A Study of the Cough Reflex in Idiopathic Pulmonary Fibrosis
advertisement

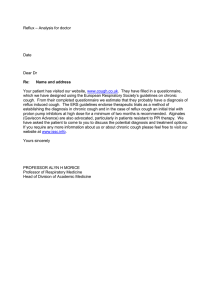
A Study of the Cough Reflex in Idiopathic Pulmonary Fibrosis Benjamin D. M. Hope-Gill, Simon Hilldrup, Christine Davies, Russell P. Newton, and Nicholas K. Harrison Respiratory Unit and Pathology Department, Morriston Hospital; and Biological Sciences, University of Wales, Swansea, United Kingdom Little is known about the pathogenesis of cough in idiopathic pulmonary fibrosis (IPF). We hypothesized that abnormalities of respiratory tract tachykinin-containing sensory nerves may be implicated. We studied cough response to capsaicin, substance P (SP), and bradykinin in 10 healthy control subjects and 10 patients with IPF. Six patients were tested before and after steroid therapy. Induced sputum cell counts and neurotrophic factor levels were also measured in 13 patients and 13 control subjects. The results show that cough sensitivity to capsaicin was greater in patients (p ⬍ 0.01). Neither SP nor bradykinin induced cough in normal subjects. SP and bradykinin induced cough in 7/10 patients (p ⬍ 0.002) and 2/10 patients (not significant) with IPF, respectively. Prednisolone caused a reduction in cough sensitivity to capsaicin (p ⬍ 0.05) and SP (p ⬍ 0.05) in all six patients treated. There were significantly more neutrophils (p ⫽ 0.001) and higher levels of nerve growth factor (p ⬍ 0.01) and brain-derived neurotrophic factor (p ⬍ 0.01) in patient’s sputa. These findings suggest functional upregulation of lung sensory neurones in IPF. The cough response to inhaled SP in most patients may reflect disrupted respiratory epithelium. The response to corticosteroids demonstrates that the cough is amenable to therapy. Keywords: idiopathic pulmonary fibrosis; cough; neurotrophins Idiopathic pulmonary fibrosis (IPF) is a condition characterized by fibroproliferation and modest mononuclear inflammation of the pulmonary interstitium. Patients typically present with worsening shortness of breath. However, an irritating, nonproductive cough is an additional distressing feature in 73 to 86% of cases (1, 2). Little is known about the pathogenesis of this cough, which frequently proves resistant to conventional antitussive therapies. Anecdotal evidence suggests that corticosteroids may be beneficial, but there have been no formal studies to confirm this. One previous study reported enhanced cough reflex sensitivity to inhaled capsaicin in patients with IPF. By simulating a restrictive defect in normal subjects, they demonstrated that this was not due to greater deposition of aerosolized particles in proximal airways (3). This suggests there is something intrinsic to the mechanism of disease in IPF that enhances the cough reflex. Cough is mediated by the interaction of sensory afferent nerves, central cough reflexes, and local axon reflexes (4). Various peptides have been implicated in the modulation of the sensory afferents, and it is known that airway sensory fibers can mediate neurogenic inflammation as an effector function within the respiratory epithelium (5). Previous studies suggest there are two principal cough receptors: rapidly adapting receptors, (Received in original form April 30, 2003; accepted in final form July 31, 2003) Supported by a grant from Iechyd Morgannwg Health R&D Consortium. Astra Zeneca Pharmaceuticals donated the Omeprazole used in this study. Correspondence and requests for reprints should be addressed to Nicholas K. Harrison, M.D., F.R.C.P., Respiratory Unit, Morriston Hospital, Swansea, SA6 6NL UK. E-mail: resp.unit@swansea-tr.wales.nhs.uk Am J Respir Crit Care Med Vol 168. pp 995–1002, 2003 Originally Published in Press as DOI: 10.1164/rccm.200304-597OC on August 13, 2003 Internet address: www.atsjournals.org which are innervated by A␦ fibers, and unmyelinated c-fibers (4, 5). Unmyelinated sensory fibers have been shown using immunohistochemical techniques to contain calcitonin gene–related peptides and the tachykinins, substance P (SP) and neurokinin A (6, 7). When stimulated by irritants such as capsaicin, c-fibers antidromically release calcitonin gene–related peptides, SP and neurokinin A (6, 8). Capsaicin is a vanilloid extract from hot pepper, which acts specifically on c-fibers at low concentrations but does not cause tachyphylaxis, thus allowing the construction of dose–response curves (9–13). Animal studies have shown that pretreatment with bradykinin increases this effect, suggesting that in inflammatory conditions bradykinin may sensitize sensory afferents (14, 15). By contrast, the in vitro insensitivity of rapidly adapting receptors to chemical irritants supports the notion that such irritants have an indirect action on these fibers (4, 5). Furthermore, both SP and neurokinin A have been shown to stimulate fibroblast proliferation, and neurokinin A increases fibroblast chemotaxis in vitro (16). In other conditions characterized by cough such as asthma, it has been reported that there is an increase in tachykinincontaining nerves within the larger airways (17, 18). There is also evidence of increased levels of neurotrophic factors in the airways in asthma (19, 20). Neurotrophic factors in turn may modulate neuronal mechanisms that induce cough. Whether levels of neurotrophic factors are increased in IPF is not known. In this context the aims of the present study were: To examine the cough reflex response to capsaicin in a defined group of patients with IPF, in whom all other causes of cough had been excluded. To determine the cough response to bradykinin and SP and investigate whether these peptides modulate the cough response to capsaicin. To measure levels of the neurotrophic factors: nerve growth factor (NGF), brain-derived neurotrophic factor (BDNF), and glial cell line–derived neurotrophic factor in the epithelial lining fluid of the larger airways by analyzing induced sputum. To assess the effect of oral corticosteroid therapy on the cough response to capsaicin and SP in a smaller group of patients with IPF who had severe cough. Some of the results of these studies have been previously reported in the form of abstracts (21–24). METHODS Patients Thirteen patients fulfilling the American Thoracic Society criteria for the diagnosis of IPF were recruited (25). All patients were elderly (mean age 71.7 years) and had clinical, and physiologic features consistent with a diagnosis of IPF. They also had characteristic changes on highresolution computed tomography scan, and therefore surgical lung biopsies were not performed. Thirteen healthy volunteers acted as control 996 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 168 2003 subjects. Exclusion criteria are shown in Table 1. Informed consent was obtained from all subjects, and the Local Research Ethics Committee approved the study. All 13 patients studied had a metacholine challenge to exclude airway hyperreactivity (26). No patients or control subjects with a history of gastroesophageal reflux (GER) were included. Patients but not control subjects were given the proton pump inhibitor Omeprazole (AstraZeneca Pharmaceuticals Ltd., Loughborough, UK) 20 mg/day for 1 month before starting the study and continued this therapy for its duration to exclude subclinical GER. No patients or control subjects had smoked within 1 year of testing. All subjects were asked to grade their cough severity from 0 (no cough) to 10 (disabling) using a 10-cm visual analog scale (VAS). Measurement of pulmonary function was performed using published guidelines (26, 27). Cough Challenge Ten patients and 10 control subjects underwent an initial capsaicin cough challenge by compressed air–driven dosimeter (Mefar MB3, Bovezzo, Italy) as described elsewhere (16). Dosimeter driving pressure 1.8 ⫾ 0.1 bars, aerosol output of 9.7 mg/second, particle mass mean diameter 3.5 m, and fixed 1-second inhalation and 60-seconds pause times were set. Two further capsaicin challenges were performed. The first repeat capsaicin challenge occurred at least 1 minute after SP inhalation, and the second challenge occurred 1 hour later. Similar capsaicin challenges before and after bradykinin inhalation were performed 1 week later. One micrometer solutions of each of SP and bradykinin (Clinalfa, Nottingham, UK) were prepared. Five separate inhalations of each solution were received within 5 minutes of the initial capsaicin challenge on each occasion, providing total doses of 0.50 g bradykinin and 0.64 g SP, respectively. Inhalations of these substances were received at 60-second intervals. Six additional patients with IPF, diagnosed using the same criteria (25), who had disabling cough were treated with oral Prednisolone 40 to 60 mg/day for at least 4 weeks. Patient selection for this group was based on severity of cough symptom (all had a VAS score greater than 5); however, there was no difference in lung function tests between these patients and those not treated with steroids. Before starting steroid therapy they underwent a capsaicin cough challenge followed by SP inhalation, and these tests were then repeated after 4 weeks of treatment. Coughs produced within 60 seconds of each inhalation were recorded. Cough threshold was defined as the concentration causing two or more coughs (C2). The concentration causing five coughs (C5) was also recorded. The challenge was terminated at C5 or when the maximum concentration of inhalant was reached. Sputum Induction and Processing Sputum was induced in 13 patients with IPF and 13 control subjects by a standard technique (28) using an ultrasonic nebulizer (Sonix 2000; Medix, Harlow, UK; 0.7 ml/minute output, 5.5 m mean particle size). Increasing concentrations of hypertonic saline (3, 4, 5%) were administered, each for 5 minutes. Expectorated sputum was collected on ice and processed immediately at 4⬚C as described previously (29). Sputum plugs were selected and divided into two parts. Briefly, one part was treated with 4⫻ wt/vol 0.1% dithiothreitol (DTT) (Sigma, Poole, UK) plus 4⫻ wt/vol Dulbecco’s phosphate-buffered saline (Sigma). The suspension was filtered through 48 m nylon gauze (Sefar Ltd, Bury, UK) and centrifuged at 2,000 rpm for 10 minutes. The supernatant was decanted and stored at ⫺80⬚C pending measurement of NGF and albumin levels. The cellular portion was resuspended in Dulbecco’s phosphate buffered saline and total cell counts were performed using a Neubauer Haemocytometer (Fisher Scientific, Loughborough, UK). The remaining selected sputum plugs were treated with equal wt/vol 1% protease inhibitor cocktail (containing 4-(2-aminoethyl)benzenesulfonyl fluoride hydrochloride (AEBSF), Aprotonin, Leupeptin, Bestatin, Pepstatin A and E-64) (Sigma). The suspension was treated as described previously and the supernatant stored at ⫺80⬚C pending measurement of BDNF and glial cell line–derived neurotrophic factor levels. Neurotrophic Factor ELISA Assays NGF, glial cell line–derived neurotrophic factor (Promega, Southampton, UK), and BDNF (R&D Systems Europe Ltd, Abingdon, UK) were measured in sputum samples using a quantitative “sandwich” enzyme assay technique. Samples were run in duplicate and compared with a standard curve. Results were corrected for sample dilution and expressed as absolute values. Statistical Analysis Negative logarithmic transformation was applied to construct dose– response curves. Mann–Whitney U test and Wilcoxon’s signed rank test were used to compare nonparametric data. Fisher’s exact test was used to compare response to bradykinin and SP. The unpaired t test was used to compare baseline variables between groups and the Spearman’s rank correlation was used to analyze association between variables (30). p Values less than 0.05 was taken as significant (30). The software package SPSS (SPSS, Inc., Chicago, IL) was used for statistical analysis. RESULTS Baseline Data Demographic and pulmonary function data for patients and control subjects are shown in Table 2. Cough symptom severity as assessed by VAS is shown in Table 3. Patients with IPF had significantly greater cough symptom scores assessed by VAS compared with normal subjects (p ⬍ 0.05). There was no correlation in the IPF group between cough symptom severity as assessed by the VAS score and any measurement of pulmonary function (FEV1, FVC, total lung capacity, and lung diffusing capacity for carbon monoxide [DlCO]). Capsaicin Cough Challenge In all subjects, a dose–response curve was constructed. No subject coughed during sodium chloride inhalation. After inhalation of capsaicin, it was observed that the cough response occurred immediately and was consistently completed within 15 seconds for both patients and control subjects. No subject had prolonged bouts of coughing. Figure 1A shows the concentration of capsaicin (⫺log10 ⫾ SEM) required to induce C2 in patients with IPF (2.97 ⫾ 0.40) was significantly lower than in control subjects (2.22 ⫾ 0.39; p ⬍ 0.01). The cumulative frequency plot in Figure TABLE 2. BASELINE DATA FOR PATIENTS WITH IDIOPATHIC PULMONARY FIBROSIS AND CONTROL SUBJECTS TABLE 1. STUDY EXCLUSION CRITERIA 1. 2. 3. 4. 5. 6. Evidence of respiratory tract infection within 1 mo History of smoking within 1 yr Postnasal drip, rhinitis, or catarrhal symptoms Symptoms of GER Asthma or other respiratory disease, other than IPF Angiotensin-converting enzyme inhibitor, bronchodilator, or nonsteroidal antiinflammatory drug therapy 7. Other major systemic illness Definition of abbreviations: GER ⫽ gastroesophageal reflux; IPF ⫽ idiopathic pulmonary fibrosis. Mean age, yr Sex, male:female Mean FEV1, % predicted FVC, % predicted TLC, % predicted DLCO, % predicted Control Subjects (n ⫽ 10 ) Patients with IPF (n ⫽ 10 ) 59.3 8:2 99.35 103.60 97.95 87.10 71.7* 9:1 84.68 77.43* 67.02* 42.44* Definition of abbreviations: DLCO ⫽ lung diffusing capacity for carbon monoxide; IPF ⫽ idiopathic pulmonary fibrosis; TLC ⫽ total lung capacity. * p ⬍ 0.05 compared with control subjects. Hope-Gill, Hilldrup, Davies, et al.: Cough in IPF 997 TABLE 3. BASELINE COUGH SYMPTOM VISUAL ANALOG SCALE DATA FOR INDIVIDUAL PATIENTS WITH IDIOPATHIC PULMONARY FIBROSIS AND CONTROL SUBJECTS Subject No. 1 2 3 5 6 7 8 9 10 Mean VAS Control Subjects Patients with IPF 0 0.5 0 0 3 0 2.5 1 1 0.8 5 0 1.5 3.5 1 4 5 5.5 8 4.0* Definition of abbreviations: IPF ⫽ idiopathic pulmonary fibrosis; VAS ⫽ visual analog scale. * p ⬍ 0.05. 1B further illustrates the difference in C2 response between the groups. Similar differences were seen for C5 values (IPF 2.70 ⫾ 0.60 vs. control subjects 1.01 ⫾ 0.59; p ⬍ 0.01). The mean concentration of capsaicin causing C2 and C5 at the first visit and a second visit 1 week later was reproducible (Figure 1C). There was no significant difference in the two-cough response (p ⫽ 0.87) or five-cough response (p ⫽ 0.32) to capsaicin in patients with IPF or in control subjects (p ⫽ 0.44, p ⫽ 0.75, respectively) between the two visits. In patients with IPF, cough sensitivity to capsaicin did not correlate with lung function (FEV1, FVC, total lung capacity, and DlCO), severity of disease on high-resolution computed tomography, or VAS grading of cough symptom severity. Effects of SP and Bradykinin Inhalation There was no significant change in immediate or delayed C2 or C5 cough response to capsaicin after SP inhalation (Figure 2). Similar results were obtained after inhalation of bradykinin (results not shown). Healthy control subjects showed no cough response to either SP or bradykinin inhalation. However, there was a direct cough response to inhaled SP in 7/10 patients with IPF (p ⬍ 0.002). Nine out of 10 patients completed five inhalations of SP. One patient tolerated one SP inhalation, which caused a prolonged paroxysm of coughing. As a result, this patient withdrew from further testing. In the other patients with IPF, cough response to SP occurred within a few seconds of inhalation and did not produce prolonged paroxysms of coughing. The total number of coughs produced in response to five sequential SP inhalations, each 1 minute apart, ranged between 2 and 56 coughs. However, patients with IPF showed no consistent dose–response to either sequential inhalations or increasing concentration (1.0 and 2.0 M) of SP. Only two/nine patients coughed in response to inhaled bradykinin (p ⫽ 0.21). One patient with IPF who had a prolonged paroxysm of coughing after SP inhalation declined further testing with bradykinin due to discomfort caused by the previous cough response. Effects of Prednisolone Therapy Figure 3A shows that in all six patients from the additional group treated with corticosteroid therapy there was a significant reduction in cough reflex sensitivity to capsaicin (p ⬍ 0.05). Figure 3B shows that Prednisolone markedly abrogated a direct cough response to SP inhalation in all patients (p ⬍ 0.03). This was associated with a reduction in mean VAS score from 7.2 ⫾ Figure 1. The concentration of inhaled capsaicin (mean ⫺log10 ⫾ SEM) required to induce both two and five coughs in patients with idiopathic pulmonary fibrosis (IPF) (circles) is significantly lower than in healthy control subjects (triangles); p value less than 0.01. The negative logarithmic transformation generates a higher numerical value for a lower dose of capsaicin for a given response (A ). The cumulative frequency plot in (B ) further illustrates the difference in two coughs (C2) response to increasing concentration of inhaled capsaicin between the groups. Reproducibility of C2 and five coughs (C5) response to inhaled capsaicin on two separate visits is shown in (C ). There was no significant difference in C2 or C5 cough response in either patients (circles) or control subjects (triangles) between Visit 1 and Visit 2. 998 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 168 2003 Figure 2. There was no difference in C2 response to inhaled capsaicin (mean –log10[capsaicin] ⫾ SEM) in either patients with IPF (triangles) or control subjects (circles) after substance P (SP) inhalation immediately or after 1 hour. Furthermore, there was no alteration in concentration of capsaicin required to induce five coughs after SP inhalation in either group (data not shown). Similarly, bradykinin inhalation had no effect on C2 or C5 cough response in either group (data not shown). 0.8 to 2.2 ⫾ 2.5 in this group (p ⬍ 0.05) (Figure 3C). Although five/six patients did show an improvement in gas transfer coefficient (Kco), there was no significant change in other lung function (FEV1, FVC, total lung capacity, DlCO) over the treatment period (data not shown). Sputum Induction Sputum induction was well tolerated in all subjects without a significant drop in FEV1. Sputum was induced in all 13 control subjects; however, adequate supernatant for analyzing NGF levels was obtained in 10/13 patients with IPF and for BDNF analysis in 12/13 patients. Sputum Cell Counts Selected sputum was mucoid with a mean percentage squamous cell count in both patients and control subjects of 8.8 ⫾ 7.6% and nonsquamous viability of 47.2 ⫾ 17.7% indicating adequacy of the selection process. The presence of significant numbers of macrophages and bronchial epithelial cells confirmed origin from the lower respiratory tract. The mean total cell count (⫻ 106/g sputum ⫾ SEM) was 4.9 ⫾ 4.8 in patients with IPF compared with 1.2 ⫾ 1.0 in control subjects (p ⫽ 0.001). There were significantly more neutrophils (2.8 ⫾ 3.9 vs. 0.29 ⫾ 0.31 ⫻ 106/g; p ⫽ 0.001) and lymphocytes (0.09 ⫾ 0.08 vs. 0.02 ⫾ 0.02 ⫻ 106/g; p ⬍ 0.01) in patients compared with control subjects. There was no significant difference in absolute count of macrophages (1.82 ⫾ 1.26, patients with IPF vs. 0.75 ⫾ 0.74, control subjects), eosinophils (0.07 ⫾ 0.09, IPF vs. 0.01 ⫾ 0.01, control subjects), or bronchial epithelial cell counts (0.12 ⫾ 0.66, IPF vs. 0.08 ⫾ 0.11, control subjects) between the groups. The predominant cell type in patients with IPF was the neutrophil (54 ⫾ 14.5%), whereas macrophages predominated (65 ⫾ 19.4%) in healthy control subjects (Figure 4). No subject had a sputum eosinophilia greater than 3% (Figure 4). Figure 3. (A ) Demonstrates a significant reduction in C2 response to inhaled capsaicin (⫺log10[capsaicin]) after steroid therapy in all six patients with IPF studied (p ⬍ 0.05). Steroid therapy also caused abrogation of the direct cough response to inhaled SP (B; p ⬍ 0.03). The total number of coughs in (B ) represents a cumulative cough score produced in response to five sequential inhalations of 1.0 M SP solution. (C ) Shows a significant reduction in cough symptom severity (p ⬍ 0.05) assessed by visual analog scale (VAS) in five/six patients with IPF after 4 weeks of steroid therapy. One patient was unable to reliably indicate cough symptom severity using the VAS. There was no difference in serum albumin levels between the groups. Neurotrophins in Induced Sputum Albumin Measurements Sputum albumin levels (mg/L ⫾ SEM) were 547 ⫾ 359 in patients with IPF compared with 246 ⫾ 172 in control subjects (p ⬍ 0.01). Serial dilutions of sputum showed good linearity with each of the assays used. BDNF was undetectable in samples processed with DTT, and there was poor average recovery from spiking Hope-Gill, Hilldrup, Davies, et al.: Cough in IPF 999 Figure 4. Neutrophils were the predominant cell type in sputa from patients with IPF (patients with IPF are represented by solid circles and control subjects by open circles). studies in these samples (7.9%). Therefore, measurements of BDNF were obtained from sputum portions processed separately without DTT, which showed good recovery from spiked samples (80.8%). Excellent recovery of NGF spiking was obtained from both DTT-processed (91.3%) and neat sputum (96.1%). However, preliminary studies indicated that higher levels of NGF were measured in samples processed with DTT. Therefore, DTT-processed samples were used for measuring NGF. Figure 5 shows that levels of NGF and BDNF were higher in sputum from patients compared with control subjects. Median values of NGF (ng/ml) were 23.13 in patients and 10.49 in control subjects (p ⬍ 0.01). Median values of BDNF (pg/ml) were 40.98 in patients and 17.87 in control subjects (p ⬍ 0.01). The glial cell line–derived neurotrophic factor was undetectable in induced sputa from either group. DISCUSSION The initial observations in this study confirm previous findings that patients with IPF have greater cough reflex sensitivity to inhaled capsaicin than healthy control subjects and that this cough response is highly reproducible (3). The careful exclusion of confounding factors such as bronchial hyperreactivity and GER strongly suggests that this enhanced cough is part of the underlying disease process. In addition we show, for the first time, that most patients with IPF cough in direct response to inhaled SP but not to bradykinin. Interestingly, neither inflammatory mediator altered cough reflex sensitivity to subsequent capsaicin challenge. We also demonstrate that oral corticosteroid therapy reduced cough reflex sensitivity to inhaled capsaicin and SP in all patients who received treatment. Furthermore, patients reported a clear reduction in cough symptoms as assessed by VAS after therapy. The induced sputum studies demonstrate that patients with IPF have higher levels of the neurotrophins NGF and BDNF in their bronchial epithelial lining fluid than healthy control subjects. Sputum neutrophilia and increased albumin levels reflect wellestablished findings from bronchoalveolar lavage studies in this condition (31, 32). However, a recent study has demonstrated that induced sputum samples central rather than peripheral airways and alveoli (33). It is therefore possible that our findings suggest inflammation within the more proximal bronchial epithelium where sensory innervation is greatest. Our observation that there was no correlation between cough reflex sensitivity, baseline lung Figure 5. There were higher levels of nerve growth factor (NGF) (p ⬍ 0.01) and brain-derived neurotrophic factor (BDNF) (p ⬍ 0.01) within induced sputa from patients with IPF (solid circles) compared with control subjects (open circles). There was inadequate supernatant obtained from three patients with IPF to allow NGF measurement and one patient for BDNF measurement. 1000 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 168 2003 function and severity of cough symptoms in patients with IPF provides indirect evidence for abnormalities affecting the central airways. By contrast, lung function tests reflect the disease process within the lung interstitium. Interestingly, prior inhalation of either bradykinin or SP did not result in an increase in cough reflex sensitivity to capsaicin. This was the case both for those who coughed in response to SP or bradykinin and those who did not. One reason for this may be that repeated inhalation of high doses of capsaicin causes a plateaux in cough response as has been observed previously in healthy subjects (34). This phenomenon occurred in seven of our control subjects and two patients with IPF who had a C2 response but did not cough five times even in response to the maximum concentration of capsaicin tested. However, consistent dose–response curves were obtained at lower doses despite sequential testing. It appears therefore that in some patients and most control subjects a maximum cough response is obtained beyond which no further increase in stimulation produces any additional effect. Alternatively, it is possible that individual subjects may exhibit idiosyncratic patterns of coughing, for example, some may control themselves to produce a few coughs only, whereas others may produce more prolonged paroxysms of coughing. We therefore conclude that the C2 threshold is a more reliable measure of cough reflex sensitivity than C5. Only two previous studies have investigated cough reflex sensitivity in fibrozing alveolitis. Doherty and coworkers found no association between cough reflex sensitivity to capsaicin and either cough symptom severity or lung function (3). Lalloo and coworkers made similar observations in patients with pulmonary fibrosis associated with systemic sclerosis (35). However, neither of these studies excluded the possible confounders of GER or bronchial hyperreactivity. Acid reflux is a recognized cause of chronic dry cough even in the absence of dyspeptic symptoms, and it enhances cough reflex sensitivity in patients without cough (36–39). It has also been proposed that GER may be an etiologic factor in IPF (39). Furthermore, GER is common in patients with systemic sclerosis, many of whom have esophageal dysmotility (40). For this reason we were careful to exclude subjects with symptoms of GER and gave empirical therapy with proton pump inhibitors to minimize any subclinical effect of this confounding factor (41). It is possible that the increased cough reflex sensitivity to capsaicin and SP observed in patients with IPF is caused by pretreatment with Omeprazole, as control subjects were not pretreated before testing. However, this seems unlikely given that Omeprazole therapy has been shown to improve cough symptoms (42–44) and reduce cough response to inhaled capsaicin (44) in patients with GER. All patients with IPF also had a negative metacholine challenge, thereby excluding bronchial hyperreactivity. In addition, the absence of sputum eosinophilia in these patients provides further evidence that an asthmatic component is not responsible for cough in IPF. Neurotrophins regulate the development and survival of distinct subsets of sensory neurones (45). They also act as mediators of inflammatory hyperalgesia (46, 47). NGF and BDNF levels are known to be elevated in both inflamed tissues and neurones innervating sites of inflammation (48–50) and they have been shown to induce synthesis of tachykinins such as SP within noiciceptive sensory neurones (48–53). NGF also increases nerve conductance and sensitivity (54). After allergen challenge of the airways of individuals with asthma, NGF induces phenotypic transformation of non–tachykinin-containing neurones into tachykinin-containing nociceptors (48). In addition, NGF and BDNF specifically cause increased capsaicin sensitivity in sensory neurones (46, 48). In vitro BDNF but not NGF directly regulates capsaicin sensitivity in vagal sensory afferents (55), whereas NGF does so primarily in dorsal root ganglia (56). However, NGF stimulates BDNF gene transcription in sensory nerves in response to tissue inflammation (57), thereby suggesting an indirect effect on capsaicin sensitivity in vivo. Neurotrophins are therefore likely candidates to mediate the respiratory tract neural hypersensitivity we have observed in IPF both directly and via increased tachykinin synthesis. It is also noteworthy that increased levels of SP have previously been measured in bronchoalveolar lavage fluid in patients with IPF (58) and that SP is a key mediator of neurogenic inflammation, which is characterized by microvascular leakage (59). It is not clear from this study whether the observed increase in sputum neurotrophin levels represents increased production in the lungs or increased vascular permeability. However, our demonstration of higher levels of neurotrophins in sputum of patients with IPF indicates that these mediators are found in a location where they could influence the reactivity, differentiation, and proliferation of sensory nerves thereby enhancing the cough reflex. It is interesting to note that intense NGF-immunoreactivity within the bronchial epithelium and submucosa has recently been demonstrated in individuals with asthma (60). Higher neutrophil counts in bronchoalveolar lavage fluid are known to be related to increased disease severity detected on computed tomography scanning (61), and it is believed that neutrophils originate from the cystic spaces associated with pulmonary fibrosis. Therefore, one possible explanation for our findings is that cells and mediators generated peripherally at these sites pass proximally on the mucocilary escalator to exert effects on the epithelium and sensory afferents in larger airways. Alternatively, our findings may represent direct epithelial infiltration by neutrophils more centrally. There are several possible mechanisms that may explain the pathogenesis of cough in IPF. Increased proximal airway deposition of capsaicin seems unlikely given the previous study by Doherty and coworkers (3). Furthermore, in a study using radiolabeled aerosol particles a greater cough response to inhaled capsaicin was observed when small (3.5 m mass mean diameter) particles were used compared with large (5.5 m mass mean diameter) particles, resulting in more peripheral airways deposition (62). The observation that cough reflex sensitivity to capsaicin is enhanced compared with control subjects suggests functional upregulation of sensory fibers within the respiratory tract. In this context, it is noteworthy that a significant number of our patients with IPF coughed in direct response to inhalation of SP. This phenomenon has been recognized in patients with upper respiratory tract infections and asthma, both conditions in which disruption of the respiratory epithelium facilitates access to epithelial sensory afferents. Furthermore, epithelial disruption causes reduced levels of neutral endopeptidase and angiotensinconverting enzyme, which rapidly metabolize SP and bradykinin. Therefore, this process may enhance the effect of these mediators on sensory nerves. IPF is characteristically a disease affecting the interstitium with epithelial disruption, inflammatory cell infiltration, and interstitial edema most evident in the alveoli. However, our findings of a neutrophilic infiltrate and evidence for microvascular leakage within induced sputa of patients with IPF raises the possibility that abnormalities within the proximal bronchial epithelium may also occur. In conclusion, this study confirms enhanced cough reflex sensitivity in patients with IPF and demonstrates that most patients have a direct cough response to SP. The increased response to capsaicin, which is c-fiber–specific, supports the hypothesis that there is functional upregulation of respiratory tract sensory nerves in IPF. The direct cough response to SP in some patients, the abrogation of this effect by steroid therapy, and the presence of neurotrophins in airway epithelial lining fluid support the notion that an inflammatory process can affect more proximal Hope-Gill, Hilldrup, Davies, et al.: Cough in IPF airways. The demonstration that cough in IPF is amenable to therapeutic intervention is encouraging and should promote further investigation into this phenomenon. 1001 23. Conflict of Interest Statement : B.D.M.H.-G. has no declared conflict of interest; S.H. has no declared conflict of interest; C.D. has no declared conflict of interest; R.P.N. has no declared conflict of interest; N.K.H. has no declared conflict of interest. 24. References 25. 1. Turner-Warwick M, Burrows B, Johnson A. Cryptogenic fibrosing alveolitis: clinical features and their influence on survival. Thorax 1980;35: 171–180. 2. Crystal RG, Fulmer JD, Roberts WC, Moss ML, Line BR, Reynolds HY. Idiopathic pulmonary fibrosis: clinical, histological, radiographic, physiological, scintigraphic, cytological and biochemical aspects. Ann Intern Med 1976;85:769–788. 3. Doherty MJ, Mister R, Pearson MG, Calverley PMA. Capsaicin induced cough in cryptogenic fibrosing alveolitis. Thorax 2000;55:1028–1032. 4. Widdicombe JG. Neurophysiology of the cough reflex. Eur Respir J 1995; 8:1193–1202. 5. Fox AJ. Modulation of cough and airway sensory nerves. Pulm Pharmacol 1996;9:335–342. 6. Martling CR, Saria A, Fischer JA, Hokfelt T, Lundberg JM. Calcitonin gene-related peptide and the lung: neuronal coexistence with substance P, release by capsaicin and vasodilatory effect. Regul Pept 1988;20: 125–139. 7. Lucchini RE, Facchini F, Turato G, Saetta M, Caramori G, Ciaccia A, Maestrelli P, Springall DR, Polak JM, Fabbri L, et al. Increased VIPpositive nerve fibres in the mucous glands of subjects with chronic bronchitis. Am J Respir Crit Care Med 1997;156:1963–1968. 8. Kroll F, Karlsson J-A, Lundberg JM, Persson CGA. Capsaicin-induced bronchoconstriction and neuropeptide release in guinea-pig perfused lungs. J Appl Physiol 1990;68:1679–1687. 9. Ventresca PG, Nichol GM, Barnes PJ, Chung KF. Inhaled furosemide inhibits cough induced by low chloride content solutions but not by capsaicin. Am Rev Respir Dis 1990;142:143–146. 10. Choudry NB, Fuller RW, Pride NB. Sensitivity of the human cough reflex: effect of inflammatory mediators prostaglandin E2, bradykinin and histamine. Am Rev Respir Dis 1989;140:137–141. 11. Fox AJ, Barnes PJ, Urban L, Dray A. An in-vitro study of the properties of single vagal afferents innervating guinea-pig airways. J Physiol 1993; 469:21–35. 12. Fujimura M, Kasahara K, Kamio Y, Naruse M, Hashimoto T, Matsuda T. Female gender as a determinant of cough threshold to inhaled capsaicin. Eur Respir J 1996;9:1624–1626. 13. Dicpinigaitis PV, Rauf K. The influence of gender on cough reflex sensitivity. Chest 1998;113:1319–1321. 14. Schuligoi R, Peskar BA, Donnerer J, Amann R. Bradykinin-evoked sensitisation of neuropeptide release from afferent neurones in the guinea-pig lung. Br J Pharmacol 1998;125:388–392. 15. Emanueli C, Grady EF, Madeddu P, Figini M, Bunnett NW, Parisi D, Regoli D, Geppetti P. Acute ACE inhibition causes plasma extravasation in mice that is mediated by bradykinin and substance P. Hypertension 1998;31:1299–1304. 16. Harrison NK, Dawes KE, Kwon OJ, Barnes PJ, Laurent GJ, Chung KF. Effects of neuropeptides on human lung fibroblast proliferation and chemotaxis in-vitro. Am J Physiol 1995;268:L278–L283. 17. O’Connell F, Springall DR, Moradoghli-Haftvani A, Krausz T, Price D, Fuller RW, Polak JM, Pride NB. Abnormal intraepithelial airway nerves in persistent unexplained cough. Am J Respir Crit Care Med 1995;152:2068–2075. 18. Ollerenshaw SL, Jarvis D, Sullivan CE, Woolcock AJ. Substance P immunoreactive nerves in airways from asthmatics and non-asthmatics. Eur Respir J 1991;4:673–682. 19. Braun A, Lommatzsch M, Lewin GR, Virchow JC, Renz H. Neurotrophins: a link between airway inflammation and airway smooth muscle contractility in asthma? Int Arch Allergy Immunol 1999;118:163–165. 20. Undem BJ, Hunter DD, Liu M, Haak-Frendscho M, Oakragly A, Fischer A. Allergen-induced sensory neuroplasticity in airways. Int Arch Allergy Immunol 1999;118:150–153. 21. Hope-Gill BDM, Hilldrup S, Harrison NK. An investigation into the pathogenesis of cough in patients with cryptogenic fibrosing alveolitis [abstract]. Am J Respir Crit Care Med 2001;163:A706. 22. Hope-Gill BDM, Hilldrup S, Harrison NK. Evidence for respiratory 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. tract c-fibre upregulation in cryptogenic fibrosing alveolitis [abstract]. Thorax 2001;56:S134. Hope-Gill BDM, Hilldrup S, Dawson A, Harrison NK. Induced sputum neutrophilia and raised neurotrophins in patients with cryptogenic fibrosing alveolitis [abstract]. Eur Respir J 2002;20:S1120. Hope-Gill BDM, Newton RP, Harrison NK. Elevated levels of nerve growth factor and brain-derived neurotrophic factor within the central airways of patients with cryptogenic fibrosing alveolitis [abstract]. Am J Respir Crit Care Med 2003;176:A982. American Thoracic Society. American Thoracic Society/European Respiratory Society multidisciplinary consensus classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med 2002;165: 277–304. Sterk PJ, Fabbri LM, Quanjer PhH, Cockcroft DW, O’Byrne PM, Anderson SD, Juniper EF, Malo JL. Airway responsiveness: standardised challenge testing with pharmacological, physical and sensitising stimuli in adults. Eur Respir J Suppl 1993;16:53–83. Quanjer PhH, ed. Standardisation of lung function tests, 1993. Update of Report of Working Party for the European community for Steel and Coal. Eur Respir J Suppl 1993;16:5–52. Pavord ID, Pizzichini MMM, Pizzichini E, Hargreave FE. The use of induced sputum to investigate airway inflammation. Thorax 1997;52: 498–501. Pizzichini E, Pizzichini MMM, Efthimiadis A, Evans S, Morris MM, Squillace D, Gleich GJ, Dolovich J, Hargreave FE. Indices of airway inflammation in induced sputum: reproducibility and validity of cell fluidphase measurements. Am J Respir Crit Care Med 1996;154:308–317. Altman DG. Practical statistics for medical research. London: Chapman & Hall; 1997. Turner-Warwick M, Haslam PL. The value of serial bronchoalveolar lavages in assessing the clinical progress of patients with cryptogenic fibrosing alveolitis. Am Rev Respir Dis 1987;135:26–34. Lynch JP III, Standiford TJ, Rolfe MW, Kunkel SL, Strieter RM. Neutrophilic alveolitis in idiopathic pulmonary fibrosis: the role of interleukin-8. Am Rev Respir Dis 1992;145:1433–1439. Alexis NE, Hu SC, Zeman K, Alter T, Bennett WD. Induced sputum derives from the central airways: confirmation using a radiolabelled aerosol bolus delivery technique. Am J Respir Crit Care Med 2001;164: 1964–1970. Midgren B, Hansson L, Karlsson JA, Simonsson BG, Persson CG. Capsaicin-induced cough in humans. Am Rev Respir Dis 1992;146: 347–351. Lalloo UG, Lim S, Du Bois RM, Barnes PJ, Chung KF. Increased sensitivity of the cough reflex in progressive systemic sclerosis patients with interstitial lung disease. Eur Respir J 1998;11:702–705. Palombini BC, Villanova CA, Aranj E, Gastal OL, Alt DC, Stolz DP, Palombini CO. A pathogenic triad in chronic cough: asthma, postnasal drip syndrome, and gastroesophageal reflux. Chest 1999;116:279–284. Irwin RS, Madison JM, Fraire AE. The cough reflex and its relation to gastroesophageal reflux. Am J Med 2000;108(Suppl 4a):73S–78S. Ferrari M, Olivieri M, Sembenini C, Benini L, Zuccali V, Bardelli E, Bovo P, Cavallini G, Vantini I, Lo Cascio V. Tussive effect of capsaicin in patients with gastroesophageal reflux without cough. Am J Respir Crit Care Med 1995;151:557–561. Tobin RW, Pope CE II, Pellefrini CA, Emond MJ, Sillery J, Raghu G. Increased prevalence of gastroesophageal reflux in patients with idiopathic pulmonary fibrosis. Am J Respir Crit Care Med 1998;158: 1804–1808. Akesson A, Akesson B, Gustafson T, Wollheim F. Gastrointestinal function in patients with progressive systemic sclerosis. Clin Rheumatol 1985;4:441–448. Ours TM, Kavuru MS, Schilz RJ, Richter JE. A prospective evaluation of esophageal testing and a double-blind, randomised study of Omeprazole in a diagnostic and therapeutic algorithm for chronic cough. Am J Gastroenterol 1999;94:3131–3138. Kiljander TO, Salomaa ER, Hietanen EK, Terho EO. Chronic cough and gastro-oesophageal reflux: a double-blind placebo-controlled study with omeprazole. Eur Respir J 2000;16:633–638. Poe RH, Kallay MC. Chronic cough and gastroesophageal reflux disease: experience with specific therapy for diagnosis and treatment. Chest 2003;123:679–684. 1002 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 168 2003 44. McGarvey LPA, Heaney LG, Lawson JT, Johnston BT, Scally CM, Ennis M, Shepherd DRT, Macmahon J. Evaluation and outcome of patients with chronic non-productive cough using a comprehensive diagnostic protocol. Thorax 1998;53:738–743. 45. Lewin GR, Barde Y-A. Physiology of the neurotrophins. Annu Rev Neurosci 1996;19:289–317. 46. Koltzenburg M. The changing sensitivity in the life of the nociceptor. Pain 1999;(Suppl 6):S93–S102. 47. Shu X, Mendell LM. Nerve growth factor acutely sensitises the response of adult rat sensory neurones to capsaicin. Neurosci Lett 1999;274: 159–162. 48. Donnerer J, Schuligoi R, Stein C. Increased content and transport of substance P and calcitonin gene-related peptide in sensory nerves innervating inflamed tissue: evidence for a regulatory function of nerve growth factor in-vivo. Neuroscience 1992;49:693–698. 49. Lindsay RM, Harmar AJ. Nerve growth factor regulates expression of neuropeptide genes in adult sensory neurons. Nature 1989;337:362–363. 50. Braun A, Lommatzsch M, Mannsfeldt A, Neuhaus-Steinmetz U, Fischer A, Schnoy N, Lewin G, Renz H. Cellular sources of enhanced brainderived neurotrophic factor production in a mouse model of allergic inflammation. Am J Respir Cell Mol Biol 1999;21:537–546. 51. Maclean DB, Lewis SF, Wheeler FB. Substance P content in cultured neonatal rat vagal sensory neurones: the effect of nerve growth factor. Brain Res 1988;457:53–62. 52. Woolf CJ, Safieh-Garabedian B, Ma Q-P, Crilly P, Winter J. Nerve growth factor contributes to the generation of inflammatory sensory hypersensitivity. Neuroscience 1994;62:327–331. 53. Yao L, Zhang D, Bernd P. Differential regulation of substance P by all members of the nerve growth factor family of neurotrophins in avian 54. 55. 56. 57. 58. 59. 60. 61. 62. dorsal root ganglia throughout development. Neuroscience 1997;79: 1197–1206. Undem BJ, Hunter DD, Liu M, Haak-Frendscho M, Oakragly A, Fischer A. Allergen-induced sensory neuroplasticity in airways. Int Arch Allergy Immunol 1999;118:150–153. Winter J. Brain derived neurotrophic factor, but not nerve growth factor, regulates capsaicin sensitivity of rat vagal ganglion neurones. Neurosci Lett 1998;241:21–24. Winter J, Forbes CA, Sternberg J, Lindsay RM. Nerve growth factor (NGF) regulates adult rat cultured dorsal root ganglion neuron responses to capsaicin. Neuron 1988;1:973–981. Cho H-J, Kim S-Y, Park M-J, Kim D-S, Kim J-K, Chu M-Y. Expression of mRNA for brain-derived neurotrophic factor in the dorsal root ganglion following peripheral inflammation. Brain Res 1997;749:358–362. Takeyama M, Nagai S, Mori K, Ikawa K, Satake N, Izumi T. Substance P-like immunoreactive substance in bronchoalveolar lavage fluids from patients with idiopathic pulmonary fibrosis and pulmonary sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis 1996;13:33–37. Barnes PJ. Neurogenic inflammation in airways. Int Arch Allergy Appl Immunol 1991;94:303–309. Hogland CO, de Blay F, Oster J-P, Duvernelle C, Kassel O, Pauli G, Frossard N. Nerve growth factor levels and localisation in human asthmatic bronchi. Eur Respir J 2002;20:1110–1116. Wells AU, Hansell DM, Haslam PL, Rubens NM, Cailes J, Black CM, Du Bois RM. Bronchoalveolar lavage cellularity: lone cryptogenic fibrosing alveolitis compared with the fibrosing alveolitis of systemic sclerosis. Am J Respir Crit Care Med 1998;157:1474–1482. Hansson L, Wollmer P, Dahlback M, Karlsson JA. Regional sensitivity of human airways to capsaicin-induced cough. Am Rev Respir Dis 1992; 145:1191–1195.