DOI: 10.1161/CIRCULATIONAHA.115.020338
Outcomes After Vena Cava Filter Use in Non-Cancer Patients with Acute
Venous Thromboembolism: A Population-Based Study
Running title: White et al.; Effect of vena cava filter use in patients with VTE
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
Richard H. White, MD, FACP1; Ann Brunson, MS2; Patrick S. Romano, MD, MPH1;
Zhongmin Li, PhD1; Ted Wun, MD2
1
Division
Di
ivi
visi
sion
si
on ooff Ge
G
General
nerral Internal Medicine, Department
ne
Departme
mennt of Medicine,, UC D
me
Davis
avis School of Medicine
Medicine,
Sacram
Sacramento,
men
nto
o, CA
CA;; 2Di
Division
Div
visi
siionn ooff H
Hematology
ema
mattologyy O
ma
Oncology,
ncol
nc
ollog
ogy, D
Department
eparrtm
tmeent of M
Medicine
edic
ed
i in
inee
UC
CD
avis
av
is S
ch
hoo
ool ooff M
ed
diccinee, S
acraame
ac
mentto, CA
A
Davis
School
Medicine,
Sacramento,
Address for Correspondence:
Richard H. White, MD, FACP
Division of General Medicine
UC Davis School of Medicine
Suite 2400, PSSB
4150 V Street, Sacramento, CA 95817
Tel: 916-734-7005
Fax: 916-734-2732
Email: rhwhite@ucdavis.edu
Journal Subject Terms: Embolism; Thrombosis; Epidemiology; Complications; Quality and
Outcomes
1
DOI: 10.1161/CIRCULATIONAHA.115.020338
Abstract
Background—Evidence that vena-cava filters (VCFs) are beneficial is limited.
Methods and Results—We retrospectively analyzed all non-cancer patients admitted to nonfederal California hospitals for acute venous thromboembolism (VTE) from 2005-2010.
Analysis was stratified by presence/absence of a contraindication-to-anticoagulation (active
bleeding, major surgery). Outcomes were death within 30/90 days of admission, and the one-year
incidence of recurrent-VTE manifested as pulmonary embolism (PE) or deep-vein thrombosis
(DVT). Propensity-score methods were used to account for observed systematic differences in
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
baseline characteristics between patients treated versus not treated with a VCF. Among 80,697
patients with no contraindication-to-anticoagulation, VCF-use (N=7762, 9.6%) did not
ignificantly reduce the 30-day risk of death (HR, 1.12; 95%CI, 0.98-1.28). Amongg 3,
33,017
0177
01
significantly
patients with active bleeding, VCF-use (N=1095, 36.3%), reduced the 30-day riskk of ddeath
eath
ea
th bby
y
32% (HR, 0.68; 95%CI, 0.52-0.88) and the 90-day risk by 27% (HR, 0.73; 95%CI, 0.59-0.90).
VCFF-us
Fusee (N=489,
us
(N=4
(N
= 899, 33.8%) did not reduce mortality
mortali
liity aamong
mong 1445 patients
ts w
ho underwent major
VCF-use
who
urg
gery (HR,
R 1.1
.1
1; 95
995%CI,
%CI,
%C
I, 00.71-1.77).
.711-1.
11.77
1.
77).
77
). IIn
n al
ll su
subgrou
ups ffilter-use
ilte
il
terte
r-us
ru e did
did not
not reduce
r duce
re
ce the
the riskk of
surgery
1.1;
all
subgroups
ubs
bsequent PE. H
owev
ver, th
he risk of su
ubseque
uent D
ue
VT iincreased
ncre
nc
reassed by
re
y 50%
% am
monng VCF
CF patients
paatiientss
subsequent
However,
the
subsequent
DVT
among
wi
ith nno
o co
cont
ntrain
nt
in
ndi
dica
c ti
ca
tion
on ((HR,
HR
R, 1.
11.53;
53;; 95
53
5%C
%CI,
I, 1.3
.34.3
4-1.74
474)) an
74
andd by 135
35%
35
% am
amo
ong VC
ong
VCF
F pati
ppatients
a ien
entss w
ithh
with
contraindication
95%CI,
1.34-1.74)
135%
among
with
acti
ac
tive
ti
vee bbleeding
leed
le
edin
ed
ingg (H
in
(HR
R, 22.35;
.35;
35; 995%CI,
5%CI
5%
CI, 11.56-3.52).
CI
.56
56-3
3.52)
52)
2).
active
(HR,
Conclusions—VCF-use significantly reduced the short-term risk of death only among patients
with acute VTE who had a contraindication-to-anticoagulation because of active bleeding.
These results support the findings of a randomized clinical trial and current guidelines, which
recommend VCF-use only in patients who cannot receive anticoagulation treatment.
Key words: epidemiology; thrombosis; pulmonary embolism; venous thromboembolism
2
DOI: 10.1161/CIRCULATIONAHA.115.020338
Introduction
Vena cava filters (VCFs) are frequently deployed in patients who are hospitalized for acute
venous thromboembolism (VTE). If anticoagulant treatment cannot be given, placement of a
VCF may be the only treatment option available to reduce the risk of pulmonary embolism (PE)
or dying of fatal PE. However, there is no strong evidence that use of a VCF prevents either
death or further pulmonary embolism (PE).1-3 Instead, observational studies of VTE patients
treated with a VCF in conjunction with anticoagulant therapy have reported numerous
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
thrombotic and embolic complications.4-9
In a study of VCF use in California hospitals,10 we observed wide variation in the use of
VCFs, from 0% to 40%, among patients admitted to different hospitals with a principal
priinc
ncip
ipal
ip
al diagnosis
dia
iagn
gnos
gn
o is
of VTE, even after adjusting for important clinical parameters. These findings suggest that
patients
patien
ents
en
ts with
wit
ithh similar
simi
mila
mi
l r clinical characteristics are being
la
bein
be
ing treated or not treated
in
treat
ated
at
e with a VCF based
largely
practice
arg
gely on theirr hhospital’s
ospi
pittal’
pi
l’ss prev
l’
pprevalent
rev
eval
alen
al
entt pr
en
raaccticee ppattern.
attern
n.
relatively
with
In two
wo rel
e ative
at elyy small
smaall
al randomized
r nddom
ra
o iz
izeed clinical
clinnicaal trials,
triaalss, VCF
VCF use
usse was
w s studied
wa
sttuddied
ied in patients
pat
atienntss wit
th
acute
acut
ac
ute
te DV
DVT
T 3 aand
nd aacute
cute
cu
te P
PE
E 11 who
ho also
als
lsoo re
rece
received
ceiv
ce
ived
ed sstandard
tand
ta
ndar
nd
ardd an
ar
anti
anticoagulation
tico
ti
coag
co
agul
ag
ulat
lat
atio
ionn th
io
ther
therapy.
erap
er
apy. V
ap
VCF
CF use
se
provided no significant survival benefit and did not reduce the frequency of subsequent PE in
patients who presented with PE.11 In the study of patients who presented with acute DVT
(randomized to a permanent or no VCF), the incidence of pulmonary embolism was decreased in
patients randomized to VCF use, but recurrent VTE manifested as acute DVT was increased. 3
Current 2016 American College of Chest Physicians (ACCP) guidelines recommends use
of a VCF only in patients with acute VTE who have a contraindication to anticoagulation, such
as recent or planned major surgery or active bleeding. Conducting a randomized study of VCF
use in patients with a contraindication to anticoagulation would be exceptionally difficult
3
DOI: 10.1161/CIRCULATIONAHA.115.020338
because most clinicians would feel compelled to insert a VCF if they were unable to administer
anticoagulant treatment. However, it is possible to use administrative health data to identify
patients with acute VTE patients who have a contraindication to anticoagulation, and determine
the effect of VCF use by propensity-score methodology to analyze important outcomes, such as
mortality and recurrent VTE.
The aim of this study was to use a large observational dataset to analyze the effectiveness
of VCF use in patients hospitalized for acute VTE who either had or did not have a
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
contraindication to anticoagulation therapy. The principal outcomes of interest were death
within 30 or 90 days of admission, and recurrent VTE manifested as either PE or DVT within
effect
shortone year of hospital discharge. We hypothesizedd that VCF use would have no effe
fect
fe
ct oon
n sh
shor
ortor
tterm
erm survival, but would increase the incidence of recurrent VTE manifested as DVT.
Methods
Metthods
Me
Study
Sttud
udyy Design
Desiign
This
using
data.
Wee de
determined
death
This was
as a rretrospective
etro
et
rosp
ro
spec
sp
ecti
ec
tive
ti
vee sstudy
tudy
tu
dy usi
sing
si
ng oobservational
bser
bs
erva
er
vati
ati
tion
onal
on
al da
data
ta. W
ta
dete
term
te
rmin
rm
ined
in
ed tthe
he iincidence
ncid
nc
iden
id
ence
en
ce ooff de
deat
athh
at
or recurrent VTE among adults without active cancer who were admitted to a non-federal
California hospital for acute VTE during a 6-year period from 2005 through 2010 and who either
received, or did not receive, a VCF during the index hospitalization. We stratified the study
population by the presence or absence of a contraindication to anticoagulation therapy.
Database
The study was conducted using the California Patient Discharge database (PDD) linked with the
California Emergency Department (ED), and master death file databases.12 This data is collected
and maintained by the California Office of Statewide Planning and Design (OSHPD). The PDD
4
DOI: 10.1161/CIRCULATIONAHA.115.020338
contains administrative hospital discharge data, as required (and audited) by the Center for
Medicare & Medicaid Services (CMS). The database includes demographic information, a
principal diagnosis for the hospitalization and up to 25 additional clinical diagnoses, and a list of
up to 20 major procedures performed on every patient hospitalized in all non-federal acute-care
hospitals in California (the PDD includes 95-97% of all discharges in the state). The ED records
include similar data for cases evaluated, but not admitted, at all hospital-affiliated ED’s. Serial
hospital/ED records can be linked using an encrypted form of the social-security number called
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
the record-linkage-number (RLN) that is generated by OSHPD for the 95% of patients who have
a social security number. The PDD and ED data sets do not list the medications prescribed to the
not
reliable
patient. Codes for the administration of parenteral anticoagulation exist but are no
ot re
reli
liab
li
able
ab
le aass
there
here is no information about intensity of anticoagulation therapy, duration off therapy or overall
adequacy
events
adeq
qua
uacy
cy ooff an
aanticoagulation
tiico
coagulation therapy. VTE event
ntts di
ddiagnosed
agnosed and treatedd in
in the out-patient arena
are not
ar
not include
includ
de in either
eitthe
herr the
the PDD
PDD orr ED
ED data
ta bases.
bases.
Medical
Medi
diccal diagnoses
di
diag
di
a noses and
an
nd major
m jo
ma
jorr procedures
prooced
durres (with
(w h date
datee performed)
per
errfo
orm
med
e ) are
arre coded
code
d d using
usiing
us
International-Classification-of-Disease,
V-9,
Clinically-Modified
Since
nte
tern
rnat
rn
atio
at
iona
io
nall-Cl
na
Clas
Cl
assi
as
sifi
si
fica
fi
cati
ca
tion
ti
on-of
of-Dis
Dis
isea
ease
ea
se, V
se
-99, C
lini
li
nica
call
lly-Mo
ll
Modi
Mo
difi
di
fied
fi
ed ((ICD-9-CM).
ICD
IC
D-99-CM
CM)). S
CM
ince
in
ce 11996
9966 al
99
alll
medical diagnoses in the PDD require a present-on-admission (POA) indicator, which indicates
if the condition was present-on-admission (POA=Y/W) or developed during the hospitalization
(POA=N/U).13 Cause of death on death certificates is coded using ICD-10. This study was
approved by the California Health and Human Services Agency’s Committee for the Protection
of Human Subjects, and the University of California, Davis Human Research Protections
Program.
Study Population
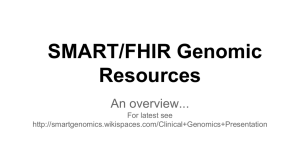
Figure 1 shows a schematic flow diagram of the criteria applied to assemble the study
5
DOI: 10.1161/CIRCULATIONAHA.115.020338
populations. We identified all cases age 18 years or older who had a RLN. Cases were excluded
if they had a VCF previously placed, back to July 1, 1991, or if there was a diagnosis of active
cancer (140.0-209.9, except for non-melanoma skin cancer, 173.0-173.9) either at the time of the
index hospitalization or during any hospitalization within the prior 6 months.
Acute VTE
Cases admitted for acute VTE were identified by the presence of a specific principal diagnosis
code (see Supplemental Table 1) for either PE or lower-extremity DVT. For each linked record,
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
only the first hospitalization for acute VTE was analyzed. Cases coded as having both DVT and
PE were classified as having a PE. ICD-9-CM codes for a principal diagnosis of acute lower
predictive
extremity DVT or acute PE have been validated and shown to have a positive pred
edic
ed
icti
ic
tive
ti
ve vvalue
alue
al
ue of
approximately 95%.14 The POA indicator has also been validated. 15
Vena
na
a Cava
Cav
avaa Filter
F lter
Fi
er U
se
Use
VCF
VC
F placemen
placement
nt wa
w
wass id
iden
identified
enti
en
tiffied
ti
fied bby
y th
the pr
ppresence
reesen
ncee off th
the
he IC
ICDICD-9-CM
D-9D9-CM
9CM ccode
ode
od
de 38
338.7
8.7 ((interruption
inte
in
terr
te
rrup
rr
uptiion ooff th
up
thee
vena
ve
ena cava). VC
V
VCF
F rremoval
emo
oval is IICD-9-CM=39.99
CD-9
CD
9-C
-CM
M=39.
9..99
9 or C
CPT=037203,
PT=
T=00377203
T=
7203
3, bu
but
ut these
t esee codes
th
co
ode
des were
werre
we
encountered
enco
en
coun
co
unte
nte
tere
redd so iinfrequently
re
nfre
nf
requ
re
quen
entl
en
tly (3
tl
(314
14 ooff 93
9346
46 ccases,
ases
as
es, 33.4%)
es
.44%) tthat
hatt re
ha
retr
retrieval
trie
tr
ieva
ie
val
al was
waas no
nott iincorporated
ncor
nc
orpo
or
pora
po
rate
ra
tedd in
te
into
to
any analysis.16
Active bleeding
To isolate the cases who were likely to have not received anticoagulation during all or part of the
hospital stay, we identified all cases with active bleeding, which was ascertained using specific
ICD-9-CM codes (Supplemental Table 2) that have been validated in other studies. 17,18 and the
bleeding was classified as intracranial, gastrointestinal, and other. Hematuria and epistaxis were
included as ‘other-bleed’ only if there was coding for one or more blood transfusions (99.00,
99.03, 99.04-99.07). Bleeding events were categorized as being “present-on-admission”
6
DOI: 10.1161/CIRCULATIONAHA.115.020338
(POA=Y/W) or “not present on admission” (POA=N/U) based on the POA indicator code, which
accompanies each ICD-9-CM diagnosis codes.
Surgery
To isolate another subgroup of cases who were likely to have had anticoagulation withheld
during all or part of the hospital stay, we identified cases that underwent a major surgical
operation during the hospital stay. Major diagnostic or therapeutic operating room procedures
were defined using a modification of the CMS reference codes,19 specifically excluding VCF
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
insertion (38.7) as a surgical procedure. Vascular procedures for venous thrombectomy or
procedures used in conjunction with thrombolysis were not included in the definition of major
urgery. (Supplemental Table 3)
surgery.
Outcomes
Prin
nci
cipa
pall ou
pa
outc
tcom
tc
mess were death 30 days and 90
90 days,
d ys, recurrent VTE
da
E manifested
manifested as PE (+/Principal
outcomes
DVT
DV
T) or DVT al
alon
ne
1 year
yeaar
ye
ar ooff ho
hosp
spit
sp
ital
it
a dis
isch
char
ch
a gee. A rrecurrent
ecur
ec
urrre
rent
n V
nt
TE eevent
vent aafter
fter
ft
er tthe
he iindex
nddex
DVT)
alone
1
hospital
discharge.
VTE
ad
dmi
miss
s ion was
wa defined
d finedd by
de
by a hospital
hos
ospi
p taal readmission
reeaddmis
issiion orr ann ED
ED visit
visiit with
visi
with
h a pr
princ
cipa
cipa
pall di
iagnosiss of
iag
admission
principal
diagnosis
acut
ac
ute
te DV
DVT
T or P
E, oorr by
by a ddiagnosis
iagn
ia
gnos
gn
osis
os
is ooff ac
acut
ute
te VT
VTE
E du
dduring
uri
ring
ri
ng a ssubsequent
ub
ubse
bse
sequ
quen
entt ho
en
hosp
spit
sp
ital
it
aliz
al
izat
atio
at
ionn (P
io
(POA
OA=N)
N)
acute
PE,
acute
hospitalization
(POA=N)
that was within the specified follow-up time period.
Covariates
Covariates included demographic variables, comorbidities, prior surgery, severity-of- illness, PE
versus DVT, use of thrombolysis day 1-2, and bleeding present on admission. Pre-existing comorbid conditions (n=23) were defined using the Elixhauser co-morbidity software.20,21
Proprietary software from 3MTM (APR-DRG grouper, V-24) was applied to every record to
generate a severity-of-illness (SOI) level and a risk-of-mortality (ROM) level at the time of
admission.22,23 Software categorized each of these parameters as mild, moderate, major or
7
DOI: 10.1161/CIRCULATIONAHA.115.020338
extreme. Hospital characteristics were specified based on size (< 100, 101-200, >200 beds), type
(private, Kaiser-affiliated, academic), location (rural versus urban) and kind (profit, not-forprofit).
Analytic and Statistical Methodology
All cases were classified into one of three mutually exclusive groups: Group_1 had neither of the
two identifiable contraindications to anticoagulant treatment; Group_2 had a transient
contraindication to anticoagulant therapy because they underwent a major operating room
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
procedure, with or without active bleeding, during the index hospitalization or within 3 days
prior to admission; Group_3 had had a transient or permanent contraindication to anticoagulant
therapy
during
herapy because they had active bleeding, either present on admission or arising du
duri
ring
ri
ng tthe
he
hospitalization. In the absence of any reliable data (coding) to define ongoing therapeutic
anticoagulation,
likely
antico
coag
co
agul
ag
ulat
ul
atio
at
ion, this
io
thi
h s grouping allowed us to distinguish
disti
ting
ti
ngui
ng
u sh patients who li
ike
kely received therapeutic
anticoagulation
treatment
VTE
patients
who
probably
delayed,
antiicoagulationn ffor
an
orr tr
reatm
tmen
entt of tthe
en
he aacute
cutte V
cu
TE from
om
m pat
atie
at
ient
ie
ntss wh
nt
ho pr
prob
obab
ob
ably rreceived
ecei
eive
ive
vedd de
del
laye
yed,
ye
d,
interrupted,
anticoagulation
nte
t rr
rrup
u ted,
d,, iinadequate
nade
d quatte or noo an
antico
oaguulaatio
on ttreatment.
reatm
tm
men
nt .
Propensity
Pr
Propen
sit
si
ity SScore
core
A logistic regression model was used to estimate each patient’s propensity of having a VCF
inserted, based on factors likely associated with VCF use, 10 including hospital variables (type,
location, size), demographic variables (age, sex, race/ethnicity) and clinical variables (e.g., PE,
proximal DVT, distal DVT alone, comorbid conditions, severity-of-illness). Hospital-specific
fixed effects were used to proxy for unobserved patient characteristics that may differ across
hospitals. Outcomes were compared using models that used either inverse probability of
treatment weighting, or matching based on the propensity score using the calipers method, with
caliper = 0.001.24 The effect of propensity score adjustment on the standardized mean differences
8
DOI: 10.1161/CIRCULATIONAHA.115.020338
in baseline covariates between the cases who received or did not receive a VCF was determined
for each subgroup.25
Immortal-time-bias
Because the day of VCF insertion can vary from early to late during the index hospitalization,
analysis of the effect of VCF use is subject to immortal time bias.26-28 Cases who did not receive
a VCF might have died before a VCF could be inserted, whereas all of the VCF-treated cases
were alive when the VCF was inserted (hence they were ‘immortal’ during the interval from the
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
date of admission to the date of insertion). To account for this bias, VCF use was entered as a
time-dependent covariate in the inverse probability weighted proportional hazard models for
death.25 In propensity-matched analyses, cases not treated with a VCF had to be alive
ali
live
ve on
on the
the
hospital day when the matched VCF case had the filter inserted.28
Outc
Ou
tcom
tc
o es were
were modeled using proportional
proportion
onal
on
al hazard methodology
gy after
f testing for the
Outcomes
pproportionality
rop
portionalityy assumption.
assump
mpti
mp
tion
ti
on.. For
on
For cases
case
ca
ses in Group_1
se
G ou
Gr
oup_
p 1 and
and Group_3,
Grou
Gr
ouup_
p_3,
3 death
dea
eath
ea
th was
was aanalyzed
nallyze
na
lyze
zedd att 30
30
days,
da
ays
ys,, and 990
0 day
da
days
ays fr
from
rom
m thee da
dayy of adm
admission,
dmissi
dm
siionn, w
whereas
heerea
eaas for
fo
or Group_2,
Grou
Gr
up_
p_2,
2 death
death
hw
was
a ana
as
analyzed
nallyzedd from
na
om
the
he da
day of ssurgery.
urrge
urge
gery
ry. The
The demographic
demo
de
mogr
mo
grap
gr
aphi
ap
hicc and
hi
and clinical
clin
cl
inic
in
ical
ic
al risk
risk ffactors
acto
ac
tors
to
rs use
used
sedd fo
se
forr ad
adju
adjustment
just
stme
st
ment
me
nt iin
n th
thee mo
mode
models
dels
de
ls
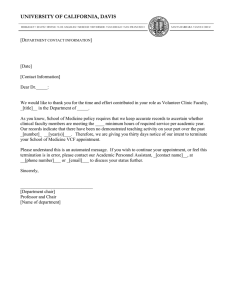
for death (and recurrent VTE) in each group are shown on Forest plots (Figures 2-4), and
included bleeding subtypes, PE (versus DVT) and risk-of-mortality.
Categorical data were analyzed using Chi-square testing. Analyses were performed using
SAS® V 9.3 and a two-sided p-value less than 0.05 was considered statistically significant. All
models were tested for proportionality using log-negative log plots.
Results
The clinical characteristics of the cases in each subgroup are shown in Table 1. Across all three
9
DOI: 10.1161/CIRCULATIONAHA.115.020338
subgroups, cases treated with a VCF were older, had more chronic comorbidity, had a higher
frequency of proximal DVT, and had greater severity-of-illness and risk-of-mortality at the time
of admission.
Figures 5-7 show the standardized mean differences of these parameters in each group
before and after adjusting for propensity score using inverse probability weighting. As shown in
these figures, the inverse probability of treatment weighting made the characteristics of the VCF
and No-VCF groups more balanced compared to the observed differences.
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
A VCF was placed in 7762 of the 80697 (9.6%) cases who had no contraindication to
anticoagulation, in 489 of the 1445 (33.8%) cases who underwent a major operating room
procedure, and in 1095 of the 3017 (36.2%) cases who had active bleeding. Overall,
Overral
all,
l, 19.4%
19.
9.4%
4% of
of
the
he VCFs were inserted on hospital day 1, 29.2% on day 2, 17.8% on day 3 and 11.1% on day 4,
with
h 22.5%
22.
2.5%
5% inserted
ins
n errte
ted after this day.
effect
outcomes
summarized
Table
The ef
ffe
fecct off VC
VCF
F use
use on
on tthe
he pprincipal
rinncip
ipall out
ip
tco
omees is
is sum
umma
um
mari
rize
ize
zedd in Ta
abl
blee 22.. As shown
sho
hown
wn in
in
Figure
use
VCF
significantly
improve
survival
Group_1
Fiigu
gure
r 2, us
se off a VC
CF did nnot
ot sig
igni
ig
nifica
ni
cant
ca
n ly im
mprov
ve su
surv
r iv
val aamong
mong
mo
ng the
he Gr
roup_1
rou
up ccases,
ases, whoo
had
unadjusted
mortality
had no ccontraindication
ontr
on
trai
tr
aind
ai
ndic
nd
icat
ic
atio
at
ionn to aanticoagulation.
io
ntic
nt
icoa
ic
oagu
oa
gula
lati
la
tion
ti
on. Th
on
Thee unad
un
nad
adju
just
sted
st
ed 330-day
0-da
day mo
da
mort
rtal
rt
alit
al
ity ra
it
rate
te was
as 44.5%
.5%
5% in tthe
hee
VCF cases and 3.3% in the no-VCF cases. Using inverse probability weighting and adjusting for
immortal time bias, the risk of death within 30 days was not significantly higher among VCFtreated cases (HR, 1.12; 95% CI, 0.98-1.28). There was no interaction between VCF use and a
diagnosis of PE versus DVT (P>0.5). Similar findings were noted using matching methodology.
The unadjusted incidence of PE 1 year was 2.8% among VCF cases and 3.2% among no VCF
cases. There was no difference in the risk of recurrent PE within 1 year after discharge in the
adjusted model (HR, 1.05; 95% CI, 0.89-1.24). The incidence of DVT 1 year was 5.4% among
VCF cases and 3.7% among no-VCF groups. The adjusted risk of recurrent DVT within one
10
DOI: 10.1161/CIRCULATIONAHA.115.020338
year was significantly higher among VCF treated cases than among no-VCF cases (HR, 1.53;
95% CI, 1.34-1.74).
Among the Group_2 cases who underwent surgery, VCF use did not affect: the 30-day
risk of death (HR, 1.12; 95% CI, 0.71-1.77), the one-year risk of recurrent PE (HR, 0.85; 95%
CI, 0.35-2.10), or the one-year risk of recurrent DVT (HR, 1.15; 95% CI, 0.57-2.32).
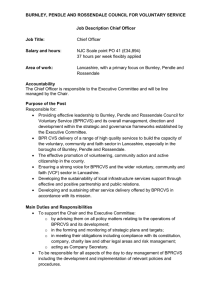
Among Group_3 cases, all of whom had active bleeding, VCF use was associated with a
crude 30 day mortality of 9.5% among VCF cases 11.5% among no-VCF cases. There was a
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
statistically significant 32% reduction in the adjusted risk of death within 30 days, after inverse
probability weighting of the propensity and adjusting for immortal time bias (HR, 0.68; 95% CI,
0.52-0.88). The Forest plot is shown in Figure 3. Similarly, using propensity-matching
propensity-mattch
chin
ingg an
in
andd
adjusting for immortal time bias, the risk of death associated with VCF use was reduced by 39%
(HR,
CI,
hazard
HR,
R, 00.61;
.61;
.6
1; 995%
5 C
5%
I 0.39-0.95). Proportional haza
I,
zard
za
rd models for death 9900 days after admission
showed
VCF
remained
with
similar
how
owed that VC
CF uuse
se re
ema
main
ined
in
ed aassociated
ssocia
iateed wi
ia
w
th a si
imila
larr significant
la
sign
si
gniffic
gn
ican
nt reduction
reedu
duction
on in
in the
the risk
riisk of
of death
deaath
de
(HR,
who
HR, 0.73; 95%
95%
5 CI,
CI, 0.59-0.90).
0..599-0.90
90).
90
). The
he distribution
diist
strribu
utioon of
of the
thee day
day off death
deaath
h among
amo
ong tthe
he cases
es wh
ho
received
receive
Figure
ece
ceiv
ived
ed oorr di
didd no
nott re
rece
ceiv
ce
ivee a VC
VCF
F is shown
sho
hown
wnn in
in Fi
Figu
gure
re 88,, which
whhic
whic
ichh demonstrates
demo
de
mons
mo
nstr
ns
trat
tr
ates
at
es that
tha
hatt the
the majority
majo
ma
jori
jo
rity
ri
ty of
of
deaths in the first 8 days occurred in cases who did not receive a VCF, making adjustment for
immortal time bias mandatory.
In the Group_3 cases, who had active bleeding, the crude incidence of PE 1 year was
2.6% for VCF cases and 2.6% among the no-VCF cases, and there was no significant reduction
in the adjusted risk of recurrent PE within 1 year (HR, 1.04; 95% CI, 0.67-1.61). Performing a
sensitivity analysis to include recurrent PE events coded as occurring during the index
hospitalization (POA=N/U), there was no change in the results. In this group, the crude incidence
of recurrent DVT 1 year in the VCF cases was 6.1% versus 2.5% in the no-VCF cases, and in
11
DOI: 10.1161/CIRCULATIONAHA.115.020338
the adjusted risk model, recurrent DVT within 1 year was significantly higher among VCF cases
(HR, 2.35; 95% CI, 1.56-3.52).
Among the 1095 cases with active bleeding who received a VCF, 104 (9.5%) died within
30 days compared with 221 (11.5%) deaths among the 1922 cases who did not receive a VCF.
Twenty-four of the 104 (23.1%) VCF treated cases who died had VTE listed as the cause of
death, and 8 (33%) of these VTE deaths had a death-certificate diagnosis of PE (ICD-10= I26.9).
In comparison, 57 (25.8%) of the deaths among the cases not treated with a VCF had VTE listed
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
as the cause of death, and 38 (66%) of these VTE deaths had a death-certificate diagnosis of PE.
Discussion
The principal findings of this study were that VCF use did not prevent either death or recurrent
venous
who
veno
ous thromboembolism
thr
hrom
omboem
om
embolism manifest as PE in patients
em
pattie
ient
nts with acute VTE w
nt
ho had no
contraindication
anticoagulation,
VCF
reduce
day
death
contraindicati
con
nt
ion
n too an
ant
tico
coag
co
agul
ag
ulat
ul
atio
at
ion,
io
n, bbut
ut V
CF uuse
se ddid
idd red
educ
ed
ucee th
uc
tthee 30 aand
nd 90 da
ay ri
risk
isk ooff de
deat
athh by
at
approximately
therapy
ap
ppr
prox
o imatel
elyy 30%
el
300% inn patients
patienntss with
w th
wi
h active
acctiv
ve bleeding
bleeeding
ng who
who likely
lik
kelly had
hadd anticoagulation
a tiico
an
oag
gul
ulat
a ionn th
ther
rap
py
withheld
admission
index
hospitalization.
finding
wiith
with
thhe
held
he
ld eeither
ithe
it
herr at tthe
he
he ttime
imee of ad
im
admi
miss
mi
ssio
ss
ionn or dduring
io
urrin
urin
ingg th
thee in
inde
dex ho
de
hos
spi
pita
tali
ta
liza
li
zati
ati
tion
on. Th
on
Thee fi
find
ndin
nd
ingg th
in
that
at tthe
he
lower risk of death persisted out to 90 days after admission suggests that VCF use did not simply
delay the time of death. These findings are consistent with the recently published findings from
the Prevention of Recurrent Pulmonary Embolism by Vena Cava Interruption 2 (PREPIC 2)
clinical trial study,11 which reported that VCF use had no effect on morality or recurrent PE
among patients who presented with PE who had no contraindication to anticoagulant therapy.
Our findings support the recent 2016 American Society of Chest Physician guidelines,29 which
recommends that a VCF be used for early treatment only in patients with an acute proximal
lower extremity DVT or PE who cannot receive anticoagulant therapy.
12
DOI: 10.1161/CIRCULATIONAHA.115.020338
The rather striking reduction in short-term mortality associated with VCF use among the
acute VTE patients who had active bleeding was not expected. In an analysis of a small number
of patients in a European VTE registry who were at increased risk for bleeding during
anticoagulation,30 VCF use was not associated with a significant reduction in death within 30
days. This study did report that VCF use was associated with a significant reduction in death
attributed to PE, but no adjustment was made for immortal time bias.31 Similarly, several
retrospective studies have reported a beneficial effect of VCF on mortality in highly specified
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
subgroups of patients with acute VTE who were at high risk for dying, but again, none of these
studies used rigorous methodology to account for immortal time bias.30,32-34
A possible explanation for the observed reduction of mortality associated wi
with
th V
VCF
CF uuse
se
in
n acute VTE patients who had active bleeding is treatment bias, i.e., ordering insertion of a VCF
preferentially
pref
fer
eren
enti
en
tial
ti
ally
al
ly in le
less
s ill patients. However, the ov
overall
ver
eral
a l level of severityseverity-of-illness
-of
of-illness and risk-ofmortality
treated
m
orrtality (ROM)
(ROM
M) at
at the
the time
tim
imee of admission
adm
dmis
issi
is
s on was
wass significantly
sig
gniifica
caant
ntly
ly higher
h gh
hi
gher
err among
amo
mong ppatients
atie
at
ient
ie
ntss tr
nt
trea
ated
ted wi
with
th a
VCF
patients
who
VCF.
admission,
VC
F compared
comp
par
ared
e tto
o the pa
atien
nts
t w
hoo ddid
id
d nnot
ot rreceive
ecceivee a V
CF At tthe
CF.
hee ttime
im
me of
of adm
dmis
dm
i sion
onn, 46.8% of
the
bleeding
VCF
placed
he patients
pati
pa
tien
ti
ents
en
ts with
wit
ithh major
it
majo
ma
jorr bl
jo
blee
eedi
ee
ding
di
ng who
ho hhad
ad a V
CF pl
plac
aced
ac
ed were
wer
eree classified
er
clas
cl
assi
as
sifi
si
fied
fi
ed as
as having
havi
ha
ving
ing major
maj
ajor
or or
or
extreme ROM , versus only 31.3% of the patients with major bleeding who did not receive a
VCF. In fact, severity-of-illness and risk-of-mortality were significantly higher among the
patients who had a VCF inserted in each of the three groups that were analyzed. Moreover, in the
models for death, we adjusted for important risk factors for death including age, race, insurance
status, and the number of comorbidities in addition to the risk-of-mortality.
Although the acute VTE patients who required major surgery likely had anticoagulation
discontinued. at least transiently, during the perioperative period, use of a VCF had no effect on
the risk of death within 30 or 90 days. We had no direct measure of the duration or intensity of
13
DOI: 10.1161/CIRCULATIONAHA.115.020338
anticoagulant therapy, but we suspect that patients who underwent an unrelated major procedures
during their hospitalization for VTE were probably highly selected, and these patients likely had
therapeutic anticoagulation withheld for a relatively brief period. By contrast, patients with
active bleeding were not selected (i.e., most of these events were probably unexpected
complications of initial VTE therapy) and probably had a longer mean duration without
receiving anticoagulation.
The finding that VCF use reduced the short-term risk of death among patients with active
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
bleeding but had no long-term effect on the risk of recurrent PE may seem contradictory. If a
VCF provides a physical barrier that prevents or retards the migration of embolus into the lungs,
then
PEs,
hen VCF use should theoretically prevent both early deaths and symptomatic PEs
Es, at lleast
Es
east
ea
st uuntil
ntil
nt
the
he time of VCF retrieval. Several factors may explain this paradox. First, many patients with
probably
therapy
active
ve bbleeding
leed
le
edin
ed
ing pr
in
prob
o ably had anticoagulation ther
erap
er
apy restarted as soon as the risk of further
ap
bleeding
bl eding was deemed
blee
dee
eem
med too be
be sufficiently
suuff
ffiicie
icie
ient
n ly low.
nt
low
w. Second,
Secondd, a modest
m de
mo
dest
s proportion
pro
ropo
port
po
rtio
rt
ionn off the
io
the VCFs
VCF
CFss might
migh
mi
ghtt
gh
have
removed
within
weeks
insertion.
ha
ave bbeen
een re
emo
m ved wi
ith
hin a few
ew w
e ks ooff in
ee
nseertio
on.16 T
Third,
hird
rd
d, VCF
VC us
use
se might
mighht hhave
mi
ave iimproved
mpro
oved
urv
rviv
ival
al not
not by
by “catching”
“cat
“c
atch
at
chin
ch
ing”
in
g” large
lar
arge
ge clots
clo
lots
ts that
tha
hatt embolized
embo
em
boli
bo
lize
li
zed
ed toward
towa
to
ward
ard the
the lung,
lung
unng, but
butt by
by breaking
brea
br
eaki
ea
king
ki
ng upp these
thes
th
esee
es
survival
embolizing thrombi into smaller pieces that were better tolerated hemodynamically. Although
causes of death on death certificates are often not accurate,35 we did find that in the patients with
active bleeding who died in the hospital, the proportion deaths of attributed to PE was higher in
those who did not receive a VCF compared to those who had a VCF inserted. However, this
finding could be due to attribution bias, as physicians may be less likely to blame a death on PE
knowing that a VCF had been inserted.
It is unlikely that a clinical trial will ever be conducted to assess the efficacy of VCF use
among patients with a clear contraindication to anticoagulation therapy because of active
14
DOI: 10.1161/CIRCULATIONAHA.115.020338
bleeding. Such patients are relatively uncommon, they are quite ill, and the need to obtain
prompt informed consent would make conducting such a study extremely challenging. The
current retrospective analysis represents an attempt to determine whether VCF use may be
beneficial among patients who have at least a temporary contraindication to anticoagulation.
To minimize sources of bias inherent in retrospective observational studies, we used
propensity score analytic methods to balance the distribution of all observed baseline
characteristics 24, and we adjusted for immortal-time-bias.26-28 Immortal-time-bias arises in
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
observational studies when patients who appear to be eligible for an intervention, such as VCF
insertion, die before they can receive the intervention yet they are included in the analysis and
categorized as not receiving the intervention. Accepted methods off circumventingg this
thi
hiss bias
bias to
to
ensure a fair comparison of VCF use and non-use were incorporatedd into our analysis.26,28 In our
anallys
ysis
is ooff th
the pa
ati
tients who had a contraindicati
ion to
to anticoagulation because
beccause of active bleeding,
be
analysis
patients
contraindication
the
he reduction
reduction inn the
the risk
ris
iskk of
of dying
dyin
dy
ingg associated
in
asso
as
s ci
c ated
ed
dw
with
ith VC
VCF
CF us
use fe
fell
l ffrom
ll
r m 53
ro
53%
% to 332%
2% aafter
fter
ft
er aaccounting
cccou
ount
ntin
nt
i g
for
foor im
immortal
immortal-time-bias.
al-t
al
- im
-t
me--biaas.
Limitations
Limi
Li
mita
mi
tati
ta
tion
ti
onss of tthis
on
hiss an
hi
anal
analysis
alys
al
ysis
sis include
inc
nclu
lude
de tthe
he absence
abse
ab
senc
se
ncee of any
nc
any
ny information
inf
nfor
orma
or
mati
ma
tion
ti
on about
abo
bout
utt the
the use,
use
se,
se
intensity, or duration of anticoagulation therapy. Except for patients with active bleeding and
those who underwent major surgery, we assumed that anticoagulation therapy was administered
to all patients. Active bleeding is likely an excellent surrogate for avoidance of anticoagulation.
To the extent that patients classified as having major bleeding actually had only minor bleeding,
and were either maintained on anticoagulation or taken off for only a short period of time, our
findings may have underestimated the true effect of VCF-use on mortality among VTE patients
who did not receive anticoagulation therapy. Because fewer than 5% of the VCF treated patients
had a procedure code for VCF removal, we did not adjust for removal. The findings of this study
15
DOI: 10.1161/CIRCULATIONAHA.115.020338
do not apply to patients with cancer, who were excluded because of the difficulty of adjusting for
their short-term risk of death. Finally, our data base did not allow us to identify any patients who
had recurrent DVT diagnosed and treated only in the outpatient arena. However, because the
proportion of patients diagnosed with recurrent DVT in the outpatient setting was likely similar
among patients treated and not treated with a VCF, the results of our proportional hazard
modeling are likely unaffected.
In summary, the findings of this retrospective analysis of observational data suggest that
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
VCF use reduced the short-term risk of death among VTE patients without cancer who had a
temporary contraindication to anticoagulation due to active bleeding. This lower risk of death
was not observed among patients who had no contraindication to anticoagulationn ttreatment,
reat
re
atme
at
ment
me
nt,, an
nt
and
itt was not observed in patients who had a temporary contraindication to anticoagulation because
they
hey
y underwent
und
nder
erwe
er
went major
we
maj
a or surgery. Among patients with
with or without a contraindication
contra
raain
indication to
anticoagulation,
associated
with
higher
risk
diagnosed
antiicoagulation,
an
n iinsertion
nser
erttion
er
on ooff a VC
VCF
F wa
was asso
soociated
ci d w
itth a hi
high
g er ri
iskk ooff bbeing
ein
ng di
diag
agnnose
ag
nose
sedd wi
with
th
acute
within
filter
was
ac
cut
utee DVT wi
withi
in onee yyear,
ear, bbut
ut filt
ltter
e uuse
see w
as not associated
asssoociiate
ia ed with
with
th
h a reduction
red
e uc
uction
on in
in the
th
he risk
riskk of
of
recurrent
ecu
curr
rren
rr
entt PE within
en
wit
ithi
it
hinn one
hi
one year.
yeear
year
ar.
Funding Sources: This study was supported by the Hibbard E Williams Endowment at UC
Davis.
Conflict of Interest Disclosures: None.
References:
1. Girard P, Meyer G, Parent F, Mismetti P. Medical literature, vena cava filters and evidence of
efficacy. A descriptive review. Thromb Haemost. 2014;111:761-769.
2. Prasad V, Rho J, Cifu A. The inferior vena cava filter: How could a medical device be so well
accepted without any evidence of efficacy? JAMA Intern Med. 2013;173:493-495.
16
DOI: 10.1161/CIRCULATIONAHA.115.020338
3. Group TPS. Eight-Year Follow-Up of Patients With Permanent Vena Cava Filters in the
Prevention of Pulmonary Embolism. Circulation. 2005;112:416-422.
4. Nicholson W, Nicholson WJ, Tolerico P, Taylor B, Solomon S, Schryver T, McCullum K,
Goldberg H, Mills J, Schuler B, Shears L, Siddoway L, Agarwal N, Tuohy C. Prevalence of
fracture and fragment embolization of Bard retrievable vena cava filters and clinical implications
including cardiac perforation and tamponade. Arch Intern Med. 2010;170:1827-1831.
5. White RH, Zhou H, Kim J, Romano PS. A population-based study of the effectiveness of
inferior vena cava filter use among patients with venous thromboembolism. Arch Intern Med.
2000;160:2033-2041.
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
6. Wittenberg G, Kueppers V, Tschammler A, Scheppach W, Kenn W, Hahn D. Long-term
results of vena cava filters: experiences with the LGM and the Titanium Greenfield devices. J
Vasc Interv Radiol. 1998;21:225-229.
7. Rajasekhar A, Streiff MB. Vena cava filters for management of venous thromboembolism: a
2013;27:225-241.
clinical review. Blood Rev. 2013;27:225
241.
LaMuraglia
GM.
8. Malek JY, Kwolek CJ, Conrad MF, Patel VI, Watkins MT, Lancaster RT, LaMu
Mura
Mu
ragl
ra
glia
gl
ia G
M.
Presentation and treatment outcomes of patients with symptomatic inferior vena cava filters. Ann
Vasc Surg. 2013;27:84-88.
(IVC)
Communication:
9.. U.S.
U.S.
S Food
od
d and Drug Administration. Inferior Vena
Venna Cava (IVC
C) Filters: Initial Communication
Risk
Adverse
Events
with
Term
Bethesda,
MD;
R
iskk of Advers
se E
ven
ents
en
ts w
ithh Lo
it
Long
ng T
errm Us
Use. Bet
theesdda, M
D; 22010.
D;
0 0.
01
hhttp://www.fda.gov/safety/medwatch/safetyinformation/safetyalertsforhumanmedicalproducts/uc
ht
tp
p://www.fda.ggov/saafeety/me
medwatch/ssaffetyiinforma
me
nf maationn/s
/saf
afet
af
etyaleerttsforhu
et
humaanmedic
nm iccalprod
al ductss/u
uc
m221707.htm
Accessed
Mar
2016.
m221
m2
21707.httm A
21
cccesssedd Ma
ar 28,
28 20
2016
6.
10. White
10
Whit
Wh
itee RH,
it
RH Geraghty
Gera
Ge
ragh
ra
ghty
gh
ty E,
E, Brunson
Brun
Br
unso
nso
sonn A,
A, Murin
Murin
urrin S,
S, Wun
Wunn T,
Wu
T, Spencer
Spe
penc
ncer
nc
er F,
F, Romano
Roma
Ro
mano
ma
no PS.
PS. HIgh
HIg
Ighh variation
vaari
vari
riat
atio
at
ionn
io
between hospitals in vena cava filter use for venous thromboembolism. JAMA Intern Med.
2013:1-7.
11. Mismetti P, Laporte S, Pellerin O, Ennezat PV, Couturaud F, Elias A, Falvo N, Meneveau N,
Quere I, Roy PM, Sanchez O, Schmidt J, Seinturier C, Sevestre MA, Beregi JP, Tardy B,
Lacroix P, Presles E, Leizorovicz A, Decousus H, Barral FG, Meyer G. Effect of a retrievable
inferior vena cava filter plus anticoagulation vs anticoagulation alone on risk of recurrent
pulmonary embolism: a randomized clinical trial. JAMA. 2015;313:1627-1635.
12. Office of Statewide Health Planning and Development. Data Request Center. Available at:
(http://www.oshpd.ca.gov/HID/Data_Request_Center/Types_of_Data.html) Accessed Mar 28,
2016.
13. Kassed C, Kowlessar N, Pfunter A, Parlato J, Andrews RM The Case for the POA Indicator:
Update 2011. ONLINE November 1, 2011. U.S. Agency for Healthcare Research and Quality.
Available: http://www.hcupus.ahrq.gov/reports/methods/methods.jsp.
17
DOI: 10.1161/CIRCULATIONAHA.115.020338
14. White RH, Garcia M, Sadeghi B, Tancredi DJ, Zrelak P, Cuny J, Sama P, Gammon H,
Schmaltz S, Romano PS. Evaluation of the predictive value of ICD-9-CM coded administrative
data for venous thromboembolism in the United States. Thromb Res. 2010,126:61-67.
15. Khanna RR, Kim SB, Jenkins I, El-Kareh R, Afsarmanesh N, Amin A, Sand H, Auerbach A,
Chia CY, Maynard G, Romano PS, White RH. Predictive value of the present-on-admission
indicator for hospital-acquired venous thromboembolism. Med Care. 2015;53:e31-36.
16. Peterson EA, Yenson PR, Liu D, Lee AYY. Predictors of attempted inferior vena cava filters
retrieval in a tertiary care centre. Thrombs Res. 2014;134:300-304.
17. Fang MC, Go AS, Chang Y, Borowsky LH, Pomernacki NK, Udaltsova N, Singer DE. A
new risk scheme to predict warfarin-associated hemorrhage: The ATRIA (Anticoagulation and
Risk Factors in Atrial Fibrillation) Study. J Amer Col Cardio. 2011;58:395-401.
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
18. Arnason T, Wells PS, van Walraven C, Forster AJ. Accuracy of coding for possible warfarin
complications in hospital discharge abstracts. Thromb Res. 2005;118:253-262.
19. CMS. Appendix E Operating Room Procedures and Procedure Code/MS-DRG
Code/MS-DR
RG Index.
Inde
In
dex.
de
x. 2014
201
0144
ed. http://www.cms.gov/icd10manual/fullcode_cms/P0033.html. Accessed Mar 228,
8, 22016.
016.
01
6.
20. Healthcare Cost and Utilization Project (HCUP). HCUP Comorbidity Software. 2008.
Agency
Healthcare
Rockville,
www.hcupAgen
en
ncy ffor
or H
ealt
lthc
lt
h are Research and Quality, Ro
ock
ckvi
v lle, MD. www.hcu
cu
upus.ahrq.gov/toolssoftware/comorbidity/comorbidity.jsp.
uss.a
.ahhrq.gov/
hr
v/to
v/
toolssoftware/comorbidity/comorbidiity
to
y.jsp. Accessed
ed Mar 28, 2016.
21.
2 . Schoenman JA,
21
JA, Sutton
JA
Suuttton JP,
JP, Elixhauser
Elixhau
useer A, Love
Lovee D.
D. Understanding
Und
ndeersstan
ndiing and
nd Enhancing
Enh
nhancinng the
nh
thee Value
Valuue of
Hospital
Discharge
Data.
Care
Hosp
Ho
spit
sp
i al Dis
issch
c arrgee Da
ataa. Med
Meed Ca
C
re Res
es Rev.
Rev
evv. 22007;64:449-468.
0077;64::44
449-46
468.
46
8
22.
Health
Information
Systems.
groups
22 3M H
ealt
ea
lthh In
lt
Info
form
fo
rmat
rm
atio
at
ionn Sy
io
S
yst
stem
st
emss. HCUP
em
HCU
CUP
P All
All Patient
Pati
Pa
tien
ti
entt Refined
en
Refi
Re
fine
fi
nedd Diagnosis
ne
Diag
Di
agno
ag
nosi
no
siss Related
si
Rela
Re
late
la
tedd gr
te
grou
oups
ps ((APR
APR
AP
R
DRGs), Version 24.0. Methodology Overview. 2007. https://www.hcupus.ahrq.gov/db/nation/nis/v24_aprdrg_meth_ovrview.pdf. Accessed Mar 28, 2016.
23. Baram D, Daroowalla F, Garcia R, Zhang G, Chen J.J., Healy E, Riaz A, P R. Use of the All
Patient Refined-Diagnosis Related Group (APR-DRG) Risk of Mortality Score as a Severity
Adjustor in the Medical ICU. Clin Med Insights Circ Respir Pulm Med. 2008;2:19-25.
24. Austin PC, Schuster T. The performance of different propensity score methods for estimating
absolute effects of treatments on survival outcomes: A simulation study. Stat Methods Med Res.
2014. Feb 3. [Epub ahead of print] doi:10.1177/0962280213519716.
25. Curtis LH, Hammill BG, Eisenstein EL, Kramer JM, Anstrom KJ. Using inverse probabilityweighted estimators in comparative effectiveness analyses with observational databases. Med
Care. 2007;45:S103-107.
26. Liu J, Weinhandl ED, Gilbertson DT, Collins AJ, St Peter WL. Issues regarding /`immortal
time/' in the analysis of the treatment effects in observational studies. Kidney Int. 2012;81:341-
18
DOI: 10.1161/CIRCULATIONAHA.115.020338
350.
27. Giobbie-Hurder A, Gelber RD, Regan MM. Challenges of Guarantee-Time Bias. J Clin Onc.
2013;31:2963-2969.
28. Lévesque LE, Hanley JA, Kezouh A, Suissa S. Problem of immortal time bias in cohort
studies: example using statins for preventing progression of diabetes. BMJ. 2010;340:340:b5087.
29. Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, Huisman, M, King CS,
Morris T, Sood N, Stevens SM, Vintch JRE, Wells P, Woller SC, Moores CL, Antithrombotic
Therapy for VTE Disease: CHEST Guideline, Chest 2016;149:315-352.
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
30. Muriel A, Jimenez D, Aujesky D, Bertoletti L, Decousus H, Laporte S, Mismetti P, Munoz
FJ, Yusen R, Monreal M. Survival effects of inferior vena cava filter in patients with acute
symptomatic venous thromboembolism and a significant bleeding risk. J Am Coll Cardiol.
2014;63:1675-1683.
31. Fernandes TM, White RH. Immortal time bias and the use of IVC filters. J Am C
Coll
o l Cardiol.
ol
2014;64:955.
32. Stein PD, Matta F. Vena cava filters in unstable elderly patients with acute pulmonary
embolism. Am J Med. 2014;127:222-225.
33.
PD,
vena
333. Stein
St PD
D, Dalen JE, Matta F. Underuse of ven
na cava filters in
n uunstable
nstable patients with acute
pulmonary
embolism.
pulm
monary embo
boliism
bo
m. Am J Med.
Med
ed. 2014;127:6.
201
014;
4 127:
7:6..
7:
34.
T,, Yasunaga
344. Isogai
Isog
Is
o ai T
Y su
Ya
sunagga H, Matsui
Mats
Mats
tsui H,
H, Tanaka
Tannaka H,
Ta
H, Horiguchi
Hooriggucchi H,
H Fushimi
Fushhimi
m K.
K. Effectiveness
Effe
Ef
feectiven
enesss of
en
of
Inferior
Therapy.
Med.
nferi
rior
ri
or Vena
Vena Cava
Cava Filters
Fil
ilte
terrs
rs on Mortality
Morrtality
Mo
rt y as an
an Adjuvant
Adju
Ad
juva
vant
ntt to
to Antithrombotic
Anttith
An
hro
romb
mbot
mb
otic
ic T
heera
rapy
py. Am
py
mJM
ed.
ed
2015;128:312.e23-31.
2015
20
15;1
15
;128
;1
28:3
28
:312
:3
12.e23
e23-31
3 1.
35. Tavora F, Crowder C, Kutys R, Burke A. Discrepancies in initial death certificate diagnoses
in sudden unexpected out-of-hospital deaths: the role of cardiovascular autopsy. Cardiovasc
Pathol. 2008;17:178-182.
19
DOI: 10.1161/CIRCULATIONAHA.115.020338
Clinical Perspective
This observational study analyzed outcomes associated with inferior vena cava filter (VCF) use
in 85159 patients who were hospitalized for acute venous thromboembolism (VTE). There was a
statistically significant 30% reduction in the 30 & 90-day risk of death in the patient treated with
a VCF vs. no-VCF, but this was observed only in the small subgroup (3.5%) of patients who had
active bleeding. Among patients (1.8%) who underwent major surgery immediately before or
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
during the acute-VTE hospitalization, use of a VCF was not beneficial. In the remaining 80697
patients (95%) who had no-contraindication to anticoagulation therapy, use of a VCF (N= 7762)
had no effect on survival or the risk of developing a pulmonary embolism (PE) w
within
ithi
it
hinn 1 ye
hi
year
year,
ar, bu
ar
bbutt
VCF-use did increase the risk of recurrent deep-vein-thrombosis (DVT) by 50%. These findings
were
ree similar
sim
imil
ilar
il
ar to
to the
th
he results of two small randomized
randomiize
zedd studies, which reported
repoort
rted
e that use of a VCF did
nnot
ot reduce the risk
ris
iskk off subsequent
sub
ubse
sequ
se
quen
qu
entt PE,
en
PE but
but did
bu
did lead
lead
d too ann increase
inc
ncre
reas
re
a e inn the
as
the rrisk
issk de
dev
developing
velo
velo
lopi
ping
pi
ng a nnew
ew
DVT.
this
study
are
alignment
with
the
American
College
DVT
DV
T. The ffindings
T.
indinngs off th
in
his st
tud
udyy ar
re in
n al
lign
nme
ment w
ith
h th
he rrecent
ecen
ec
nt 2016
2016
1 A
merrica
can Co
ca
Col
lleg
ge of
Chest
Ches
Ch
estt Ph
es
Phys
Physician
ysic
sic
icia
iann An
ia
Anti
Antithrombotic
tith
ti
thro
th
romb
ro
mbot
mb
otic
ot
ic T
Therapy
hera
he
rapy
ra
py ffor
or V
VTE
TE D
Disease
isea
is
ease
ea
se G
Guidelines,
uiide
uide
deli
line
li
ness, whi
ne
which
hich
hi
ch rrecommends
ecom
ec
omme
om
mend
me
ndss th
nd
that
at a
VCF not be inserted in patients with acute VTE who can be treated with standard anticoagulation
therapy. In light of the American Board of Internal Medicine’s “Choosing Wisely” initiative, the
implications are straightforward: do not use a VCF if your patient can receive standard
anticoagulation therapy.
20
DOI: 10.1161/CIRCULATIONAHA.115.020338
Table 1. Baseline Characteristics of Acute VTE Patients in each Subgroup.
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
Variable
Age
<50
50
50-59
0-59
60-69
0-69
70-79
0-79
80+
0+
Gender
er
Male
Female
ema
male
ma
l
le
Race-Ethnic
Ethni
nc
Non-hispanic
on-hi
h spanic White
African-American
frican-American
a
Hispanic
isp
spanic
ni
Asian/Pacific
sian/
n/Pa
n/
Paci
Pa
cifi
ci
ficc Is
fi
Isla
Islander
landerr
la
Other/Unknown
ther/Unknown
Insurance
ance
Medicare
Medi-Cal, government
Private
Self-Pay
Other/Unknown
Bleeding
POA=Y
POA=N
No Bleed
Group 1: No Contraindication to
Anticoagulation
N= 80697 (94.8%)
Group 2:
Surgery (+/- Bleed)
N= 1445 (1.8%)
Group 3:
Active Bleeding
N=3017 (3.5%)
%
No VCF
(N=72935)
%
VCF
(N=7762)
p-value
%
No VCF
(N=956)
%
VCF
(N=489)
p-value
%
No VCF
(N=1922)
%
VCF
(N=1095)
p-value
26.0
16.4
16.5
18.3
22.9
16.1
12.9
15.9
21.1
34.1
<.001
<.001
0.15
<.001
<.001
27.0
16.9
16.3
20.5
19.2
17.8
18.0
18.4
21.3
24.5
0.001
0.62
0.32
0.73
0.02
22.7
14.5
14.55
15
15.3
.33
19.7
27.8
10.
0.7
7
10.7
12.0
12.0
15.9
15
.9
24.7
36.7
<.001
0.049
0.69
<.001
<.001
45.4
54.6
46.1
53.9
0.30
47.5
52.5
50.1
49.9
0.35
0.
35
49.0
51.0
43.2
56.8
0.002
6
69
.0
69.0
11.1
1
13.9
3
3.22
2.8
771.4
1.4
10.
00
10.0
12.
29
12.9
0
3.0
2.8
<
.001
<.001
.
0.003
.
0.011
0.22
0.22
0.82
64.3
43
11.77
166.11
16.1
4.7
4.7
3.1
69.1
9.22
9.2
14.33
45
4.
4.5
2.9
0.
0
077
0.07
0.155
0.15
0.377
0.37
0 866
0.
0.86
0.77
68
.22
68.2
11.0
12.9
5.0
0
5.0
3.0
67.
7.7
7.
7
67.7
10.
06
10.6
14.
44
14.4
4.4
4
4.4
2.9
0.78
0.74
0.24
0.45
0.95
49.6
12.0
34.7
3.3
0.3
62.6
8.3
26.4
2.3
0.3
<.001
<.001
<.001
<.001
0.826
52.2
11.4
33.9
2.3
0.2
54.6
10.4
33.3
1.4
0.2
0.39
0.58
0.83
0.26
0.99
56.1
11.2
27.8
4.2
0.6
67.9
8.7
21.7
1.3
0.5
<.001
0.03
<.001
<.001
0.67
-
6.0
4.2
90.5
12.3
12.3
76.5
<.001
<.001
<.001
79.1
22.0
71.6
31.0
<.001
<.001
-
21
DOI: 10.1161/CIRCULATIONAHA.115.020338
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
Type of Bleed
Intracranial
Gastrointestinal
Other Bleed or Transfusion
Major Surgery
Yes
No Surgery
Vascular Procedure
Prior Major Surgery
<3d
Prior Major Surgery
<4-60
4-60 d
Comorbidities
orbidities
0
1
2+
+
VTE Event
Even
nt
PE
E (+/(+/
+ - DVT)
D T)
DV
Proximal
rox
o imal
m DVT
Distal
istall DVT
Severity-of-Illness
ity-of-Illness
o
Minor
Mino
in r
Moderate
Mode
dera
de
r te
Major
Extreme
xtr
trem
emee
em
THROMBOLYTIC
OMBOLYTIC
Yes
Treatment
No
Risk of Mortality
Minor
Moderate
Major
Extreme
1.3
5.7
-
0.6
4.0
4.9
3.1
10.8
9.6
0.001
<.001
0.006
<.001
85.0
15.0
12.8
96.3
3.7
9.4
<.001
-
15.1
4.1
<.001
0.06
3.7
49.8
46.4
11.0
65.5
23.6
100.0
2.0
100.0
3.5
<.001
<.001
<.001
0.012
-
10.4
12.5
0.19
25.2
18.8
0.002
10.77
14.4
14.4
0.003
15.6
21.9
62.4
7.8
15.8
76.4
<.001
<.001
<.001
13.1
16.0
70.9
4.5
12.3
83.2
<.001
0.058
<.001
9.6
16.4
75.0
3.2
9.9
86.9
<.001
<.001
<.001
55.3
28
2
28.3
.3
16.4
1 .4
16
48.2
334.6
4.6
6
17.2
17.
72
<.001
<
<.
<.001
001
00.07
0.
07
45.6
41.4
.4
4
13.
13.0
30
52.4
330.3
0.3
0.
3
17
17.4
.44
0.015
0.01
015
<.
<.001
.00
001
1
00.024
. 244
.0
68.8
21
21.3
.33
9.99
56.7
226.8
68
6.
16.5
16.
6.5
6.
5
<.001
<.001
<.001
27.8
7
43.6
3.6
25.1
33.5
.5
5
14.4
4
338.5
8.5
8.
.
39.2
2
77.9
.9
9
<
<.001
.001
<.00
<.001
001
00
<
<.
<.001
001
1
<
<.001
.00
001
00
1
15.8
58
34
34.6
4.6
6
38
38.8
.8
8
10
10.8
.8
8
6.1
1
227.6
7.6
6
45.0
21
21.3
.3
3
<.00
<.001
001
00
0.
0.007
.00
0 7
0.024
<
<.001
.00
001
00
1
10.2
336.6
36
.6
6
40.0
40
0
13
13.2
.2
2
44.2
4.
2
24.
24.4
44
51.6
19
19.8
.8
8
<.001
<.001
<.001
<.001
2.0
8.7
<.001
7.1
9.0
0.20
4.0
7.3
T<.001
98.0
91.3
92.9
91.0
96.0
92.7
52.8
30.8
14.0
2.4
30.9
37.4
26.2
5.4
21.7
36.7
20.7
4.9
22.5
38.2
28.4
10.8
34.8
33.9
23.4
7.9
16.8
36.4
35.0
11.8
<.001
<.001
<.001
<.001
22
<.001
0.57
<.001
<.001
<.001
0.15
<.001
<.001
DOI: 10.1161/CIRCULATIONAHA.115.020338
Table 2. Study Outcomes of Death and Recurrent Thromboembolism.
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
Study Sub-Group
1)) No Contraindication
To Anticoagulation
2)) Ma
Majo
Major
j r Surgery
jo
Surger
eryy
er
3)) Ac
Acti
Active
tive
ti
ve B
Bleeding
leed
le
edin
ed
ingg
in
Outcome
Death 30 days
from admission
Hazard
Ratio
(VCF Use
Analytic Method
vs. No VCF) 95% CIs
Propensity-IPW, Adjusted for ITB
1.12
(0.98-1.28)
Propensity-matched, Adjusted for ITB
1.03
(0.90-1.19)
Pvalue
0.11
0.61
Death 90 days
Propensity-IPW, Adjusted for ITB
1.15
(1.05-1.27)
(1.
1 05
1.
05-1
1.2
.27)
7
0.004
PE 1 yr. of discharge
DVT 1 yr. of discharge
Propensity-IPW
Propensity-IPW
1.05
5
1.53
(0
(0.89-1.24)
0.8
.899-1.
91.24
1.
24))
24
(1.34-1.74)
0.56
<.0001
Death 30 days
Propensity-IPW, Adjusted for ITB
1.12
(0.71-1.77)
0.63
after surgery
Death 90 days
PE 1 yr.
r.. after
aft
fter
er surgery
sur
u ge
gery
DVT 1 yr.
DV
r after surge
surgery
g ry
y
Death
De
ath
th 30 days
daays
y
ffrom
fr
om admission
adm
dmis
issi
is
sion
si
Death
Deat
De
athh 9900 days
at
days
PE 1 yr
yr. of discharge
DVT 1 yr. of discharge
Propen
Propensity-matched,
nsi
sity
ty-m
ty
- atched, Adjusted for ITB
TB
Propensity-IPW,
Prop
ensity
n t -IPW, Adjusted ffor
o ITB
or
Propensity-IPW
Prop
pen
ensi
sity
si
ty-I
ty
-IPW
W
Propensity-IPW
Pr
open
pen
e si
sity
ty-IPW
I
Propensity-IPW,
Prop
r ensity
n t -IIPW
PW, Ad
A
Adjusted
djust
u ed
d ffor
o IITB
or
TB
B
Propensity-matched,
Prop
Pr
open
op
en
nsi
sity
ty-m
ty
-mat
atch
tch
ched
ed, Ad
ed
Adju
Adjusted
justed
ted ffor
o IITB
or
TB
Propensity-IPW,
Prop
Pr
open
op
ensi
en
sity
si
ty-I
ty
-IIPW
PW, Ad
Adju
Adjusted
just
ju
sted
st
ed ffor
or IITB
TB
Propensity-IPW
Propensity
IPW
Propensity-IPW
1.63
1.10
0.85
0.
85
1.15
00.68
0.
68
0.61
0.
61
00.73
.73
73
11.04
04
2.35
(0.70-3.78)
(0.76-1.60)
(0.35-2.10)
(0
.3355-2.
2.10
10)
0)
(0.57-2.32)
(0
0.57-2.32
3 )
(0.52-0.88)
(0
0.52-0.88
8 )
(0.39-0.95)
(0
.39.3
399-0.
0 95
0.
95))
(0.59-0.90)
(0
.59599 0.90
90))
90
(0.67-1.61)
(0
67 1 61)
(1.56-3.52)
0.25
0.61
0.73
0.70
0.003
0.027
0.003
0.88
<0.001
All hazard ratios reflect VCF use vs. No use.
VCF = Vena cava filter
IPW = Inverse probability weighted
ITB = Immortal time bias
23
DOI: 10.1161/CIRCULATIONAHA.115.020338
Figure Legends:
Figure 1. Study Flow Diagram.
Figure 2. Forest Plot of Multivariable Model to Predict Death < 30 days in Patient with No
Contraindication to Anticoagulation.
Figure 3. Forest Plot of Multivariable Model to Predict Death < 30 days in Patients undergoing
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
Major Surgery.
Figure 4. Forest Plot of Multivariable Model to Predict Death < 30 days in Patientss with
witth Active
Acti
tive
Bleeding.
Bleeding
g.
Figure
Figu
Fi
ure 5. Stan
Standardized
andaard
an
dizeed Mea
Mean
an Di
D
Differences
fferren
ncees be
between
etw
ween Ca
Cases
ase
sess wi
w
with
th a V
Vena
ena Ca
C
Cava
avaa F
Filter
ilter ve
versu
versus
us Casess
without a Vena Cava Filter who had No Contraindication to Anticoagulation.
Anticoagu
g lation.
Figure 6. Standardized Mean Differences between Cases with a Vena Cava Filter versus Cases
without a Vena Cave Filter who underwent Major Surgery.
Figure 7. Standardized Mean Differences between Cases with a Vena Cava Filter versus Cases
without a Vena Cave Filter who had Active Bleeding.
Figure 8. Hospital Day of Death among Patients with Active Bleeding who Received or did not
Receive a Vena Cava Filter.
24
Acute VTE Cases N=104,677
First admission with a principal diagnosis of
pulmonary embolism or venous thromboembolism
in the study period (POA Y): 2005 through 2010
Exclude cases with an
active cancer:
N=18,735
Exclude cases from
Hospitals < 55 Acute
VTE opportunities:
N=783
Acute-VTE, No Cancer: N= 85,159
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
No Contraindication
Major Operating Room
Procedure (+/- Bleeding*)
N=80,697
N=1,445
1) NO operation in-hosp
AND
2) No recent operation
< 3 days prior to admit
AND
2)) No bleeding,
bleed
din
ing, either
POA
A = Y or N
1) Major operation during
hospital stay
OR
2) Recent operation
< 3 days prior to admit
Bleeding Coded
POA = Y or N
(without surgery)
N=3,017
1) Bleed POA = Yes
OR
2) Bleed POA = No
*Bleed POA
OA Y or N
included if surgery
VCFF
VC
N V
No
VCF
CF
VCFF
VC
N VCF
No
VCF
VCFF
VC
N V
No
VCF
CF
N=7,762
N=72,935
N=489
N=956
N=1,095
N=1,922
VTE = Venous thromboembolism
VCF = Vena Cava Filter
1
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
No Filter
9%
Filter
6%
3%
Hospital Day Patient Died
29
25
21
17
13
9
5
1
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
0%
Percent Deaths Occuring within 30-days of
Admission
12%
Outcomes After Vena Cava Filter Use in Non-Cancer Patients with Acute Venous
Thromboembolism: A Population-Based Study
Richard H. White, Ann Brunson, Patrick S. Romano, Zhongmin Li and Ted Wun
Circulation. published online April 5, 2016;
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 2016 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://circ.ahajournals.org/content/early/2016/04/05/CIRCULATIONAHA.115.020338
Data Supplement (unedited) at:
http://circ.ahajournals.org/content/suppl/2016/04/05/CIRCULATIONAHA.115.020338.DC1.html
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in
Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.
Once the online version of the published article for which permission is being requested is located, click Request
Permissions in the middle column of the Web page under Services. Further information about this process is
available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/
SUPPLEMENTAL MATERIAL
Supplemental Table 1. ICD-9-CM Codes to Identify Cases with PE or Lower
Extremity DVT.
CODE
673.2
415.11
415.13
415.19
VTE Type
PE
PE
PE
PE
DESCRIPTION
Obstetrical blood clot embolism (PE) (673.2)
Iatrogenic pulmonary embolism and infarction (415.11)
Saddle pulmonary embolus
Other pulmonary embolism (415.19)
453.2
453.8
451.11
451.19
451.81
453.40
453.41
453.42
671.31
671.33
671.42
671.44
LE-DVT
LE-DVT
LE-DVT
LE-DVT
LE-DVT
LE-DVT
LE-DVT-PROXIMAL
LE-DVT-DISTAL
LE-DVT
LE-DVT
LE-DVT
LE-DVT
Venous thrombosis of inferior vena cava (453.2)
(PRE Oct 1, 2009) eliminated Oct 1, 2009
Thrombophlebitis, deep vessels of lower extremities femoral vein (451.11)
Thrombophlebitis of deep vessel of lower extremities, other (451.19)
Thrombophlebitis of other sites iliac vein (451.81)
Acute venous thrombosis of unspecified deep vessels of lower extremity (453.40)
Acute venous thrombosis of deep vessels of proximal lower extremity (453.41)
Acute venous thrombosis of deep vessels of distal lower extremity (453.42)
DVT antepartum-Delivered (671.31)
DVT-antepartum (671.33)
Thrombosis postpartum-del W P/P (671.42)
DVT-postpartum (671.44)
Supplemental Table 2. ICD-9-CM Codes to Identify Cases with Acute Bleeding.
Outcome
Intracranial
hemorrhage
ICD-9-CM Codes
430- subarachnoid
431-intracerebral
432.0-other ICH
432.1-Subdural
432.9-Unspecified
Note: all 5th digits 0-9 are searched for
using the following traumatic ICH codes:
852.0-SAH after injury
852.2-subdural after injury
852.4-extradural after injury
853.0- other after injury
Excluded Codes
All codes for ICH with open
intracranial
wound (i.e., 852.1 852.3,
852.5, 853.1)
Outcome
GI hemorrhage
Codes Included
455.2-internal hemorrhoids
455.5-external hemorrhoids
455.8- unspecified hemorrhoids
456.0-varices with bleeding
456.20-varices with bleeding
459.0-hemorrhage unspecified
530.7-laceration hemorrhage
530.82 esophogeal hemorrhage
531.00-.01-gastric ulcer bleed +/- obstruct
531.20-.21- gastric ulcer bleed+perf+/- obstr
531.40-.41-chronic gastric bleed
531.60-.61-chronic gastric bleed+perf
532.00-.01-duodenal ulcer bleed+/-perf
532.20-.21- duodenal ulcer bleed+perf+/- obstr
532.40-.41- chronic duodenal+ bleed
532.60-.61- chronic duodenal bleed+perf
533.00-.01- peptic ulcer bleed +/- obstruct
533.20-.21- peptic ulcer bleed+perf+/- obstr
533.40-.41- chronic peptic+ bleed
533.60-.61- chronic peptic bleed+perf
534.00-.01-gastrojejunal bleed
534.20-.21- gastrojejunal bleed + perf
534.40-.41- chronic gastrojejunal bleed
534.60-.61- chronic gastrojejunal + perf
535.01- acute gastritis with bleed
535.11-atrophic gastritis with bleed
535.21-gastric mucosal hypertrophy + bleed
535.31-alcoholic gastritis+bleed
535.41-other gastritis +bleed
535.51-unspecified gastritis with bleed
Excluded Codes
All ulcer codes without
mention of hemorrhage
(e.g., 534.31, 534.51)
535.61-duodenitis with bleed
537.83 angiodysplasia with bleed, stomach
562.02 small bowel diverticulosis with bleed
562.03-small bowel diverticulitis with bleed
562.12 diverticulosis of colon with bleed
562.13 diverticulitis of colon with bleed
568.81-hemoperitoneum
569.3-hemorrhage of anus and rectum
569.85-angiodyplasia of intestine with bleed
578.0-hematemesis
578.1-blood in stool
578.9-GI hemorrhage, not specified
Outcome
Other bleed
Codes Included
423.0 (hemopericardium)
593.81 (vascular disorders of kidney)
599.7 (hematuria)
719.1x (including fifth digits: 0-9)
784.7 (epistaxis)
784.8 (hemorrhage from throat) (added
12/4/00)
786.3 (hemoptysis)
Excluded Codes
623.8 (excessive vaginal
bleeding)
626.2 (excessive vaginal
bleeding
626.6 (menorrhagia)
Supplemental Table 3. ICD-9-CM Codes to Identify Vascular Interventions the
Might Reflect Procedures done to Remove or Thrombolyse a Lower Extremity
Deep Vein Thrombosis.
INCLUDED
ICD-9-CM CODE
00.66
38.08
38.09
38.18
39.50
ICD-9-CM CODE DESCRIPTION
PTCA OR CORONARY ATHER (Begin 2005)
EMBOLECTOMY LEG VESSEL
LOWER LIMB VEIN INCISION
ENDARTERECTOMY LEG VESL
ANGIOPLAST/ATHERECT (Begin 1995)
EXCLUDED
ICD-9-CM CODE
38.03
38.07
39.27
39.56
39.57
39.58
39.59
39.99
54.0
ICD-9-CM CODE DESCRIPTION
UPPER LIMB VESSEL INCIS
ABDOMINAL VEIN INCISION
DIALYSIS ARTERIOVENOSTOM
REPAIR VESS W TIS PATCH
REP VESS W SYNTH PATCH
REPAIR VESS W PATCH NOS
REPAIR OF VESSEL NEC
VESSEL OPERATION NEC (filer removal)
ABDOMINAL WALL INCISION
Use of aThromobolytic AGENT
ICD-9-CM =99.10