whether universal, targeted or specialist, flexibly and locally wherever possible. Figure 2 (right) shows how the range of services and the needs of the child population interface. For example, children with additional needs may access universal, targeted and specialist services from all agencies, while the majority of children will access universal service only. Integrated services may or may not take the form of children’s trusts. For example, in Wales, children and young people partnerships within each local authority area provide a similar function. In Scotland, community health partnerships bring together health, education and social services. In all cases the single commissioner for children (or equivalent in Scotland) will ensure services are commissioned in an integrated way and that joint funding streams are established as appropriate. The aim is to avoid duplication of services and use resources in a more effective way. Within the health sector, the implementation of practicebased commissioning highlights the need for a full understanding of the scope of practice of SLTs and range of service delivery for children with speech, language and communication needs. Equally, commissioners in education and social care (including head teachers as well as children’s trust commissioners) will need to accept greater responsibility for commissioning aspects of the services provided for children with speech, language and communication needs. The use of ‘pooled budgets’ under Section 31 of the Health Act 1999 25 is an example of existing mechanisms for integrating resources and the services they fund. There are relatively few examples of these processes being used to provide more effective support for children with speech, language and communication needs. However, the use of aligned budgets, where many of the flexibilities of a pooled budget are possible but the financial accounting systems retain the budgets within individual organisations, is beginning to increase. The development of children’s trust arrangements will no doubt result in a greater focus on these flexibilities. 10 Figure 2 Population of children and the services provided Specialist services Targeted services Universal services Children with additional needs Vulnerable children All children Practice example 1 Example 1a – Pooled budget The Medway pooled budget was set up in 2000 using matched funding from Medway PCT and Medway Council to meet the speech and language needs of children in special educational placements and mainstream primary schools in the Medway towns. The Medway Communication Team supports children in mainstream primary schools from year one to their transfer to secondary school. It is a multidisciplinary team consisting of therapists, specialist language teachers and two SLT technicians – one for speech sounds and one for social skills. The skill mix enables children who need to be seen by a therapist to have access to one, while allowing all children with speech and language difficulties access to SLT support. Contact Dawn West on 01634 812858 or dawn.west@nhs.net Example 1b – Aligned budget The integrated speech and language therapy service for children in Hackney is a service jointly managed across City & Hackney PCT and The Learning Trust (the body responsible for education in Hackney) and staff are employed flexibly on either PCT or Learning Trust contracts and terms and conditions. The budgets are held separately in each organisation, but there is one manager with overall responsibility for the service who is supported by management accountants in both organisations. This method of working has allowed the service to move forward operationally at a greater pace than might have been the case had formal ‘pooled budgets’ been pursued. Contact Marie.Gascoigne@chpct.nhs.uk Supporting children with speech, language and communication needs within integrated children’s services 2.3 Delivering integrated services through multi-agency models The delivery of services through integrated systems and processes has been conceptualised within the Every Child Matters framework as shown in the diagram below 26. This model shows the importance of integrating thinking at every level to provide an integrated package as an outcome to the child. In Early Years these changes are being effected through the development of children’s centres and the mainstreaming of Sure Start and similar initiatives27. Early education is provided alongside family support and relevant health services (including speech and language therapy specifically). Extended schools and learning communities provide a similarly community-focused base from which families can access services for older children and young people. ency Gove rn g A rt e d Stra an te e gr a c t t In rate d Pro e gy e eg o n t - c ess t Lin In d F r e e ty i lie ni Fam Parents very Outcome for children and young people e li Inte g s te D ra In In England, the use of the of the Early Support Programme targeted at the child with complex needs introduces the concept of a key worker or lead professional to guide the family through the maze of support needed for their child. Other examples of this approach include the wraparound project in Northern Ireland 28.These and other programmes embrace the ‘team around the child’ 29 approach, where pathways are developed with the child’s needs at the centre and traditional professional pathways are secondary. s C o mm u 11 www.rcslt.org 2.4 Workforce review Integrated commissioning sits alongside workforce review and the emphasis on competency based profiling of roles. The RCSLT has been proactive in this area in recognising the need for a competency-based framework30 31. The Children’s Workforce Strategy32 emanating from the Department of Education and Skills (England) and the UK-wide Skills for Health33, share the ambition of redesigning the workforce to meet the needs of the service user without assuming restrictions of existing professional boundaries. These cross-disciplinary and crossagency reviews of competences, needed to deliver support for children with varying needs, present a challenge to all discrete professions. The RCSLT is actively encouraging SLTs to respond to these shifts in policy and engage in role redesign. Part of this process is to recognise which skills and competences are unique to an individual who has a professional registration as an SLT and which are shared with others (or could be shared with others). Alongside this, the opportunity to develop new roles across traditional professional and agency boundaries must be exploited. 2.5 Theory underpinning intervention for speech, language and communication needs Language is the unique attribute that defines us as humans; it is the key tool we use in shaping our understanding of the world, in transmitting our culture from generation to generation and in forming and maintaining social relationships. It is also the key/main medium of education. Children are surrounded by language and for those who have difficulties acquiring language, their difficulties pervade most aspects of their everyday lives – interactions with families, attempts to make and keep friends, learning about their world and their education. Children learn language in a social context that provides them with opportunities and motivation to interact and that provides feedback on the success of their communicative attempts. In order to effectively support children with speech and language impairments, interventions must consider how best to shape all these different contexts. As long ago as 1978, Bloom and Lahey 34, talked about intervention that addresses the entire communication context in terms of: • • • • Children’s opportunities to communicate Reactions children receive Topics of conversation that are available The language models (grammar, vocabulary, sounds) they hear • The modality used (adapted from Bloom & Lahey, 1978) The delivery of intervention following these principles requires a team around a child to structure the activities and interaction opportunities of a child’s everyday life. It is therefore necessary and appropriate for teams rather than sole SLTs to deliver intervention. Equally as important as the form, content and use of language, as outlined by Bloom and Lahey, is recognising the child and their communication within the wider context in which they exist. 12 Brofenbrenner’s Ecological Systems Theory 35 demonstrates the interaction between levels within the child’s environment and highlights the need to address issues and difficulties across the ecosystem in order to effect real change in the child. Figure 3 (top right) illustrates how the child is placed within the wider context and that the child’s development will be partly dependent on the feedback within the system with interactions at all levels. The understanding that the child in isolation cannot be meaningfully supported underpins much of the integrated children’s agenda outlined above. In terms of professional practice, the International Classification of Functioning, Disability and Health (ICIDH-2)36 classification of impairment, activity, and participation provides a framework for examining the focus for professional input within the wider context. This framework considers input in terms of the desired impact for the child. Intervention can be targeted at the following levels as shown in diagram opposite: • Impairment – within the child • Activity – addressing the impact of the impairment on the child’s ability to do certain activities • Participation – considering the impact of the impairment and restricted activity in terms of the child’s ability to participate as they would like within their particular context Supporting children with speech, language and communication needs within integrated children’s services Figure 3 after Brofenbrenner (1989) Societ y m un it y Com Fa m ily Child Interaction The focus for input When should SLTs be working at the level of impairment? Impairment Activity Assessment and diagnosis? Intervention? Participation Across all types of child? When should SLTs be working at the level of activity? i.e. working to address the impact of the impairment on the individual’s activities When should SLTs be working at the level of participation? Working to ensure that the individual opportunities for participating fully are maximised. Should this be all children? Vulnerable children? Children with specific additional needs? 13 www.rcslt.org 2.6 Current professional consensus – what is good practice? The RCSLT Clinical Guidelines by Consensus 37 published in 2005 following extensive consultation with expert groups within and beyond the profession, provide a comprehensive summary of the evidence base for different fields within speech and language therapy, including working with children across a range of disorders and a wide age range. • • • • • • Communicating Quality 2 (CQ2)38 provides the professional standards to which all registered SLTs agree to adhere. The third edition of Communicating Quality is due to be published early in 2006 and this will provide updated information that takes account of the significant changes in the external context over the past decade. In addition, delegates were asked to consider: Neither of these texts, however, provides information regarding the models of service delivery found to be most effective – the former focuses on the impairment level and the latter on professional standards. In order to inform this paper the RCSLT held a UK- wide forum on children’s services in September 2004. A representative sample of SLTs from across the four UK countries, as well as from statutory, voluntary and independent sectors, was invited to attend a one day event. Delegates were presented with the policy direction from all four countries and asked to consider a number of case studies. The case studies were explored in facilitated small groups. The brief was to consider the following issues within a potential future framework of integrated children’s services: 2.7 Summary of the context The Every Child Matters: Change for Children programme 39, while England-based, encapsulates key policy direction that is echoed in Scotland, Wales and Northern Ireland. The move towards integrating children’s services is a common direction of travel across the UK. The combination of changing legislative framework for children’s services, changing organisational infra-structure and changing workforce strategy results in a momentum for change which has not been evident in the past. The RCSLT and its membership need to be visionary in responding to the opportunities and challenges at this time. 14 What are the desired outcomes for the child? What interventions are required to achieve these? Why are these appropriate interventions? How can the desired outcomes be achieved? Where does the intervention take place? Who delivers the intervention? • Who commissions the interventions? • Who funds the interventions? Delegates were also asked to have in mind the need to consider the full scope of intervention based on the ICIDH-2 classification of impairment, activity, participation as outlined above. The outputs from the case studies indicated there is consensus regarding key features of good practice in terms of ensuring that the contribution of the SLT is set within a wider context in order to be effective and to have maximum impact on the child and their family. Clear themes include desired outcomes that highlight activity and participation goals as well as impairment goals, speech and language therapy interventions as part of a wider package of support, flexibility in terms of where and how support is delivered, and the need for SLTs to work as part of wider multi-professional and inter-agency teams. Supporting children with speech, language and communication needs within integrated children’s services 3. Articulating the vision: focus on impact 3.1 Delivering effective support Recommendation 2: In a continually evolving and dynamic system, it is not possible, or desirable, to identify ‘good practice’ as a narrow construct. However, in order to maintain a professional integrity in a rapidly changing context, it is necessary to identify some key elements that need to be present in any context where an SLT is working with children. Services should offer the full range of support for children, including direct intervention where appropriate, while ensuring that overall management includes goals relating to activity and participation, managed by those most relevant the child. Recommendation 1: Any SLT working with children should: • Identify the speech, language, communication or eating/drinking needs of the child as part of, or with reference to, the appropriate multidisciplinary team (this does not imply a static membership, more the team of relevant professionals for the individual child) • Identify the functional impact of these needs • Consider the most appropriate context for support ie. which settings are most relevant to the child and their family • Identify the contribution of the SLT as part of the wider team working with the child to meeting the child’s needs – including the full range of options from advice to colleagues through setting up programmes to direct intervention where appropriate. Figure 4 Figure 4 40 (below) illustrates how packages of support can be classified according to the lead responsibility and focus of intervention. The underlying philosophy is that if intervention and support are effective a child will typically follow the direction of the arrow. It is fully acknowledged that not all children will be able to move away from an SLT-led package. However, there is an important premise that for all children the need to have interventions, which are focused on activity and participation that are embedded within the relevant context, is essential. Service model for packages of support TRAINING LEAD RESPONSIBILITY school/setting parent other professional School run language group Individual speech programme with modelling SLT set up Language Group PCI Children centre based speech and language groups Speech and Language Therapist Individual assessment Speech Group Curriculum planning and differentiation Language for Thinking Package Social skills group Parent training with SENCO Playground games group Hanen Curriculum based/ classroom group Classroom Strategy Modelling Central training School INSET Training Staff training Social communication/ complex individual Individual language programme with modelling Home visit for therapy and modelling ‘Talking Time’ Individual assessment in context Participation Impairment FOCUS OF INTERVENTION 15 www.rcslt.org Recommendation 3: The RCSLT regards trans-disciplinary working as central to work with children. The RCSLT supports the exploration of SLT roles within trans-disciplinary models and the development of new models, which maximise the contribution of SLTs while ensuring the specialist contribution to the system is recognised as essential. Emerging key worker roles and lead professional roles are also central to this model of working if it is to be successfully implemented for the benefit of children and their families. The concepts of interdisciplinary and trans-disciplinary working are familiar in multidisciplinary teams and show the potential for service delivery to be streamlined for the child and their family when teams are working so closely together (Figure 5 – Models of multi-professional working 41). For this model to be successfully implemented it is essential that there is clear understanding about the individual professional contributions and that the transdisciplinary model is not intended to replace any of the disciplines, but to enhance the service to the child by ensuring that the child’s pathway is holistic. Figure 5 Within any team and/or context, the particular skills and competences of any individual team members will vary depending on their training and experience. The specific roles and responsibilities regarding the planning and delivery of any child’s care will therefore also vary. Because of this variation, these roles should be explicitly discussed and agreed by the team around the child. Strong professional leadership is essential to develop appropriate trans-disciplinary working models that provide a positive, integrated, streamlined experience for the child and their family, while ensuring quality is maintained with the necessary expertise within the system. When these factors are addressed, the trans-disciplinary model provides cohesive service delivery. Models of multi-professional working Multi-disciplinary working Interdisciplinary working Discipline A Discipline A CHILD CHILD Discipline B Discipline C Discipline B Discipline C Trans-disciplinary working A CHILD IN THE ENVIRONMENT B 16 C Supporting children with speech, language and communication needs within integrated children’s services Recommendation 4: Training of others, including parents, should be viewed as a central activity for SLTs in order to maximise impact for the child and their family If competences are to be shared effectively with students, less experienced members of the speech and language therapy profession, colleagues from other disciplines and, most crucially, parents, there needs to be greater understanding of the therapeutic process. Speech and language therapists training others require the skills to impart insight into the precise therapeutic interactions that make an activity a speech and language therapy tool as opposed to merely an activity. They also need the time to prepare training materials and deliver training as an integral part of the service delivery around a child and their family. Successful training of others involved in the child’s care is crucial to achieving real change for the child in terms of their speech, language, communications and eating and drinking skills. 3.2 Planning for maximum impact Recommendation 5: Service planning for children with speech, language, communication or eating/drinking needs should always be in partnership with other agencies. Recommendation 6: Service planning should take account of the most functionally communicative and socially appropriate environment for effecting change. This extends across the age range. Pre-school children should be supported in the home or early years setting if possible. The mainstreaming of Sure Start activities with clinic approaches will facilitate this shift and children’s centres and early years settings will become the most appropriate base from which pre-school services can operate. For children of school age, the school setting continues to be the most appropriate place for support. Practice example 2 Joint service planning for children’s services Example 2a The Bridgend Children with Disabilities Team is made up of social workers, day care support workers, family link workers, an SLT, occupational therapist and physiotherapist. The CWD steering group involves heads of service from the Therapies Health Directorate and social services, as well as the Children’s Partnership Coordinator. Thus planning is informed by three Bridgend statutory agencies. Contact Rosie Jones – Rosie.Jones@bromor-tr.wales.nhs.uk Example 2b Glasgow City Council – Provision for Children with Autistic Spectrum Disorder (ASD) • An interagency framework group made up of middle management representatives from education (including psychological services), social work, community paediatrics and speech and language therapy. • Developing an interagency approach to assessment, diagnosis, reporting, sharing information and supporting staff in mainstream schools which have children with ASD • Protocols for joint assessment and a format for joint reporting • Pack for mainstream schools: ‘Autistic Spectrum Disorder – Information and Procedures Pack’ targeted to head teachers • ‘Support and Development Group’ for mainstream staff who have or are anticipating children with ASD in their classes • A multi-professional seminar resulting in an Interagency Action Plan Contact Pauline Beirne – pauline.beirne@yorkhill.scot.nhs.uk 17 www.rcslt.org Recommendation 7: There is a need to define the parameters of an appropriate advisory needs based and dynamic approach to supporting children that integrates the concept of skill mix both within the profession and across professional boundaries. The term ‘consultative’ model should be replaced by a more accurate description of the service being delivered. The RCSLT supports the need for research to further define and investigate the impact of approaches, which rely on the implementation of speech and language therapy advice by others. The term ‘consultative model’ has not helped in conveying the key principles of transferring skills and competences to others in order that they can support children more effectively throughout their daily activities. It has been widely interpreted to mean anything from a once a year visit to a school for annual review, to a six week on, six week off model within mainstream school with an assistant taking over in the six weeks off (Law et al, 2000)42. Whatever approach to skill mix and sharing of competence, the key role for SLTs as trainers and educators is once again highlighted. The positive development of service models that draw on the skills of others within the child’s system – be they parents, teachers, learning support assistants or others – arose from the recognition that working at the level of impairment (see the ICIDH-2 impairment, activity, participation outline above) is in itself of limited value to the total life experience of the child if they are not also able to benefit in terms of activity and participation. Unfortunately, where models involving the delegation of tasks and programmes to others have been perceived as resource saving strategies, the positive reasons for such approaches have been lost. Fortunately, there are examples of positive models where others within the workforce around the child contribute to the achievement of speech, language and communication goals. This is important, as the demographics of the workforce continues to change significantly. The demographic data provided by the children’s workforce unit 43 predicts a dearth of highly trained professional individuals over the next 10 to 20 years. This shortfall in the potential workforce will be attributable to demographic and epidemiological effects rather than lack of opportunity for training. The development of new support worker roles is therefore a logical way forward and such roles are already emerging. For example, educational health workers who are education-based staff with specific training for supporting all health interventions for children in educational settings. These support workers are assistant practitioners in the sense they are implementing interventions devised by qualified professionals. However, in order to be in these roles they have had training and can demonstrate they have developed the necessary competences to support children within the educational setting. 18 Practice example 3 Multi-agency support worker roles Example 3a North West London Hospitals Trust Speech and Language Therapy Department and Harrow LEA Portage Service Speech and language therapy assistant and portage worker run the Early Bird Programme together in an Early Excellence Centre Contact Marie Luscombe – maria.luscombe@nwlh.nhs.uk Example 3b Independent SLT developing the role of tutors, teachers, support workers and classroom assistants through training in order that they can support the delivery of support for the child. Contact Sheilagh Urwin – family@urwin9969.freeserve.co.uk Example 3c Sure Start Hailsham and Eastbourne Downs PCT Speech and language therapy assistant and Sure Start home visitor work together to run the Basic Skills Agency Early Start programme. This is a programme for parents designed to improve basic skills and provide practice opportunities to develop play and communication with their young children. Contact Suki Ahsam – suki.ahsam@eastbournedownspct.nhs.uk Example 3d A speech and language therapist and assistant work with a designated teacher [usually the SENCo] and a designated TA in each school on a rolling programme. ‘Standard’ group programmes are demonstrated and then run by the school staff and cascaded to other staff as necessary. Initially the group programmes focused on children with additional needs and some vulnerable children, but over time it soon became clear that the benefits were much wider. Contact Mary Auckland – mary@aucklandsalt.fsnet.co.uk Supporting children with speech, language and communication needs within integrated children’s services Considering the ‘horizontal’ spread of competence implies role redesign that involves crossing boundaries at the professionally qualified level. That is, looking at other professional groups and considering where overlaps in skills and competence might make a sensible case for one or the other being involved rather than both. The ‘team around the child’ approach for disabled children is an example of a system that values individual professional contributions, but challenges assumptions about who does what and when 44. Figure 6 (below) presents a diagrammatic representation of the continuum of competences within the workforce and the impact of this on the point at which an SLT can safely delegate the delivery of interventions around a child. The decision-making process around where to draw this line for an individual child needs to be explicit. The concept of risk assessment will be useful in exploring the Figure 6 uniquely within the remit of a speech and language therapist parameters involved. Where there is a high level of competence within the child’s context, be that home, early years school or setting, it may be possible for the SLT to take on an appropriately advisory role. Where the competence is less certain, then the focus of the SLT, may be best placed in developing the competence in the environment. The key point is that the place ‘the line is drawn’ should be in response to the dynamic environment and not set in time or place. The concept of managing a child’s speech, language, communication or eating and drinking goals as part of the their daily routine, and therefore undertaken by the people who are part of that routine, should be seen as a positive option. This is not a dilution of a specialist resource, but the effective implementation of an ecological approach45 whereby the requirements of the individual child and the setting where the goals will be addressed are both taken into account. Continuum of competences could sit either with the SLT or with another can and should be handed on 19 www.rcslt.org Recommendation 8: Service structures should reflect the changing context. Highly specialist, principal and consultant therapists need to use time to train, develop, coach and mentor less experienced therapists who in turn need to be given the opportunity to work with all caseloads. The most specialist should focus their skills on the strategic developments within their specialist area. The highly experienced therapist should be used as a true ‘consultant’ in the sense that they can be clinically accountable for a team of less experienced but qualified registered practitioners. They in turn advise a team of assistant practitioners and/or students in delivering the programmes. The more senior therapist may have an overarching responsibility for the delivery of services to a large number of children without being directly involved themselves for the majority of their time. This would necessitate examining roles at every level, as the senior practitioner may have direct regular contact with a very small number of families at any one time. The allocation of children and families throughout the team will be based on clearly defined criteria at specific times in their pathway through a service. Empowering the newly qualified practitioner and valuing the expert are equally important for future service delivery. Practice example 4 Perth & Kinross SLT Surestart Project The SLT Department is running a Sure Start funded project that is extending the role of the SLT assistant. Two NNEB(Equivalent)-trained staff have been recruited. Following extensive in-house SLT training the SLT(A)s are providing direct therapy programmes to children in nurseries under the supervision of therapists. Initial results show positive outcomes for children, parents, nursery staff and therapists. Contact Jeanette Seaman – jeanette.seaman@tpct.scot.nhs.uk 20 3.3 Systems for strategy Recommendation 9: The RCSLT recommends that within each local authority area there needs to be an SLT professional lead for children, who can interpret national policy and ensure that partnership working occurs in terms of integrated commissioning of speech and language therapy provision, strategic planning and operational delivery. This professional lead should ideally be a member of key strategic multi-agency planning groups and be empowered to make key strategic decisions on behalf of local speech and language therapy services. The role of professional lead should also provide a focal point in terms of professional standards for all speech and language therapy provider services both within statutory and non-statutory provider organisations (including independent practitioners). The introduction of the concepts of plurality and contestability to the provision of statutory services highlights the need for members of the speech and language therapy profession, along with other AHP colleagues, to engage at a strategic level. It will be increasingly important for professional advice to be provided to commissioners, who will come from increasingly diverse backgrounds and experiences as services come together across traditional agency boundaries. Those managing speech and language therapy services need to: • gain membership of key strategic multi-agency planning groups • have the required high level negotiation skills (including in depth knowledge of the functioning of the different agencies) • actively influence at director level and at a strategic level across agencies Supporting children with speech, language and communication needs within integrated children’s services Recommendation 10: The role of the SLT must be seen within the context of the specialist and wider workforce. Commissioners need to be aware of the unique contribution of SLTs across the population base. In considering the place of the SLT within the children’s workforce it is essential to see the ‘whole system’. The Workforce deployment pyramid for integrated children’s services 46 (see Figure 7 below) offers a framework in which it can be seen that SLTs have an equal role to play at all levels of the ‘pyramid of need’. This model proposes that it is equally as relevant to have an SLT supporting a child with a complex disability as it is to be involved in the preventative work aimed at the general population of ‘all children’. The key factor is that the workforce dimension of the model represents the pool of specialist resource available for children at each level of need. The suggestion is that an SLT working with a child with specialist additional needs will sit as part of a large workforce around that child and therefore needs to consider the specific contribution that they can make as an SLT in this context. A child’s speech, language, communication or eating/drinking goals can be achieved using a team around the child. The model also implies that all levels of experience in terms of SLT practitioner can operate at all levels of the pyramid. Clinical experts are relevant in all areas of speech and language therapy practice as are student therapists. The rationale for ensuring that the unique contribution of the SLT is relevant for all children lies in the changing context as outlined in part 1 of this paper. In an inclusive model of service delivery, which aims to deliver services in the most accessible and effective way for children and their families, it is essential that therapists can support at all levels and across a range of settings. This model allows for the possibility of a child with a complex communication need to be supported via a children’s centre, nursery or mainstream school in that the skills and competences required can be present in all three as well as in more traditional specialist centres and settings. The ‘whole system’ approach needs to extend to include all settings in which SLTs work. An SLT working within universal services at a largely population focused level may, on the other hand, find themselves as a more significant proportion of the specialist workforce. The numbers of children impacted upon, however, will be significantly greater in this context and therefore the proportion of ‘time per child’ for the therapist working with ‘all children’ will be significantly less than for the therapist working with the relatively few children with additional needs. Figure 7 Workforce deployment pyramid for integrated children’s services Specialist Workforce Specialist services SLT others Children with additional needs Proportion of SLT time per child SLT others Vulnerable children Targeted services Service focus SLT others All children Universal services Population 21 www.rcslt.org Recommendation 11: Managers and service leads should work together with their AHP colleagues as well as colleagues from education and social care, in the development of new roles, in particular the development of consultants/specialist advisory posts and cross-agency posts. The development of consultant posts should offer potential in integrated children’s services. A consultant in disability, inclusion, or neonatology could be held by a number of professionals and SLTs are in a strong position to compete for such posts. The reports on how consultant posts are emerging indicate that they are being created where the local management are seeking to create the role. The RCSLT therefore urges managers to actively seek out those contexts where a consultant lead will enhance services. Practice example 5 Multi-agency working Example 5a COMET (Communication and Education Together) project in Northern Ireland Speech and language therapists employed as advisory SLTs to enable teachers to identify and support children with speech, language and communication difficulties in mainstream schools. Emphasis on collaborative practice, training and a consultative role for the SLTs Contact Anne McMahon – Anne.McMahon@seelb.org.uk Example 5b At I CAN Dawn House School a residential care officer has a role across the school in supporting children with augmentative and alternative communication (AAC) devices. She uses her knowledge of communication disability, together with technical expertise to support staff in their knowledge, use and maintenance of hightech communication aid – as well as being involved in running AAC groups for children. Contact Alex Hall – Ahall@ican.org.uk 22 Supporting children with speech, language and communication needs within integrated children’s services Recommendation 12: Management opportunities across agencies and across professional boundaries should be actively developed. The integration agenda relies on professionals from all backgrounds engaging in the development of services in new ways. In order to ensure that the needs of children with speech, language and communication needs are met, it is imperative that there is balanced representation at all levels of service planning and management. Care group management and teams based around children’s journeys are now common within many statutory organisations. The management arrangements within an integrated children’s service are set to become more diverse and based less and less on historic professional groupings. Practice example 6 Cross professional/Cross agency leadership Example 6a – Operational Oxfordshire Integrated Service Manager. Since October 2004, the “language” strand of Communication, Language, Autism and Sensory Support Services (CLASS) has been managed as part of an integrated service by one of Oxfordshire’s speech and language therapy coordinators. The integrated service manager (SLT) has dual accountability – to the head of CLASS and to the manager of children’s therapy services – and manages: teacher team leaders, teachers, therapists and therapy and teaching assistant staff across preschool settings, mainstream schools and additionally resourced bases linked to mainstream schools. Contact Liz Shaw – Liz.Shaw@OxfordCity-PCT.NHS.UK Example 6b – Strategic Hackney Integrated Therapy Service City & Hackney PCT and The Learning Trust (the local provider of education services in Hackney) jointly fund an integrated therapy service with SLTs being employed by either organisation but managed as one team. As part of the strategic management of therapies within the integrated agenda the children’s therapy manager is part of the SEN Senior Management Team within the Learning Trust as well as part of the health structures within the PCT. Service planning is integrated so as to meet the strategic objectives of both organisations. Contact Marie Gascoigne – Marie.Gascoigne@chpct.nhs.uk 3.4 Developing the workforce In order to respond to the challenges of the integrated children’s agenda and ensure the appropriate skills sets are available within the workforce, there is a need to consider training and continuing professional development (CPD) at all levels. Recommendation 13: The RCSLT supports the development of placements that offer student therapists a full range of opportunities as part of their practice based learning and this would include working as part of trans-disciplinary teams. This should include opportunities to work independently (with appropriate supervision) in schools and settings. This view is reflected in the RCSLT position paper on practice placements 47. The RCSLT is concerned that newly-qualified SLTs are sometimes expected to act as ‘consultants’ to other professionals despite their limited experience. Part of this concern arises from lack of specific experience as students. This is an issue for which the responsibility lies with practitioners as well as the HEIs in that students can only access the placements they are offered. Increasingly confident newly-qualified SLTs are emerging in areas where placements in mainstream schools and other settings, which offer real opportunities to manage a caseload, are available. Practice example 7 Student placements Placements in mainstream schools in Greenwich Teaching PCT Students are placed in mainstream primary schools in pairs for one day a week for one or two terms. The supervising SLT attends the school four times per term. The special educational needs coordinator (SENCO) in the school is the main point of contact for issues arising when the SLT is not on site. The SLT can be contacted by mobile phone at any time. Students are involved in assessment and therapy with pupils as well as joint planning and discussion of ideas with education staff and demonstrating activities to staff and parents. This model was initially a pilot scheme following which a list of essential criteria for a successful placement was drawn up. For further information contact Jan Baerselman, Coordinator of Mainstream Schools Service, jan.baerselman@nhs.net or Roz Weeks, Clinical Manager of Speech and Language Therapy Services to Education, roz.weeks@nhs.net. 23 www.rcslt.org Recommendation 14: Recommendation 15: Speech and language therapists working with children should undertake continuing professional development (CPD) activities across health, education and social care to develop knowledge and skills that will prepare them for cross-agency roles. The RCSLT values CPD activities that are not limited to the health context. The challenges of the changing context mean that business and entrepreneurial skills sets will become more relevant for senior managers. All speech and language service leads should also develop excellent communication and negotiation skills as part of a portfolio of leadership competence. Within education, horizontal skill mix could see the emergence of new roles for SLTs as officers within education structures as well as health professionals. Integrated specialist learning support teams drawing together specialist teachers and SLTs are not uncommon, and in some areas reciprocal membership of senior management teams across education and health are being piloted. In Scotland, the creation of community health partnerships led by social care will bring further opportunities. 24 In order to respond as leaders in the changing context, SLTs should recognise the importance of key leadership skills. Service leads should not only ensure that they demonstrate these skills, but also encourage leadership development throughout the structures for which they are responsible. Supporting children with speech, language and communication needs within integrated children’s services 4. Conclusions and way forward There are revolutionary changes underway in children’s services across the UK. Speech and language therapists, managers and commissioners are all being required to think in new ways and embrace new structures and processes. In order to continue to keep the child and their family at the centre of the arena, it will be necessary to continually re-examine the professional view in relation to the external context. Consequently, the recommendations set out in this paper will be reviewed in 2008 and evaluated in the context of the reality of services at that time. The RCSLT envisages that, as well as informing joint working within each of the home countries, the paper will also provide SLTs with a framework to support local service development and delivery. The consultation involved in the development of this paper has in itself initiated a process within the RCSLT and its membership. The structures within the RCSLT that will best support the membership in responding to the changing context for children’s services are under review as a result of this process. In addition, it is hoped service planners and managers throughout the UK will be able to use the frameworks outlined to develop services that will best meet the needs of children with speech, language and communication needs in the UK. 25 www.rcslt.org References 1 Law J, Boyle J, Harris F, Harkness A, Nye C. (1998) ‘Screening for speech and language delay – a systematic review of the literature’ Health Technology Assessment – Volume 2 Number 9 pages 1- 184 2 The 4 Nations Child Policy Network Review 2003 – 2004 www.childpolicy.org.uk/AfcStyle/DocumentDownload.cfm?DType =DocumentItem&Document=4Nannualreview0304%2Epdf 3 www.scotland.gov.uk/Topics/People/Young-People/childrenfamilies/15939/3896 www.scotland.gov.uk/library5/education/sure_start_mapping.pdf 4 www.wales.gov.uk/subichildren/content/circulars/start/start-e.htm www.wales.gov.uk/subichildren/content/entitlement/earlyentitlement-2004-e.pdf 5 www.nics.gov.uk/press/hss/041216a-hss.htm 6 www.surestart.gov.uk/_doc/0-1D9968.pdf 7 www.earlysupport.org.uk/pilot2/index.htm 8 ‘making it r wrld 2’ 05 NI Children’s Strategy www.allchildrenni.gov.uk/ 9 www.everychildmatters.gov.uk/ 10 Removing Barriers to Achievement (DfES, 2004) www.standards.dfes. gov.uk/literacy/publications/inclusion/883963/dfes011704_remo vebarrier.pdf 11 The Education (Additional Support for Learning) (Scotland) Act 2004 www.scotland-legislation.hmso.gov.uk/legislation/scotland/ acts2004/20040004.htm 12 Shaping the Future for Special Education – An Action Programme for Wales www.wales.gov.uk/subieducationtraining/content/ special/spcled_cnts_e.htm 13 Special Educational Needs and Disability Order 2005 www.deni.gov.uk 14 Health for ALL Children www.health-for-all-children.co.uk 15 Children’s Workforce Strategy (2005) www.everychildmatters. gov.uk/deliveringservices/workforcereform/ 16 Common Core of Skills and Knowledge for a Children’s Workforce www.dfes.gov.uk/commoncore/docs/5610_COMMON_CORE.pdf 17 Creating a Patient-led NHS www.dh.gov.uk/assetRoot/04/10/65/07/04106507.pdf 18 Commissioning a Patient-led NHS www.dh.gov.uk/assetRoot/04/11/67/17/04116717.pdf 19 Lewin (1951) 20 www.wales.gov.uk/subichildrenfirst/documents/circulars/ circ8-e.htm 21 For Scotland’s Children: Better Integrated Children’s Services (2001) www.scotland.gov.uk/library3/education/fcsr-00.asp 22 The Commissioner for Children and Young People (Northern Ireland) Order 2003 www.nics.gov.uk/press/ofmdfm/030626aofmdfm.htm 23 www.scotland.gov.uk/library3/education/fcsr-07.asp 26 24 Children and Young People: Rights to Action: Stronger Partnerships for Better Outcomes – Draft Guidance on Local Co-operation under the Children Act 2004 www.learning.wales.gov.uk/scripts/fe/news_ details.asp?NewsID=1909 25 Partnership Arrangements under the Health Act 1999 www.dh.gov.uk/PolicyAndGuidance/OrganisationPolicy/Integrated Care/HealthAct1999PartnershipArrangements/fs/en 26 Every Child Matters Strategic Integration Framework www.everychildmatters.gov.uk/_files/E2E9228ED8ACAB6106900 C353A69468B.doc 27 Every Child Matters website for examples www.everychildmatters.gov.uk/ 28 www.shssb.org/partnership_working/wraparound/ 29 Limbrick P. (2001) www.handseltrust.org/ 30 Williamson K. (2001) Capable, confident and competent, RCSLT Bulletin, 592, 12-13 31 www.rcslt-members.org/membersonly/comp-introduction.shtml 32 Children’s Workforce Strategy: A strategy to build a world-class workforce for children and young people (DfES 2005) DfES/1117/2005 www.dfes.gov.uk/consultations/downloadableDocs/5958-DfESECM.pdf 33 www.skillsforhealth.org.uk/ 34 Bloom L, Lahey M. (1978) Language development and disorders. New York: Wiley 35 Bronfenbrenner U. (1989). Ecological systems theory. In R. Vasta (Ed.). Annals of child development, 6 (pp. 187-251) Six theories of child development. Greenwich, Conn: JAI Press 36 World Health Organisation (2001) www3.who.int/icf/ebres/english.pdf 37 RCSLT Clinical Guidelines Edited by Sylvia Taylor-Goh (2005) 38 Communicating Quality 2 – Professional Standards for Speech and Language Therapists. (RCSLT, 1996) 39 www.everychildmatters.gov.uk/_files/F9E3F941DC8D4580539 EE4C743E9371D.pdf 40 Service model for packages of support. Hackney Speech and Language Therapy Integrated Service Handbook (2005) 41 After M Giangreco, J York & B Rainforth 1989, cited in Mackey, S and McQueen J, 1998 42 Law J, Lindsay G, Peacey N, Gascoigne MT, Soloff N, Radford J and Band S. (2000) “Provision for Children with Speech and Language Needs in England and Wales: Facilitating Communication between Education and Health Services” DfEE research report 239 43 Pay and workforce strategy for the children’s workforce: evidence chapter (unpublished DfES 2004) 44 www.handseltrust.org/ 45 Fey M. (1986) Language Intervention with Young Children San Diego, California: College Hill Press 46 Gascoigne MT. (2006) Supporting children with speech, language and communication needs within integrated children’s services, RCSLT Position Paper, RCSLT London 47 RCSLT Position Paper: Practice Placements Supporting children with speech, language and communication needs within integrated children’s services Notes 27 Supporting children with speech, language and communication needs within integrated children’s services Royal College of Speech & Language Therapists 2 White Hart Yard, London SE1 1NX Telephone: 020 7378 1200 visit: www.rcslt.org Company number: 5183445 • Registered Charity: 273724 Designed by: Wildcat Design (wildcat1@ntlworld.com) Photography by: Getty Images Printed by: Hubbards (via McMillan Scott) © RCSLT, January 2006