AUGUST 2013
Vol 4, No 3
A Supplement to
Improving Outcomes in the
Management of Chemotherapy-Induced
Nausea and Vomiting:
The Pharmacist’s Role
CONTRIBUTING FACULTY
Joanna Schwartz,
PharmD, BCOP
Assistant Professor
Department of Pharmacy Practice
Albany College of Pharmacy
and Health Sciences
Vermont Campus
Colchester, VT
James J. Natale,
PharmD, BCOP
Manager, Outpatient Oncology
Pharmacy Services
UPMC Cancer Center
a partner with University of
Pittsburgh Cancer Institute
Pittsburgh, PA
Supported by an educational grant
from Eisai, Inc.
This activity is jointly sponsored by Medical Learning Institute Inc and Center of Excellence Media, LLC.
Evolving Treatment Paradigms for CINV
Sponsors
This activity is jointly sponsored by Medical Learning Institute Inc and
Center of Excellence Media, LLC.
Commercial Support Acknowledgment
This activity is supported by an educational grant from Eisai, Inc.
Target Audience
This program was developed for health system pharmacists and oncology
pharmacists involved in the management of chemotherapy-induced nausea
and vomiting (CINV).
Registered Pharmacy Designation
The Medical Learning Institute Inc is accredited by the Accreditation
Council for Pharmacy Education as a provider of continuing pharmacy
education. Completion of this knowledge-based activity provides for 1.0
contact hour (0.1 CEU) of continuing pharmacy education credit.
The Universal Activity Number for this activity is 0468-9999-13-010-H01-P.
Learning Objectives
Upon completion of this activity, the participant will be able to:
•Discuss recent advances and emerging therapies in the treatment of
patients with CINV
•Evaluate key recommendations from updated clinical practice guidelines
for the management of CINV, including those established by ASCO,
NCCN, MASCC, and ONS
•Formulate effective treatment strategies for improving outcomes in
patients with CINV
Disclosures
Before the activity, all faculty and anyone who is in a position to have control over the content of this activity and their spouse/life partner will disclose
the existence of any financial interest and/or relationship(s) they might
have with any commercial interest producing healthcare goods/services to
be discussed during their presentation(s): honoraria, expenses, grants, consulting roles, speakers bureau membership, stock ownership, or other special
relationships. Presenters will inform participants of any off-label discussions.
All identified conflicts of interest are thoroughly vetted by Medical Learning
Institute Inc for fair balance, scientific objectivity of studies mentioned in
the materials or used as the basis for content, and appropriateness of patient
care recommendations.
The associates of Medical Learning Institute Inc, the accredited provider for
this activity, and Center of Excellence Media, LLC, do not have any financial relationships or relationships to products or devices with any commercial
interest related to the content of this CPE activity for any amount during
the past 12 months.
Planners’ and Managers’ Disclosures
Dana Delibovi, Medical Writer, has nothing to disclose. She does intend
to discuss either non–FDA-approved or investigational use for the following
products/devices: AFP530; NEPA, netupitant.
Teresa Haile, RPh, MBA, MLI Reviewer, has nothing to disclose.
Faculty Disclosures
James J. Natale, PharmD, BCOP, is on the speakers’ bureau for Eisai and
Merck. He does intend to discuss either non–FDA-approved or investigational use for the following products/devices: NEPA and rolapitant.
Joanna Schwartz, PharmD, BCOP, has nothing to disclose. She does
intend to discuss either non–FDA-approved or investigational use for the
following products/devices: aprepitant, published studies for challenging
cases in CINV.
Disclaimer
The information provided in this CPE activity is for continuing education
purposes only and is not meant to substitute for the independent medical
judgment of a healthcare provider relative to diagnostic and treatment
options of a specific patient’s medical condition. Recommendations for the
use of particular therapeutic agents are based on the best available scientific
evidence and current clinical guidelines. No bias toward or promotion for
any agent discussed in this program should be inferred.
Instructions for Credit
There is no fee for this activity. To receive credit after reading this CPE
activity in its entirety, participants must complete the pretest, posttest, and
evaluation. The pretest, posttest, and evaluation can be completed online
at www.mlicme.org/P13020.html. Upon completion of the evaluation
and scoring a 70% or better on the posttest, you will immediately receive
your certificate online. If you do not achieve a score of 70% or better on
the posttest, you will be asked to take it again. Please retain a copy of the
Certificate for your records. For questions regarding the accreditation of this
activity, please contact Medical Learning Institute Inc at (609) 333-1693 or
cgusack@mlicme.org. For pharmacists, Medical Learning Institute Inc will
report your participation in this educational activity to the NABP only if
you provide your NABP e-Profile number and date of birth. For more information regarding this process or to get your NABP e-Profile number: go to
www.mycpemonitor.net.
Estimated time to complete activity: 1 hour
Date of initial release: August 16, 2013
Valid for CPE credit through: August 16, 2014
The Oncology Pharmacist®, ISSN 1944-9607 (print); ISSN 1944-9593 (online) is published 8 times a year by Green Hill Healthcare Communications, LLC, 1249 South River Road,
Suite 202A, Cranbury, NJ 08512. Telephone: 732.656.7935. Fax: 732.656.7938. Copyright ©2013 by Green Hill Healthcare Communications LLC. All rights reserved. The Oncology
Pharmacist® logo is a registered trademark of Green Hill Healthcare Com­munications, LLC. No part of this publication may be reproduced or transmitted in any form or by any means
now or hereafter known, electronic or mechanical, including photocopy, recording, or any informational storage and retrieval system, without written permission from the Publisher.
Printed in the United States of America.
EDITORIAL CORRESPONDENCE should be addressed to EDITORIAL DIRECTOR, The Oncology Pharmacist®, 1249 South River Road, Suite 202A, Cranbury, NJ 08512.
E-mail: editorial@greenhillhc.com. YEARLY SUBSCRIPTION RATES: United States and possessions: individuals, $105.00; institutions, $135.00; single issues, $17.00. Orders will
be billed at individual rate until proof of status is confirmed. Prices are subject to change without notice. Correspondence regarding permission to reprint all or part of any article
published in this journal should be addressed to REPRINT PERMISSIONS DEPARTMENT, Green Hill Healthcare Commun­i­cations, LLC, 1249 South River Road, Suite 202A,
Cranbury, NJ 08512. The ideas and opinions expressed in The Oncology Pharmacist® do not necessarily reflect those of the Editorial Board, the Editorial Director, or the Publisher.
Publication of an advertisement or other product mention in The Oncology Pharmacist® should not be construed as an endorsement of the product or the manufacturer’s claims. Readers
are encouraged to contact the manufacturer with questions about the features or limitations of the products mentioned. Neither the Editorial Board nor the Publisher assumes any
responsibility for any injury and/or damage to persons or property arising out of or related to any use of the material contained in this periodical. The reader is advised to check the
appropriate medical literature and the product information currently provided by the manufacturer of each drug to be administered to verify the dosage, the method and duration of
administration, or contraindications. It is the responsibility of the treating physician or other healthcare professional, relying on independent experience and knowledge of the patient,
to determine drug dosages and the best treatment for the patient. Every effort has been made to check generic and trade names, and to verify dosages. The ultimate responsibility,
however, lies with the prescribing physician. Please convey any errors to the Editorial Director. BPA Worldwide membership applied for April 2011.
2
August 2013
Supplement
Evolving Treatment Paradigms for CINV
PUBLISHING STAFF
Senior Vice President, Sales & Marketing
Nicholas Englezos
nick@engagehc.com
Vice President/Director of Sales & Marketing
Joe Chanley
joe@greenhillhc.com
Group Director, Sales & Marketing
John W. Hennessy
john@greenhillhc.com
Publisher
Cristopher Pires
cris@engagehc.com
Table of Contents
4
Evolving Treatment Paradigms for
Chemotherapy-Induced Nausea and Vomiting
Dana Delibovi, Medical Writer
12
Managing Nausea and Vomiting in a Patient Receiving
Multiday Chemotherapy
Joanna Schwartz, PharmD, BCOP
Editorial Director
Kristin Siyahian
kristin@greenhillhc.com
Managing Editor
Kristen Olafson
kristen@greenhillhc.com
Copy Editors
Mollie Friedman
Peggy Roeske
Editorial Assistant
Jennifer Brandt
Production Manager
Stephanie Laudien
The Lynx Group
President/CEO
Brian Tyburski
Chief Operating Officer
Pam Rattananont Ferris
Vice President of Finance
Andrea Kelly
Director, Human Resources
Blanche Marchitto
15
Update on Emerging Agents in CINV: Are Practice
Changes Ahead?
James J. Natale, PharmD, BCOP
Associate Editorial Director, Projects Division
Terri Moore
Director, Quality Control
Barbara Marino
Quality Control Assistant
Theresa Salerno
Director, Production & Manufacturing
Alaina Pede
Director, Creative & Design
Robyn Jacobs
Creative & Design Assistant
Lora LaRocca
Director, Digital Media
Anthony Romano
Web Content Managers
David Maldonado
Anthony Travean
Digital Programmer
Michael Amundsen
Senior Project Manager
Andrea Boylston
Project Coordinators
Deanna Martinez
Jackie Luma
Executive Administrator
Rachael Baranoski
Office Coordinator
Robert Sorensen
1249 South River Road - Ste 202A
Cranbury, NJ 08512
phone: 732-656-7935
fax: 732-656-7938
COE55
August 2013
3
Evolving Treatment Paradigms for CINV
Evolving Treatment Paradigms
for Chemotherapy-Induced Nausea
and Vomiting
Dana Delibovi, Medical Writer
D
espite major advancements in the treatment and
supportive care of patients with cancer, chemotherapy-induced nausea and vomiting (CINV)
continues to burden the healthcare system, compromise
patients’ quality of life, and reduce adherence to beneficial anticancer therapies.1,2 For many patients, poorly
controlled CINV also leads to metabolic imbalances,
nutrient depletion, anorexia, and decline in performance
status and mental status.1,2
Incidence rates of acute and delayed CINV are greater
than 50%, even when antiemetic prophylaxis is used.3-5
More than 90% of patients who do not receive prophylaxis will experience vomiting after receiving such highly
emetogenic chemotherapies as cisplatin, with 30% still
experiencing vomiting even when antiemetic prophylaxis is administered prior to treatment.1
Costs associated with CINV are substantial. In a database of 19,139 patients who received highly or moderately emetogenic chemotherapy and at least 1 antiemetic
agent, 13.8% (approximately 2600 patients) reported a
CINV-associated hospital visit following their chemotherapy.6 Inpatient visits (ie, hospital admissions) accounted for 64% of these visits, with a mean cost of
$7448 per visit. Outpatient visits represented 26% of
these visits, with a mean cost of $1494 per visit; 10% of
the visits were to the emergency department, with a mean
cost of $918 each.6 Another database analysis reported
that despite the use of antiemetic therapy with serotonin
(5-HT3) receptor antagonists in approximately 87% of
patients, 27.9% experienced uncontrolled CINV, resulting in monthly direct medical costs that were $1383
higher than for those with controlled CINV (P<.0001).7
The ongoing burden of CINV has motivated a vigorous search for improved antiemetic therapy, with novel
agents and combination regimens changing the paradigm
of care for patients undergoing chemotherapy. When
used prophylactically, these interventions have shown
promise in enhancing control of CINV. Moreover, evidence-based clinical practice guidelines1,8-10 are routinely
updated, which helps clinicians integrate these novel
treatments into clinical practice. For pharmacy healthcare professionals, who have always played a pivotal role
in emesis care, the evolving paradigm is an exciting development. To make optimal use of novel antiemetic
4
August 2013
Supplement
agents, however, pharmacists must stay up to date on the
latest clinical data and evidence-based recommendations.
Overview of CINV
The mechanism of emesis is not fully understood, but
current models suggest mediation by various neurotransmitters in the gastrointestinal (GI) tract and central
nervous system (CNS).11,12 These neurotransmitters, including dopamine, serotonin, and substance P, are the
targets of current and emerging pharmacotherapies for
CINV (Table 1).9,11,13 Vomiting is triggered by specific
afferent nervous inputs to the vomiting center located in
the brainstem (medulla oblongata; see Figure 1).11-13
Chemotherapeutic agents appear to cause emesis through
activation of neurotransmitter receptors in the vomiting
center, in the chemoreceptor trigger zone (CTZ)—another region of the medulla that receives inputs about
drugs or toxins in the blood and communicates these inputs to the vomiting center—and in the GI tract.11,13 In
CINV, nausea can be characterized as a prodromal phase
of vomiting, although significant nausea may occur without any vomiting.11
Some individuals have an elevated risk for CINV.
Major patient-specific risk factors include female gender,
younger age (<50 years), low regular alcohol use (<1
ounce per day), and history of prior CINV.11 Other, less
Table 1 Neurotransmitter Targeting of Antiemetic
Agents9,11,13
Target Receptor
Class (Agents)
Dopamine receptor Dopamine antagonists
•Phenothiazines (olanzapine,
prochlorperazine)
•Metoclopramide
•Butyrophenones (domperidone)
Serotonin (5-HT3)
receptor
5-HT3 serotonin receptor
antagonists (dolasetron,
granisetron, ondansetron,
palonosetron, tropisetron)
Substance
P-neurokinin 1
(NK1) receptor
NK1 receptor antagonists
(aprepitant, fosaprepitant)
Evolving Treatment Paradigms for CINV
Figure 1 Pathogenesis of CINV.11-13
Release of
neuroactive agents
CNS indicates central nervous system.
Reprinted with permission from Navari RM. Pathogenesis-based
treatment of chemotherapy-induced nausea and vomiting—two
new agents. J Support Oncol. 2003;1:89-103. Copyright © 2003
BioLink Communications.
significant risk factors are history of emesis during pregnancy (morning sickness) and history of motion sickness.11 Risk-prediction models are in development, designed to provide pharmacists and other healthcare
professionals with tools to help identify those patients at
risk for CINV.14 Of course, one key risk factor for emesis
that is not specific to the individual patient is the type of
anticancer treatment being used and the dose. Chemo­
therapeutic agents are ranked from highly emetogenic
(eg, cisplatin, dacarbazine) to minimally emetogenic (eg,
vincristine).9,11 It is interesting to note, however, that a
recent retrospective analysis of electronic medical records showed that CINV risk was increased across the
board for patients with a history of CINV, even when
they were treated with low–emetic-risk chemotherapy.15 These results serve as a reminder that CINV is a
complex process, in which patient profile and drug/
dosage interact dynamically.
CINV has been classified into 5 types: acute, delayed,
anticipatory, breakthrough, and refractory.11 Acute CINV
occurs 0 to 24 hours postchemotherapy and delayed
CINV occurs 24 hours or longer after chemotherapy.9,11
Patients who have experienced prior CINV may develop
a conditioned response to the memory of emesis, known
as anticipatory CINV, which occurs before an upcoming
cycle of chemotherapy.9,11 Breakthrough CINV occurs
within 5 days after the use of antiemetic prophylaxis and
requires rescue antiemetic treatment.11 Refractory CINV
refers to the failure to respond adequately to antiemetic
prophylaxis and/or rescue.9,11
Pharmacologic Management of CINV: Focus on Novel
and Emerging Agents
As discussed earlier, antiemetic agents target neurotransmitters involved in the process of emesis. This is
true for older agents, such as metoclopramide and
prochlorperazine, as well as for the newer antiemetic drug
classes, including 5-HT3 receptor antagonists and the
tachykinin neurokinin 1 (NK1) receptor antagonists.11 In
addition, corticosteroids such as dexamethasone have
been used traditionally to control emesis and remain an
important component of CINV management.11
5-HT3 receptor antagonists
The use of this class of antiemetics, introduced in the
1990s, has dramatically improved patient outcomes.13
5-HT3 receptor antagonists developed for the prevention
and management of CINV include the first-generation
agents ondansetron, granisetron, dolasetron, and tropisetron (not available in the United States), as well as the
second-generation 5-HT3 receptor antagonist palonosetron.11,13 5-HT3 receptor antagonists act at the specific
subtype of serotonin receptor believed to be the most
critical in CINV.13
5-HT3 receptors are located centrally in areas of the
medulla in and around the CTZ, as well as in peripheral
nerves of the GI tract that supply afferent emetic impulses.13 Serotonin binding to the 5-HT3 receptor mediates
emesis, so receptor blockade helps to suppress CINV.16
These results serve as a reminder that
CINV is a complex process, in which patient
profile and drug/dosage interact dynamically.
The use of first-generation 5-HT3 receptor antagonists
is supported by robust clinical evidence from multiple
randomized trials and meta-analyses of these trials, which
demonstrate good antiemetic response across the class.13,17-19
However, clinicians need to carefully weigh the therapeutic benefits of these agents against the risks. For example,
in 2010, the US Food and Drug Admini­stration (FDA)
announced that intravenous (IV) dolasetron should no
longer be used to prevent CINV, as this formulation was
associated with an increased risk for cardiac arrhythmias.20 The oral form of dolasetron, however, is still a
recommended treatment option for CINV prophylaxis.1
The following year, the FDA issued a drug safety warning
for ondansetron, stating that use of this agent may increase the risk for development of abnormal changes in
the electrical activity of the heart. It is therefore recommended that ondansetron not be used in patients with
congenital long QT syndrome.21
August 2013
5
Evolving Treatment Paradigms for CINV
Palonosetron differs from these earlier 5-HT3 receptor
antagonists in its stronger binding affinity for the target
receptor and a longer half-life (approximately 40 hours).13
Three pivotal, randomized, noninferiority trials initially
demonstrated that palonosetron provides efficacy at least
comparable to or better than that of first-generation
5-HT3 receptor antagonists.22-24 In one of these trials, the
investigators observed that a single IV dose of palonosetron was significantly superior to a single IV dose of ondansetron in achieving a complete response (CR) in both
Current evidence-based consensus is that
first-generation 5-HT3 receptor antagonists
are effective in acute CINV but less effective
in delayed CINV.
acute and delayed CINV 30 minutes prior to initiation of
moderately emetogenic chemotherapy.22 This was an interesting finding, since first-generation 5-HT3 receptor
antagonists have not been shown to be as effective in
delayed CINV as in acute CINV. Current evidence-based
consensus is that first-generation 5-HT3 receptor antagonists are effective in acute CINV but less effective in delayed CINV, but palonosetron administered via the IV
route appears to be effective in both the acute and the
delayed phases of CINV.1
These trials have been followed up by additional studies demonstrating the clinical efficacy of palonosetron in
highly specific settings, including in combination with
dexamethasone. Aogi and colleagues reported sustained
rates of antiemetic response to palonosetron in patients
receiving repeated cycles of highly emetogenic, cisplatin-based chemotherapy or anthracycline-cyclophosphamide combination chemotherapy.25 Saito and colleagues
compared palonosetron plus dexamethasone with granisetron plus dexamethasone and found the 2 regimens to be
comparable in efficacy in patients experiencing acute
CINV.26 Palonosetron plus dexamethasone was superior
to granisetron plus dexamethasone in the delayed phase,
however, with 56.8% versus 44.5% of patients, respectively, achieving a CR (P<.0001). In a recent retrospective, claims-based data analysis by Hatoum and colleagues, the use of palonosetron was associated with a
reduced risk for CINV-related hospitalizations compared
with the use of other 5-HT3 regimens.27
In several retrospective analyses, palonosetron has
been associated with lower CINV event rates in a hospital outpatient setting and a reduced risk for uncontrolled
CINV compared with other 5-HT3 regimens.28-30 One of
these trials, conducted by Feinberg and colleagues, evaluated antiemetic regimens in patients receiving multiday
6
August 2013
Supplement
chemotherapy29—a particularly challenging setting.9,10
The investigators reported that in cycles in which palonosetron was used, the risk for uncontrolled CINV events
was 63% lower than in cycles in which ondansetron was
used (P<.0001).29 In a trial by Schwartzberg and colleagues, patients receiving highly emetogenic chemotherapy were treated with palonosetron or another 5-HT3
receptor antagonist within triple therapy30—a regimen
that combines a 5-HT3 receptor antagonist with an NK1
receptor antagonist and dexamethasone, which is the
standard of antiemetic prophylaxis when highly emetogenic chemotherapy is used.1,8-10 This study demonstrated
that when used prior to the start of highly emetogenic
chemotherapy, palonosetron-based triple therapy may
reduce the risk for an uncontrolled CINV event compared with triple therapy based on first-generation 5-HT3
receptor antagonists.30
Classwide adverse events associated with the use of
5-HT3 receptor antagonists include headache, constipation, asthenia, somnolence, and diarrhea.31 Because of
the risk for cardiac toxicity discussed above, it is recommended that patients with other risk factors for cardiac
conduction problems (eg, congestive heart failure, cardiac disease, hypokalemia, and bradycardia) should undergo
routine electrocardiographic monitoring while receiving
5-HT3 receptor antagonist therapy.1
NK1 receptor antagonists
This class of novel antiemetic agents targets substance
P, an emesis-inducing neuropeptide found in the GI tract
and CNS.32 Since substance P exerts its emetic effect by
binding to the NK1 receptor, antagonism of this receptor
suppresses emesis.32
Classwide adverse events associated with
the use of 5-HT3 receptor antagonists
include headache, constipation, asthenia,
somnolence, and diarrhea.
Two NK1 receptor antagonists are approved by the
FDA: oral aprepitant and IV fosaprepitant, which is a
prodrug of aprepitant. Two pivotal phase 3 trials—in a
combined 1043 patients treated with highly emetogenic
chemotherapy—compared a regimen of aprepitant, ondansetron, and dexamethasone with a regimen of ondansetron and dexamethasone alone.33,34 In the study by
Warr and colleagues, significantly less nausea was reported in the aprepitant group over the study period, along
with better performance on functional assessment in the
domains of nausea and vomiting.33 Aprepitant-containing
triple therapy also improved prevention of delayed emesis
Evolving Treatment Paradigms for CINV
Investigational Agents and Adjunctive Therapies
An intriguing area of current research involves treatment with NEPA—an investigational, oral, fixed-dose
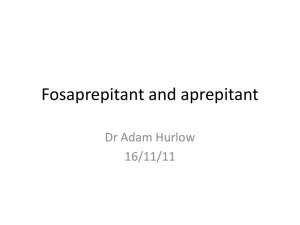
Figure 2 Complete response rates for triplet
therapy versus doublet therapy (N=1044).
66
Complete Response (%)
70
60
69
53
50
41
40
Women
Men
30
20
10
0
Control GroupAprepitant Group
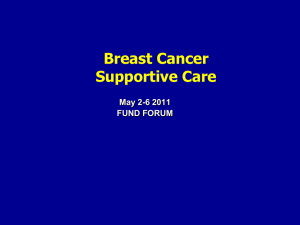
Figure 3 NEPA plus dexamethasone versus
palonosetron plus dexamethasone.
NEPA + dexamethasone (n=724)
90
88.4
Palonosetron + dexamethasone (n=725)
85.0
76.9
80
Complete Response (%)
by 16% among patients who did not experience acute eme­
sis and by 17% in those with acute emesis.33 The addition of
aprepitant to the regimen was also associated with fewer
breakthrough emesis and rescue events.33 A subgroup analysis of the pooled data by Hesketh and colleagues suggested
that triple therapy containing aprepitant in the antiemetic
regimen may overcome the negative prognostic impact of
female gender on CINV (Figure 2).34
At the 2013 American Society of Clinical Oncology
(ASCO) Annual Meeting, investigators reported updated results of a meta-analysis of 20 randomized clinical trials that compared standard antiemetic therapy
(dexamethasone plus 5-HT3 receptor inhibitors) versus
NK1 receptor antagonists plus standard therapy for
CINV prevention. Triplet therapy that included an
NK1 receptor antagonist was associated with improved
CR rates, from 56% to 72%, in both delayed and acute
CINV (P<.00001).35 Also presented at the meeting
were the results of a phase 3 clinical trial that compared a regimen of aprepitant, palonosetron, and dexamethasone with a regimen of aprepitant, granisetron,
and dexamethasone.36 Regarding the primary end
point—overall rate of CR—the regimens were numerically, but not significantly, different: 66% with aprepitant/palonosetron/dexamethasone versus 59% with
aprepitant/granisetron/dexamethasone (P=.0539). In
the acute CINV phase, the 2 regimens were associated
with equivalent CR rates (92%). In the delayed phase
of CINV, however, a significant difference in CR rates
was observed that favored the palonosetron regimen
(67%) over the granisetron regimen (59%; P=.0142).
This result is consistent with current opinion that NK1
receptor antagonists and palonosetron are of particular
benefit in patients who experience delayed CINV.1,32
Common adverse events associated with the use of
aprepitant include asthenia, fatigue, anorexia, and GI effects.37 Aprepitant is metabolized by the hepatic enzyme
pathway cytochrome P450 (CYP)3A4 and thus may interact with other agents that share this metabolic pathway, including corticosteroids; in triple therapy, dexamethasone dosing should be reduced by 50% with oral
administration and by 25% with IV administration.9,32
Aprepitant may also interact with other CYP3A4metabolized drugs, including such benzodiazepines as
lorazepam and alprazolam (used supportively in patients
who experience emesis) and some chemotherapeutic
agents.1,32 Aprepitant appears to reduce plasma concentrations of drugs metabolized via the CYP2C9 pathway,
including warfarin and oral contraceptives.32
69.5
70
74.3
66.6
60
50
40
30
20
10
0
Acute Emesis
(0-24 h)
Delayed EmesisOverall
(24-120 h)
(0-120 h)
All differences statistically significant; P≤.047.
NEPA indicates netupitant plus palonosetron in an oral fixed
combination.
combination of the novel NK1 receptor antagonist netupitant plus palonosetron. At the 2013 ASCO Annual
Meeting, investigators presented the results of 2 new trials
of NEPA as part of triple therapy. In a phase 3 study,
Aapros and colleagues compared NEPA with palonosetron alone for the prevention of CINV in patients receiving moderately emetogenic chemotherapy; all of the patients received dexamethasone as well.38 As shown in
Figure 3, use of NEPA was associated with higher rates of
CR versus palonosetron alone during both delayed and
acute CINV phases. NEPA also demonstrated superiority
over palonosetron alone with respect to the number of
patients with no emesis and no significant nausea.38
In a separate randomized trial of patients receiving
August 2013
7
Evolving Treatment Paradigms for CINV
highly emetogenic chemotherapy, Hesketh and colleagues reported that 3 different oral doses of NEPA
(netupitant 100 mg, 200 mg, or 300 mg plus palonosetron 0.5 mg) administered with dexamethasone resulted in significantly higher rates of CR compared with
palonosetron alone overall (acute plus delayed phases;
P=.018, P=.017, and P=.004, respectively) and in the
delayed phase (P=.018, P=.010, and P=.018, respectively).39 Treatment with netupitant 300 mg plus palonosetron 0.5 mg was also superior to palonosetron alone in
the acute CINV phase (P=.007).39
Pharmacy practice and decision-making in
antiemetic therapy can be facilitated by
clinical practice guidelines for CINV.
In addition to netupitant, casopitant is also emerging
as a promising NK1 receptor antagonist.11 Also in development is APF530—granisetron formulated to sustain
plasma levels for 5 days following a single subcutaneous
injection. However, application for FDA approval of
APF530 was rejected in 2013, based on the need for improvements in quality analytical test method and analysis
of clinical trial data; the manufacturer plans to address
these issues.40
Benzodiazepine tranquilizers (eg, lorazepam), cannabinoids, guided imagery, acupuncture, and a host of other
interventions are used along with antiemetic triple therapy, although clinical evidence in support of their use is
limited.3 Herbal supplementation with ginger has also
shown some promise, but current studies do not support
its use for CINV prevention.10,11
Clinical Practice Guidelines for CINV
Pharmacy practice and decision-making in antiemetic
therapy can be facilitated by clinical practice guidelines
for CINV. Current guidelines are issued by ASCO,9,10 the
National Comprehensive Cancer Network (NCCN),1
and the Multinational Association of Supportive Care
in Cancer/European Society for Medical Oncology
(MASCC/ESMO).8 In addition, the Oncology Nursing
Society has developed a “Putting Evidence Into Practice”
report on CINV.3
CINV prevention
Although guidelines vary in the details of recommendations for emesis control, all support the use of triple
therapy with a 5-HT3 receptor antagonist, an NK1 receptor antagonist, and dexamethasone for the prevention of
acute CINV in patients treated with highly emetogenic
chemotherapy.1,8-10 For delayed CINV prevention, the
8
August 2013
Supplement
NCCN and ASCO advocate triplet therapy when highly
emetogenic chemotherapy is used, whereas MASCC/
ESMO guidelines recommend doublet therapy with an
NK1 receptor antagonist and dexamethasone.1,8,10 Recom­
mendations differ more markedly among guidelines for
prevention of CINV following the use of moderately
emetogenic chemotherapy. Palonosetron is the preferred
5-HT3 receptor antagonist in both ASCO and NCCN
guidelines after patients receive moderately emetogenic
chemotherapy; the NCCN also prefers palonosetron for
highly emetogenic chemotherapy. Key antiemetic recommendations are summarized in Table 2.1,8-10
Recommended dosing strategies for the use of doublet
and triplet therapies are complex, and are not consistent
across the various published clinical practice guidelines.
Moreover, recommendations include additional supportive measures (eg, benzodiazepines and histamine-2 blockers or proton pump inhibitors). Therefore, it is essential
for pharmacists to learn the details of guidelines and for
facilities to develop institutionwide protocols based on a
thorough review of these recommendations.
Managing breakthrough/refractory CINV
Across all clinical practice guidelines, there is strong
consensus that prevention of emesis is far more effective
than attempting to treat emesis in the refractory/breakthrough settings.1,8-10 When emesis does occur, however,
a cornerstone of management is to administer an antiemetic agent not previously used.1,8,9 Another option for
rescue is to administer multiple agents by various routes—
for example, older dopamine-targeting agents, such as
metoclopramide—or alternative drugs, such as cannabinoids, may be needed.1,8,9
Recommendations differ more markedly
among guidelines for prevention of
CINV following the use of moderately
emetogenic chemotherapy.
Multiday chemotherapy
Multiday chemotherapy presents a challenge in emesis
control, since the sequence of therapies adds complexity
to the emetogenic potential of the various agents.1 Phar­
macists also need to address such special issues as setting,
preferred route of administration, patient adherence,
dosing, and tolerability of antiemetics in the context of
multiday therapy.
No standard of care exists for CINV prevention in
multiday chemotherapy. The NCCN suggests dexamethasone and a 5-HT3 receptor antagonist in patients receiving moderately to highly emetogenic multiday chemo-
Evolving Treatment Paradigms for CINV
Table 2 Updated ASCO,9,10 NCCN,1 and MASCC/ESMO8 Guidelines: Antiemetic Recommendations for High– and
Moderate–Emetic-Risk Chemotherapy Regimens
High–Emetic-Risk Chemotherapy
Professional Society Regimens
Moderate–Emetic-Risk Chemotherapy Regimens
ASCO10
3-drug combination:
NK1 receptor antagonist, 5-HT3
receptor antagonist, and dexamethasone
2-drug combination:
Palonosetron + dexamethasone
“Preferential use of palonosetron is recommended.”
If palonosetron is not available, any first-generation
5-HT3 receptor antagonist, preferably granisetron
or ondansetron
Evidence on adding aprepitant is limited, but
clinicians may consider use of the agent
NCCN1
Acute and delayed prevention:
Prior to initiating chemotherapy,
begin combination regimen with
5-HT3 receptor antagonist on day 1
(palonosetron is preferred)
Steroida on days 1-4
NK1 receptor antagonist on days 1-3
Data for postcisplatin (≥50 mg/m )
emesis prevention are category 1;
others are category 2A
2
Prevention:
Day 1
Prior to initiating chemotherapy, begin
day 1 combined regimen of 5-HT3 receptor
antagonist (all are category 1; palonosetron,
on day 1 only, is preferredb)
Steroida
With/without NK1 receptor antagonist
Data for postcarboplatin ≥300 mg/m2,
cyclophosphamide ≥600-1000 mg/m2, and
doxorubicin ≥50 mg/m2 emesis prevention are
category 1
Days 2 and 3
5-HT3 receptor antagonist (dolasetron [oral only],
granisetron, or ondansetron)
Or
Steroid monotherapya
Or
NK1 receptor antagonist with or without steroid
(if NK1 antagonist is used on day 1)c
MASCC/ESMO8
Acute prevention:
5-HT3 receptor antagonist,
dexamethasone, and aprepitant
Acute prevention for AC regimens:
5-HT3 receptor antagonist, dexamethasone,
and aprepitant
Delayed prevention:
Dexamethasone and aprepitant
Delayed prevention (other than AC):
Dexamethasone
Delayed prevention for AC regimens:
Aprepitant
AC indicates anthracycline plus cyclophosphamide; ASCO, American Society of Clinical Oncology;
MASCC/ESMO, Multinational Association of Supportive Care in Cancer/European Society for Medical Oncology;
NCCN, National Comprehensive Cancer Network.
a
Use of steroids is contraindicated with such agents as interleukin-2 (ie, IL-2, aldesleukin) and interferon.1
b
Data with palonosetron are based on randomized studies with 2-drug combinations.1
c
As with high–emetic-risk prevention, aprepitant should be added (to dexamethasone and a 5-HT3 antagonist regimen) for select patients receiving other chemotherapy regimens of moderate emetic risk (eg, carboplatin, doxorubicin, epirubicin, ifosfamide, irinotecan, or methotrexate).1
August 2013
9
Evolving Treatment Paradigms for CINV
therapy, with an NK1 receptor antagonist added if the
multiday regimen is expected to be highly emetogenic
and likely to cause delayed emesis.1 Treatment administration may occur throughout chemotherapy and for 2 to
3 days after, depending on the agent selected and patient
needs.1 According to the NCCN, a single dose of palonosetron administered prior to the initiation of chemotherapy may be sufficient for a 3-day chemotherapeutic regimen, rather than multiple daily doses of other 5-HT3
receptor antagonists.1 ASCO 2011 guidelines suggest that
Treatment administration may occur
throughout chemotherapy and for 2 to 3
days after, depending on the agent
selected and patient needs.
antiemetic agents appropriate for the emetogenic risk
class of the chemotherapy be administered for each day of
chemotherapy and for 2 days thereafter, based on patient
needs.10 Triple therapy is recommended by ASCO for
5-day cisplatin-based regimens.10 Limited clinical evidence also supports the use of the granisetron transdermal
system in multiday chemotherapy regimens with a moderate to high emetogenic risk.10
Conclusion
Novel, targeted antiemetics have expanded clinical
treatment options for CINV prophylaxis. The use of
these agents, however, requires complex, multidrug regimens and meticulous attention to dosing recommendations. Clearly, the art and science of pharmacy practice
are critical for the successful use of antiemetic agents. For
this reason, pharmacists remain at the forefront of CINV
management.
References
1. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in
Oncology (NCCN Guidelines®): Antiemesis. Version 1.2013. http://www.nccn.org/
professionals/physician_gls/PDF/antiemesis.pdf. Accessed June 20, 2013.
2. Celio L, Ricchini F, De Braud F. Safety, efficacy, and patient acceptability of single-dose fosaprepitant regimen for the prevention of chemotherapy-induced nausea
and vomiting. Patient Prefer Adherence. 2013;7:391-400.
3. Tipton JM, McDaniel RW, Barbour L, et al. Putting evidence into practice: evidence-based interventions to prevent, manage, and treat chemotherapy-induced
nausea and vomiting. Clin J Oncol Nurs. 2007;11:69-78.
4. Liau CT, Chu NM, Liu HE, et al. Incidence of chemotherapy-induced nausea and
vomiting in Taiwan: physicians’ and nurses’ estimation vs. patients’ reported outcomes. Support Care Cancer. 2005;13:277-286.
5. Neymark N, Crott R. Impact of emesis on clinical and economic outcomes of
cancer therapy with highly emetogenic chemotherapy regimens: a retrospective analysis of three clinical trials. Support Care Cancer. 2005;13:812-818.
6. Burke TA, Wisniewski T, Ernst FR. Resource utilization and costs associated with
chemotherapy-induced nausea and vomiting (CINV) following highly or moderately
emetogenic chemotherapy administered in the US outpatient hospital setting. Support
Care Cancer. 2011;19:131-140.
7. Tina Shih Y-C, Xu Y, Elting LS. Costs of uncontrolled chemotherapy-induced
nausea and vomiting among working-age cancer patients receiving highly or moderately emetogenic chemotherapy. Cancer. 2007;110:678-685.
10
August 2013
Supplement
8. Roila F, Herrstedt J, Aapro M, et al; on behalf of the ESMO/MASCC Guidelines
Working Group. Guideline update for MASCC and ESMO in the prevention of
chemotherapy- and radiotherapy-induced nausea and vomiting: results of the Perugia
consensus conference. Ann Oncol. 2010;21(suppl 5):v232-v243.
9. Kris MG, Hesketh PJ, Somerfield MR, et al. American Society of Clinical Oncology
guideline for antiemetics in oncology: update 2006. J Clin Oncol. 2006;24:2932-2947.
10. Basch E, Prestrud AA, Hesketh PJ, et al. Antiemetics. American Society of Clinical
Oncology clinical practice guideline update. J Clin Oncol. 2011;29:4189-4198.
11. Navari RM. Management of chemotherapy-induced nausea and vomiting: focus
on newer agents and new uses for older agents. Drugs. 2013;73:249-262.
12. Navari RM. Pathogenesis-based treatment of chemotherapy-induced nausea and
vomiting—two new agents. J Support Oncol. 2003;1:89-103.
13. Hesketh PJ. Chemotherapy-induced nausea and vomiting. N Engl J Med.
2008;358:2482-2494.
14. Molassiotis A, Stamataki Z, Kontopantelis E. Development and preliminary validation of a risk prediction model for chemotherapy-related nausea and vomiting.
Support Care Cancer. 2013 May 30. [Epub ahead of print]
15. Schwartzberg L, Szabo S, Gilmore J, et al. Likelihood of a subsequent chemotherapy-induced nausea and vomiting (CINV) event in patients receiving low, moderately or highly emetogenic chemotherapy (LEC/MEC/HEC). Curr Med Res Opin. 2011;
27:837-845.
16. Cubeddu LX, Hoffmann IS, Fuenmayor NT, Finn AL. Efficacy of ondansetron
(Gr 38032F) and the role of serotonin in cisplatin-induced nausea and vomiting.
N Engl J Med. 1990;322:810-816.
17. del Giglio A, Soares HP, Caparroz C, Castro PC. Granisetron is equivalent to
ondansetron for prophylaxis of chemotherapy-induced nausea and vomiting: results of
a meta-analysis of randomized controlled trials. Cancer. 2000;89:2301-2308.
18. Jordan K, Hinke A, Grothey A, Schmoll HJ. Granisetron versus tropisetron for
prophylaxis of acute chemotherapy-induced emesis: a pooled analysis. Support Care
Cancer. 2005;13:26-31.
19. Jordan K, Hinke A, Grothey A, et al. A meta-analysis comparing the efficacy of
four 5-HT3-receptor antagonists for acute chemotherapy-induced emesis. Support Care
Cancer. 2007;15:1023-1033.
20. US Food and Drug Administration. FDA Drug Safety Communication: Abnormal
heart rhythms associated with use of Anzemet (dolasetron mesylate). December 17,
2010. http://www.fda.gov/Drugs/DrugSafety/ucm237081.htm?rf=60121.htm. Accessed
July 10, 2013.
21. US Food and Drug Administration. FDA Drug Safety Communication: Abnormal
heart rhythms may be associated with use of Zofran (ondansetron). September 15,
2011. http://www.fda.gov/Drugs/DrugSafety/ucm271913.htm. Accessed July 18, 2013.
22. Gralla R, Lichinitser M, Van der Vegt S, et al. Palonosetron improves prevention
of chemotherapy-induced nausea and vomiting following moderately emetogenic
chemotherapy: results of a double-blind randomized phase III trial comparing single
doses of palonosetron with ondansetron. Ann Oncol. 2003;14:1570-1577.
23. Eisenberg P, Figueroa-Vadillo J, Zamora R, et al; 99-04 Palonosetron Study
Group. Improved prevention of moderately emetogenic chemotherapy-induced nausea and vomiting with palonosetron, a pharmacologically novel 5-HT3 receptor antagonist: results of a phase III, single-dose trial versus dolasetron. Cancer. 2003;98:
2473-2482.
24. Aapro MS, Grunberg SM, Manikhas GM, et al. A phase III, double-blind, randomized trial of palonosetron compared with ondansetron in preventing chemotherapy-induced nausea and vomiting following highly emetogenic chemotherapy. Ann
Oncol. 2006;17:1441-1449.
25. Aogi K, Sakai H, Yoshizawa H, et al. A phase III open-label study to assess safety
and efficacy of palonosetron for preventing chemotherapy-induced nausea and vomiting (CINV) in repeated cycles of emetogenic chemotherapy. Support Care Cancer.
2012;20:1507-1514.
26. Saito M, Aogi K, Sekine I, et al. Palonosetron plus dexamethasone versus granisetron plus dexamethasone for prevention of nausea and vomiting during chemotherapy: a double-blind, double-dummy, randomised, comparative phase III trial. Lancet
Oncol. 2009;10:115-124.
27. Hatoum HT, Lin S-J, Buchner D, Cox D. Comparative clinical effectiveness of
various 5-HT3 RA antiemetic regimens on chemotherapy-induced nausea and vomiting associated with hospital and emergency department visits in real world practice.
Support Care Cancer. 2012;20:941-949.
28. Balu S, Buchner D, Craver C, Gayle J. Palonosetron versus other 5-HT3 receptor
antagonists for prevention of chemotherapy-induced nausea and vomiting in patients
with cancer on chemotherapy in a hospital outpatient setting. Clin Ther. 2011;33:
443-455.
29. Feinberg B, Gilmore J, Haislip S, et al. Impact of initiating antiemetic prophylaxis with palonosetron versus ondansetron on risk of uncontrolled chemotherapy-induced nausea and vomiting in patients with lung cancer receiving multi-day chemotherapy. Support Care Cancer. 2012;20:615-623.
30. Schwartzberg L, Jackson J, Jain G, et al. Impact of 5-HT3 RA selection within
triple antiemetic regimens on uncontrolled highly emetogenic chemotherapy-induced
nausea/vomiting. Exp Rev Pharmacoecon Outcomes Res. 2011;11:481-488.
31. Goodin S, Cunningham R. 5-HT3-receptor antagonists for the treatment of nausea and vomiting: a reappraisal of their side-effect profile. Oncologist. 2002;7:424-436.
Evolving Treatment Paradigms for CINV
32. Roila F, Fatigoni S. New antiemetic drugs. Ann Oncol. 2006;17(suppl 2):ii96-ii100.
33. Warr DG, Grunberg SM, Gralla RJ, et al. The oral NK1 antagonist aprepitant for
the prevention of acute and delayed chemotherapy-induced nausea and vomiting:
pooled data from 2 randomised, double-blind, placebo controlled trials. Eur J Cancer.
2005;41:1278-1285.
34. Hesketh PJ, Grunberg SM, Herrstedt J, et al. Combined data from two phase III
trials of the NK1 antagonist aprepitant plus a 5HT3 antagonist and a corticosteroid for
prevention of chemotherapy-induced nausea and vomiting: effect of gender on treatment response. Support Care Cancer. 2006;14:354-360.
35. dos Santos LV, Brunetto AT, Sasse AD, et al. NK1 receptor antagonists for the
prevention of chemotherapy-induced nausea and vomiting: an updated meta-analysis.
J Clin Oncol (ASCO Annual Meeting Abstracts). 2013;31(suppl):Abstract e20506.
36. Hashimoto H, Yamanaka T, Shimada Y, et al. Palonosetron (PALO) versus granisetron (GRA) in the triplet regimen with dexamethasone (DEX) and aprepitant
(APR) for preventing chemotherapy-induced nausea and vomiting (CINV) in patients (pts) receiving highly emetogenic chemotherapy (HEC) with cisplatin
(CDDP): a randomized, double-blind, phase III trial. J Clin Oncol (ASCO Annual
Meeting Abstracts). 2013;31(suppl):Abstract 9621.
37. Dando TM, Perry CM. Aprepitant: a review of its use in the prevention of chemotherapy-induced nausea and vomiting. Drugs. 2004;64:777-794.
38. Aapro MS, Rossi G, Rizzi G, et al. Phase III study of NEPA, a fixed-dose combination of netupitant (NETU) and palonosetron (PALO), versus PALO for prevention
of chemotherapy-induced nausea and vomiting (CINV) following moderately emetogenic chemotherapy (MEC). J Clin Oncol (ASCO Annual Meeting Abstracts).
2013;31(suppl):Abstract LBA9514.
39. Hesketh PJ, Rossi G, Rizzi G, et al. Efficacy of NEPA, a novel combination of
netupitant (NETU) and palonosetron (PALO), for prevention of chemotherapy-induced nausea and vomiting (CINV) following highly emetogenic chemotherapy
(HEC). J Clin Oncol (ASCO Annual Meeting Abstracts). 2013;31(suppl):Abstract 9512.
40. A.P. Pharma Inc. A.P. Pharma receives FDA complete response letter for
APF530. http://phx.corporate-ir.net/phoenix.zhtml?c=115565&p=irol-newsArticle
&ID=1801306&highlight=. Accessed June 24, 2013.
August 2013
11
Case Study: CINV with Multiday Chemotherapy
Managing Nausea and Vomiting in a Patient
Receiving Multiday Chemotherapy
Joanna Schwartz, PharmD, BCOP
Assistant Professor, Department of Pharmacy Practice, Albany College of Pharmacy and
Health Sciences, Vermont Campus, Colchester, VT
J
K is a 25-year-old man who presents with a mixed
germ cell, predominantly seminoma, locally advanced
(positive paraaortic lymph node) stage IIB testicular
cancer. Three weeks ago, he underwent an orchiectomy
and today will begin a multiday chemotherapy regimen of
BEP, with curative intent. The patient will receive bleomycin (B) 30 units administered intravenously (IV) once
weekly; IV etoposide (E) administered at 100 mg/m2 IV
on days 1 through 5; and cisplatin (P) administered IV at
20 mg/m2 on days 1 through 5. The patient will also receive subcutaneous pegfilgrastim (6 mg) on day 6, repeated every 21 days. The physician asks you, the pharmacist,
to provide recommendations for antiemetic prophylaxis
to write on the chemotherapy orders, as well as home
antiemetic prescriptions that may be helpful (in addition
to prochlorperazine 10 mg orally, as needed, for breakthrough nausea or vomiting).
The duration of BEP-related delayed
CINV may last into days 7 to 9 due to the
multiple cumulative dosing of the cisplatin
in this particular regimen.
Discussion
The American Cancer Society determines that approximately 8500 new cases of testicular cancer will be
diagnosed during 2013 in the United States.1 The majority (95%) of testicular neoplasms are germ cell tumors
(GCTs); other testicular neoplasms (ie, sex-cord stromal
tumors, lymphomas) occur less frequently.2 The introduction of the multiday BEP regimen has established testicular cancer as a model of a curable malignancy, even in
advanced stages.2 According to both American Society of
Clinical Oncology (ASCO) and National Comprehensive
Cancer Network guidelines,3,4 cisplatin is classified in the
“high” emetic risk category. Because BEP is one of the few
multiday cisplatin-based regimens, it is associated with
reports of severe acute and delayed chemotherapy-induced nausea and vomiting (CINV), despite the advent
of newer antiemetic agents such as the serotonin (5-HT3)
12
August 2013
Supplement
receptor antagonists and neurokinin 1 (NK1) receptor
antagonists.2-4 Because GCTs account for only 1% of all
diagnosed cancers,1 the appropriate CINV prophylaxis
regimens are not well studied or defined.
Given the challenges related to CINV control for
patients receiving multiagent chemotherapy, ASCO
addressed this issue in their updated 2011 guidelines,
stating that “antiemetics appropriate for the emetogenic
risk class of the chemotherapy should be administered to
provide antiemetic coverage for each day of the chemotherapy and 2 days afterward. Based on limited data, patients who receive 5-day cisplatin should receive aprepitant/fosaprepitant and 5-HT3 receptor antagonists and
dexamethasone.”3
Unfortunately, these guidelines do not give specific
recommendations for dosing and duration of antiemetics for multiday chemotherapy. When the NK1 receptor
antagonists fosaprepitant and aprepitant are given at
the dosing approved by the US Food and Drug Ad­
ministration (FDA), they have duration of action ranging from 3 to 5 days.5,6 The duration of action of the
second-generation 5-HT3 receptor antagonist palonosetron typically ranges from 3 to 4 days.7 However, the
duration of BEP-related delayed CINV may last into
days 7 to 9 due to the multiple cumulative dosing of the
cisplatin in this particular regimen.8,9 Therefore, the
appropriate dosing frequency of fosaprepitant, aprepitant, and palonosetron for patients receiving this regimen remains undetermined. Additionally, both the risks
associated with extending the duration of dexamethasone therapy and the best dosing of dexamethasone for
7 to 9 days to cover the extended period of risk for delayed CINV are still unclear.
In a study by Einhorn and colleagues, investigators
assessed the efficacy of palonosetron plus dexamethasone
in 41 patients receiving 5-day cisplatin for the treatment
of GCT. Patients who received palonosetron on days 1,
3, and 5 and dexamethasone on days 1, 2, 6, 7, and 8
achieved complete response rates of 34.1% and 61.0%,
respectively, in acute and delayed CINV phases.10 Clearly,
these outcomes may be further improved with the addition of a NK1 receptor antagonist, although the suggested
Case Study: CINV with Multiday Chemotherapy
Table Recent Studies of Antiemetic Prophylaxis Strategies Using 5-HT3 Receptor Antagonists, NK1
Receptor Antagonists, and Steroids for Multiday Cisplatin-Based HEC Chemotherapy
Treatment Arms
Results
Author, Year
Design and Size (N) (A) and (B) (if randomized)
(A) versus (B)
Albany et al,
201211
Randomized,
double-blind,
placebo-controlled,
phase 3 crossover
N=69
A: aprepitant 125 mg po day 3,
80 mg po days 4-7 (5 total days);
dexamethasone 20 mg IV days 1-5,
then 8 mg po BID days 6 and 7,
then 4 mg po BID day 8;
ondansetron 8 mg IV days 1-5
B: placebo + dexamethasone/
ondansetron as noted above
Gao et al, 201312
Single-arm,
prospective
N=41
(Cisplatin given 3
days only)
Jordan et al,
200913
Single-arm,
observational
N=38
(Multiday HEC)
CR overall: 42% vs 13%
(P <.001)
CR delayed: 63% vs 35%
(P <0.001)
CR acute: 47% vs 15%
(P <.001)
VAS nausea: trend favoring A, but
not statistically significant
Patient preference:
38% vs 11% (P <.001)
Aprepitant 125 mg po day 1,
80 mg po days 2 and 3;
palonosetron 0.5 mg IV day 1
and day 3;
dexamethasone 5 mg IV on days 1,
2, and 3
CR overall: 58.3%
CR delayed: 78%
No nausea: 17%
Aprepitant 125 mg po day 1,
80 mg po days 2, 3, 4, 5, 6, and 7
(7 total days);
granisetron 1 mg IV days 1, 2, 3,
4, and 5;
dexamethasone 8 mg IV days 1, 2,
3, 4, 5; then
dexamethasone 8 mg po days 6
and 7
CR overall: 57.9%
CR delayed: 68%
CR acute: 66%
The 2011 updated ASCO antiemesis guidelines recommend a triple-therapy prophylaxis regimen containing a steroid, NK1 receptor antagonist, and 5-HT3 receptor antagonist prior to HEC regimens. Cisplatin is listed in the “high
emetic risk” category in the guidelines.
ASCO indicates American Society of Clinical Oncology; BID, twice daily; CR, complete response: no vomiting episodes, no use of breakthrough (rescue) antiemetics for days 1-5 (overall phase), delayed phase, days 2-9; HEC, highly
emetogenic chemotherapy; IV, intravenously; NCCN, National Comprehensive Cancer Network; PO, orally; VAS,
visual analog scale (ratings of nausea on a scale of 1-10).
dosing in this situation remains unclear and is not delineated in the most recent ASCO guidelines.
Fortunately, as shown in the Table, data from several
recent trials using the triple regimen of a 5-HT3 receptor
antagonist, an NK1 receptor antagonist, and a steroid may
provide some insight on reducing the incidence and severity of CINV.11-13 The limitations of some of these trials
include lack of randomization and small sample size.
However, a large definitive study of CINV management
in the treatment of patients with GCTs is not anticipated, due to the rarity of the disease. It is also important to
note that these studies were performed prior to the FDA
approval of fosaprepitant; the use of this agent has since
increased substantially.
Applying Clinical Data to Everyday Practice
Because our clinic has fosaprepitant and palonosetron
on our formulary, I would recommend that the patient in
the above case study receive IV fosaprepitant at 150 mg
prior to chemotherapy on day 1 and day 4 to emulate the
extended durations of aprepitant shown in the Table.
This dosing would take into consideration that if fosa­
prepitant were given just once on day 1 or aprepitant
given on just days 1, 2, and 3, as per the FDA-approved
labeling, the treatment would not cover the delayed nausea of a multiday cisplatin regimen on days 2 to 9. Addi­
tionally, I would recommend IV palonosetron at 0.25 mg
prior to chemotherapy on days 1, 3, and 5 based on the
excellent results reported in the study by Einhorn and
August 2013
13
Case Study: CINV with Multiday Chemotherapy
colleagues10, as well as IV dexamethasone 12 mg on day
1, then 8 mg on days 2 to 5 prior to chemotherapy, and
then a home prescription for dexamethasone 8 mg (2
tablets) on day 6 and 4 mg (1 tablet) on day 7. We have
found that the addition of an IV formulation of an NK1
antagonist, as well as a longer-acting 5-HT3 receptor antagonist has helped many of the patients at our clinic
without drug coverage insurance or with high copays, and
has improved patient compliance as well. Both aprepitant
capsules and ondansetron tablets are expensive, and in
my experience I have observed that some patients do not
choose to pick up these prescriptions or take them as directed to save costs.
As per the ASCO guidelines, refractory
CINV despite this prophylaxis may be treated
with olanzapine, lorazepam, or dronabinol.
Clinics or hospitals with formularies that include aprepitant and ondansetron may use one of the regimens from
the studies in the Table. All patients should be counseled
to take prochlorperazine, a dopamine antagonist, for the
treatment of breakthrough nausea and vomiting every 6
hours, as needed. As per the ASCO guidelines, refractory
CINV despite this prophylaxis may be treated with olanzapine, lorazepam, or dronabinol.
Conclusion
CINV remains one of the most significant side effects
of cancer treatment, impacting patients’ quality of life
and treatment compliance and potentially necessitating
changes in therapy. Several evidence-based guidelines
now exist to assist clinicians regarding the best regimens
for CINV prevention, and these guidelines have recently
14
August 2013
Supplement
been updated to reflect the publication of major clinical
trials and the approval of new agents.
Pharmacists have a vital role in reviewing the published studies on this topic with their colleagues and assisting with preprinted templates and orders for multiday
chemotherapy, especially as the ASCO guidelines do not
clearly delineate specific recommendations for dosing and
frequency of antiemetics to help prevent CINV during
multiday chemotherapy regimens. It is through such efforts that we can significantly improve patient outcomes.
References
1. American Cancer Society. Cancer Facts and Figures 2013. Atlanta, GA: American
Cancer Society; 2013. http://www.cancer.org/acs/groups/content/@epidemiologysurveilance/documents/document/acspc-036845.pdf. Accessed July 24, 2013.
2. Feldman DR, Bosl GJ, Sheinfeld J, et al. Medical treatment of advanced testicular
cancer. JAMA. 2008;299:672-684.
3. Basch E, Prestrud AA, Hesketh PJ, et al. Antiemetics. American Society of Clinical
Oncology clinical practice guideline update. J Clin Oncol. 2011;29:4189-4198.
4. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in
Oncology (NCCN Guidelines®): Antiemesis. Version 1.2013. http://www.nccn.org/
professionals/physician_gls/PDF/antiemesis.pdf. Accessed July 31, 2013.
5. Emend (aprepitant) Capsules [package insert]. Whitehouse Station, NJ: Merck &
Co, Inc; 2011.
6. Emend (fosaprepitant dimeglumine) for Injection, for intravenous use [package insert]. Whitehouse Station, NJ: Merck & Co, Inc; 2011.
7. Aloxi (palonosetron HCl) injection for Intravenous Use [package insert].
Albuquerque, NM: OSO Biopharmaceuticals, LLC; Dublin, Ireland: Helsinn
Healthcare SA; Woodcliff Lake, NJ: Eisai, Inc; 2009.
8. Navari RM. Prevention of emesis from multiple-day chemotherapy regimens. J Natl
Compr Canc Netw. 2007;5:51-19.
9. Hainsworth JD. The use of ondansetron in patients receiving multiple-day cisplatin
regimens. Semin Oncol. 1992;19(suppl 10):48-52.
10. Einhorn LH, Brames MJ, Dreicer R, et al. Palonosetron plus dexamethasone for
prevention of chemotherapy-induced nausea and vomiting in patients receiving multiple-day cisplatin chemotherapy for germ cell cancer. Support Care Cancer.
2007;15:1293-1300.
11. Albany C, Brames MJ, Fausel C, et al. Randomized, double-blind, placebo-controlled, phase III cross-over study evaluating the oral neurokinin-1 antagonist aprepitant in combination with a 5HT3 receptor antagonist and dexamethasone in patients
with germ cell tumors receiving 5-day cisplatin combination chemotherapy regimens:
a Hoosier Oncology Group study. J Clin Oncol. 2012;30:3998-4003.
12. Gao HF, Liang Y, Zhou NN, et al. Aprepitant plus palonosetron and dexamethasone for prevention of chemotherapy-induced nausea and vomiting in patients receiving multiple-day cisplatin chemotherapy. Intern Med J. 2013;43:73-76.
13. Jordan K, Kinitz I, Voigt W, et al. Safety and efficacy of a triple antiemetic combination with the NK-1 antagonist aprepitant in highly and moderately emetogenic
multiple-day chemotherapy. Eur J Cancer. 2009;45:1184-1187.
Update on Emerging Agents
Update on Emerging Agents in CINV:
Are Practice Changes Ahead?
James J. Natale, PharmD, BCOP
Manager, Outpatient Oncology Pharmacy Services, UPMC CancerCenter, a partner with
University of Pittsburgh Cancer Institute
Pittsburgh, PA
N
ausea and vomiting are among the most common
and distressing adverse events associated with
cancer therapy.1,2 Patients report that inadequately controlled chemotherapy-induced nausea and
vomiting (CINV) disrupts their physical, emotional,
cognitive, and functional well-being, resulting in diminished quality of life, loss of income, and the inability to
perform activities of daily living.2,3 Over the past few decades, great progress has been made in the development
and approval of more effective antiemetic agents.
However, the medical need still exists for better prevention and management of symptoms, particularly delayed
nausea and vomiting. In this article, James J. Natale,
PharmD, BCOP, offers his perspectives on therapies that
may lead to improved outcomes for patients undergoing
chemotherapy.
Can you share your thoughts on the recent studies of
netupitant plus palonestron (NEPA) for the management of CINV?
NEPA is a novel, single-day, fixed-dose combination
of the highly selective neurokinin-1 (NK1) receptor antagonist, netupitant, and the second-generation 5-HT3
(5-hydroxytryptamine) receptor antagonist, palonosetron. This formulation allows for the targeting of 2 critical
pathways associated with CINV, and the results of recent
studies assessing the safety and efficacy of NEPA in patients undergoing chemotherapy have been promising.
In a phase 2 study, Hesketh and colleagues sought to
determine the appropriate dose of netupitant to combine
with palonosetron. This was a randomized, double-blind,
parallel-group study that enrolled patients who were undergoing cisplatin-based highly emetogenic chemotherapy. The investigators used 5 study arms to compare 3
different oral doses of NEPA (netupitant 100 mg, 200 mg,
or 300 mg plus palonosetron 0.50 mg) as well as a combination arm (ondansetron and aprepitant) versus a single
oral dose of palonosetron (0.50 mg).4 Of note, all 5 arms
employed the use of dexamethasone at recommended
doses in both the acute and delayed phases. They reported that each NEPA dose, in addition to the combination
arm, resulted in a superior complete response (CR) rate
compared with palonosetron alone during the overall
phase. Each NEPA dose was found to be superior in the
delayed phase compared with palonosetron. The results
of the combination arm were not broken down by phases
of treatment. In addition, patients in the NEPA arm who
received the 300-mg dose of netupitant had superior CR
rates (compared with palonosetron alone) in the acute
CINV phase. Adverse events were comparable across
arms with no dose-dependent response. The percentage
of patients exhibiting electrocardiogram changes was also
comparable across arms. In the phase 3 study by Aapro
and colleagues, investigators compared a single oral dose
of NEPA (netupitant 300 mg plus palonosetron 0.50 mg)
versus a single oral dose of palonosetron (0.50 mg) for the
prevention of CINV following moderately emetogenic
chemotherapy.5 They reported that NEPA was superior
to palonosetron alone in preventing CINV during both
delayed and acute CINV phases. Patients in the NEPA
arm were also less likely to report emesis and significant
nausea. The most frequently reported adverse events associated with NEPA included headache (3.3%) and
constipation (2.1%). The type and frequency of toxicities
were comparable with NEPA and palonosetron, and
there was no evidence of any cardiac safety concerns in
either study arm.
I think we have made tremendous strides in our ability
to control chemotherapy-induced vomiting, although
there is more work to be done. Unfortunately, we have
been less successful in the prevention of chemotherapy-induced nausea, which remains a troubling and underreported symptom for many patients. Therefore, one of
the most encouraging facts about these studies is the potential for NEPA to reduce the incidence of nausea, by
combining antiemetics targeting 2 prominent pathways.
I also think that the tolerability profile associated with
this therapy makes it an attractive option; we may be able
to offer patients better efficacy without substantially higher toxicity. Furthermore, the fact that NEPA is available
as a single oral formulation and combines 2 agents with
such long half-lives would be an important advantage in
terms of convenience for our patients by allowing once-acycle dosing for most chemotherapy regimens.
August 2013
15
Update on Emerging Agents
What other studies have reported encouraging results
for the prevention of nausea or vomiting?
Dronabinol has traditionally been used to combat
acute nausea and vomiting in patients undergoing therapy. However, investigators are revisiting the potential of
this agent to prevent delayed nausea. A 2012 study by
Grunberg and colleagues evaluated the safety and efficacy of dronabinol in patients receiving highly or moderately emetogenic chemotherapy.6 All participants in this
study received palonosetron (0.25 mg) and dexamethasone (10 mg) prior to chemotherapy. After double-blind
randomization, they received low-dose dronabinol (5
mg) or placebo. Dronabinol was shown to be superior to
placebo in no nausea and the duration of nausea.
Expected but tolerable toxicities seen with this agent
included fatigue, headache, dizziness, constipation, and
diarrhea. It was encouraging in this study that no patients discontinued therapy due to mood changes, a
common side effect with higher doses of cannabinoids
such as dronabinol. I think it is interesting to see this
agent used in a new way to address the unmet need of
delayed nausea, and it appears to have complementary
activity with palonosetron and dexamethasone, which
may lead to better overall control of CINV.
We are also seeing good results with the investigational
agent rolapitant, which is a potent and long-acting NK1
receptor antagonist. In a recent drug–drug interaction
study, Poma and colleagues evaluated the need for potential dose adjustments of drugs metabolized by cytochrome
P450 3A4 (CYP3A4) that might be coadministered with
rolapitant.7 Participants received oral doses of midazolam,
a sensitive CYP3A4 substrate, on days 1, 3, 8, and 11 of
the study, and received a single oral dose of rolapitant (200
mg) on day 3. Results showed that administration of rolapitant had no effect on midazolam at any measured point in
time, including on day 3, when rolapitant plasma levels
were at peak concentration. Furthermore, SCH 720881,
the active metabolite of rolapitant, did not alter plasma
levels of midazolam. These results suggest that neither rolapitant, nor its active metabolite, are inhibitors or inducers of CYP3A4. This was an important finding because
certain drugs used in the treatment of cancer are metabolized by the CYP3A4 liver enzyme pathway, which could
lead to serious drug interactions when combined with the
NK1 inhibitor aprepitant if appropriate dose reductions or
withdrawals are not instituted.8
Rolapitant is now being evaluated in a phase 3, multicenter, randomized, double-blind study in patients re-
16
August 2013
Supplement
ceiving highly emetogenic chemotherapy. Rolapitant or
placebo will be administered prior to initiation of che­
motherapy on day 1 with granisetron and dexamethasone, and patients will record all events of emesis and use
of rescue medication for established nausea and/or vomiting, and will indicate the severity of nausea they experienced in each of the previous 24 hours prior to chemotherapy administration through day 6 of cycle 1. Safety
and tolerability will be assessed by clinical review of adverse events, physical examinations, electrocardiograms,
and safety laboratory values.9
Conclusion
It is important to remember that CINV remains a serious problem for many patients receiving chemotherapy,
despite recent advancements in antiemetic therapy. In
particular, acute and delayed nausea are areas in which we
need to focus a great deal of attention. A number of organizations have published extensive guidelines on the use
of prophylactic regimens as well as directives on the management of patients with acute, delayed, breakthrough,
and anticipatory CINV. Pharmacists and other healthcare
professionals should be encouraged to remain up to date
on the most current versions of these recommendations, as
well as the latest data on investigational agents and combinations from clinical trials, to ensure the best protection
for their patients undergoing chemotherapy.
References
1. Bloechl-Daum B, Deuson RR, Mavros P, et al. Delayed nausea and vomiting continue to reduce patients’ quality of life after highly and moderately emetogenic chemotherapy despite antiemetic treatment. J Clin Oncol. 2006;24:4472-4478.
2. Hesketh PJ. Chemotherapy-induced nausea and vomiting. N Engl J Med. 2008;
358:2482-2494.
3. Vanscoy GJ, Fortner B, Smith R, et al. Preventing chemotherapy-induced nausea
and vomiting: the economic implications of choosing antiemetics. Commun Oncol.
2005;2:127-132.
4. Hesketh PJ, Rossi G, Rizzi G, et al. Efficacy of NEPA, a novel combination of netupitant (NETU) and palonosetron (PALO), for prevention of chemotherapy-induced
nausea and vomiting (CINV) following highly emetogenic chemotherapy (HEC).
J Clin Oncol (ASCO Annual Meeting Abstracts). 2013;31(suppl):Abstract 9512.
5. Aapro MS, Rossi G, Rizzi G, et al. Phase III study of NEPA, a fixed-dose combination of netupitant (NETU) and palonosetron (PALO), versus PALO for prevention
of chemotherapy-induced nausea and vomiting (CINV) following moderately emetogenic chemotherapy (MEC). J Clin Oncol (ASCO Annual Meeting Abstracts).
2013;31(suppl):Abstract LBA9514.
6. Grunberg SM, Munsell MF, Morrow PKH, et al. Randomized double-blind evaluation of dronabinol for the prevention of chemotherapy-induced nausea. J Clin Oncol
(ASCO Annual Meeting Abstracts). 2012;3(suppl):Abstract 9061.
7. Poma A, Christensen JC, Pentikis HP, et al. Rolapitant and its major metabolite do
not affect the pharmacokinetics of midazolam, a sensitive cytochrome P450 3A4
substrate. Support Care Cancer. 2013;21(suppl 1):Abstract MASCC-0441.
8. Emend (aprepitant) Capsules [package insert]. Whitehouse Station, NJ: Merck &
Co, Inc; 2011.
9. ClinicalTrials.gov. Phase 3 safety and efficacy study of rolapitant for the prevention
of chemotherapy-induced nausea and vomiting (CINV) in subjects receiving highly
emetogenic chemotherapy (HEC). NCT01499849. ClinicalTrials.gov. http://clinicaltrials.gov/ct2/show/NCT01499849. Accessed August 1, 2013.

![[Physician Letterhead] [Select Today`s Date] . [Name of Health](http://s3.studylib.net/store/data/006995683_1-fc7d457c4956a00b3a5595efa89b67b0-300x300.png)