Design of a Modified Slip Casting Procedure for the Single Step
advertisement

Design of a Modified Slip Casting Procedure for the Single Step Manufacture of
Sealed Silicone Balloons
THESIS
Presented in Partial Fulfillment of the Requirements for the Degree Master of Science in
the Graduate School of The Ohio State University
By
Michael W. Hudoba, B.S.
Graduate Program in Mechanical Engineering
********
The Ohio State University
2011
Master's Examination Committee:
Dr. Blaine Lilly, Advisor
Dr. Jose Castro
Copyright by
Michael W. Hudoba
2011
Abstract
Many applications in engineering and medicine require a flexible, ‘bag-like’
device that can withstand large amounts of internal and external pressure. In medicine,
these devices are used to control the pressure of urethras and blood vessels in urethral and
vascular occlusion procedures, respectively. Currently these devices are made by
stacking two flat sheets of silicone and gluing them together at their edges. This
eliminates the benefit of silicon’s high strength, and the strength of the device becomes
limited by the properties and application of the glue. This report outlines the research
and approach of using platinum cure silicone to make a one-piece, hollow device capable
of withstanding significant internal and external pressures. An apparatus was designed to
manufacture these devices, and a full factorial experiment was implemented to help
define the manufacturing parameters. Success was defined by enclosure of the void as
well as uniformity of the device along each of its faces. This report will outline the
procedural and technical specifics needed to create the devices. The results of these
findings can not only improve the success rate of certain procedures already using similar
devices (vascular and urethral occlusion), but can be implemented to improve any
process where a strong, flexible part with an internal void is required.
iii
Dedication
This document is dedicated to my greatest influence, my father;
And to my biggest fan, my mother
iv
Acknowledgments
I would like to thank the Ohio State University, especially the mechanical and
aerospace engineering department, for helping me develop the skills necessary to grow as
an engineer through my undergraduate and master’s degrees.
I would like to thank Josh Hassenzahl, Chad Bivens, and Neil Gardner, staff
members at the Ohio State University, for their support and assistance in manufacturing
processes used in this thesis.
I would like to thank Dr. Chris Adin, who developed the hydraulic urethral
occluders, for allowing me to help with the redesign of his device. Without Dr. Adin,
none of this would have been possible. It was a pleasure to work with him over the past
several years.
I would like to thank my family; my mother Marilyn, my father Russell, and my
brother Doug. Their continuous encouragement, love, and support are the motivation that
drives me toward success. My mother is my biggest supporter, and she always makes me
realize that I am capable of anything I put my mind to. My father has always inspired me
to strive for greatness, as I attempt to emulate his success. My brother Doug has always
been my role model and my best friend. I am where I am today because of them, and I
will continue to succeed because of their support.
v
Finally, I would especially like to thank my advisor, Dr. Blaine Lilly. Over the
past few years Dr. Lilly has become an advisor, a supporter, and a friend. Dr. Lilly’s
enthusiasm as a teacher sparked my interest in product design, research, and education.
He was very influential throughout my master’s program, and prepared me for my future
as a PhD candidate. I would not be the engineer I am today without his guidance and
support, and for that I am forever grateful.
vi
Vita
November 28, 1986 .......................................Born – Youngstown, Ohio
2005................................................................Canfield high School
September, 2009 ...........................................B.S. Mechanical Engineering, The Ohio
State University
2009 to present ..............................................Graduate Teaching Associate, Department
of Mechanical Engineering, The Ohio State
University
Fields of Study
Major Field: Mechanical Engineering
Specialization: Design and Manufacturing
vii
Table of Contents
Abstract .............................................................................................................................. iii
Dedication .......................................................................................................................... iv
Acknowledgments............................................................................................................... v
Vita.................................................................................................................................... vii
Fields of Study .................................................................................................................. vii
Table of Contents ............................................................................................................. viii
List of Tables ..................................................................................................................... xi
List of Figures ................................................................................................................... xii
List of Appendix Figures .................................................................................................. xv
Chapter 1:
Introduction and Objectives .......................................................................... 1
1.1 Introduction ............................................................................................................... 1
1.2 Canine Incontinence .................................................................................................. 2
1.3 Handmade Hydraulic Urethral Occluders ................................................................. 5
1.4 Thesis Objectives .................................................................................................... 11
Chapter 2:
Technical Background ................................................................................ 14
2.1 Similar Product Investigation .................................................................................. 14
viii
2.1.1 U.S. Patent #4592339 – Gastric Banding Device (4) ....................................... 15
2.1.2 U.S. Patent #5449368 – Laparoscopic Adjustable Gastric Banding Device (5)
................................................................................................................................... 16
2.1.3 U.S. Patent #4632114 – Urethral Sphincter Cuff (6) ....................................... 17
2.2 Process Investigation ............................................................................................... 18
2.2.1 Injection Molding ............................................................................................. 18
2.2.2 Slip Casting....................................................................................................... 22
2.3 Material Investigation ............................................................................................. 25
Chapter 3:
Occluder Design.......................................................................................... 28
3.1 Design Development ............................................................................................... 28
3.2 HUO for use in Process Development .................................................................... 33
3.3 Dacron Infusion ....................................................................................................... 36
Chapter 4:
Process Design ............................................................................................ 44
4.1 Mold Development .................................................................................................. 44
4.2 Process Development .............................................................................................. 46
4.3 Evolution from HUO to Generic Silicone Balloon ................................................. 57
Chapter 5:
Optimization Strategy ................................................................................. 64
5.1 Full Factorial Experiments ...................................................................................... 64
5.2 Developing Treatments and Treatment levels ......................................................... 65
ix
5.3 Running the experiments ......................................................................................... 72
5.4 Full Factorial results ................................................................................................ 76
Chapter 6:
Conclusions and Future Work .................................................................... 89
6.1 Conclusions ............................................................................................................. 89
6.2 Future Work ............................................................................................................ 95
Appendix A: MATLAB Code ......................................................................................... 97
Calculate avg. and SD of mass and volume .................................................................. 98
Calculate avg. and SD of lumen area ............................................................................ 99
Plot wall thickness of devices from full factorial experiment ..................................... 100
Appendix B: Gimbal Drawings ..................................................................................... 103
Appendix C: Mold Procedure ........................................................................................ 113
C1: Preparing the mold .............................................................................................. 114
C2: Creating the Flow Tube ....................................................................................... 114
C3: Mixing of Silicone A and B Components ........................................................... 114
C4: Applying the Silicone to the Mold Cavity........................................................... 115
References ....................................................................................................................... 117
x
List of Tables
Table 5.1: Full Factorial Design ...................................................................................... 73
Table 5.2: Enclosure of Experimental Devices................................................................ 78
Table 5.3: Visual Uniformity of Experimental Devices .................................................. 80
Table 6.1: Average Enclosure and Visual Output Values for Treatment A .................... 90
Table 6.2: Average Enclosure and Visual Output Values for Treatment B..................... 91
Table 6.3: Average Enclosure and Visual Output Values for Treatment C ..................... 91
Table 6.4: Average Enclosure and Visual Output Values for 8 different Parameter
Combinations .................................................................................................................... 92
Table 6.5: Treatment Levels Producing Most Successful Results ................................... 93
xi
List of Figures
Figure 1.1: Implantation of HUO....................................................................................... 4
Figure 1.2: Handmade HUO .............................................................................................. 5
Figure 1.3: Failure of Handmade HUO .............................................................................. 6
Figure 1.4: Handmade HUO Mass against Average Mass ................................................ 7
Figure 1.5: Handmade HUO Volume against Average Volume ....................................... 8
Figure 1.6: ImageJ Program to Measure Internal Lumen Area ....................................... 10
Figure 1.7: Internal Lumen Area of Handmade HUOs.................................................... 11
Figure 2.1: Gastric Banding Device................................................................................. 15
Figure 2.2: Laparoscopic Adjustable Gastric Banding Device ........................................ 16
Figure 2.3: Urethral Sphincter Cuff ................................................................................. 17
Figure 2.4: Mold Design with Inclusion of Tongue (Single Mold Half) ......................... 19
Figure 2.5: Slip Casting Procedure (Drain Slip Casting) ................................................. 24
Figure 3.1: Proposed Design 1 ......................................................................................... 28
Figure 3.2: Proposed Design 2 ......................................................................................... 29
Figure 3.3: Proposed Design 3 ......................................................................................... 31
Figure 3.4: Proposed Design 4 ......................................................................................... 31
Figure 3.5: Proposed Design 5 ......................................................................................... 32
Figure 3.6: Proposed Design 6 ......................................................................................... 32
Figure 3.7: Solid Model for Injection Molded Device .................................................... 34
xii
Figure 3.8: Solid Model with Extension Link ................................................................. 35
Figure 3.9: Teardrop Shape of Occluder.......................................................................... 36
Figure 3.10: Pressure Distribution of Donut-shaped Pressure Vessel ............................. 37
Figure 3.11: Cylindrical Pressure Vessel ......................................................................... 39
Figure 3.12: Creep Apparatus .......................................................................................... 41
Figure 3.13: Channel for Dacron Infusion ....................................................................... 43
Figure 3.14: Example of Device Infused with Dacron .................................................... 43
Figure 4.1: Silicone Mold Cavity..................................................................................... 44
Figure 4.2: Initial FDM Mold .......................................................................................... 46
Figure 4.3: Injection Method ........................................................................................... 47
Figure 4.4: Modified Syringe ........................................................................................... 48
Figure 4.5: Exit Port of Syringe ....................................................................................... 49
Figure 4.6: Successful Void A ......................................................................................... 50
Figure 4.7: Successful Void B ......................................................................................... 50
Figure 4.8: Device with Improved Uniformity of Wall Thickness .................................. 51
Figure 4.9: Sliced Open Device with Improved Uniformity of Wall Thickness ............. 52
Figure 4.10: 5 RPM 12 VDC Motor ................................................................................ 53
Figure 4.11: Assembly Drawing of Gimbal Device ........................................................ 54
Figure 4.12: Gimbal and Heat Gun Molding Setup ......................................................... 57
Figure 4.13: HUO with no Dacron or Injection Port ....................................................... 58
Figure 4.14: HUO with Dacron and Injection Port (A) ................................................... 58
Figure 4.15: HUO with Dacron and Injection Port (B) ................................................... 59
xiii
Figure 4.16: Plastic Mold Cavity ..................................................................................... 60
Figure 4.17: Enlarged Aluminum Mold Cavity ............................................................... 61
Figure 4.18: Weld-line Issue ............................................................................................ 62
Figure 4.19: Repeatable Sealed Silicone Balloon ............................................................ 63
Figure 5.1: Mold Cavity Horizontally Oriented in Gimbal ............................................. 68
Figure 5.2: Mold Cavity Vertically Oriented in Gimbal.................................................. 70
Figure 5.3: Experimental Matrix for Full Factorial Experiment...................................... 72
Figure 5.4: Orientation of Mold Cavity in Compartment for B- Treatment Level .......... 75
Figure 5.5: Orientation of Mold Cavity in Compartment for B+ Treatment Level ......... 75
Figure 5.6: Visual Uniformity Values (from left to right) of 1, 2, and 3 ......................... 79
Figure 5.7: Parameter Set 1 .............................................................................................. 81
Figure 5.8: Parameter Set 2 .............................................................................................. 82
Figure 5.9: Parameter Set 3 .............................................................................................. 83
Figure 5.10: Parameter Set 4 ............................................................................................ 84
Figure 5.11: Parameter Set 5 ............................................................................................ 85
Figure 5.12: Parameter Set 6 ............................................................................................ 86
Figure 5.13: Parameter Set 7 ............................................................................................ 87
Figure 5.14: Parameter Set 8 ............................................................................................ 88
Figure 6.1: Face Thickness of Run Parameter 4 ............................................................... 93
Figure 6.2: Run Parameter 4 - Device 6 .......................................................................... 94
Figure 6.3: Run Parameter 4 - Device 14 ........................................................................ 94
xiv
List of Appendix Figures
Figure B 1: Gimbal Base................................................................................................ 104
Figure B 2: Gimbal BaseTop ......................................................................................... 104
Figure B 3: Gimbal BaseVert ........................................................................................ 105
Figure B 4: Gimbal RingHorizontal .............................................................................. 105
Figure B 5: Gimbal RingVert1 ...................................................................................... 106
Figure B 6: Gimbal RingVert2 ...................................................................................... 106
Figure B 7: Gimbal RingShaftTop ................................................................................. 107
Figure B 8: Gimbal RingShaftBottom ........................................................................... 107
Figure B 9: Gimbal SleeveBearing ................................................................................ 108
Figure B 10: Gimbal InnerShaft .................................................................................... 108
Figure B 11: Gimbal MoldCavitySlot ........................................................................... 109
Figure B 12: Gimbal MotorPlate ................................................................................... 109
Figure B 13: Gimbal Motor ........................................................................................... 110
Figure B 14: Gimbal InnerBottom ................................................................................. 110
Figure B 15: Gimbal ConductingRing ........................................................................... 111
Figure B 16: Gimbal ConductingRing2 ......................................................................... 111
Figure B 17: Gimbal BrushHousing .............................................................................. 112
xv
Chapter 1: Introduction and Objectives
1.1 Introduction
The medical field is an industry that benefits greatly from the contributions made
from design engineers. From instruments and implants to diagnostic and life-support
machines, engineers play a key role in designing the equipment used in medicine.
Many implant applications in medicine require ‘bag-like’ devices that are solid, onepiece plastic objects that can be filled with fluid. Examples include vascular or urethral
occluders – devices that are capable of controlling the pressure and thus the flow of blood
or urine in a blood vessel or urethra, respectively. There are many processes in
manufacturing that are used to create a void within an object, such as lost-wax or blow
molding. These processes, although very effective in many situations, are not the best
choice when designing medical implant devices. With lost-wax, for example, the
additional material in the manufacturing process (the wax that is dissolved away) is not
implantable and should not be mixed with implant grade plastics. Blow molding is a very
commonly used process for creating hollow parts; however, the process requires an
opening into the cavity for gas injection. The bag-like implant devices needed for
vascular or urethral occlusion require a completely closed void capable of being filled
1
with a pressurized fluid, which are left in the body cavity. Any leakage of the fluid from
the occluder is clearly not acceptable.
The purpose of this thesis was to develop a process for fabricating one-piece silicone
occluders. The immediate application area for this project was to design a urethral
occluder for use in alleviating canine incontinence. Incontinence in female dogs typically
occurs after spaying, due to a lack of pack pressure in the urethra. Using the urethral
occlusion problem as the foundation, a process was designed that is capable of creating a
solid, one-piece silicone occluder that can hold saline solution for long periods of time
without leakage. Although the design described here was intended specifically as a
urethral occluder, the process can potentially be adapted for molding hollow silicone
parts for varied applications.
1.2 Canine Incontinence
Canine incontinence is the term used to describe the inability of a dog to control the
flow of urine through its urethra. This condition is most commonly seen in spayed
female dogs. Urethral sphincter mechanism incompetence (USMI) is seen in 13.6% to
20.1% of dogs following a hysterectomy (1). Although this condition is not fatal, it is
very detrimental to the quality of life for both the dog and its owners.
There are multiple devices and procedures that can be used to deal with or even cure
USMI. One of these options is a surgical treatment in which the anatomic position of the
bladder neck and pelvic urethra is altered causing what is known as urethral bulking.
Unfortunately, restoration of continence prior to these procedures only occurred in about
2
14% to 56% of dogs in clinical studies (1). Another option includes the administration of
estrogen or a-adrenoceptor agonists. These drugs, however, must be given 2 or 3 times a
day for the remainder of the dog’s life and do not guarantee curing the USMI (2).
A third option involves the implantation of a hydraulic urethral occluder (HUO). An
HUO is a device that wraps around the urethra and then is filled with a saline fluid. The
volume of saline used to fill the HUO determines the pressure on the urethra. In humans
with incontinence, these devices are dynamically controlled by the patient, giving them
the ability to release fluid to lower the pressure and allow for urination. In canines,
however, the pressure in the devices must be static. A pressure has to be found that will
restrict urine flow during everyday activity, yet will allow nature urine flow when the dog
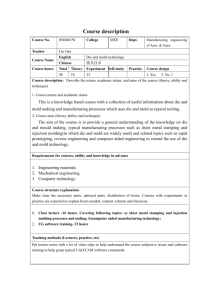
desires. Figure 1.1 is an intraoperative photograph showing the surgical placement of an
HUO in a dog (3). In this figure, the white arrowhead shows the HUO, which is wrapped
around the right caudal branch (white arrow) of the portal vein (PV). The location of the
gallbladder (GB) is also indicated.
3
Figure 1.1: Implantation of HUO
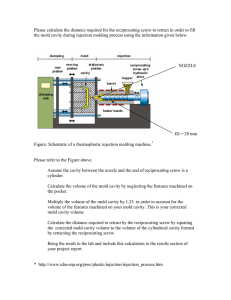
These HUOs, shown in Figure 1.2, are currently fabricated one at a time by a
laborious manual method. Because the fabrication process used to manufacture the
devices is not automated, the quality of the devices is inconsistent, which can lead to
failure of the device after surgery, necessitation a second operation to replace the
defective device. Clearly, a need exists for a manufacturing procedure that can produce
devices in standard sizes, reliably.
4
1.3 Handmade Hydraulic Urethral Occluders
Figure 1.2: Handmade HUO
As shown in Figure 1.2, the HUO (indicated by the arrow in the bottom right of
the figure) is connected via a tube to a valve (indicated by the arrow at the top of the
figure). During the HUO implant procedure, the valve is implanted underneath the skin.
The valve is used to inject or extract saline fluid. The amount of saline fluid injected in
the device controls the pressure of the occluder, and thus the pressure of the urethra.
The handmade HUOs are created by first taking two flat pieces of silicone sheet
and placing them on top of one-another. Then, the manufacturer adds a silicone adhesive
to the edges of the sheets to glue the two halves together. This gluing process is done by
hand. The manufacture of HUOs using manual methods leads to several problems with
the devices. These problems include device reliability, variation of the size of device,
and variation of the internal lumen area of the device.
After implementation, the stresses seen in the HUO over the course of its lifetime
are significantly less than the stress limit of the silicone used to make the device. Device
5
failure, however, can occur at the seams where glue is used to secure the silicone halves
together. This can be due to the strength of the glue, the amount of glue used (which
varies due to the manual nature of the application), or a combination of both. This lack
of reliability led to failure of devices in two of the first five dogs involved in a clinical
study at the University of Florida (1). Figure 1.3 shows an example of a leaking HUO.
The leak, shown at the top of the device, occurred at the glued seam.
Figure 1.3: Failure of Handmade HUO
Device-to-device variability is another important drawback with handmade
HUOs. A sample of ten handmade HUOs was measured to obtain their mass and
volume. Mass was measured using a small scale, and volume was measured using a
volume displacement technique. The average mass of the ten HUOs was found to be
3.548 g, and the average volume was 1.71 mL. Figure 1.4 and Figure 1.5 show the
masses and volumes of each HUO against the average value, respectively. As seen in the
6
figures, the standard deviation from average of the mass was low (SDmass = 0.0786 g), but
the standard deviation from average of the volume was slightly more significant (SDvolume
= 0.2025 mL).
Average mass of Handmade HUOs
3.7
3.65
3.6
mass (g)
3.55
3.5
3.45
3.4
3.35
3.3
0
1
2
3
4
5
6
Occluder
7
8
9
10
Figure 1.4: Handmade HUO Mass against Average Mass
7
11
Average Volume of Handmade HUOs
2.1
2
1.9
Volume (mL)
1.8
1.7
1.6
1.5
1.4
1.3
1.2
1.1
0
1
2
3
4
5
6
Occluder
7
8
9
10
11
Figure 1.5: Handmade HUO Volume against Average Volume
Even more critical to the success of the device than its mass and volume is the
internal lumen area. The internal lumen area is defined as the cross-sectional area
enclosed by the HUO when the HUO is sutured closed. The canine urethra travels
through the lumen. As the HUO is filled with saline fluid, the internal lumen area
decreases until it is the same size as the cross-sectional area of the urethra. From this
point, any additional volume of saline fluid added will increase the pressure on the
urethra. Variability in the manually fabricated HUOs leads to inconsistent base-line
lumen areas, which results in a lack of correlation between volume of saline injected and
urethral pressure for like-sized urethras.
8
The program ImageJ was used to calculate the base-line internal lumen area
(base-line defines the size of the internal lumen area of an empty HUO with no saline
fluid). Ten devices (different from the mass/volume analysis) were used to calculate the
variance in lumen area. Each device was sutured closed and placed in a test tube holder,
with the lumen area perpendicular to the axis of the test tube holder. Images of each
device were captured individually, with the presence of a reference measurement (a
millimeter ruler). ImageJ was then used to physically outline the lumen area, after which
the program calculated the area in pixels2. Using the reference image of the ruler, pixels2
were then converted into mm2. Figure 1.6 shows how ImageJ was used to obtain the
measurements; the yellow outline was drawn by hand onto the photograph of the HUO.
9
Figure 1.6: ImageJ Program to Measure Internal Lumen Area
To improve accuracy, each area was outlined and measured three times, and the
recorded area was the average of the three measurements. After measuring all ten HUOs
(30 total measurements), the average internal lumen area was found to be 28.8105 mm2.
Figure 1.7 shows a plot of each HUOs lumen area against the average value. As
displayed in the figure, there is a large standard deviation for internal lumen area for the
handmade HUOs (SDlumenarea = 6.2568 mm2).
10
Average Lumen Area of Hand-made HUOs
40
Area (mm2)
35
30
25
20
15
0
1
2
3
4
5
6
Occluder
7
8
9
10
11
Figure 1.7: Internal Lumen Area of Handmade HUOs
Both variability and non-reliability of handmade HUOs were the motivating factors
driving this research. Creating devices that are both reliable and consistent were two of
the important thesis objectives, which are described in the following section.
1.4 Thesis Objectives
The objectives of this research evolved throughout the life of the project. Initially,
the research focused on specifically designing a HUO to be used to cure canine
incontinence. Accordingly, the objectives were initially based around the design of the
HUO:
11
Design a clasping mechanism to eliminate the need for sutures
Develop adjustability so the device can be used on a wide-range of dog
sizes
Improve reliability reduce variability by designing the device to be
injection-molded
Research began with focus on the third objective – designing the device to be
injection-molded. After working with the material and becoming familiar with its
properties and molding characteristics, it became clear that injection-molding of platinum
cure liquid silicone might not be the best solution.
With injection-molding no longer a viable option, a new method of HUO
fabrication needed to be developed. Research began on a manufacturing method known
as slip casting, and this investigation led to the evolution of the research objectives for
this thesis. At this point, focus moved from specifically designing an HUO to designing
a manufacturing procedure for creating sealed silicone balloons. This approach is more
general and is relevant to a variety of needs both in and outside of the medical field. The
‘process-based’ objectives are described here:
Design the procedure for a modified slip casting method to create sealed
silicone balloons
Determine the parameters that have an effect on the manufacture of the
device
12
Develop a full factorial experiment to test how each parameter effects the
device
From the experiment, determine the best process and parameters for
manufacturing sealed silicone balloons
13
Chapter 2: Technical Background
2.1 Similar Product Investigation
There are many products in existence today that function in a similar manner to the
HUO devices. To aid in the improved design of the HUOs, research was done on a
number of patents for devices that control flow either by controlling the pressure or the
size of the cross-sectional area of the flow path.
The following devices were investigated to aid in the design of the HUO. Each of
these devices is designed to alter the flow through a pathway. The first two devices
control flow into the stomach by changing the cross-sectional area of the stomach
opening. The third device controls flow of urine by controlling the external pressure of
the urethra. Each device was investigated to determine both functionality as well as their
method of latching and adjustability.
14
2.1.1 U.S. Patent #4592339 – Gastric Banding Device (4)
Figure 2.1: Gastric Banding Device
Functionality – Used to treat morbid obesity by wrapping around the top of the stomach.
This creates a stoma opening that is smaller in cross-sectional area than the natural
opening of the stomach.
Latching Method – Similar to a belt. The narrower end slides into the slot at the wide
end and is pulled through. Excess length of the narrow end is cut and sutured to the band.
Adjustability – Size is controlled upon implantation. To create a smaller stoma opening,
the ‘belt’ is pulled tighter.
15
2.1.2 U.S. Patent #5449368 – Laparoscopic Adjustable Gastric Banding Device (5)
Figure 2.2: Laparoscopic Adjustable Gastric Banding Device
Functionality – Serves the same function as the gastric banding device above, only this
device can be implanted laparoscopically.
Latching Method – A flap at one end is inserted into a slot at the other end. A pin then
slides through a hole in the flap and the slot to lock them together. The pin is then
screwed into place to secure the band.
Adjustability – Size is controlled by the location of the slot relative to the flap. This size
is static and cannot be changed.
16
2.1.3 U.S. Patent #4632114 – Urethral Sphincter Cuff (6)
Figure 2.3: Urethral Sphincter Cuff
Functionality – Used to treat incontinence in humans. The cuff wraps around the urethra
and is filled with a fluid to control the pressure within the urethra. This device is similar
to the HUOs being designed in this thesis, however, the pressure exerted on the urethra
by the sphincter cuff is dynamic - the patient can control the fluid in the device by
squeezing a diaphragm (not pictured) which will add or extract fluid from the cuff.
Latching Method – Holes (left end) are placed on pins (right end) and snap into place.
Silicone adhesive is used on the pegs to lock the device into place.
Adjustability – As displayed in the image, the device has many holes similar to belt
loops to control the size of the device. This size adjustment is done intraoperatively, and
cannot be changed once it is locked into place.
17
2.2 Process Investigation
2.2.1 Injection Molding
Injection molding is a very versatile process that can be used for the manufacture of
endless types of plastic parts. There are many different types and methods of injection
molding, and each type serves a specific purpose. Injection molding methods that result
in parts with internal voids were examined to determine their usefulness in the
manufacture of the HUOs. The methods investigated include injection molding with the
use of a solid inner core, injection molding with a fusible core, and gas-assisted injection
molding.
The first injection molding process that was considered involved designing the mold
cavity with a ‘tongue’ portion that would create the cavity within the device. Figure 2.4
shows an example of a possible mold half with the inclusion of the tongue cavity.
With
this method, plastic could be injected at the top of the mold and flow around the tongue
portion of the mold, creating the cavity. When the device solidifies, it could be slid off of
the tongue and the open end (created from the bottom of the tongue portion that is
connected to the mold) can be glued together using a silicone adhesive.
18
Figure 2.4: Mold Design with Inclusion of Tongue (Single Mold Half)
The main advantage of this method would be that it could be done using standard
injection molding techniques and equipment. The disadvantage is the lack of strength
that comes from gluing the edge closed, which far outweighs the process’ advantage.
One of the objectives of this thesis is to increase the mechanical reliability of the devices
by eliminating the need to glue the edges of the device together. This ensures that the
strength of the device is based entirely on the properties of the silicone instead of the
properties and application of the silicone adhesive. The device will only be as strong as
its weakest section, so any gluing (even though the gluing was reduced 75%) would
defeat the purpose of the re-design.
Fusible core injection molding (also known as lost or soluble core injection molding)
is a process used to design hollow parts, which is precisely what the HUO is. The device
is created first by designing an insert which is a temporary core made from a material
19
with a low melting point. Examples of these materials include a tin-bismuth alloy, wax,
or a thermoplastic. The insert is placed inside of the mold, and the liquid silicone
material flows into the mold and around the temporary core. After solidification of the
silicone, the core is melted or chemically dissolved and drained, leaving behind a hollow
device.
An interesting phenomenon occurs with fusible core injection molding. Since the
melting point of the core is lower than the melting point of the silicone, it would seem
that during injection the liquid silicone would cause the core to melt. However, due to
high thermal diffusivity, large thermal inertia and latent heat of possible core materials,
the insert remains solid during the injection phase.
An advantage to the fusible core injection molding process is that the secondary step
of gluing is eliminated and the solid device is molded in a single step (the core must still
be dissolved with an additional step, but the actual device is created in a single step). The
elimination of glued edges would increase the mechanical reliability of the occluder.
Also, HUOs already have a hole used to inject or extract saline fluid. This hole could
initially be used to drain out the melted core during the lost wax procedure.
An additional advantage is that most of the temporary core materials can be re-used
and recycled. This means that the addition of a core would not significantly increase the
overall amount of material (and thus overall cost) necessary for the process.
There are certain disadvantages in using fusible core injection molding for the
purpose of manufacturing HUOs. First, appropriate core materials would have to be
investigated and tested. Silicone is a very unique plastic material; much consideration
20
would be needed to find a core material that has the appropriate mechanical and chemical
properties. These considerations come from the fact that the device is made from implant
grade silicone. Implant grade silicone is made to be safely implanted inside of a living
body for extended periods of time. With fusible core injection molding, one would also
have to ensure that the core material would not degrade or change the chemical properties
of the implant grade silicone.
Another disadvantage is that fusible core injection molding is a very expensive
process. The injection molding machine would not need to change, but the mold would
need to be designed in such a way so the temporary core can be inserted into the mold
cavity prior to injection. And although the injection molding of the device is completed
in a single step, the addition of a melting station would need to be implemented to
remove the temporary core from each device. This increases cycle time, equipment
needs, and energy cost.
The final injection molding process that was initially examined was gas-assisted
injection molding. Gas-assisted injection molding is a unique form of injection molding
in which the plastic is injected into the mold cavity and is followed by injection of a gas
that hollows out the center of the device. The typical gas used in this type of molding is
nitrogen, mainly because of its lack of reactivity with most polymers, its availability, and
its low cost. When the gas is injected into the core, it fills the thicker areas of the part
because this is where the plastic material remains liquid the longest. Thus, for the HUOs,
the walls of the device would solidify first and allow the nitrogen gas to expand
throughout the center of the device leaving behind a cavity.
21
The advantage to gas-assisted injection molding is that the device can be completed
in a single step. No additional gluing or melting stations would be needed, as with the
other injection molding procedures. This would help with mechanical reliability, as well
as mass production efficiency.
The disadvantage of gas-assisted injection molding is that a unique injection molding
machine would be needed. The machine would need to first inject the molten silicone,
and then inject the compressed gas through the sprue. This would initially require a
larger investment. However, after the initial investment, since the cost of the nitrogen is
low and the process can be completed in a single step, the per-part price would remain
low and the product process would be efficient and reliable. Although a viable option,
the high cost due to equipment requirements of gas-assisted injection molding limited its
applicability at this level of the research.
2.2.2 Slip Casting
The three possible manufacturing methods described above are all variations of the
basic injection molding process. The main problem with injection molding methods for
this application did not even become evident until the silicone material was chosen and
experimented with. Platinum cure silicone is an extremely viscous substance that does
not flow well. While heat can be added to decrease the viscosity, the addition of heat
greatly reduces the working and curing time of the silicone. Two specific problems arose
when attempting to use an injection molding procedure. First, the act of injecting the
liquid silicone was extremely difficult. The injection cavity either had to be very large,
22
or the injection force needed to be significantly high. Secondly, once injected into the
cavity the liquid silicone would not separate from itself to coat the inner walls of the
cavity and leave a void. Instead, the silicone would cohere as a single solid piece. A
third indirect problem with injection molding of silicone is the upkeep and maintenance
of the injection molding machine. The liquid silicone leaves some of itself behind on
anything it comes in contact with, and it is very difficult to clean/remove. Upkeep of the
injection molding machine would include a very tedious process of cleaning the injection
port to ensure that no silicone is left behind to harden inside the machine. Because of
these issues, alternatives to the initial injection molding manufacturing method needed to
be investigated and considered.
A method of manufacturing known as colloid casting was investigated to determine if
it could be beneficial to the design and manufacture of the HUOs. A colloid is defined as
a substance microscopically dispersed evenly throughout another. This sounds similar to
platinum cure liquid silicone rubber – even amounts of Part A and Part B are mixed
together. Once mixed, the material cures and solidifies. Typically, ceramics are the
materials used in colloid casting procedures. Although silicone is obviously not a
ceramic, two types of colloid casting were investigated to see if the procedure could be
modified for the manufacture of the HUOs.
The most common form of colloid casting is known as slip casting. Slip casting is
used to produce items such as tableware, structural tubing, and a variety of automotive
and biomedical components. The procedure begins with the pouring of the aqueous
23
material (known as a slip) into a permeable mold that has the shape of the desired part.
Next, one of the three following methods is used:
Drain slip casting – The slip material is cast for a limited amount of time to
form a wall layer of desired thickness. After the desired wall thickness is
reached, the slip material is then drained from the mold (Figure 2.5) (4).
Solid slip casting – The slip material is continuously added until a solid cast of
desired thickness is formed. No additional material exists to drain.
Vacuum slip casting – A vacuum is applied to the mold to increase the rate of
filtration
Figure 2.5: Slip Casting Procedure (Drain Slip Casting)
A second form of colloid casting is known as centrifugal casting. Centrifugal casting
is similar to slip casting, except coating the walls of the mold and separating the colloid
material is assisted by centrifugal motion. Centrifugal casting will push all of the liquid
material outward from the axis of rotation. Thus, if the axis of rotation is defined as the
24
axis of the desired part, then all of the material will be pushed to the outer walls leaving a
voided inner core.
By themselves, none of the above described methods would work for the manufacture
of an HUO for this research, either due to the specific procedure or limiting factors such
as equipment availability and cost. However, information learned from injection molding
in combination with the slip and centrifugal casting procedures led to the development of
the modified slip casting method that was used throughout the experiment to create
devices. The specifics of that procedure are outlined in chapter 4, Process Design.
2.3 Material Investigation
An important step in the development of the HUOs is determining the material to be
used in manufacture. The manufacturing process for making the hand-made HUOs
begins with sheets of solid silicone, yet the modified design of the HUOs requires the use
of platinum cure silicone that begins as a liquid. Aside from having an initial liquid state,
the other important characteristic required of the material is that it is implantable in a
living body.
Silicones have inherently low toxicity, which presents low risk for biological
reactions. For this reason, they have gained recognition and acceptance in a wide range
of industrial and medical applications. There are three ‘types’ of FDA tested silicones
(5), with each level of silicones undergoing more rigorous testing. The first type is ‘food
grade’ silicones. These are not accepted as usable silicones for medical applications.
The next type is ‘USP Class 6’ silicones. These silicones are typically used for
25
packaging drugs and food. Although more pure than food grade silicones, USP Class 6
silicones are still not acceptable for implantable devices. For an implant application, one
must use the third class of silicone known as ‘medical grade’ or ‘implant grade’ silicone.
These silicones go through rigorous biological testing and are rated by the FDA to be
used in medical procedures, including implantation devices.
Material investigation led to an implant grade silicone supplier, Applied Silicone
Corporation. After the development of a non-disclosure agreement, Applied Silicone
Corporation assisted in determining an implant grade silicone for manufacture of the
HUOs. The material chosen was Applied Silicone Implant Grade Liquid Silicone Rubber
30 (LSR 30). LSR 30 is a two part pourable silicone elastomer that has been rated as
implant grade by the FDA. The material is a two part, 10:1 mixture (10 parts A 1 part B
by mass or volume) with a 30 durometer, Shore A hardness.
Although ideal for the application, LSR 30 is not ideal for research purposes for a
number of reasons. First, the cure time was extremely high. The mold, although solid
after about 24 hours, remained tacky for a few days. Complete cure and total
solidification was not reached until approximately 72 hours after mixing. Since dozens
of parts needed to be made for experiment and testing procedures, a 3 day cure time was
too long for the purpose of this research. In addition to the long cure time, LSR 30 has an
extremely high price. A 1.1 lb kit of liquid silicone rubber cost approximately $250, and
thus it would not have been a monetarily viable option to use the LSR 30 in dozens of
trial runs and experiments.
26
For these reasons it was critical to find an alternative material to use throughout the
test phase of the research. The mold company Perma-flex assisted in determining a
research material. Perma-flex recommended using a silicone known as DragonSkin 30
(DS 30). DS 30 is a two part, 1:1 mixture (1 part A 1 part B by mass or volume) with a
hardness rating identical to that of LSR 30. DS 30 is chemically very similar to LSR 30
and behaves in a very similar manner. The main difference is that DS 30 has not
undergone the rigorous purity testing procedures that would qualify it as medical or
implant grade. For this reason, the price of DS 30 is a fraction of LSR 30’s price. The
other advantage is that DS 30 cures much more quickly, having an average cure time less
than 24 hours. For this reason, DS 30 was used throughout the course of the research.
27
Chapter 3: Occluder Design
3.1 Design Development
Before the focus of the thesis evolved to generic silicone balloon devices, the initial
objectives were focused on improving the already existing HUO design. The initial
proposed designs focused on two objectives: designing a latching mechanism to
eliminate the need for sutures and making the device intraoperatively adjustable so that it
would fit dogs of various sizes.
The initial six designs are shown in the following six figures. Each design was rated
in terms of its latching mechanism and adjustability.
Figure 3.1: Proposed Design 1
28
Figure 3.2: Proposed Design 2
Figure 3.1 was a very simple model focused on creating a latching mechanism to
replace the need for sutures during implantation. The principle of the design is simple: a
‘stretch-fit’ is used to lock the device on itself. A hole in one end of the device is
stretched over a ‘hook’ like extrusion at the other end. Once the hole is stretched over the
hook, the hoop stress seen in the device ensures that it will stay together. To unlock the
device, one would have to pull in the opposite direction of the forces seen within the
device until the hook is released from the hole. This is not something that would happen
naturally, ensuring that the device stays locked.
Although the design in Figure 3.1 offered a solution to the latching mechanism, it did
not serve to solve the adjustability problem. Figure 3.2 is a design that uses the basic
principles of the previous design, yet it provides a choice of holes to lock into the hook.
Each hole would correspond to a different circumference length, making the device
capable of fitting a variety of dogs.
29
The main problem with the previous design is that if a smaller size is desired, then the
excess length of the HUO is left hanging tangent to the circular occluder. Although
technically speaking this device is adjustable, it is not desirable to have excess length of
the HUO hanging off of the urethra. The following two designs kept the ‘stretch-fit’
principle for the locking mechanism from the first two designs but attempted an
alternative adjustment method to eliminate any overhang seen in design 2.
The designs in Figure 3.3 and Figure 3.4 attempted to solve the adjustability issue by
placing a slit at one end that goes all the way through the device. In each design, the
portion at the left of the drawing does not contain a silicone bag. Instead, this flat piece
can be slid into the slot at the opposite end of the device and then placed on the
appropriate hook (depending on desired size). The excess length that remains tangent to
the HUO in Figure 3.2 is now forced to remain circular, following the shape of the rest of
the device. The designs in Figure 3.3 and Figure 3.4 are the same, except that the former
uses a hole and hook latching method and the latter uses a tab and slot latching method.
30
Figure 3.3: Proposed Design 3
Figure 3.4: Proposed Design 4
The next two designs used a latching mechanism different from the ‘stretch-lock’
method seen in the previous designs. In the design depicted in Figure 3.5, one end of the
device has a single opening referred to as the sleeve. The other end of the device slides
into the sleeve. The adjustment of this device is simple: sliding the one end farther into
the sleeve will result in a smaller circumference. The latching method relies on the
pressure exerted by the saline fluid filling the device. The entire length of the device has
31
a saline bag, even the portion that enters into the sleeve. When the device is filled, the
expansion of the saline bag will secure the one end in the sleeve.
Figure 3.5: Proposed Design 5
The design in Figure 3.6 is the same as the design of Figure 3.5; only this design
adds the concept of a zip tie to aid in locking the device in place. In this design, the
expansion of the saline bag still secures itself within the sleeve but additional latching
support is added by a series of holes and angled notches on the sleeve and opposite end,
respectively.
Figure 3.6: Proposed Design 6
32
These initial design ideas focused on two of the three initial thesis objectives;
designing a device that can be secured without the use of sutures and designing it to be
adjustable. After the development of these initial ideas, the research shifted to focus on
the third and final of the initial objectives which was to design the device to be injectionmolded. Research into an injection-moldable design led to the modification of the part
and the eventual evolution of the research objectives.
3.2 HUO for use in Process Development
The next design that was developed included solutions to the latching and
adjustability objectives, but unlike those in the previous section this design also focused
on the third objective, i.e., designing the device to be injection molded. Figure 3.7 is a
solid model of this design. Although it appears simple, this design proved to be the best
solution to this phase of the research problem.
33
Figure 3.7: Solid Model for Injection Molded Device
The body of the device depicted in Figure 3.7 is asymmetrical. The main portion of
the device is a rectangular shaped silicone bag. The ends of the device are solid and
would not be filled with saline fluid. These ends are complementary to one another; one
end is a solid, cylindrically shaped piece while the other end is a hollow partial cylinder.
The hollow portion of the left end of Figure 3.7 would wrap around and lock into place
over top of the right end. The integrity of the latching that occurs would be determined
by the strength and stiffness of the plastic used to make the ends of the device.
Adjustability of the device is possible with the inclusion of extension pieces, one of
which is shown attached to the HUO in Figure 3.8. This portion of the device would all
be made from the same material. Unlike the main body of the device seen in Figure 3.7,
the extension piece has no silicone bag portion. Its ends, however, are identical to the
ends of the main device. As a result, the HUO can be locked together in the exact same
manner, with or without the addition of the extension piece.
34
Figure 3.8: Solid Model with Extension Link
An initial concern was that since the extension piece does not contain a saline bag
portion capable of expansion and contraction, the device would not be successful at
controlling the pressure of the urethra. After discussion with Dr. Chris Adin, the
veterinary surgeon whose idea it was to develop an improved HUO, it was determined
that this would not be an issue. Figure 3.9 is a close-up of a sutured hand-made HUO.
As seen in the figure, the likely shape of the device is a teardrop shape (from the plane
normal to the axis of the lumen area). Because of the shape of the enclosed device, the
top (tip of the teardrop) area does not induce as much pressure on the urethra as the rest
of the internal lumen area (rounded portion of the teardrop). This, however, does not
negatively affect the ability of the device to control back pressure. It was expected, then,
that as long as the extension piece remained small it would not affect the overall
effectiveness of the device.
35
Figure 3.9: Teardrop Shape of Occluder
Following Dr. Adin’s advice, it was determined that there would be a total of three
different sized occluders, each capable of including or not including the extension piece.
The extension piece would be the same for each size of occluder. The three devices
would result in a lumen diameter of 6, 8, and 10 millimeters, which corresponds to
occluder lengths of 6π mm (~18.85 mm), 8π mm (~25.13 mm), and 10π mm (~31.42
mm), respectively. The extension piece would be designed to add 1 mm to the lumen
diameter, resulting in a length of π mm (~3.14 mm). Thus, only three different devices
are needed to accommodate 6 precise urethra diameters (6, 7, 8, 9, 10, and 11 mm).
3.3 Dacron Infusion
An additional concern with the device was the desire to control not just how much
pressure the device exerted, but also in which direction the device was exerting the
pressure. Figure 3.10 displays this concern. The image on the left of the figure is the
typical pressure distribution of a donut-shaped pressure vessel. If the pressure within the
36
vessel is increased, it exerts this pressure both on the outer as well as the inner walls. If
the walls of the device are made from a non-rigid material (i.e. silicone), then one could
expect expansion not only of the inner diameter but of the outer diameter as well.
Figure 3.10: Pressure Distribution of Donut-shaped Pressure Vessel
The HUOs would ideally achieve the pressure distribution displayed on the right hand
side of Figure 3.10. In this image, the outer circumference is rigid (shown in red), so as
pressure is exerted on the outer wall, expansion will not occur. The inner wall of the
device, however, remains non-rigid. As the internal pressure of the device increases,
expansion of the device occurs, but the expansion is restricted to the inner lumen area.
Thus, all of the pressure being exerted is directed inward.
In attempts to incorporate this effect, research led to a material known as Dacron.
Dacron is a high strength flexible material made from PET fibers, used commonly for
sailcloth. The goal was to infuse the Dacron in one side of the silicone balloon, and
designate this side as the outer wall of the HUO. When saline fluid fills the HUO, the
37
inner walls made of silicone will expand but the outer walls infused with Dacron will
keep its shape.
Before designing the HUO to include the Dacron, it was important to determine its
material properties to ensure that it has a high enough strength for this application. Two
different tests were performed on the Dacron, a tensile test and a creep test.
An Instron tensile test machine was used to determine the modulus of elasticity (E) of
the Dacron. A constant velocity experiment was performed at a rate of 0.2 inches per
minute. The output of the experiment was a stress strain curve, and E was able to be
determined by measuring the slope of the stress strain plot. Equation 1 shows an example
calculation of E from the stress-strain curves. A total of ten pieces of Dacron material
were tested, resulting in an average modulus of elasticity of 15,143 psi.
(1)
To determine the effectiveness of Dacron as a backing material, it was necessary to
determine the typical stresses that would be seen on the outer walls of the device.
Roark’s Formulas for Stress and Strain by Warren C. Young has tabulated equations for
stresses for a multitude of different cases (6). In order to find typical stresses seen in the
HUOs, certain simplifying assumptions needed to be made to match up with a case seen
in the tables.
38
First, the HUO was designated as a cylindrical pressure vessel with uniform internal
pressure. The HUOs take this shape when wrapped around a urethra. The wall of the
pressure vessel was assumed to only be the silicone half with the infused Dacron. The
pressure is supplied by the saline fluid, and the inner wall is ignored. The inner geometry
can be ignored in these calculations because the important characteristics are the shape of
the outer wall (where stress is being determined) and the application of the pressure
(uniform internal pressure). Finally, the ends were assumed to be capped. Figure 3.11
and the corresponding equations (2) show the theoretical pressure vessel used to calculate
the stresses seen in the device.
Figure 3.11: Cylindrical Pressure Vessel
(2a)
(2b)
39
In the above equations, q is the internal pressure of the device, R is the radius (from
the center point of the cross-section to the inner edge of the outer wall), and t is the
thickness of the outer wall. Typical pressures seen in the HUOs are in the range of 60
mmHg to 100 mmHg. For purposes of stress calculation, the maximum pressure of 100
mmHg was used. The thickness of the wall was designated to be 1 mm, and the radius R
ranged from 2 mm to 4.5 mm (half the lumen diameter minus the wall thickness t).
Using these factors, a range of the meridional stress (σ1) and hoop stress (σ2) were found.
Equations (2a) and (2b) are considered valid when R/t is on the order ≥ 10. In the
above case, R/t ranges from only 2 to 4.5. Because of this in addition to the geometrical
assumptions made, the above stress values are not entirely accurate. However, they do
give an idea of the magnitude of stresses seen in the device. This magnitude of stress is
not even near the calculate elastic modulus (≈ 15,000 psi) of the Dacron, so it is safe to
assume that the Dacron is capable of handling the stresses that it will endure over its
lifetime.
The other test performed on the Dacron was to determine the effect of creep on the
material. Creep is defined as a permanent change of shape due to viscous deformation of
the material, induced over a long period of time (7). Although it was concluded above
that the stresses seen in the device are far lower than the modulus of the material,
40
consistent stresses over a long time (in this case, the lifetime of the implant can be over
10 years) can cause change in shape of the material.
A flexural creep test is completed by applying a constant weight to a specimen and
measuring the displacement at 1, 6, 12, and 30 minutes, then again at 1, 2, 5, 20, 50, 100,
200, 500, 700, and 1000 hours. To perform this test, a creep apparatus was designed and
built, and is shown in Figure 3.12. Each end of a strip of Dacron material is clamped to
the horizontal bars, and a calculated weight is applied in the downward direction. The
top horizontal bar is fixed, and the bottom horizontal bar is free to move in the up and
down direction. A dial indicator is used to measure the downward displacement of the
bottom horizontal bar (thus measuring the displacement of the strip of Dacron). The dial
indicator is set to 0.0” at the initial application of the downward force, and measurements
were taken at the time intervals mentioned above.
Figure 3.12: Creep Apparatus
41
The magnitude of the force applied during the creep test was determined from the
maximum hoop stress calculated above (σmax = 8.70 psi). To determine the pound-force
required for the test, σmax was multiplied by the cross-sectional area of wall of the device,
whose normal axis is parallel to the applied force. The width of the cross sectional area
was taken to be 11 mm, and the height of this area was 1 mm (this came from the
thickness of the outer wall of the theoretical pressure vessel). Multiplying σmax by the
cross sectional area, the maximum force in the direction of the hoop stress was calculated
to be Fmax = 0.15 lbs. This is a relatively small force, and since the Dacron is expected to
withstand much larger stresses, a much higher force value was used in the creep test in an
attempt to understand the materials creep behavior. The force value used in the
experiment was approximately 3 lbs.
The 3 lb force was applied to the sample of Dacron, and measurements were
tabulated at the predetermined times. After 100 hours under 3 lbs of force, the dial
indicator still read 0 (the specific dial indicator was in units of 0.001”). Even at a greatly
increased force (approximately 20 times the maximum force expected in the device), the
Dacron material showed no signs of creep. It was then concluded that the Dacron
material is strong enough to withstand the pressures seen in the device and will not be
effected by creep over the lifetime of the implant.
Once it was decided that Dacron is an appropriate material for the application, the
mold needed to be modified to allow the infusion of the Dacron in one side of the device.
To do this, an angled channel was designed into the mold. The one opening of the
channel existed at the edge of the mold cavity. This channel angled upward and
42
terminated where the two mold halves meet. The Dacron was cut to size and shape; the
center of the Dacron strip matched the shape of the device, and each end had a more
narrow extension that was fed through the channels. When these extensions were pulled
tight, the Dacron strip inside the mold cavity was suspended approximately 0.5 mm
above the bottom of the mold cavity. This allowed the liquid silicone to fill around the
Dacron sheet, infusing it approximately in the middle of the 1 mm thick silicone wall.
The channel that was designed into the mold cavity is shown at the right side of Figure
3.13, and Figure 3.14 shows an example of a device infused with the Dacron strip.
Figure 3.13: Channel for Dacron Infusion
Figure 3.14: Example of Device Infused with Dacron
43
Chapter 4: Process Design
4.1 Mold Development
The first step in the process design was to develop a prototype mold that could be
used to manufacture the test devices. This required deciding on a mold material. A
typical mold cavity material for platinum cure silicones is the platinum cure silicone
itself. The behavior of the material is such that once parts A and B are mixed and cured
(solidified), they are in a stable state and no longer chemically reactive. Thus, once a
mold cavity made from silicone cures, silicone parts can be cured in the cavity with no
chemical reaction; the mold cavity and the mold itself remain separate. The first mold,
made from the same silicone used to make the device, is shown in Figure 4.1.
Figure 4.1: Silicone Mold Cavity
44
The cavity for the mold in Figure 4.1 was designed to be just a generic rectangular
shape with length, width, and height dimensions the same as the HUOs. Although this
mold cavity served its initial intended purpose, it did not prove practical as a permanent
material for the mold cavity. The first problem was that the silicone mold cavity was
non-rigid. In addition to the flexibility of the mold, a problem existed because it was
difficult to add detailed features to the mold cavity. This method was sufficient for
making simple shapes (like rectangular cavities), but would prove impossible to add any
design details, such as the cavity for Dacron infusion.
A mold cavity material needed to be found that was not only rigid, but capable of
being designed into detailed and intricate shapes. The next approach used a rapid
prototyping method known as Fused Deposition Modeling (FDM). FDM can be used in
conjunction with modeling software to create three-dimensional parts from acrylonitrile
butadiene styrene (ABS) thermoplastic. In this project, a solid model of the desired final
product was made in the modeling software SolidWorks. After the part was modeled, a
mold cavity was modeled by subtracting the volume of the part from a solid mold cavity
shape. The negative that is left behind from this subtraction results in a mold cavity with
the same shape as the part. The image seen in Figure 3.13 was a mold cavity made from
the FDM procedure.
Cavities made from the FDM procedure proved to be very advantageous for this
application. There were three main advantages. First, the FDM machine automatically
created the blueprint necessary for 3D modeling from SolidWorks part files. All that the
user needed to do was design the part in SolidWorks, after which the software converted
45
it into the proper format for 3D FDM modeling. Second, the FDM machine is capable of
creating features on the size scale of about 0.1 mm. This allows for the addition of fine
details, such as the Dacron cavity. Third, the machine can produce a prototype mold in a
few hours. Whenever modifications to the mold cavity were required, a new cavity was
created and ready to use within a day. The FDM produced ABS plastic mold cavity was
used for a good portion of the experimental procedure. It was not until later in the design
process that the mold cavity was machined out of aluminum. This is discussed in more
detail in section 4.3
4.2 Process Development
To begin the process development, a simple rectangular mold cavity was designed in
SolidWorks and prototyped in the FDM machine. Figure 4.2 shows the solid model of
one of the mold halves. This model was a rectangular piece with filleted edges and a
material injection site.
Figure 4.2: Initial FDM Mold
46
Initially, the intent was to use a syringe pump to inject the silicone into the mold
cavity at the injection site. The liquid silicone was poured into a syringe. The syringe
was connected to one end of a tube, and the other end of the tube was inserted into the
injection site. This setup is shown in Figure 4.3.
Figure 4.3: Injection Method
The extremely high viscosity of the liquid silicone caused two problems with the
injection method. First, it was difficult to get the material to flow from the syringe,
through the tube and into the mold cavity. Even when attempting to use larger diameter
hoses, the pressure exerted on the setup from the forced flow caused many mechanical
failures to the procedure, such as leakage at the hose ends or mechanical breakdown of
the syringe pump.
The second problem caused by the high viscosity of the material was the resistance of
the material to separate inside the mold cavity. The goal was to coat only the walls of the
mold cavity with the silicone, creating a void in the center of the cavity. Using an
47
injection method, however, the material never separated by itself; instead, the material
congealed into a solid mass, filling a portion of the mold cavity.
The next approach was to develop a procedure that assisted in the development of the
desired internal void. The first attempt at this approach was to modify the exit port of a
syringe to match the desired shape and thickness of the front and back faces of the device
(width = 11 mm, thickness = 1 mm). With the modified syringe, the silicone was
manually added to each half of the mold in a consistent, uniform manner. This modified
syringe was modeled and manufactured using the same FDM procedure for making the
mold cavities. Figure 4.4 and Figure 4.5 show the modified syringe and its exit port,
respectively.
Figure 4.4: Modified Syringe
48
Figure 4.5: Exit Port of Syringe
Although this idea seemed like a viable option, the modified syringe was not
consistent at outputting a uniform single layer of silicone, 1 mm thick. Similar to using
the syringe pump, typical results were congealed masses of silicone with no uniformity or
internal void.
The next method that was tried was the simplest in concept, however, it produced the
most repeatable and successful outputs. The walls of both mold halves were coated with
liquid silicone using a simple paint brush. If the volume of material added was controlled
well enough, the silicone would stick to the walls of the mold cavity and cure without
combining with silicone on the opposite wall, leaving behind the desired void.
Using the mold cavity modeled in Figure 4.2 and the brushing procedure described
above, devices were produced with the desired internal voids. Two examples of devices
with internal voids are shown below in Figure 4.6 and Figure 4.7.
49
Figure 4.6: Successful Void A
Figure 4.7: Successful Void B
As seen in the figures, the procedure results in a sealed device with an internal void
(the device in Figure 4.7 had been cut open, so it appears empty whereas the device in
Figure 4.6 is filled with air). A common problem with both devices is that the wall
thickness is highly non-uniform. Both devices show a buildup of silicone at the bottom
50
of the device. Because the silicone resin requires up to twenty hours to cure, if the mold
is left stationary, the material will collect in the bottom of the mold cavity.
To eliminate the variation in wall thickness due to gravity, trials were done in which
the mold was manually rotated every few minutes for the first 10 hours of the cure
process. This rotation did in fact eliminate the buildup of material at the bottom face, and
two examples of these trials are shown in Figure 4.8 and Figure 4.9. In Figure 4.9, the
device is shown cut open in order to see the internal shape of the void. At this point in
the process development, the volume of material used in fabrication was not yet
standardized, so each device appears to have different wall thicknesses. The focus here
was the uniformity of wall thickness of each individual device. It is easily seen in Figure
4.8 that the top wall thickness is approximately the same as the bottom wall thickness. In
these figures, red die was added to the silicone in an attempt to better see the voids that
were being created.
Figure 4.8: Device with Improved Uniformity of Wall Thickness
51
Figure 4.9: Sliced Open Device with Improved Uniformity of Wall Thickness
These results showed that rotating the object while it is curing would alleviate the
negative effects caused by gravity, creating a more uniform wall thickness in the device.
To accomplish this, a device known as a gimbal mount was designed and machined. A
gimbal is a device that is pivoted at two ends and allows the rotation of an object about a
single axis. Rotation about multiple axes can be accomplished by designing a gimbal
within a gimbal, with the axis of each gimbal perpendicular to the other.
The gimbal that was made for this experiment was designed to house the mold cavity
of the HUOs and rotate it on two of its three axes. The first step was to find motors that
were capable of rotating the heavy aluminum apparatus yet relatively slow; the goal of
the rotation was not to create a centrifugal effect, but to slowly rotate the mold during
curing to alleviate the effects of gravity. The motor used, shown in Figure 4.10, is a 12
VDC capable of rotating at speeds up to 5 RPMs. The motor itself is very powerful, and
52
the slow speed is achieved by slowing down the motor with a worm gear driving a four
gear train.
Figure 4.10: 5 RPM 12 VDC Motor
Once the motors were obtained, they were measured and modeled in SolidWorks
(Figure B 13) and the gimbal device was designed to incorporate their specific shape.
The gimbal, whose design is shown in Figure 4.11, was machined from 1.5” x 1.25”
aluminum stock, and the base was made from a flat sheet of 0.5” thick aluminum. The
figures in appendix B show the dimensioned drawings of each part of the gimbal, and
Figure 4.11 is an assembly drawing of the device.
53
Figure 4.11: Assembly Drawing of Gimbal Device
One of the challenges of designing the gimbal device was supplying power to the
motor on the inner ring. One of the motors is mounted to the stationary frame of the
device and rotates the outer ring about the vertical axis. Supplying power to this motor is
trivial. The problem comes about when trying to power the motor that rotates the inner
ring. This multi-axial rotation is accomplished because the motor that causes the inner
ring to rotate is mounted to the rotating outer ring. Supplying constant power to a
rotating motor is challenging, but was achieved by developing a brush and copper ring
power system.
54
The brush and ring system uses brushes from power hand drills. These brushes, a
coiled copper wire with a graphite head, were mounted in a housing designed and
machined specifically for this purpose. These housings, shown in Figure B 17, were
designed to be mounted on the bottom of the inner ring of the gimbal. The top of the
housing has a screw hole, and the screw hole terminates at the bottom of the housing in
the shape of the graphite head of the brush. The shape of the brush is a small rectangle;
machining this shape was accomplished with the use of a wire EDM machine.
Next, a conductive material was needed to keep contact with the rotating brush. The
copper rings were machined using an abrasive waterjet machine; these drawings are
shown in Figure B 15 and Figure B 16. One brush/ring system provided current for the
positive terminal of the motor, with the other brush/ring system used for ground. Each
terminal of the motor is connected to the brush housing, which is insulated from the rest
of the gimbal device by a small piece of non-conductive plastic. A setscrew is placed in
the top of the housing, and tightening of the setscrew uses compression to keep contact
between the graphite brush head and the copper ring. The copper rings, also insulated
from the rest of the gimbal, are then connected to the positive and ground ports of the 12
VDC power supply.
The next challenge was to supply heat to the mold cavity during the curing process.
The entire gimbal apparatus itself could not simply be placed in an elevated environment
because it was not known if the motors were able to withstand elevated heat
(approximately 130° F) for extended periods of time. The first attempt at applying
location-specific heat was to create a heating pad using an insulating material and a
55
nichrome wire. Nichrome wire is ideal for supplying heat due to its high electrical
resistivity. When current is passed through the nichrome wire, the high resistivity
opposes the flow of the electric current, which in turn heats up the wire.
The amount of heat output by the nichrome wire is a function of the diameter of the
wire, the length of the wire, and the supplied current. Since the diameter is constant,
elevated temperatures can be reached by increasing the length of the wire in the system or
the current being supplied. To increase the length of the wire, the nichrome was coiled.
This coiled wire was then glued in a horizontal pattern into a pocket machined into a
piece of highly insulating ceramic using a high temperature epoxy. The current was
applied to the system by connected the ends of the nichrome wire to a disposable 12 V
battery. The entire system was then mounted to the mold cavity housing of the gimbal.
Although the nichrome wire heater elevated the temperature of the mold cavity
housing, it did not elevate it to high enough temperatures to be effective at improving the
flow of the silicone during curing. Thus, an alternative method for supplying heat to the
mold was needed that was capable of elevating the temperature up to 150° F.
A heat gun is a device that is capable of supplying heat across small distances by
generating a flow of hot air. Using a thermocouple, it was determined that at 9 inches
(measured from the nozzle of the heat gun to the center of the gimbal device) the heat
gun used in these trials was able to elevate temperatures to 116° F and 131° F on its low
and high settings, respectively. The heat gun was then placed 9 inches away from the
gimbal device and aimed at the rotating mold cavity. This set up, shown in Figure 4.12,
56
elevated the mold cavity during curing to high temperatures but did not elevate the
temperature of the motors.
Figure 4.12: Gimbal and Heat Gun Molding Setup
4.3 Evolution from HUO to Generic Silicone Balloon
Now that a procedure was developed, HUOs could be consistently made using the
apparatus shown in Figure 4.12 and the mold cavity shown in Figure 3.13. Figure 4.13,
Figure 4.14, and Figure 4.15 show examples of the HUOs that were made using this
procedural setup. The HUO in Figure 4.13 excludes the Dacron infusion and the
injection port seen in Figure 4.14 and Figure 4.15.
57
Figure 4.13: HUO with no Dacron or Injection Port
Figure 4.14: HUO with Dacron and Injection Port (A)
58
Figure 4.15: HUO with Dacron and Injection Port (B)
These HUOs were successfully created with the existence of an internal void, and the
HUOs in Figure 4.13 and Figure 4.14 created completely sealed voids. With the current
setup, approximately 50% of HUOs being made were successfully creating an internal
sealed void. Controlling the fabrication and shape of the internal void at these small
scales (40 x 11 x 3 mm) proved to be very difficult. The next step in the design process
would be to determine what factors affect the uniformity of the HUOs. However, with
only a 50% yield it is difficult to make conclusions about variables because of the
inconsistency of the devices.
In order to be able to better understand the parameters that affect the production of
the devices, a new mold was designed that was twice as wide and twice as thick as the
original occluder mold (40 x 22 x 6 mm). The idea here was to create a mold cavity of
similar shape that would give a much higher percentage of viable devices with
59
completely enclosed voids. Having a higher yield would better facilitate the investigation
into what factors specifically affect the molding of the devices.
Figure 4.16 and Figure 4.17 show the old and new mold cavities, respectively. The
old mold cavity was made from plastic in a rapid prototyping machine, while the new
mold was machined from aluminum. The thermal diffusivity of aluminum is much
greater than the thermal diffusivity of the plastic material. Having a mold cavity made
from a material with a high thermal diffusivity allows for an even distribution of heat to
the mold while it is curing, as opposed to the insulating effect that was occurring due to
the plastic material of the mold.
Figure 4.16: Plastic Mold Cavity
60
Figure 4.17: Enlarged Aluminum Mold Cavity
In the cavity in Figure 4.17 there exists a recess along the edges of each mold half.
When the mold was first machined these did not exist. The problem observed was that
the material was having trouble fusing at the weld lines (the weld lines exist at the plane
where the two mold halves meet). Figure 4.18 shows an example of the first few devices
that were made using the new mold cavity. As seen in the figure, the device did not fuse
at the edges (centerline of the side walls) of the mold halves.
61
Figure 4.18: Weld-line Issue
To solve this issue, small 0.001” deep recesses were machined into each half of the
mold at the edges. This gave the material extra surface area to stick to, and trials using
this modified mold cavity proved it to be a solution to the weld-line issue. After molding
is complete, the 0.002” thick flange can be trimmed away if desired. Figure 4.19 is an
example of a completely sealed void using the mold cavity in Figure 4.17. In this figure,
the flanges can be seen around the edges of the device.
62
Figure 4.19: Repeatable Sealed Silicone Balloon
63
Chapter 5: Optimization Strategy
5.1 Full Factorial Experiments
A full factorial experimental design is a well-established statistical method for
optimizing a product or process by evaluating the effects and interactions of variables
that affect the output variable of interest. For the purposes of this research, a full factorial
experiment was designed and implemented to determine how certain parameters affect
the successful fabrication of the silicone balloon in Figure 4.19, using the mold cavity in
Figure 4.17. A successful outcome in this case is defined as a combination of full
enclosure of the molded cavity, along with uniformity of wall thickness.
The designed experiment is known as a 2k experiment (8), where k describes to the
number of treatments. A treatment is a variable being tested that is assumed to affect the
outcome of the trial. Each of the different treatments is constrained to only two levels,
denoted in this experiment as ‘+’ or ‘-‘; a total of three treatments are evaluated in this
factorial experiment. Thus, this experiment is defined as a 23 experiment, resulting in a
total of 23 = 8 combinations of treatments and treatment levels. For this experiment, each
treatment level combination was run twice, resulting in a total of 16 runs.
64
5.2 Developing Treatments and Treatment levels
The next step in the experimental design process was to develop the treatments that
would be tested. Each treatment was known or thought to affect the output success based
on trials prior to the factorial experiment development. After treatments were selected,
treatment levels needed to be defined. This experiment is designed to include only two
levels for each treatment, so a ‘+’ and a ‘-’ level needed to be developed for each
treatment.
There were a number of possible variables that could be considered treatments for the
experimental design:
Gimbal rotational speed
Silicone mixture composition
Orientation in gimbal
Heat added to the system
Each of these possibilities was investigated independently to determine if they could or
should be defined as a treatment in the factorial experiment design.
The first variable investigated was the rotational speed of the gimbal device. The
gimbal was initially designed to spin at very low RPMs. The intention was not to hold
the silicone to the walls by centrifugal force, but instead to use slow rotation of the mold
to negate the effects of gravity and help maintain wall thickness uniformity. However,
this is not to say that a higher RPM and a centrifugal effect could not help improve the
success of the outputs.
65
In the present case, the gimbal works specifically with the motors it was designed to
use, and these motors have a low maximum rotational speed. The motor speed is directly
related to the supplied voltage across the terminals. The maximum voltage rating for
these motors is 12 volts, which corresponds to a slow rotational speed of 5 RPMs.
Since it is already known from prior testing that rotation is beneficial, a rotational
speed treatment with treatment levels of 0 RPMs and 5 RPMs would not add any value to
the experiment. Also, since 5 RPMs is already a slow revolution speed, not much
information would be gained by experimentally testing against two slow speeds, such as
2.5 and 5 RPMs. It might well be useful to test slow speeds against relatively much
higher speeds, on the order of 5 RPMs and 25 RPMs. However, due to the rating of the
motors and the design of the gimbal, speeds of 25 RPMs are not obtainable. This option
as a treatment level is definitely valid, and is discussed in further detail in the future work
section concluding this report.
The next variable investigated as a possible treatment level was the chemical
composition of the two-part platinum cure silicone rubber. The standard mixing ratio of
the A and B components is 1:1 by volume or weight. It was hypothesized that modifying
the mixture ratio would change the properties of the material, and some of these changes
may prove to be advantageous to the molding procedure.
To test this hypothesis, three different samples of silicone were molded. Each of the
samples was identical except the composition ratio of the A and B components. Two
grams of total silicone were molded into a simple rectangular mold cavity. The first
66
sample was the control, with an A:B composition of 1:1 grams. The second sample had a
composition of 0.9:1.1 grams, and the third sample had a composition of 1.1:0.9 grams.
Each mixture was molded in a separate but identical mold cavity and allowed to
solidify for 24 hours. Twenty-four hours is long enough to allow the curing process to
take place; earlier trials have shown that the mixture will completely cure in less than at
least 19 hours at room temperature, with a 1:1 composition ratio. After the 24-hour
period, the control sample had completely cured and behaved as expected. Both
experimental samples, however, were slightly tacky as though the curing process was not
complete. The samples were given an addition 24, then 48 hours to solidify. Even after
72 hours, though, there was still a slight tacky texture to the molds and no apparent
strength advantage in comparison to the silicone with a 1:1 composition ratio.
The problem is that there is a finite amount of platinum catalyst that exists in the A
component to cause the reaction of part A with an equal amount of part B. Whether there
was more A than B or more B than A, excess material remained that had nothing to react
with to cause the curing process. For this reason, chemical composition is not a valid
treatment option for the full factorial experiment with the platinum cure silicone being
used. Alternative materials, however, are a valid treatment and are discussed in the
future work section of this report.
The next variable investigated was the orientation of the mold cavity within the
gimbal device. Figure B 11 shows the compartment of the gimbal designed to hold the
mold cavity. The design intended for the longest edge of the mold cavity to be parallel
67
with the axis of rotation of the inner ring. With this orientation, shown in Figure 5.1, the
edge of the mold cavity was flush with the edge of the mold cavity compartment.
Figure 5.1: Mold Cavity Horizontally Oriented in Gimbal
The gimbal is designed to rotate the object within the mold cavity compartment about
2 of its 3 axes. Experiments were first done to determine if orientation differences, while
keeping the axes of rotation the same, would noticeably affect the output. Multiple
devices were molded in the orientation depicted in Figure 5.1, making sure to keep the
same mold half facing upward each time. Then, a new set of devices was molded with
180° rotation, rotating about the same 2 axes (this would look identical to Figure 5.1
except the mold halves would be on opposite sides of the compartment). After molding
was complete, each group of devices was compared and no noticeable differences were
found between the two sets (mold-half was identifiable because a small, .0005” circular
68
indentation was machined into the face of one of the mold halves. This mark is small
enough not to affect the overall shape or volume of the device, yet allows identification
of mold half).
The next step was to determine the effect of orientation when comparing rotation
about different axes. To accomplish this, a group of devices were molded with the
orientation depicted in Figure 5.1, and a second group of devices were molded with the
‘vertical’ orientation depicted in Figure 5.2. One set allows rotation about the x and y
axes of the device, while the other allows rotation about the y and z axes. When
comparing the molded devices from each group, there was a distinctly noticeable
difference in the success of the device, in terms of both degree of enclosure and
uniformity of wall thickness. For this reason, horizontal versus vertical orientation was
chosen to be a treatment for the full factorial experiment. The treatment is labeled
treatment B, with B+ referring to the vertical treatment level and B- referring to the
horizontal treatment level.
69
Figure 5.2: Mold Cavity Vertically Oriented in Gimbal
The next and possibly most critical treatment that was investigated was the addition
of heat into the process. Adding heat can be advantageous because it has the effect of
decreasing the viscosity of the extremely viscous silicone. It can hinder the process,
however, by drastically reducing the cure time of the reaction. Heat can be added at
many different stages in the molding process, and can be added to many different
components of the process. A total of three different types of heat addition were
investigated, and each possibility was tested separately.
The first test was to determine if heating the mold cavity prior to the addition of the
liquid silicone would be a valid treatment level. To accomplish this, the mold cavity was
heated to approximately 110°F using a hot water bath. Once removed, the mold cavities
were dried of any excess water, filled with silicone and placed in the gimbal for the
curing process. The devices made with this process were not at all successful. First,
70
there was almost no closure at the weld lines, which resulted in two separate pieces from
each molding run. This result indicated that the silicone was curing so quickly, no
welding was occurring between the two mold halves. Second, the front and back faces of
the device were not smooth like that shown in Figure 4.19, but wavy and inconsistent. It
was determined that heating the mold cavity reduced the cure time too much, not
allowing the silicone the necessary time to flow and evenly distribute around the walls of
the cavity. For this reason, heating the mold cavity was determined not to be a valid
treatment level.
Next, tests were done to see if heating the silicone material prior to putting it into the
mold cavity could have any advantageous effects. First, the two silicone components
were mixed in an aluminum tray, and the tray was then placed in a hot water bath. After
5 to 10 minutes of heating, the tray was removed but it was found that the silicone had
already begun to solidify. It was determined, then, that mixing the components prior to
heating the material reduces the cure time below the required work time, and for that
reason was not considered a valid treatment option.
The next possible treatment option tested was the addition of heat to the separate A
and B silicone components prior to mixing. Part A of the silicone is the extremely
viscous component, and it is easily found by inspection that adding heat to isolated part A
drastically reduces its viscosity. The hope is that heating the components separately will
take advantage of the increased flow results without reducing the cure time to an
unworkable level. Devices molded under these conditions showed that addition of heat
prior to the pre-mixing stage of the process would be a valid treatment. This treatment
71
was labeled treatment C, with C- referring to the treatment level of no heat added at the
pre-mixing stage and C+ referring to the treatment level with the addition of the heat.
The final possible treatment investigated was the addition of heat during the curing
process. It was already determined that addition of heat at this stage was advantageous to
the uniformity of the molding, and the set up of each treatment level using a heat gun was
described in the process development section of this report. This treatment was labeled
treatment A, and A- refers to a treatment level with the heat gun on the cold setting
(approximately 116° F at 9 inches) and A+ refers to a treatment level with the heat gun
on the hot setting (approximately 131° F at 9 inches).
Figure 5.3 is the experimental matrix for the full factorial experiment. Each treatment
and treatment level is represented, giving a total of 23 = 8 different process conditions to
test.
B:
Orientation
B+
B-
A: Temperature
A+
AA+B+C+ A-B+C+
A+B+CA-B+CA+B-C+
A-B-C+
A+B-CA-B-C-
C+
CC+
C-
C: Pre-Heat
Figure 5.3: Experimental Matrix for Full Factorial Experiment
5.3 Running the experiments
The full factorial experiment was run over the course of a few weeks. Each of the 8
process conditions was tested twice to show consistency and repeatability. Table 5.1
72
displays the full factorial design. Each row describes one of the eight process conditions.
The second and third columns show the order in which the runs were performed, both of
which were determined by a random number generator. Each set is run separately, and
column two is completed before column three begins.
Table 5.1: Full Factorial Design
Run
1
2
3
4
5
6
7
8
Rand1
3
7
1
6
4
2
5
8
Rand2
13
10
11
14
12
9
16
15
A
+
+
+
+
-
B
+
+
+
+
-
C
+
+
+
+
-
AB
+
+
+
+
AC
+
+
+
+
BC
+
+
+
+
ABC
+
+
+
+
-
Columns four, five, and six show the treatment levels for the treatments A, B, and C,
respectively. Columns seven, eight, and nine show coefficients for evaluating
interactions between two different treatments, and column ten shows the coefficient
evaluating the interaction of all three treatments. These treatment coefficients work with
algebraic rules. Two positives or two negatives result in a positive coefficient, while one
positive and one negative result in a negative coefficient.
Appendix C describes how each run was performed. The appendix will discuss the
experimental set up, how to measure and mix the components, and how to apply the
silicone to the mold cavity. This section of the report (section 5.3) focuses specifically
on each treatment and setting up for the different treatment levels.
73
For each run, the appropriate treatment levels corresponding to the full factorial
design table had to be applied. Applying the different levels for treatment A was simple
– the heat gun was permanently set up as a part of the molding device, shown in Figure
4.12. The distance between the gimbal and the heat gun remained the constant 9 inches,
and switching from the hot (A+) condition to the cold (A-) condition was accomplished
by turning a knob to cover or uncover the exhaust on the heat gun.
Treatment B describes the orientation of the mold cavity in the gimbal, and switching
between treatment B levels is also very easy. To keep top, bottom, left and right of the
molded device consistent throughout the experiment, the mold cavity was placed in the
gimbal in the same orientation for each respective treatment levels. When the horizontal
(B-) treatment level was used, the edge of the device with the tube faced forward and the
mold half with the screw heads exposed faced upwards, as depicted in Figure 5.4. The
‘front’ of the mold cavity compartment is defined as the open side (as opposed to the side
of the rotating axle), and the ‘top’ of the compartment is defined as the face with the
setscrew holes. When the vertical (B+) treatment level was used, the mold cavity was
always oriented as depicted in Figure 5.5. As the figure shows, the mold cavity is
secured on the right setscrew, with the tube facing to the left and the mold half with the
setscrews exposed facing upwards.
74
Figure 5.4: Orientation of Mold Cavity in Compartment for B- Treatment Level
Figure 5.5: Orientation of Mold Cavity in Compartment for B+ Treatment Level
75
Treatment C referred to adding heat to the silicone prior to the curing stage. If the
treatment level C- was used, the silicone was not heated, just mixed at room temperature.
If the treatment level C+ was used, the two silicone components needed to be heated prior
to mixing. To heat the silicone, the two components were placed in separate
compartments of an aluminum mixing tray. The tray used in the experiment had 6
compartments, and one of the spare compartments was filled with tap water and used as
the reference temperature. The aluminum mixing tray was placed in a thin layer of hot
water. The temperature of the water in the mixing tray was monitored, and the mixing
tray was allowed to heat up until the water reached a temperature of 110° F. The
temperature of the silicone components could not be measured directly because in doing
so some of the component would stick to the thermometer, and the mass of each
component is very critical to the success and validity of the experiment. Because water
and the silicone components have different chemical properties, it cannot be assumed that
they will heat up in the same manner and that the silicone is assumed to be at 110° F
when removed from the water bath. What is important here, however, is consistency. It
is important that we use an elevated temperature for the C+ treatment level, and for
validity this elevated temperature should be consistent throughout the entire experiment.
5.4 Full Factorial results
Two devices were run under each of the 8 treatment level combinations, resulting in a
total of 16 devices. First, the standard deviation of the mass and the volume of the
experimentally created devices were compared to the results of the handmade HUO
76
measurements displayed in Figure 1.4 and Figure 1.5. Then, the success of each
individual device was determined by evaluation of three different parameters; enclosure,
visual uniformity, and wall thickness uniformity. Each of these three evaluation
parameters are described below, followed by figures displaying the results of the
experiment.
Section 1 of this report described the standard deviation from the average mass and
average volume for 10 handmade HUO devices. The standard deviation of mass of the
handmade HUOs was found to be 0.0786 grams. This is a very small standard deviation,
showing that the handmade HUOs are consistent in terms of mass. The mass of the
experimentally created devices was controlled by the molding procedure. Appendix C of
this report explains this procedure, which involves mixing precisely 1.85 grams of each
silicone component. The mass of each molded device, then, can expected to be very
close to 3.7 grams, with any small variation occurring due to slight inconsistencies in the
brushing method of applying the silicone to the mold cavity.
Section 1 of this report also describes the standard deviation from the average volume
of for the 10 handmade HUOs. Although the SD of the mass was very low, the standard
deviation from the average volume was not. The average volume of the handmade HUOs
was 1.71 mL, with a standard deviation of 0.2025 mL. This SD is approximately 11.8%
the magnitude of the average volume, which is significant. The benefit of using a rigid
mold cavity for producing the devices is that the volume is restricted and controlled. This
volume restriction will ensure that the volume of the experimentally created devices
remains constant, and any standard deviation would be negligible.
77
The next step was to determine the success of each experimental run. The first
parameter defining success was the extent of enclosure of the device. Ideally, the devices
would be completely enclosed with only a single inlet/exit pathway occupied by the
silicone tube. This tube can also be used to test for enclosure; blowing air into the open
end of the tube will identify any leaks or open seams. If the device was fully sealed, it
was given an enclosure value of 3. If the device was not sealed at the weld lines (Figure
4.18), it was given an enclosure value of 1. An enclosure value of 2 describes devices
that appeared entirely sealed, yet showed small leaks when filled with air. Typical
devices with an enclosure value of 2 had small holes where fluid could leak out, but did
not have large open seams like the devices with an enclosure value of 1. Table 5.2
displays the occluders and their enclosure values.
Table 5.2: Enclosure of Experimental Devices
Parameters
Run Set 1
Run Set 2
Run Set 3
Run Set 4
Run Set 5
Run Set 6
Run Set 7
Run Set 8
Occluder
3
13
7
10
1
11
6
14
4
12
2
9
5
16
8
15
78
Enclosure
3
3
3
3
3
3
3
2
1
2
3
1
2
3
3
3
The next evaluation parameter used to define the success of each device was its
uniformity based in visual inspection. Each device was examined, focusing on the
uniformity of the shape of the internal void. Devices with a uniform internal void were
given a visual value of 3, while devices that did not have a uniform internal void were
given a visual value of 2 or 1. Figure 5.6 shows an example of a visual value of 1, 2, and
3, and Table 5.3 displays the occluders and their visual values.
Figure 5.6: Visual Uniformity Values (from left to right) of 1, 2, and 3
79
Table 5.3: Visual Uniformity of Experimental Devices
Parameters
Run Set 1
Run Set 2
Run Set 3
Run Set 4
Run Set 5
Run Set 6
Run Set 7
Run Set 8
Occluder
3
13
7
10
1
11
6
14
4
12
2
9
5
16
8
15
Visual
1
3
1
1
3
2
3
3
1
2
1
1
3
3
2
3
The final parameter that was used to determine the success of each device was to take
measurements of the wall thickness along the front and back faces of each device. Three
measurements were taken on each face, totaling 6 measurements for each occluder. The
first measurement was taken at the left edge, the second taken at the middle, and the third
taken at the right edge. Then, these wall thicknesses were plotted to visually show
uniformity. Figure 5.7 to Figure 5.14 show these plots for each parameter set, along with
their corresponding enclosure and visual values. Each plot contains a total of 4 curves; a
front and back face for each of the two occluders with the specified parameters. The
parameters of each of the 8 runs can be found at the top of the plot for each figure.
80
A: Hot
B: Vertical
C: Preheat
Occluder 3 Front
Occluder 3 Back
Occluder 13 Front
Occluder 13 Back
Thickness (in)
0.1
0.05
0
1
2
3
Measurement Location (1-Left, 2-Center, 3-Right)
Occluder
3
13
Enclosure
3
3
Visual
1
3
Figure 5.7: Parameter Set 1
81
A: Hot
B: Vertical
C: No preheat
Occluder 7 Front
Occluder 7 Back
Occluder 10 Front
Occluder 10 Back
Thickness (in)
0.1
0.05
0
1
2
3
Measurement Location (1-Left, 2-Center, 3-Right)
Occluder
7
10
Enclosure
3
3
Visual
1
1
Figure 5.8: Parameter Set 2
82
A: Hot
B: Horizontal
C: Preheat
Occluder 1 Front
Occluder 1 Back
Occluder 11 Front
Occluder 11 Back
Thickness (in)
0.1
0.05
0
1
2
3
Measurement Location (1-Left, 2-Center, 3-Right)
Occluder
1
11
Enclosure
3
3
Visual
3
2
Figure 5.9: Parameter Set 3
83
A: Hot
B: Horizontal
C: No preheat
Occluder 6 Front
Occluder 6 Back
Occluder 14 Front
Occluder 14 Back
Thickness (in)
0.1
0.05
0
1
2
3
Measurement Location (1-Left, 2-Center, 3-Right)
Occluder
6
14
Enclosure
3
2
Visual
3
3
Figure 5.10: Parameter Set 4
84
A: Cold
B: Vertical
C: Preheat
Occluder 4 Front
Occluder 4 Back
Occluder 12 Front
Occluder 12 Back
Thickness (in)
0.1
0.05
0
1
2
3
Measurement Location (1-Left, 2-Center, 3-Right)
Occluder
4
12
Enclosure
1
2
Visual
1
2
Figure 5.11: Parameter Set 5
85
A: Cold
B: Vertical
C: No preheat
Occluder 2 Front
Occluder 2 Back
Occluder 9 Front
Occluder 9 Back
Thickness (in)
0.1
0.05
0
1
2
3
Measurement Location (1-Left, 2-Center, 3-Right)
Occluder
2
9
Enclosure
3
1
Visual
1
1
Figure 5.12: Parameter Set 6
86
A: Cold
B: Horizontal
C: Preheat
Occluder 5 Front
Occluder 5 Back
Occluder 16 Front
Occluder 16 Back
Thickness (in)
0.1
0.05
0
1
2
3
Measurement Location (1-Left, 2-Center, 3-Right)
Occluder
5
16
Enclosure
2
3
Visual
3
3
Figure 5.13: Parameter Set 7
87
A: Cold
B: Horizontal
C: No preheat
Occluder 8 Front
Occluder 8 Back
Occluder 15 Front
Occluder 15 Back
Thickness (in)
0.1
0.05
0
1
2
3
Measurement Location (1-Left, 2-Center, 3-Right)
Occluder
8
15
Enclosure
3
3
Visual
2
3
Figure 5.14: Parameter Set 8
88
Chapter 6: Conclusions and Future Work
6.1 Conclusions
The results of the full factorial experiment show not only how each parameter affects
the success of the device, but also how the interactions amongst different parameters
affect the success of the device. This section will discuss the results found and displayed
in Figure 5.7 through Figure 5.14. It will begin by discussing each parameter
individually, followed by a discussion of the interactions of the parameters.
The first parameter in question was denoted as parameter ‘A’, referring to the heat
added to the system during the curing process. The ‘hot’ (A+) and ‘cold’ (A-) treatment
levels indicated a cure temperature of approximately 131°F and 116°F, respectively.
Figure 5.7 through Figure 5.10 display the results using the A+ condition, while Figure
5.11 through Figure 5.14 display the results using the A- condition. From the results it
appears that overall, the elevated (A+) cure temperature condition produced more
uniform results. These results are shown not only graphically (in the plots of Figure 5.7
through Figure 5.14), but also in Table 6.1 which shows the average numerical values for
enclosure and visual success parameters. The elevated temperature lowered the viscosity
of the silicone mixture, allowing the material to flow and coat the walls in a more
uniform manner.
89
Table 6.1: Average Enclosure and Visual Output Values for Treatment A
Treatment Level
A+
A-
Enclosure
2.875
2.25
Visual
2.125
2
The next parameter in question was treatment level ‘B’, referring to the orientation of
the mold cavity in the gimbal device. The treatment levels were labeled vertical (B+,
Figure 5.2 and Figure 5.5) and horizontal (B-, Figure 5.1 and Figure 5.4). In the results
section, Figure 5.7, Figure 5.8, Figure 5.11, and Figure 5.12 show the success of devices
with the vertical treatment level, while Figure 5.9, Figure 5.10, Figure 5.13, and Figure
5.14 used the horizontal orientation. The results clearly indicate that the horizontal
orientation produced more uniform results than the vertical orientation. The figures that
show the results of a vertical orientation have an ‘L’ shape, with one end of the device
much thicker than the other end and the middle. The end with the larger wall thickness
was always the end hanging outside of the mold cavity (seen in Figure 5.2 and Figure
5.5). This is due to the fact that this portion of the mold cavity is more directly exposed
to the elevated temperatures from the A treatment parameter. This exposure causes the
silicone in this area of the mold cavity to solidify quicker than the rest of the mold,
creating the greater wall thickness. Table 6.2 shows the average values of the enclosure
and visual parameters for the two treatment levels. As the table shows, the B- treatment
level produced better results.
90
Table 6.2: Average Enclosure and Visual Output Values for Treatment B
Treatment Level
B+
B-
Enclosure
2.375
2.75
Visual
1.375
2.75
The final parameter in question was treatment level ‘C’, which referred to preheating
the silicone prior to the filling the mold (C+, Figure 5.7, Figure 5.9, Figure 5.11, and
Figure 5.13) versus no preheating (C-, Figure 5.8, Figure 5.10, Figure 5.12, and Figure
5.14). As discussed, adding heat to the silicone at any stage in the molding procedure
decreases the viscosity of the material, but at the same time reduces its cure time. It was
initially thought that preheating the silicone would be advantageous to the process;
however, the results showed the preheating actually decreased the success of the device.
Heating the silicone prior to the mixing process may be causing the silicone to begin to
solidify before it has the opportunity to be uniformly distributed on the walls of the mold
cavity. These results are shown graphically, and the average enclosure and visual
parameters are displayed in Table 6.3. As the table shows, the average enclosure value
increased when using the C- condition, yet the average visual value actually decreased. It
was hypothesized that this effect came not from the preheat treatment, but because of the
vertical orientation (treatment level B+).
Table 6.3: Average Enclosure and Visual Output Values for Treatment C
Treatment Level
C+
C-
Enclosure
2.5
2.625
91
Visual
2.25
1.875
The final step was to determine how the interaction of each treatment level affected
the success of the output. There are a total of 8 different combinations of treatment
levels, and the average value of the enclosure and visual parameters for each treatment
level combination is displayed in Table 6.4, along with a total value displaying the sum
of the average enclosure value and the average visual value.
Table 6.4: Average Enclosure and Visual Output Values for 8 different Parameter
Combinations
Run Parameter
1
2
3
4
5
6
7
8
Enclosure
3
3
3
2.5
1.5
2
2.5
3
Visual
2
1
2.5
3
1.5
1
3
2.5
Total
5
4
5.5
5.5
3
3
5.5
5.5
As seen in the table, run parameters 3, 4, 7 and 8 had the highest summation value of
5.5 (maximum of 6). To determine the best combination, the plots of Figure 5.7 through
Figure 5.14 for the run parameters with the highest total summation value were
examined. The plots clearly indicate that of the run parameters with the highest
enclosure and visual summation values, run parameter 4 produced the most uniform
devices in terms of wall thickness (in fact, the uniformity of the wall thickness for run
parameter 4 was the best for all 8 cases, not just the cases with the highest enclosure and
visual summation value). Table 6.5 describes the treatment levels of run parameter 4,
92
which was proven to be the most advantageous combination of treatment levels from the
full factorial experiment. The devices of run parameter 4 were denoted as device 6 and
14. The plot showing the thickness of the front and back faces of these devices is shown
in Figure 6.1. Figure 6.2 and Figure 6.3 show images of devices 6 and 14, respectively.
Table 6.5: Treatment Levels Producing Most Successful Results
Treatment
Level
A
A+
B
B-
C
C-
A: Hot
Verbal Description
Heat device to approximately 131°F
during the curing stage
Orient the mold cavity horizontally in
the gimbal device
Do not preheat the silicone prior to the
curing stage
B: Horizontal
C: No preheat
Occluder 6 Front
Occluder 6 Back
Occluder 14 Front
Occluder 14 Back
Thickness (in)
0.1
0.05
0
1
2
3
Measurement Location (1-Left, 2-Center, 3-Right)
Figure 6.1: Face Thickness of Run Parameter 4
93
Figure 6.2: Run Parameter 4 - Device 6
Figure 6.3: Run Parameter 4 - Device 14
94
6.2 Future Work
This project developed a method for manufacturing completely sealed silicone
balloons in a single step process, as well as identified certain treatment levels that
resulted in more successful devices. The next step in the process would be to improve
the procedure even more by identifying other treatments and treatment levels that affect
the device output. A few of these possible future treatments are discussed in this section.
The full factorial experimental procedure showed that elevating the temperature
during the curing stage of the process produced better results. The experiment, however,
only compared the results of two curing temperatures (116dF and 131dF). The results
showed that the higher temperature was more advantageous to the process, but the next
step could be to determine the specific temperature range that will give the best results.
Because of the limitations of the motors that the gimbal was designed for, rotational
speed of the gimbal during the curing process could not be greater than 5 RPMs.
Running the device at higher RPMs, however, might prove to produce more successful
devices. A future step could be to redesign the motor plates for motors that can rotate at
higher speeds, and these results could be prepared to the results from the slow, 5 RPM
motor speed of the gimbal device.
An initial possible treatment level was to change the composition of the silicone (alter
the A:B component ratio from the standard 1:1 ratio). Tests showed, however, that
altering the standard 1:1 ratio of the DragonSkin 30 material did not provide any benefits
to the molding process. In the future, different materials could be used to mold the
95
devices, and these results can be compared to the success of the procedure using the
DS30 material.
The gimbal device was designed with one gimbal inside of another gimbal, allowing
spin about 2 of the 3 axes of the device. Rotation proved to be advantageous to the
process, so redesigning the gimbal device to spin on all 3 axes could show to improve the
overall molding procedure.
The final interesting point discovered from the full factorial experiment was that areas
more directly exposed to the ambient heat (provided by the heat gun) during the curing
stage solidified quicker, resulting in a greater wall thickness in those areas. When the
mold cavity was oriented vertically, the exposed area of the cavity (the section that did
not fit inside the mold cavity compartment) solidified too quickly and produced the ‘U’
shaped wall seen in Figure 5.7, Figure 5.8, Figure 5.11, and Figure 5.12. When the mold
cavity was oriented horizontally, the edge of the mold that was flush with the outer edge
of the mold cavity compartment solidified more quickly, resulting in a larger wall
thickness at the top (edge with the inlet/exit tube) of the device. A future step in the
process could be to redesign the mold cavity compartment so every face is insulated in
the same manner, whether the mold cavity is oriented horizontally or vertically. It is
hypothesized that having a uniform exposure to the ambient heat during the curing stage
of the process would provide more uniform wall thickness across the entire device.
96
Appendix A: MATLAB Code
97
Calculate avg. and SD of mass and volume
%Mike Hudoba
%Average mass and volume of handmade HUOs
clear all
clc
%input mass and volume data
m = [3.49 3.61 3.61 3.63 3.59 3.56 3.54 3.56 3.36 3.53]; %Mass, g
V = [1.6 1.8 2.0 1.7 1.5 1.8 1.8 1.7 1.3 1.9] %Volume, mL
%average
m_avg = sum(m)/length(m);
V_avg = sum(V)/length(V);
%Calculations for standard Deviation of m
deviations_m = m - m_avg;
deviations_m_2 = deviations_m.^2;
dev_2_sum_m = sum(deviations_m_2);
factor_m = dev_2_sum_m/(length(m)-1);
STD_m = sqrt(factor_m)
%Calculations for standard Deviation of V
deviations_V = V - V_avg;
deviations_V_2 = deviations_V.^2;
dev_2_sum_V = sum(deviations_V_2);
factor_V = dev_2_sum_V/(length(V)-1);
STD_V = sqrt(factor_V)
x = [0:.1:length(m)+1];
x2 = [1:length(m)];
%Plot m against average
figure(1)
plot(x,m_avg,'x',x2,m,'o')
title('Average mass of Handmade HUOs')
xlabel('Occluder')
ylabel('mass (g)')
axis([0 11 3.3 3.7])
grid on
%Plot m against average
figure(2)
plot(x,V_avg,'x',x2,V,'o')
title('Average Volume of Handmade HUOs')
xlabel('Occluder')
ylabel('Volume (mL)')
axis([0 11 1.1 2.1])
grid on
98
Calculate avg. and SD of lumen area
%Mike Hudoba
%Average Lumen Diameter of hand-made HUOs
clear all
clc
%input area data
A = xlsread('HUO_area.xls','K3:K12')';
%Calculations to plot horizontal average
A_avg = sum(A)/length(A);
x_avg = 0:.1:length(A)+1;
%Calculations for standard Deviation
deviations = A - A_avg;
deviations_2 = deviations.^2;
dev_2_sum = sum(deviations_2);
factor = dev_2_sum/(length(A)-1);
STD = sqrt(factor);
%X axis for plot
HUO = 1:length(A);
%Plot areas against average
plot(HUO,A,'o',x_avg,A_avg,'x')
title('Average Lumen Area of Hand-made HUOs')
xlabel('Occluder')
ylabel('Area (mm^2)')
axis([0 11 15 40])
grid on
99
Plot wall thickness of devices from full factorial experiment
%Mike Hudoba
%Occluder Measurements from full factorial
clear all
clc
%%
%Load data
HUO_1 = xlsread('Occluder_Measurements.xls','B2:I2');
HUO_2 = xlsread('Occluder_Measurements.xls','B3:I3');
HUO_3 = xlsread('Occluder_Measurements.xls','B4:I4');
HUO_4 = xlsread('Occluder_Measurements.xls','B5:I5');
HUO_5 = xlsread('Occluder_Measurements.xls','B6:I6');
HUO_6 = xlsread('Occluder_Measurements.xls','B7:I7');
HUO_7 = xlsread('Occluder_Measurements.xls','B8:I8');
HUO_8 = xlsread('Occluder_Measurements.xls','B9:I9');
HUO_9 = xlsread('Occluder_Measurements.xls','B10:I10');
HUO_10 = xlsread('Occluder_Measurements.xls','B11:I11');
HUO_11 = xlsread('Occluder_Measurements.xls','B12:I12');
HUO_12 = xlsread('Occluder_Measurements.xls','B13:I13');
HUO_13 = xlsread('Occluder_Measurements.xls','B14:I14');
HUO_14 = xlsread('Occluder_Measurements.xls','B15:I15');
HUO_15 = xlsread('Occluder_Measurements.xls','B16:I16');
HUO_16 = xlsread('Occluder_Measurements.xls','B17:I17');
%%
x = [1 2 3];
figure(1)
plot(x,HUO_3(1:3),'-o',x,HUO_3(4:6),'--o',x,HUO_13(1:3),'o',x,HUO_13(4:6),'--o')
title('A: Hot
B: Vertical
C: Preheat')
ylabel('Thickness (in)')
xlabel('Measurement Location (1-Left, 2-Center, 3-Right)')
axis([0.5 3.5 0 .15])
legend('Occluder 3 Front','Occluder 3 Back','Occluder 13
Front','Occluder 13 Back')
grid on
figure(2)
plot(x,HUO_7(1:3),'-o',x,HUO_7(4:6),'--o',x,HUO_10(1:3),'o',x,HUO_10(4:6),'--o')
title('A: Hot
B: Vertical
C: No preheat')
ylabel('Thickness (in)')
xlabel('Measurement Location (1-Left, 2-Center, 3-Right)')
axis([0.5 3.5 0 .15])
legend('Occluder 7 Front','Occluder 7 Back','Occluder 10
Front','Occluder 10 Back')
100
grid on
figure(3)
plot(x,HUO_1(1:3),'-o',x,HUO_1(4:6),'--o',x,HUO_11(1:3),'o',x,HUO_11(4:6),'--o')
title('A: Hot
B: Horizontal
C: Preheat')
ylabel('Thickness (in)')
xlabel('Measurement Location (1-Left, 2-Center, 3-Right)')
axis([0.5 3.5 0 .15])
legend('Occluder 1 Front','Occluder 1 Back','Occluder 11
Front','Occluder 11 Back')
grid on
figure(4)
plot(x,HUO_6(1:3),'-o',x,HUO_6(4:6),'--o',x,HUO_14(1:3),'o',x,HUO_14(4:6),'--o')
title('A: Hot
B: Horizontal
C: No preheat')
ylabel('Thickness (in)')
xlabel('Measurement Location (1-Left, 2-Center, 3-Right)')
axis([0.5 3.5 0 .15])
legend('Occluder 6 Front','Occluder 6 Back','Occluder 14
Front','Occluder 14 Back')
grid on
figure(5)
plot(x,HUO_4(1:3),'-o',x,HUO_4(4:6),'--o',x,HUO_12(1:3),'o',x,HUO_12(4:6),'--o')
title('A: Cold
B: Vertical
C: Preheat')
ylabel('Thickness (in)')
xlabel('Measurement Location (1-Left, 2-Center, 3-Right)')
axis([0.5 3.5 0 .15])
legend('Occluder 4 Front','Occluder 4 Back','Occluder 12
Front','Occluder 12 Back')
grid on
figure(6)
plot(x,HUO_2(1:3),'-o',x,HUO_2(4:6),'--o',x,HUO_9(1:3),'o',x,HUO_9(4:6),'--o')
title('A: Cold
B: Vertical
C: No preheat')
ylabel('Thickness (in)')
xlabel('Measurement Location (1-Left, 2-Center, 3-Right)')
axis([0.5 3.5 0 .15])
legend('Occluder 2 Front','Occluder 2 Back','Occluder 9
Front','Occluder 9 Back')
grid on
figure(7)
plot(x,HUO_5(1:3),'-o',x,HUO_5(4:6),'--o',x,HUO_16(1:3),'o',x,HUO_16(4:6),'--o')
title('A: Cold
B: Horizontal
C: Preheat')
ylabel('Thickness (in)')
xlabel('Measurement Location (1-Left, 2-Center, 3-Right)')
axis([0.5 3.5 0 .15])
legend('Occluder 5 Front','Occluder 5 Back','Occluder 16
Front','Occluder 16 Back')
grid on
figure(8)
plot(x,HUO_7(1:3),'-o',x,HUO_7(4:6),'--o',x,HUO_15(1:3),'o',x,HUO_15(4:6),'--o')
101
title('A: Cold
B: Horizontal
C: No preheat')
ylabel('Thickness (in)')
xlabel('Measurement Location (1-Left, 2-Center, 3-Right)')
axis([0.5 3.5 0 .15])
legend('Occluder 8 Front','Occluder 8 Back','Occluder 15
Front','Occluder 15 Back')
grid on
102
Appendix B: Gimbal Drawings
103
Figure B 1: Gimbal Base
Figure B 2: Gimbal BaseTop
104
Figure B 3: Gimbal BaseVert
Figure B 4: Gimbal RingHorizontal
105
Figure B 5: Gimbal RingVert1
Figure B 6: Gimbal RingVert2
106
Figure B 7: Gimbal RingShaftTop
Figure B 8: Gimbal RingShaftBottom
107
Figure B 9: Gimbal SleeveBearing
Figure B 10: Gimbal InnerShaft
108
Figure B 11: Gimbal MoldCavitySlot
Figure B 12: Gimbal MotorPlate
109
Figure B 13: Gimbal Motor
Figure B 14: Gimbal InnerBottom
110
Figure B 15: Gimbal ConductingRing
Figure B 16: Gimbal ConductingRing2
111
Figure B 17: Gimbal BrushHousing
112
Appendix C: Mold Procedure
113
C1: Preparing the mold
An important first step in the design process is preparing the mold cavity for the
process. First, the mold cavity should be adequately cleaned from any dust, dirt, or
residue from past trials. Ethyl alcohol (97%) was used to clean the mold cavity and any
equipment (mixing trays, mixing spoons, etc.) that will be used. After the mold cavity
dried, a powerful air hose was used to clean off any remaining residue.
After the mold cavity was cleaned, it was coated with a release agent to ensure a
clean separation between the mold cavity and the mold after curing. A small paintbrush
was used to apply the release agent, and care was taken to ensure that the entire surface
area was brushed with the release agent. This all was done prior to the rest of the
experiment, allowing the release agent to dry for at least 5 minutes before filling the mold
cavity with silicone.
C2: Creating the Flow Tube
The mold cavity used to carry out the experiments is designed to allow the addition of
a tube to the top of the device. This tube is used to mimic the entrance or exit valve of
the HUOs, and can also be used to help determine whether the device had full enclosure.
The tube material is a stiffer silicone, and was taken from the entrance and exit ports
of the handmade HUOs used to determine hand-made HUO uniformity. Approximately
1 inch of tube was cut for each run, and was simply placed in the recess prior to putting
the two mold halves together.
C3: Mixing of Silicone A and B Components
Ensuring the correct A and B composition of the mixture for each run is critical, as
was found when attempting to vary the 1:1 composition ratio. Each device is molded
using only 3.7 grams of silicone (1.85 grams part A and 1.85 grams part B). At such a
114
small mass of material, measurement errors on the order of one-hundredth of a gram of
either part A or part B can affect the output success.
To measure the silicone components, a digital scale with a 0.01-gram tolerance was
used. If the C- treatment level was being tested, measuring and mixing of the
components is straightforward because the two components can be weighed in the same
mixing tray. To get the proper mixture, 1.85 grams of part A is added to the mixing tray.
Then, the scale is zeroed and 1.85 grams of part B is added to part A, and then the two
components are mixed for approximately 60 seconds. If the C+ treatment level was
being tested, the components had to be heated separately so they could not be measured
in the same mixing tray. Each component would have to be measured out and heated in a
separate tray and then mixed. Since component B is less viscous than component A, the
tray containing component B was emptied into the tray of component A once the desired
temperature was reached. The problem is that there is a small amount of component B
left behind when trying to empty the tray, and accuracy of the component ratios is on the
order of 0.01 grams. To ensure a 1:1 ratio, trays were filled with component B, heated,
emptied, and then weighed to determine what mass of B is left behind when emptying it
from the mixing tray. Five trials showed that on average, 0.05 grams of component B
was left behind when emptying the mixing tray (each trial was completed using the same
equipment and the same process). To ensure a 1:1 ratio exists when the C+ treatment
level was being tested, 1.85 grams and 1.90 grams of components A and B were
measured and heated separately, after which the tray containing component B was added
to the tray containing component A. The two components were then mixed together for
approximately 60 seconds.
C4: Applying the Silicone to the Mold Cavity
Once the two silicone components are combined, the mixture is ready to be applied to
the mold cavity. Approximately half of the silicone mixture is placed in each mold half.
A small paintbrush is then used to coat the mold cavities. Care is taken to ensure that the
entire surface area is brushed, including the small 0.001” indentation at the face of each
115
mold half. It is important not to let too much silicone get between the two faces of the
mold halves, however, small amounts of flash are ok and can be trimmed away after
molding is complete.
Once the entire surface area of both mold halves is covered, the tube is placed in the
recess and the two mold halves are placed and screwed together. Immediately after the
mold halves are put together the cavity is placed in the gimbal to allow the heated curing
process to begin.
116
References
1. Adin et al. Urodynamic effects of a percutaneously controlled static hydraulic urethral
sphincter in canine cadavers. Gainesville, FL : Department of Small Animal Clinical
Sciences, College of Veterinary Medicine, University of Florida, 2003.
2. Rawlings et al. Evaluation of colposuspension for treatment of incontinence in spayed
female dogs. Athens, GA : Departments of Small Animal Medicine, Anatomy and
radiology, and Physiology and Pharmacology, College of Veterinary Medicine,
University of Georgia, 2001.
3. Adin et al. Outcome associated with use of a percutaneously controlled hydraulic
occluder for treatment of dogs with intrahepatic portosystemic shunts. Gainesville, FL :
Department of Small Animal Clinical Sciences, College of Veterinary Medicine,
University of Florida, 2006.
4. Coe, Lubomry I. Kuzmak and Frederick L. Gastric Banding Device. 4592339
United States of America, June 3, 1986.
5. Kuzmak, Lubomyr I. Laparoscopic Adjustable Gastric Banding Device. 5449368
United States of America, September 12, 1995.
6. Fischell, Donald A. Todd and Robert E. Urethral Sphincter Cuff. 4632114 United
States of America, December 30, 1986.
7. Henrik Norsker, James Danisch. Forming Techniques for the Self-Reliant Potter.
s.l. : Deutsches Zentrum fur Entwicklungstechnologien, 1991.
117
8. Winn, Alastair. [Online] Applied Silicone Corporation, 2007.
http://www.appliedsilicone.com/article.html.
9. Budynas, Warren C. Young and Richard G. Roark's Formulas for Stress and Strain.
New York : McGraw-Hill Companies, Inc., 2002.
10. The Basics of Testing Plastics. West Conshohocken, PA : American Society for
Testing and Materials, 1998.
11. Mathews, Normand L. Frigon and David. Practical Guide to Experimental Design.
New York : John Wiley & Sons, Inc., 1997.
118