grady pain clinic - Emory Healthcare
advertisement

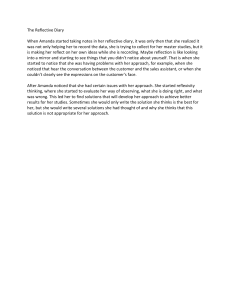
EMORY PAIN CLINIC PATIENT PAIN DIARY Please complete the following, beginning after your procedure. Please put a number from 0 to 10 to describe your pain at each hour that you are able. You do not have to fill out each hour, but the more details we have, the better we can help you. TIME 5:00 am 6:00 7:00 8:00 9:00 10:00 11:00 12:00 n 1:00 pm 2:00 3:00 4:00 5:00 6:00 7:00 8:00 9:00 10:00 11:00 12:00 mn 1:00 am 2:00 3:00 4:00 DAY 1 DAY 2 DAY 3 DAY 4 Patient name: Procedure performed: Date of procedure (day 1): Time of procedure: DAY 5 DAY 6 DAY 7