- Journal of Allergy and Clinical Immunology
advertisement

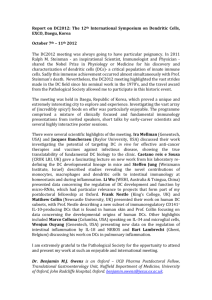
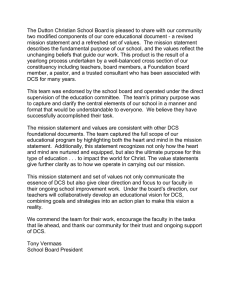
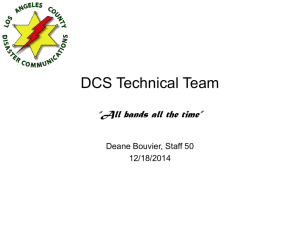
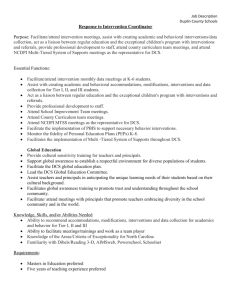
Lesional dendritic cells in patients with chronic atopic dermatitis and psoriasis exhibit parallel ability to activate T-cell subsets rez-Farin ~ as, PhD,a,c Leanne M. Johnson-Huang, PhD,a Hideki Fujita, MD, PhD,a* Avner Shemer, MD,b* Mayte Sua a a Suzanne Tintle, BS, Irma Cardinale, MSc, Judilyn Fuentes-Duculan, MD,a Inna Novitskaya, MSc,a John A. Carucci, MD, PhD,d James G. Krueger, MD, PhD,a and Emma Guttman-Yassky, MD, PhDa New York, NY, and Ramat-Gan, Israel Background: Atopic dermatitis (AD) and psoriasis represent polar immune diseases. AD is a TH2/TH22-dominant disease, whereas psoriasis is considered a TH1/TH17 disease. Local immune deviation is suggested to be regulated by dendritic cell (DC)–induced T-cell polarization and recruitment of specific T-cell subsets by chemokines. Although the role of chemokines is well documented, the actual contribution of DCs to activate polar T-cell subsets in human subjects is still a matter of speculation. Objective: We sought to elucidate the significance of each cutaneous DC subset in disease-specific T-cell immune deviation. Methods: We performed a comprehensive analysis of major cutaneous resident (Langerhans cells and blood dendritic cell antigen 1–positive dermal DCs) and inflammatory (inflammatory dendritic epidermal cells and blood dendritic cell antigen 1–negative dermal DCs) DC subsets directly isolated from the lesional skin of patients with AD and those with psoriasis. Results: The ability of each DC subset to expand TH1, TH2, TH17, and TH22 subsets was similar between the 2 diseases, despite the association of both with accumulation of resident and inflammatory DCs. We also confirmed differential upregulation of chemokine expression in patients with AD (CCL17, CCL18, and CCL22) and psoriasis (CXCL1, IL-8, and CCL20). The expression of CCL17 and CCL22 was higher in Langerhans cells from patients with AD than from patients with psoriasis, whereas the opposite was observed for CXCL9 and CXCL10. Conclusion: Our results suggest that DC polarity does not directly drive differential T-cell subset responses. Alternatively, From athe Laboratory for Investigative Dermatology and cthe Center for Clinical and Translational Science, The Rockefeller University, New York; bthe Department of Dermatology, Tel-Hashomer Medical Center, Ramat-Gan; and dthe Department of Dermatology, Weill Medical College of Cornell University, New York. *These authors contributed equally to this work. Supported in part by the Empire State Stem Cell Fund through NYSDOH contract no. C023046. Opinions expressed here are solely those of the authors and do not necessarily reflect those of the Empire State Stem Cell Fund, the NYSDOH, or the State of New York. S. T. and E. G.-Y. were supported by a Clinical and Translational Science Award grant. Disclosure of potential conflict of interest: The authors have declared that they have no conflict of interest. Received for publication March 8, 2011; revised May 7, 2011; accepted for publication May 13, 2011. Available online June 25, 2011. Reprint requests: Emma Guttman-Yassky, MD, PhD, Laboratory for Investigative Dermatology, The Rockefeller University, New York, NY 10065. E-mail: eguttman@ rockefeller.edu. 0091-6749/$36.00 Ó 2011 American Academy of Allergy, Asthma & Immunology doi:10.1016/j.jaci.2011.05.016 574 disease-specific chemokines might recruit specific memory T-cell subsets into the skin, which in turn might be activated and expanded by DCs at the site of inflammation, maintaining differential immune polarity in these diseases. (J Allergy Clin Immunol 2011;128:574-82.) Key words: Atopic dermatitis, psoriasis, dendritic cells, T-cell polarity, TH1, TH2, TH17, TH22, chemokine, skin Atopic dermatitis (AD) and psoriasis are the most common inflammatory skin diseases.1,2 Classically, these diseases have been viewed as polar TH1 versus TH2 diseases.3-5 Chronic AD lesions were shown to have a marked increase in TH2 T cells and related cytokines compared with psoriatic lesions, although a TH1 signal was also found during the chronic phase of AD.1,6,7 Recent works have also shown differences in the frequencies of TH22 and TH17 subsets between these diseases.3,8 Parallel comparison of AD and psoriasis can thus serve as a good model for dissecting disease-specific immune deviation and its underlying mechanisms versus generalized chronic inflammation.3,6,8-11 Dendritic cells (DCs), which are composed of diverse cell populations, play an essential role in the generation and regulation of T-cell immune responses.12,13 Normal human skin contains 2 major subsets of DCs: epidermal Langerhans cells (LCs; CD1a1CD2071 cells) and dermal myeloid DCs (CD11c1 blood dendritic cell antigen [BDCA] 11 cells).14 In addition, most (>95%) of the skin-homing (cutaneous lymphocyte–associated antigen–positive) resident T cells in steady state are CD45RO1 memory T cells.15 Chronic lesions from patients with psoriasis and those with AD have marked expansion of DCs, with different characteristics in each disease and differential T-cell subsets.3,7,16 In addition to resident DCs, inflamed skin also harbors inflammatory DCs both in the epidermis and dermis. Inflammatory dendritic epidermal cells (IDECs; CD1a1CD2072 cells) were largely represented in the epidermis and potentially the dermis of patients with lesional AD.6 In patients with psoriasis, a population of inflammatory DCs (CD11c1BDCA-12 cells) has been demonstrated in lesional skin.14,17,18 One hypothesis is that disease-specific DC specialization promotes and sustains the polar T-cell responses that characterize each disease.19,20 Psoriatic skin has a marked population of TNF and iNOS-producing DCs that have been shown to stimulate TH1- and TH17-cell expansion.17,21 In patients with AD, high-level production of thymic stromal lymphopoietin (TSLP) has been detected along with a population of DCs that bear TSLP receptors.6,22 TSLP-activated DCs have been shown to preferentially activate TH2 T-cell responses in autologous and allogeneic cultures in an OX40 ligand FUJITA ET AL 575 J ALLERGY CLIN IMMUNOL VOLUME 128, NUMBER 3 Abbreviations used AD: Atopic dermatitis BDCA: Blood dendritic cell antigen DC: Dendritic cell FACS: Fluorescence-activated cell sorting IDEC: Inflammatory dendritic epidermal cell LC: Langerhans cell MLR: Mixed leukocyte reaction OX40L: OX40 ligand TRAIL: TNF-induced apoptosis-inducing ligand TSLP: Thymic stromal lymphopoietin section in this article’s Online Repository).27 Antibodies used are outlined in Table E3. Intracellular cytokine staining T cells cultured with allogeneic DCs for 7 days were stimulated for 4 hours with 25 ng/mL phorbol 12-myristate 13-acetate and 2 mg/mL ionomycin in the presence of 10 mg/mL brefeldin A (all from Sigma-Aldrich, St Louis, Mo) at 378C. Thereafter, intracellular cytokine staining was performed as previously described.27 Antibodies used are outlined in Table E3. Expression of each molecule was analyzed in activated T cells (high forward scatter, high side scatter). Microarray hybridization (OX40L)–dependent manner.23-26 In addition, LCs derived from healthy skin or CD341 blood precursors have been shown to preferentially activate TH2 and TH22 T-cell subsets.27,28 Thus although specific DC subsets might regulate polar T-cell subset activation in patients with chronic skin diseases, this concept has not been tested in DC subsets isolated directly from skin lesions of patients with AD or psoriasis. To test the hypothesis that AD-related DCs induce a TH2biased immune response, we performed a comprehensive analysis of resident and inflammatory DC subsets isolated from the lesional skin of patients in the chronic stage of AD and psoriasis. Our results show that resident DC populations and inflammatory DC subsets are potent T-cell stimulators in allogeneic cultures. Each DC subset had the ability to stimulate TH1, TH2, TH17, and TH22 cells without major differences between DCs isolated from patients with each of the 2 diseases. However, some differences in the chemokines produced by DCs in these patients were detected, and this might lead to the preferential accumulation of TH2 cells in patients with AD. METHODS Skin samples Skin biopsy specimens were collected from patients with chronic AD (n 5 29), patients with psoriasis (n 5 28), and healthy volunteers (n 5 15; see the Methods section and Tables E1 and E2 in this article’s Online Repository at www.jacionline.org for details). For immunohistochemistry, biopsy specimens were frozen in OTC (Sakura, Tokyo, Japan) and stored at 2808C. Epidermal and dermal single-cell suspensions from biopsy specimens of patients with AD and patients with psoriasis were obtained after separation of the epidermis and dermis, as previously described.27 The study was approved by the Institutional Review Boards of Tel-Hashomer Medical Center and The Rockefeller University. Written informed consent was obtained from all participants. Fluorescence-activated cell sorting Fluorescence-activated cell sorting (FACS) of epidermal and dermal single-cell suspensions was performed as previously described with a FACSAria (BD Biosciences, San Jose, Calif; see the Methods section in this article’s Online Repository).27 Antibodies used are outlined in Table E3 (available in this article’s Online Repository at www.jacionline.org). Mixed leukocyte reaction FACS-sorted epidermal and dermal DCs were cultured with allogeneic total blood T cells or naive CD41 T cells from a single healthy donor at a DC/T-cell ratio of 1:50 for 7 days, and then T-cell proliferation and the cytokine profile were analyzed as previously described (see the Methods We used the Human Genome U133 Plus 2.0 arrays (Affymetrix, Santa Clara, Calif). See the Methods in this article’s Online Repository for further details. Immunohistochemistry Staining of skin sections and cell counts of positive cells were carried out as previously described.6 Antibodies used are outlined in Table E4 (available in this article’s Online Repository at www.jacionline.org). Statistical analysis Cell counts were analyzed by using a 2-tailed Student t test. The percentage of cytokine-producing cells was compared between patients with AD and psoriasis for each cell type by using repeated-measures ANOVA with between-subjects factors for analysis. P values of .05 or less were considered significant. CEL file quality control was assessed by using Harshlight29 and arrayQualityMetrics packages from R/Bioconductor. Expression measures were obtained with the GeneChip Robust Multiarray Average. Gene-set group differences for TH1 and TH2 chemokine gene sets were assessed by using a gene-set analysis approach.30 Gene-set statistics (the z score) were used to calculate the TH1 and TH2 score.31 See the Methods section in this article’s Online Repository for further details. RESULTS Marked accumulation of DCs in lesional skin characterizes both AD and psoriasis Biopsy specimens from AD, psoriatic, and healthy skin were evaluated for the presence of DCs by means of immunohistochemistry. We also analyzed several markers that might distinguish functional DC subsets. Representative immunohistochemistry is shown for each marker (Fig 1), and cell counts of all cases are represented in Fig E1 (available in this article’s Online Repository at www.jacionline.org). In comparison with healthy skin, skin from patients with AD or psoriasis showed increased numbers of dermal CD11c1 myeloid DCs. A significantly higher number of dermal BDCA-11 cells were found in AD skin compared with that seen in psoriatic and healthy skin, indicating an increased population of resident dermal DCs. The numbers of dermal BDCA-11 cells in AD and psoriatic skin were lower than CD11c1 counts, reflecting the existence of CD11c1BDCA-12 dermal inflammatory DC subset in both diseases. CD1a expression, which is common to LCs and IDECs, was increased in the epidermis of patients with both diseases compared with healthy epidermis. CD1a also displayed a dermal distribution in patients with AD only, which corroborated our previous data.6 FceRI, which is associated with LCs and IDECs in patients with AD, showed a mainly dermal staining in AD skin, which is also consistent with our previous observations.6 Because TNF-induced apoptosis-inducing ligand (TRAIL) 576 FUJITA ET AL J ALLERGY CLIN IMMUNOL SEPTEMBER 2011 FIG 1. AD and psoriasis are associated with substantial accumulation of DCs in lesional skin. Skin sections were stained for the DC-associated markers CD11c, BDCA-1, CD1a, FceRI, TRAIL, and OX40L. was recently identified as a marker of the dermal CD11c1BDCA-12 inflammatory DC population,18 TRAIL staining was also performed. The dermis of patients with both diseases was heavily populated with TRAIL1 cells, implicating these inflammatory DCs in both conditions. Finally, because OX40L is a marker of TH2-driving DCs and hypothesized to induce TH2 polarization in patients with AD, we explored its expression. A large number of OX40L1 cells were found in AD dermis, with minimal expression in psoriatic and normal dermis. Isolation of resident and inflammatory DCs from lesional skin of patients with both diseases For functional studies of DCs, we directly isolated DCs from skin samples of patients with chronic AD and those with psoriasis using FACS sorting. As shown in Fig 2, we sorted LCs from epidermal single-cell suspensions as HLA-DR1CD2071 cells, whereas IDECs were identified as HLA-DR1CD2072CD1a1 cells. For purification of dermal DCs, cells in dermal single-cell suspensions were first gated on HLA-DR1CD11c1 cells, a classic definition of myeloid DCs, and further gated according to BDCA-1 expression; BDCA-11 and BDCA-12 populations were collected separately. Both psoriatic and AD lesional skin had an appreciable increase in HLA-DRmidCD11c2 cell numbers, which are most likely monocytes. Although resident cutaneous DCs, LCs, and dermal BDCA-11 DCs were readily identified, inflammatory DCs, IDECs, and BDCA-12 dermal DCs, were only present in lesional skin of patients with AD and patients with psoriasis but not in healthy skin.17,27,32 Because the differential phenotype of LCs and IDECs is well documented, we further evaluated the expression of surface molecules on these epidermal FUJITA ET AL 577 J ALLERGY CLIN IMMUNOL VOLUME 128, NUMBER 3 FIG 2. Sorting strategy of epidermal and dermal DCs. LCs and IDECs were sorted as HLA-DR1CD2071 and HLA-DR1CD2072CD1a1 cells from epidermal single-cell suspensions, respectively, whereas resident and inflammatory dermal DCs were sorted as HLA-DR1CD11c1BDCA-11 and HLA-DR1CD11c1BDCA-12 cells from migre s, respectively. FACS plots from healthy skin are shown as negasingle-cell suspensions of dermal e tive controls for inflammatory DCs. FSC, Forward scatter. DC populations. As shown in Fig E2 (available in this article’s Online Repository at www.jacionline.org), LCs showed higher CD1a expression than IDECs in patients with both diseases. In agreement with prior reports, only LCs and IDECs in patients with AD expressed FceRI, with a higher expression level in IDECs than LCs.33,34 Similar T-cell expansion ability of lesional DCs from patients with AD or psoriasis To test the immunostimulatory ability of isolated DCs, we cocultured allogeneic bulk peripheral T cells and sorted DCs for 7 days, assessing T-cell proliferation by means of flow cytometry. All resident (LC and dermal BDCA-11 DCs) and inflammatory (IDEC and dermal BDCA-1-) DC populations from patients with AD or psoriasis induced substantial proliferation of allogeneic CD41 and CD81 T cells (see Fig E3 in this article’s Online Repository at www.jacionline.org). Thus to compare the T cell– polarizing capacity of DCs in lesional skin of patients with these diseases, intracellular cytokine staining of DC-activated T cells was conducted to evaluate IFN-g, IL-4, IL-17, and IL-22 production. Fig 3, A displays representative FACS plots showing the frequencies of the cells producing these cytokines among proliferating CD31CD41 and CD31CD81 cells stimulated by each DC subset from patients with AD or psoriasis, and the FACS gating strategy for the analysis is outlined in Fig E4 (available in this article’s Online Repository at www.jacionline.org). These experiments are summarized in Fig 3, B. Surprisingly, the general patterns of cytokine profiles of CD41 and CD81 T cells stimulated by each DC subset were similar between T cells cultured with DCs derived from AD and psoriatic skin, although BDCA-12 DCs from psoriatic dermis induced a significantly greater percentage of IL-17– and IL-22–producing CD81 cells than those from AD skin (Fig 3, B). Because the frequency of IFN-g–producing T cells was high in this culture system using bulk T cells, and IL-4 is particularly sensitive to inhibition by IFN-g, cocultures were also performed with naive CD41 T cells. Similar frequencies of IFN-g– and IL4–producing T cells in bulk and naive T-cell mixed leukocyte reaction (MLR) cultures were seen (see Fig E5 in this article’s Online Repository at www.jacionline.org), indicating that this system is sufficiently sensitive to detect the TH2-polarizing capacity of lesional DCs. Dermal BDCA-12 DCs exhibit superior ability in T-cell polarization Because the pathogenicity of inflammatory BDCA-12 dermal DCs has been proposed in patients with psoriasis,14 we further focused on the T cell–polarizing capacity of this cell population (see Fig E6 in this article’s Online Repository at www.jacionline.org). In patients with psoriasis, BDCA-12 dermal DCs were more efficient in induction of IL-22–producing CD81 T cells than LCs, IDECs, and BDCA-11 dermal DCs and also generated significantly higher levels of IL-17–producing CD81 T cells than LCs and IDECs. BDCA-12 dermal DCs were also superior to LCs in expanding IFN-g–producing CD41 T cells and to both LCs and IDECs in generation of IL-22–producing CD41 T cells. In 578 FUJITA ET AL J ALLERGY CLIN IMMUNOL SEPTEMBER 2011 FIG 3. Similar T-cell polarizing ability of lesional resident and inflammatory DCs from patients with AD and those with psoriasis. A, Total allogeneic T cells were cultured with DCs from the lesional skin of patients with AD and those with psoriasis for 7 days, and intracellular cytokine expression was examined. Representative FACS plots are shown. B, Summary of the frequencies of cytokine-producing cells from 4 experiments. Each symbol represents 1 donor. *P < .05. PS, Psoriasis. patients with AD, BDCA-12 dermal DCs induced more IL-22– producing CD41 T cells than LCs and IDECs. Thus, particularly in patients with psoriasis, BDCA-12 dermal DCs showed higher T cell–polarizing ability. Differential chemokine expression in AD versus psoriatic skin Because DCs derived from AD and psoriatic skin unexpectedly exhibited comparable capacity to polarize T cells, the expression FUJITA ET AL 579 J ALLERGY CLIN IMMUNOL VOLUME 128, NUMBER 3 FIG 4. Normalized chemokine gene expression in patients with psoriasis (x-axis) versus patients with AD (y-axis) for different DC subsets. Black lines represent the identity lines, whereas gray lines represent the 1.5fold change. A and B, Epidermal DC subsets (Fig 4, A) and dermal DC subsets (Fig 4, B). AD versus psoriasis scores for TH1 and TH2 chemokines and the respective P values (in parentheses) are presented for each DC subset. of T cell–attracting chemokines was further explored among DCs from patients with both diseases. We evaluated the gene expression profile of genes encoding known chemokines for each DC subset in patients with AD and those with psoriasis by using a gene-array analysis of the isolated DC subsets with a gene-set analysis approach, as previously described.30 The expression values for chemokine-encoding genes of individual DC subsets in both diseases are represented in Fig 4. For each cell subset, a score was generated for the gene sets of TH1 and TH2 chemokines, summarizing the differences identified between the 2 diseases for a particular TH set rather than for individual genes (Fig 4).31 Overall, although there were some similarities in chemokine expression in patients with psoriasis and those with chronic AD, which might be attributed to an appreciable TH1/IFN-g component in both diseases,6,9 several chemokines were differentially polarized. We found that the TH2-associated chemokines CCL17 and CCL22 were upregulated in AD skin–derived LCs and IDECs compared with psoriatic skin–derived LCs and IDECs, whereas the TH1-related chemokines CXCL9 and CXCL10 were downregulated (Fig 4, A). As for dermal DC subsets, the TH2-related chemokines CCL5, CCL17, and CCL18 were upregulated in AD skin–derived BDCA-11 and BDCA-12 subsets, with additional upregulation of CCL22 and CCL13 in BDCA-12 DCs (Fig 4, B). Interestingly, the IFN-g–induced chemokines CXCL9 and CXCL10 showed higher expression in AD skin–derived dermal DC subsets, particularly in the BDCA-12 population, than in psoriatic skin–derived cells. We further reviewed our recently published data of differentially expressed genes between chronic lesional AD, psoriatic, and healthy skin9 and selected genes encoding known chemokines that are upregulated in AD or psoriatic skin compared with healthy skin (see Table E5 in this article’s Online Repository at www.jacionline.org). Whereas expression of TH2-related chemokines (CCL5, CCL17, CCL18, and CCL22) was upregulated in lesional AD skin, psoriatic skin showed highly upregulated expression of TH1-associated (CXCL1 and CXCL8), and Th17associated (CCL20) chemokines compared with healthy skin. Interestingly, both diseases showed increased expression of the TH1/IFN-g–associated CXCL9 and CXCL10 chemokines compared with healthy skin. Protein expression was evaluated by means of immunohistochemistry to verify that the selected chemokines in Table E5 were potential immune response mediators in lesional AD and psoriatic skin (Fig 5). CCL17, CCL18, and CCL22 showed increased epidermal and dermal expression in AD compared with psoriatic skin. The expression of the TH17 chemokine CCL20 was upregulated in psoriatic skin–derived epidermal DCs compared with AD skin–derived DCs (Fig 4), which is consistent with the significantly increased epidermal staining seen in psoriatic compared with AD skin (Fig 5). CXCL9 showed upregulated epidermal and dermal expression in both psoriatic and AD skin compared with that seen in healthy skin. The staining results for CCL17, CCL22, CCL18, and CCL20 were consistent with our previous data.6,8 Thus lesional chronic AD skin preferentially expressed TH2 and some TH1-associated chemokines, whereas psoriatic skin was dominated by TH1/TH17-related chemokines. DISCUSSION In this study we have compared the ability of DC subsets isolated from chronic lesions of AD and psoriatic skin to expand, polarize, or both specific cytokine-producing T-cell subsets in an allogeneic MLR system. DC subsets derived from patients with AD or psoriasis were highly potent stimulators of T-cell 580 FUJITA ET AL J ALLERGY CLIN IMMUNOL SEPTEMBER 2011 FIG 5. Differential chemokine expression in the skin between patients with AD and those with psoriasis. Skin sections from healthy subjects and patients with AD and psoriasis were stained for CCL17, CCL18, CCL22, CCL20, and CXCL9. proliferation and cytokine production. Interestingly, although LCs derived from healthy skin were shown to preferentially expand TH2 and TH22 cells (over TH1 cells),27,28 this difference was not apparent with LCs derived from inflammatory lesions of AD and psoriatic skin. On the basis of current concepts around the function of TSLPDCs in the polarizing TH2 response and TNF and iNOS-producing DCs in stimulating expansion of TH1 and TH17 subsets, we expected to see differential T-cell responses to AD skin– and psoriatic skin–derived DCs. Instead, we found that DCs from AD and psoriatic skin showed similar abilities to drive broad diseaseunspecific activation of TH subsets. Even for naive T cells, DCs derived from AD and psoriatic skin showed very similar induction of TH1 and TH2 subsets. Overall, the ability of DCs to stimulate TH2 expansion or polarity in our system is compatible with that previously seen with TSLP-DCs in human systems with naive T cells as responders.26 Similar to our results with DCs isolated from chronic AD skin lesions, T cells primed by TSLP-DCs produced IFN-g while still retaining the ability to produce TH2 cytokines.26 Hence one interpretation of these data is that DCs in ‘‘polar’’ skin diseases are not intrinsically directing the underlying polarity of the T-cell responses. Alternatively, selective production of TH2-related chemokines by DCs, particularly in patients with AD, might lead to TH2 memory T-cell recruitment into the skin, where dermal DCs further stimulate memory T-cell expansion. Steady-state T-cell populations in the skin of patients with chronic diseases might reflect expansion of memory T cells resident in the skin and/or recruitment of specific TH subsets from J ALLERGY CLIN IMMUNOL VOLUME 128, NUMBER 3 the bloodstream that express subset-specific chemokine receptors.35-38 Because there were no major differences in the capability of different DC subsets to expand various T-cell subsets between these diseases, we alternatively explored the potential for recruitment of specific T-cell subsets that is largely determined by DC-associated chemokines.39 Differential TH1 versus TH2 chemokine expression has been demonstrated in the chronic phase of psoriasis and AD, such as overexpression of CCL17 and CCL22 in patients with AD40 compared with increased CXCL9 and CXCL10 expression in patients with psoriasis.41 We confirmed increased expression of TH2-associated chemokines in lesional AD skin and increased expression of TH17- and some TH1-related chemokines in psoriatic skin, whereas several TH1 chemokines showed similar expression in both AD and psoriatic skin, potentially accounting for an appreciable TH1/IFN-g component in patients with chronic AD. At the DC level, the chemokine expression pattern of LCs fits the classical TH1/TH2 dichotomy seen in patients with psoriasis and AD. Upregulated expression of CCL18 by AD dermal DC subsets was also in accordance with previous reports.6,42 Interestingly, the expression of IFN-g–regulated chemokines was higher in AD skin–derived compared with psoriatic skin–derived BDCA-12 DCs, possibly suggesting that inflammatory DCs might be responsible for the increased TH1 axis in patients with chronic AD.7 Collectively, we propose that differential expression of chemokines between patients with AD and those with psoriasis might play a crucial role in the maintenance of disease-specific T-cell polarity in the chronic stage by recruiting distinct T-cell subsets. Our experimental system might not reflect the local cytokine milieu at the time of in vivo T-cell stimulation. We acknowledge additional explanations for our surprising results and a number of limitations of our studies. First, the initiation phase of AD usually occurs in children, and it is very difficult to study early T-cell/DC responses of the skin in children. Second, AD and psoriasis each have genetic backgrounds in which T-cell responses to antigens might be intrinsically different. Variants of IL-23 receptor–encoding genes, which might affect induction of a TH17 response, have been associated with psoriasis.2 Moreover, the association of IL-4 receptor gene variants with AD has also been determined,40 and this might influence the TH2 response. Thus it is possible that in vivo AD-related T cells are more likely to become TH2 cells compared with the TH17-prone differentiation seen in psoriasis. Our model system has examined only the DC contribution to third-party responder T cells and not autologous responses. Third, antigen specificity might also affect T-cell polarization. There is also the issue of whether the route of antigen exposure (possibly epicutaneous in patients with AD) or the intrinsic nature of the antigen can affect the outcome of polar T-cell responses. In cutaneous contact hypersensitivity models, distinct TH responses have been provoked by various allergens.43 Interestingly, monocyte-derived DCs from atopic donors in the presence of collagen type I could stimulate autologous allergen-specific TH1 cells from naive T cells, as well as a TH2 to TH1 shift in memory T cells, despite the initial TH2 bias of these cells.44 In addition, FceRI expression is an important feature of AD-associated LCs and IDECs, and LCs are thought to stimulate the TH2-cell response by presenting IgE-bound allergens in patients with AD.45-47 Our data were obtained from an in vitro antigen-nonspecific allogeneic MLR system in contrast to antigen-specific in vivo reactions. FUJITA ET AL 581 Fourth, a number of factors that might influence DC/T-cell interactions in vivo might be missing from the in vitro culture system used. Exposure of DCs to different cytokines, chemokines, Toll-like receptor agonists, or costimulatory molecules, such as OX40 expression of T cells in patients with AD, are likely to be present in vivo in these diseases and might influence the outcome of T-cell responses.48,49 Fifth, the initiation of polar T-cell responses for skin-homing T cells is believed to occur in draining lymph nodes after antigenactivated DCs migrate to these nodes. Thus DCs might have different abilities to stimulate naive T cells or central memory T cells in the lymph node microenvironment.15 Sixth, the microenvironment of chronic inflammation in both diseases is complex and involves the contributions of many cell types,7 which might influence DC polarity, potentially accounting for the similarities in the T-cell responses seen in our system. Our results potentially have important therapeutic implications. Because DCs in patients with both conditions had a comparable ability to expand all classes of T cells, it is expected that nonspecific T cell–suppressing therapeutics, such as cyclosporine A and efalizumab, are effective for both diseases.50-53 However, shutting down all T-cell responses through such modalities harbors undesirable effects.54,55 Thus strategies aiming to alter T-cell recruitment to the skin by targeting chemokines might be beneficial for patients with inflammatory skin conditions. In summary, we found that DC populations in lesional skin did not preferentially expand T-cell subsets in a disease-specific fashion. Once disease-specific skin inflammation is established during the initiation phase of the disease, differential expression of TH1, TH2, TH17, and TH22 chemokines might be more important than DC polarity in sustaining local immune deviation in the chronic stage. We hypothesize that disease-specific chemokines recruit specific memory T-cell subsets into the skin, which in turn are activated and expanded by DCs at the site of inflammation, maintaining differential immune polarity in these diseases. Because we used biopsy specimens from chronic skin lesions, we did not address the role of cutaneous DCs in the initiation phase of both diseases. In patients with psoriasis, IFN-a production by plasmacytoid DCs was proposed to play a role in disease initiation.56 However, the significance of DC polarity in the acute inflammation seen in both diseases has not been fully elucidated. Future studies addressing skewing of immune responses during the initiation versus the chronic stage are warranted for completing our understanding of evolving general cutaneous inflammation versus disease-specific characteristics underlying these diseases across the various stages of their development. We appreciate the assistance and advice of the Flow Cytometry Resource Center at The Rockefeller University. Clinical implications: Effective strategies to shut down TH2 inflammation in the skin should ideally target T-cell recruitment rather than T-cell activation and proliferation. REFERENCES 1. Bieber T, Novak N. Pathogenesis of atopic dermatitis: new developments. Curr Allergy Asthma Rep 2009;9:291-4. 2. Di Cesare A, Di Meglio P, Nestle FO. The IL-23/Th17 axis in the immunopathogenesis of psoriasis. J Invest Dermatol 2009;129:1339-50. 3. Nograles KE, Zaba LC, Shemer A, Fuentes-Duculan J, Cardinale I, Kikuchi T, et al. IL-22-producing ‘‘T22’’ T cells account for upregulated IL-22 in atopic 582 FUJITA ET AL 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. dermatitis despite reduced IL-17-producing TH17 T cells. J Allergy Clin Immunol 2009;123:1244-52, e2. Homey B, Steinhoff M, Ruzicka T, Leung DY. Cytokines and chemokines orchestrate atopic skin inflammation. J Allergy Clin Immunol 2006;118:178-89. Ong PY, Leung DY. Immune dysregulation in atopic dermatitis. Curr Allergy Asthma Rep 2006;6:384-9. Guttman-Yassky E, Lowes MA, Fuentes-Duculan J, Whynot J, Novitskaya I, Cardinale I, et al. Major differences in inflammatory dendritic cells and their products distinguish atopic dermatitis from psoriasis. J Allergy Clin Immunol 2007;119:1210-7. Guttman-Yassky E, Nograles KE, Krueger JG. Contrasting pathogenesis of atopic dermatitis and psoriasis—part II: immune cell subsets and therapeutic concepts. J Allergy Clin Immunol 2011;127:1420-32. Guttman-Yassky E, Lowes MA, Fuentes-Duculan J, Zaba LC, Cardinale I, Nograles KE, et al. Low expression of the IL-23/Th17 pathway in atopic dermatitis compared to psoriasis. J Immunol 2008;181:7420-7. Guttman-Yassky E, Suarez-Farinas M, Chiricozzi A, Nograles KE, Shemer A, Fuentes-Duculan J, et al. Broad defects in epidermal cornification in atopic dermatitis identified through genomic analysis. J Allergy Clin Immunol 2009;124: 1235-44, e58. Nomura I, Gao B, Boguniewicz M, Darst MA, Travers JB, Leung DY. Distinct patterns of gene expression in the skin lesions of atopic dermatitis and psoriasis: a gene microarray analysis. J Allergy Clin Immunol 2003;112:1195-202. Nomura I, Goleva E, Howell MD, Hamid QA, Ong PY, Hall CF, et al. Cytokine milieu of atopic dermatitis, as compared to psoriasis, skin prevents induction of innate immune response genes. J Immunol 2003;171:3262-9. Novak N, Bieber T. The role of dendritic cell subtypes in the pathophysiology of atopic dermatitis. J Am Acad Dermatol 2005;53(suppl):S171-6. Steinman RM, Banchereau J. Taking dendritic cells into medicine. Nature 2007; 449:419-26. Zaba LC, Krueger JG, Lowes MA. Resident and ‘‘inflammatory’’ dendritic cells in human skin. J Invest Dermatol 2009;129:302-8. Clark RA. Skin-resident T cells: the ups and downs of onsite immunity. J Invest Dermatol 2010;130:362-70. Guttman-Yassky E, Krueger JG. Psoriasis: evolution of pathogenic concepts and new therapies through phases of translational research. Br J Dermatol 2007;157: 1103-15. Zaba LC, Fuentes-Duculan J, Eungdamrong NJ, Abello MV, Novitskaya I, Pierson KC, et al. Psoriasis is characterized by accumulation of immunostimulatory and Th1/Th17 cell-polarizing myeloid dendritic cells. J Invest Dermatol 2009;129: 79-88. Zaba LC, Fuentes-Duculan J, Eungdamrong NJ, Johnson-Huang LM, Nograles KE, White TR, et al. Identification of TNF-related apoptosis-inducing ligand and other molecules that distinguish inflammatory from resident dendritic cells in patients with psoriasis. J Allergy Clin Immunol 2010;125:1261-8, e9. Jariwala SP. The role of dendritic cells in the immunopathogenesis of psoriasis. Arch Dermatol Res 2007;299:359-66. Johnson-Huang LM, McNutt NS, Krueger JG, Lowes MA. Cytokine-producing dendritic cells in the pathogenesis of inflammatory skin diseases. J Clin Immunol 2009;29:247-56. Lowes MA, Chamian F, Abello MV, Fuentes-Duculan J, Lin SL, Nussbaum R, et al. Increase in TNF-alpha and inducible nitric oxide synthase-expressing dendritic cells in psoriasis and reduction with efalizumab (anti-CD11a). Proc Natl Acad Sci U S A 2005;102:19057-62. Ziegler SF, Artis D. Sensing the outside world: TSLP regulates barrier immunity. Nat Immunol 2010;11:289-93. Ito T, Wang YH, Duramad O, Hori T, Delespesse GJ, Watanabe N, et al. TSLP-activated dendritic cells induce an inflammatory T helper type 2 cell response through OX40 ligand. J Exp Med 2005;202:1213-23. Soumelis V, Reche PA, Kanzler H, Yuan W, Edward G, Homey B, et al. Human epithelial cells trigger dendritic cell mediated allergic inflammation by producing TSLP. Nat Immunol 2002;3:673-80. Wang YH, Liu YJ. Thymic stromal lymphopoietin, OX40-ligand, and interleukin25 in allergic responses. Clin Exp Allergy 2009;39:798-806. Watanabe N, Hanabuchi S, Marloie-Provost MA, Antonenko S, Liu YJ, Soumelis V. Human TSLP promotes CD40 ligand-induced IL-12 production by myeloid dendritic cells but maintains their Th2 priming potential. Blood 2005;105: 4749-51. Fujita H, Nograles KE, Kikuchi T, Gonzalez J, Carucci JA, Krueger JG. Human Langerhans cells induce distinct IL-22-producing CD41 T cells lacking IL-17 production. Proc Natl Acad Sci U S A 2009;106:21795-800. Klechevsky E, Morita R, Liu M, Cao Y, Coquery S, Thompson-Snipes L, et al. Functional specializations of human epidermal Langerhans cells and CD141 dermal dendritic cells. Immunity 2008;29:497-510. J ALLERGY CLIN IMMUNOL SEPTEMBER 2011 29. Suarez-Farinas M, Pellegrino M, Wittkowski KM, Magnasco MO. Harshlight: a ‘‘corrective make-up’’ program for microarray chips. BMC Bioinformatics 2005; 6:294. 30. Suarez-Farinas M, Lowes MA, Zaba LC, Krueger JG. Evaluation of the psoriasis transcriptome across different studies by gene set enrichment analysis (GSEA). PLoS One 2010;5:e10247. 31. Irizarry RA, Wang C, Zhou Y, Speed TP. Gene set enrichment analysis made simple. Stat Methods Med Res 2009;18:565-75. 32. Zaba LC, Fuentes-Duculan J, Steinman RM, Krueger JG, Lowes MA. Normal human dermis contains distinct populations of CD11c1BDCA-11 dendritic cells and CD1631FXIIIA1 macrophages. J Clin Invest 2007;117:2517-25. 33. Wollenberg A, Wen S, Bieber T. Phenotyping of epidermal dendritic cells: clinical applications of a flow cytometric micromethod. Cytometry 1999;37:147-55. 34. Wollenberg A, Kraft S, Hanau D, Bieber T. Immunomorphological and ultrastructural characterization of Langerhans cells and a novel, inflammatory dendritic epidermal cell (IDEC) population in lesional skin of atopic eczema. J Invest Dermatol 1996;106:446-53. 35. Lonsdorf AS, Hwang ST, Enk AH. Chemokine receptors in T-cell-mediated diseases of the skin. J Invest Dermatol 2009;129:2552-66. 36. Acosta-Rodriguez EV, Rivino L, Geginat J, Jarrossay D, Gattorno M, Lanzavecchia A, et al. Surface phenotype and antigenic specificity of human interleukin 17producing T helper memory cells. Nat Immunol 2007;8:639-46. 37. Annunziato F, Cosmi L, Santarlasci V, Maggi L, Liotta F, Mazzinghi B, et al. Phenotypic and functional features of human Th17 cells. J Exp Med 2007;204:1849-61. 38. Singh SP, Zhang HH, Foley JF, Hedrick MN, Farber JM. Human T cells that are able to produce IL-17 express the chemokine receptor CCR6. J Immunol 2008;180:214-21. 39. Lebre MC, Burwell T, Vieira PL, Lora J, Coyle AJ, Kapsenberg ML, et al. Differential expression of inflammatory chemokines by Th1- and Th2-cell promoting dendritic cells: a role for different mature dendritic cell populations in attracting appropriate effector cells to peripheral sites of inflammation. Immunol Cell Biol 2005;83:525-35. 40. Oyoshi MK, He R, Kumar L, Yoon J, Geha RS. Cellular and molecular mechanisms in atopic dermatitis. Adv Immunol 2009;102:135-226. 41. Bowcock AM, Krueger JG. Getting under the skin: the immunogenetics of psoriasis. Nat Rev Immunol 2005;5:699-711. 42. Pivarcsi A, Gombert M, Dieu-Nosjean MC, Lauerma A, Kubitza R, Meller S, et al. CC chemokine ligand 18, an atopic dermatitis-associated and dendritic cell-derived chemokine, is regulated by staphylococcal products and allergen exposure. J Immunol 2004;173:5810-7. 43. Toebak MJ, Gibbs S, Bruynzeel DP, Scheper RJ, Rustemeyer T. Dendritic cells: biology of the skin. Contact Dermatitis 2009;60:2-20. 44. Brand U, Bellinghausen I, Enk AH, Jonuleit H, Becker D, Knop J, et al. Allergenspecific immune deviation from a TH2 to a TH1 response induced by dendritic cells and collagen type I. J Allergy Clin Immunol 1999;104:1052-9. 45. Dubrac S, Schmuth M, Ebner S. Atopic dermatitis: the role of Langerhans cells in disease pathogenesis. Immunol Cell Biol 2010;88:400-9. 46. Mudde GC, Van Reijsen FC, Boland GJ, de Gast GC, Bruijnzeel PL, BruijnzeelKoomen CA. Allergen presentation by epidermal Langerhans’ cells from patients with atopic dermatitis is mediated by IgE. Immunology 1990;69:335-41. 47. Stingl G, Maurer D. IgE-mediated allergen presentation via Fc epsilon RI on antigen-presenting cells. Int Arch Allergy Immunol 1997;113:24-9. 48. Duraisingham SS, Hornig J, Gotch F, Patterson S. TLR-stimulated CD34 stem cellderived human skin-like and monocyte-derived dendritic cells fail to induce Th17 polarization of naive T cells but do stimulate Th1 and Th17 memory responses. J Immunol 2009;183:2242-51. 49. Lombardi V, Van Overtvelt L, Horiot S, Moingeon P. Human dendritic cells stimulated via TLR7 and/or TLR8 induce the sequential production of Il-10, IFNgamma, and IL-17A by naive CD41 T cells. J Immunol 2009;182:3372-9. 50. Akhavan A, Rudikoff D. Atopic dermatitis: systemic immunosuppressive therapy. Semin Cutan Med Surg 2008;27:151-5. 51. Amor KT, Ryan C, Menter A. The use of cyclosporine in dermatology: part I. J Am Acad Dermatol 2010;63:925-48. 52. Chacko M, Weinberg JM. Efalizumab. Dermatol Ther 2007;20:265-9. 53. Takiguchi R, Tofte S, Simpson B, Harper E, Blauvelt A, Hanifin J, et al. Efalizumab for severe atopic dermatitis: a pilot study in adults. J Am Acad Dermatol 2007; 56:222-7. 54. Di Lernia V. Progressive multifocal leukoencephalopathy and antipsoriatic drugs: assessing the risk of immunosuppressive treatments. Int J Dermatol 2010;49:631-5. 55. Ryan C, Amor KT, Menter A. The use of cyclosporine in dermatology: part II. J Am Acad Dermatol 2010;63:949-74. 56. Nestle FO, Conrad C, Tun-Kyi A, Homey B, Gombert M, Boyman O, et al. Plasmacytoid predendritic cells initiate psoriasis through interferon-alpha production. J Exp Med 2005;202:135-43. FUJITA ET AL 582.e1 J ALLERGY CLIN IMMUNOL VOLUME 128, NUMBER 3 METHODS Skin samples Biopsy specimens of lesional skin were collected from 2 sets of patients with chronic AD with moderate-to-severe disease and a recent exacerbation in their disease; data on the first set (18 patients; 12 male subjects and 6 female subjects; age, 17-66 years; median, 37 years) have been previously published.E1 Skin biopsy specimens of the first patient set were used for immunohistochemistry staining. The second set of patients with chronic AD (11 patients; age, 24-61 years; median, 39 years) was used for FACS, MLR, and genomic analysis (Table E1). Skin biopsy specimens were also collected from lesional skin of 2 sets of patients with psoriasis; data on the first set (15 patients; 11 men and 4 women; age, 28-59 years; median, 48 years) have been previously published.E1 The first set of patient samples was used for immunohistochemistry staining. FACS, MLR, and genomic analysis were performed with the second set of 13 patients (age, 26-60 years; median, 47 years; Table E2). For control subjects, skin biopsy specimens from 15 healthy volunteers (7 men and 8 women; age, 24-69 years; median, 41 years) were used. Patients with moderate-to-severe psoriasis (involvement of >10% body surface area) and with an acute exacerbation of chronic AD (SCORAD score between 20 and 76; mean, 57) who did not receive any therapy for more than 4 weeks were included. Diagnoses were confirmed histologically, and there were no cases of diagnostic discordance. Biopsy specimens were frozen in OCT medium for immunohistochemistry and liquid nitrogen for RNA extraction. FACS FACS sorting of epidermal and dermal single-cell suspensions was performed as previously described by using a FACSAria (BD Biosciences, San Jose, Calif).E2 Epidermal cells were sorted into 2 populations: HLADR1CD2071 and HLA-DR1CD2072CD1a1 cells. Dermal cells were sorted and HLAinto 2 populations: HLA-DR1CD11c1BDCA-11 DR1CD11c1BDCA-12 cells. In some skin samples the numbers of particular DC subsets collected were not sufficient for subsequent MLR assay. Antibodies used are outlined in Table E3. Isolation of T cells Total blood T cells and naive CD41 T cells were isolated from a single healthy donor by using RosetteSep T Cell Enrichment Mixture (StemCell Technologies, Vancouver, British Columbia, Canada) and the human naive CD41 T Cell Isolation Kit (Miltenyi Biotec, Bergisch Gladbach, Germany), respectively. The purity of total T cells after isolation was greater than 98%, as determined based on CD3 expression. The purity of naive CD41 T cells was greater than 95%, as determined based on the expression of CD4 and CD45RA. Microarray hybridization Cell pellets of FACS-sorted DCs from the lesional skin of patients with AD and patients with psoriasis were dissolved in TRI reagent (Ambion, Austin, Tex) and stored at 2808C until RNA extraction. Total RNA was extracted with the MagMAX-96 for Microarrays Kit (Ambion). Target 2-cycle amplification was performed according to the Affymetrix protocol, with slight modifications previously described by Kube et al.E3 Subsequent labeling of cRNA transcripts with biotin was performed with the GeneChip IVT Labeling Kit (Affymetrix). Biotin-labeled cRNA was fragmented and hybridized to Human Genome U133 Plus 2.0 arrays (Affymetrix). Statistical analysis Cell counts by means of immunohistochemistry were analyzed with a 2-tailed Student t test comparing AD dermis versus psoriatic and healthy dermis and AD epidermis versus psoriatic and healthy epidermis. For FACS Tcell cytokine profile data, the percentage of cytokine-producing cells was compared between these diseases for each cell type. Because the same donor was used to obtained different cell types, we used repeated-measures ANOVA with between-subjects factors to analyze these data. Comparisons with P values of .05 or less were considered statistically significant. For gene array analysis, CEL file quality control was assessed with the HarshlightE4 and arrayQualityMetrics packages from R/Bioconductor. Expression measures were obtained with the GeneChip Robust Multiarray Average. Gene-set group differences for the sets of genes encoding TH1 and TH2 chemokines were assessed by using a gene-set analysis approach, as we have published previously.E5 To calculate the TH1 and TH2 score, we used the gene-set statistics proposed by Irizarry et al (the z score)E6 that under the null hypothesis follow standard normal distribution. REFERENCES E1. Guttman-Yassky E, Lowes MA, Fuentes-Duculan J, Whynot J, Novitskaya I, Cardinale I, et al. Major differences in inflammatory dendritic cells and their products distinguish atopic dermatitis from psoriasis. J Allergy Clin Immunol 2007;119:1210-7. E2. Fujita H, Nograles KE, Kikuchi T, Gonzalez J, Carucci JA, Krueger JG. Human Langerhans cells induce distinct IL-22-producing CD41 T cells lacking IL-17 production. Proc Natl Acad Sci U S A 2009;106:21795-800. E3. Kube DM, Savci-Heijink CD, Lamblin AF, Kosari F, Vasmatzis G, Cheville JC, et al. Optimization of laser capture microdissection and RNA amplification for gene expression profiling of prostate cancer. BMC Mol Biol 2007;8:25. E4. Suarez-Farinas M, Pellegrino M, Wittkowski KM, Magnasco MO. Harshlight: a ‘‘corrective make-up’’ program for microarray chips. BMC Bioinformatics 2005; 6:294. E5. Suarez-Farinas M, Lowes MA, Zaba LC, Krueger JG. Evaluation of the psoriasis transcriptome across different studies by gene set enrichment analysis (GSEA). PLoS One 2010;5:e10247. E6. Irizarry RA, Wang C, Zhou Y, Speed TP. Gene set enrichment analysis made simple. Stat Methods Med Res 2009;18:565-75. E7. Guttman-Yassky E, Suarez-Farinas M, Chiricozzi A, Nograles KE, Shemer A, Fuentes-Duculan J, et al. Broad defects in epidermal cornification in atopic dermatitis identified through genomic analysis. J Allergy Clin Immunol 2009;124: 1235-44, e58. 582.e2 FUJITA ET AL J ALLERGY CLIN IMMUNOL SEPTEMBER 2011 FIG E1. Quantification of the cellular components in AD, psoriatic, and healthy skin. Cell counts per millimeter and means in healthy epidermis (Normal Epi), healthy dermis (Normal Derm), AD epidermis, AD dermis, psoriatic epidermis (Psor Epi), and psoriatic dermis (Psor Derm) are shown. *P < .05, **P < .01, and ***P < .001. J ALLERGY CLIN IMMUNOL VOLUME 128, NUMBER 3 FUJITA ET AL 582.e3 FIG E2. Differential expression of CD1a and FceRI between LCs and IDECs. HLA-DR1CD2071 LCs and HLADR1CD2072CD1a1 IDECs in epidermal cell suspensions from lesional AD and psoriatic skin were subjected to analysis of cell-surface expression of CD1a and FceRI by means of flow cytometry. Green lines, Isotype controls; blue lines, IDECs; red lines, LCs. Data are representative of 3 independent experiments. 582.e4 FUJITA ET AL J ALLERGY CLIN IMMUNOL SEPTEMBER 2011 FIG E3. Both resident and inflammatory DCs from lesional AD and psoriatic skin induce substantial proliferation of allogeneic CD41 and CD81 T cells. DCs from lesional AD and psoriatic skin were cultured with allogeneic total blood T cells labeled with carboxyfluorescein diacetate succinimidyl ester. Numbers in histograms show percentages of proliferating (low carboxyfluorescein diacetate succinimidyl ester) cells. Data are representative of 3 independent experiments. J ALLERGY CLIN IMMUNOL VOLUME 128, NUMBER 3 FUJITA ET AL 582.e5 FIG E4. FACS gating strategy used in the analysis of proliferating T cells. Live CD31 T cells were further divided into CD41CD82 and CD42CD81 populations. 582.e6 FUJITA ET AL J ALLERGY CLIN IMMUNOL SEPTEMBER 2011 FIG E5. TH1/TH2 polarization of naive CD41 T cells induced by lesional DCs from patients with AD and those with psoriasis. A, Representative FACS plots of intracellular cytokine expression of allogeneic naive CD41 T cells cultured for 7 days with DCs from lesional AD and psoriatic skin. B, Summary of the frequencies of cytokine-producing cells from 2 experiments. Each symbol represents 1 donor. PS, Psoriasis. J ALLERGY CLIN IMMUNOL VOLUME 128, NUMBER 3 FUJITA ET AL 582.e7 FIG E6. Dermal BDCA-12 DCs exhibit superior ability in T-cell polarization. Fig 3 was reorganized to compare the T-cell–polarizing capacity of dermal BDCA-12 DCs and other DC subsets. *P < .05 and **P < .01. PS, Psoriasis. 582.e8 FUJITA ET AL J ALLERGY CLIN IMMUNOL SEPTEMBER 2011 TABLE E1. Characteristics of patients with chronic AD Patient no. 1 2 3 4 5 6 7 8 9 10 11 Age (y) Family history* of atopy SCORAD score 43 37 39 48 52 61 28 27 30 24 52 No NA NA No No No Yes No No No No 28 64 32 55 45 71 45 78 65 68 74 Increased IgE levely Yes Yes NA Yes No Yes Yes Yes Yes Yes Yes Eosinophil countz Normal Normal NA Normal Normal High Normal High Normal High Normal NA, Not available. *Family history defined as history of allergic rhinitis and/or hay fever, AD, and/or asthma in a parent and/or sibling of the patient. Serum IgE reference range: 0 to 160 kU/L. àBlood eosinophil reference range: 0% to 7%. FUJITA ET AL 582.e9 J ALLERGY CLIN IMMUNOL VOLUME 128, NUMBER 3 TABLE E2. Characteristics of patients with psoriasis Patient no. 1 2 3 4 5 6 7 8 9 10 11 12 13 Age (y) PASI 42 60 53 47 40 26 45 38 56 43 49 58 51 NA NA NA NA 15 20 68 60 31.2 41.4 37 22.5 34.2 NA, Not available; PASI, Psoriasis Area and Severity Index. 582.e10 FUJITA ET AL J ALLERGY CLIN IMMUNOL SEPTEMBER 2011 TABLE E3. Antibodies used for flow cytometry Antigen-fluorophore HLA-DR–Alexa Fluor 700 CD207- phycoerythrin CD1a- allophycocyanin CD11c-FITC BDCA-1–phycoerythrin–Cy7 FceRIa-FITC CD3-allophycocyanin CD3-Pacific Blue CD4- phycoerythrin -Cy7 CD8-PerCp-Cy5.5 IFN-g–Alexa Fluor 700 IL-4– phycoerythrin IL-17–Alexa Fluor 488 IL-22–sllophycocyanin Manufacturer Clone* BioLegend, San Diego, Calif Immunotech, Buenos Aires, Argentina BD PharMingen, San Jose, Calif AbD Serotec, Oxford, United Kingdom Miltenyi Biotec Cosmo Bio, Tokyo, Japan BD PharMingen eBioscience, San Diego, Calif eBioscience BD PharMingen BD PharMingen BD PharMingen eBioscience R&D Systems, Minneapolis, Minn L243 DCGM4 HI149 BU15 AD5-8E7 CRA1 SK7 500A2 RPA-T4 RPA-T7 L243 8D4-8 eBio17B7 142928 FITC, Fluorescein isothiocyanate; PerCP, peridinin-chlorophyll-protein complex. *All are murine mAbs. Isotype IgG2a IgG1 IgG1 IgG1 IgG2a IgG2b IgG1 IgG2a IgG1 IgG1 IgG1 IgG1 IgG1 IgG1 Dilution 1:1000 1:100 1:100 1:50 1:50 1:20 1:500 1:40 1:200 1:50 1:200 1:20 1:20 1:20 FUJITA ET AL 582.e11 J ALLERGY CLIN IMMUNOL VOLUME 128, NUMBER 3 TABLE E4. Antibodies used for immunohistochemistry Antibody CD11c CD1c CD1a TRAIL OX40L CCL17 CCL18 CCL22 CCL20 CXCL9 *All are murine mAbs. Manufacturer Clone* BD Biosciences Miltenyi Biotec Abcam, Cambridge, United Kingdom R&D Systems R&D Systems R&D Systems R&D Systems R&D Systems R&D Systems R&D Systems B-ly6 AD5-8E7 Ab708 75402 159403 54026 64507 57226 67310 49106 Isotype IgG1 IgG2a IgG1 IgG1 IgG1 IgG1 IgG1 IgG2b IgG1 IgG1 Concentration (mg/mL) 20 10 20 20 30 10 10 10 10 10 582.e12 FUJITA ET AL J ALLERGY CLIN IMMUNOL SEPTEMBER 2011 TABLE E5. Chemokines upregulated in lesional skin of patients with AD and those with psoriasis compared with healthy skin Upregulated in patients with AD Description CCL22/MDC CCL18/PARC CXCL10/IP-10 CCL17/TARC CXCL1/GROa CCL5/RANTES CXCL8/IL-8 CCL2/MCP-1 CXCL9/MIG Upregulated in patients with psoriasis Fold change FDR Description Fold change FDR 26.54 15.14 8.46 4.86 4.53 4.41 3.39 3.32 3.14 <0.001 <0.001 0.008 0.001 0.076 0.006 0.129 0.006 0.198 CXCL8/IL-8 CXCL1/GROa CCL18/PARC CCL20/MIP-1a CXCL10/IP-10 CCL2/MCP-1 CXCL9/MIG CCL22/MDC 151.17 29.45 12.91 12.38 8.00 4.76 3.61 2.31 <0.001 <0.001 <0.001 <0.001 0.003 <0.001 0.088 0.048 Differentially expressed genes encoding chemokines were selected (fold change > 2) from the gene expression profiles of lesional skin of patients with AD and patients with psoriasis compared with those of healthy skin obtained by means of gene array analysis in our previous study.E7 P values for all chemokines listed are less than .1. FDR, False discovery rate; GROa, growth-regulated oncogene a; IP-10, IFN-g–inducible protein 10; MCP, monocyte chemotactic protein; MDC, macrophage-derived chemokine; MIG, monokine induced by IFN-g; MIP-1a, macrophage inflammatory protein 1a; PARC, pulmonary and activation-regulated chemokine; TARC, thymus and activation-regulated chemokine.