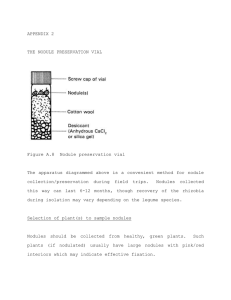
Approach to a thyroid nodule Andy Sher PGY-2 Family Medicine
advertisement

Approach to a thyroid nodule Andy Sher PGY-2 Family Medicine Case 44 y.o. woman, 2 cm nodule palpable in left lobe of thyroid gland at annual exam – smooth, non-tender. No lymphadenopathy No symptoms of hyper/hypo thyroid. No compressive symptoms Past Med Hx: HTN Meds: HCTZ Fam Hx: no hx of thyroid disease Epidemiology Palpable thyroid nodules – 4-7% of population Prevalence 19-67% - based on nodules found incidentally on ultrasound 4:1 women:men Epidemiology Geographic areas with iodine deficiency Thyroid carcinoma in 5-10% of palpable nodules Following ionizing radiation, nodules develop at a rate of 2% annually Presentation Majority are asymptomatic <1% cause hyperthyroidism Neck pressure or pain if spontaneous hemorrhage History Symptoms of hyper or hypothyroidism Previous nodules, goiters, family history of autoimmune thyroid disease, thyroid carcinoma, or familial polyposis Hashimoto’s thyroiditis – association with thyroid lymphoma History – Red Flags Male < 20 years, > 65 years Rapid growth of nodule Symptoms of local invasion (dysphagia, neck pain, hoarseness) Hx of radiation to head or neck Family hx of thyroid CA or polyposis Physical Exam Less than 1 cm usually not palpable ½ of all nodules detected by ultrasonography not detected by physical exam Should also examine for lymphadenopathy Physical Exam Smooth or nodular Diffuse or localized Soft or hard Mobile or fixed Painful or non-tender Laboratory TSH Serum calcitonin if family hx of medullary thyroid carcinoma Do not use thyroid function tests to differentiate benign from malignant Radiology Ultrasound to document size, location, and character of nodule To determine changes in size of nodules over time or to detect recurrent lesions U/S guided biopsy decreases the incidence of indeterminate specimens Radiology Thyroid scan Can not reliably distinguish benign from malignant nodules Cold nodules – 5-15% are malignant Hot nodules – almost always benign Fine Needle Aspiration Should be 1st test in the euthyroid patient Sensitivity 68-98% Specificity 72-100% False negative rate 1-11% False positive rate 1-8% Sampling errors in very large and very small nodules – minimized by u/s guided biopsy Treatment Surgical treatment indications Malignancy Indeterminate cytology and suspicious H&P Indeterminate cytology and “cold nodule” Toxic nodules (suppression of TSH, symptoms – a-fib) – can use radioactive iodine or surgery Repeated recurrence of cystic lesions Treatment Benign biopsies – can be followed without surgery and monitored q 6 months by physical exam, u/s Surveillance – change in nodule size and symptoms – repeat FNA if nodule grows. Suppression treatment Post-operative suppression treatment following resection of cancer TSH should be maintained for target of 0.5 mU per L Greater suppression for high risk patients, metastatic or locally invasive not completely removed Suppression treatment For benign solitary nodule controversial Follow at 6 month intervals Thyroxine to suppress TSH to 0.1 to 0.5 mU per L for 6-12 months After 12 months, maintain TSH in low normal range Incidental Nodule on U/S Most are benign and can be monitored without further testing FNA if nodule becomes palpable findings suggestive of malignancy on u/s larger than 1.5 cm Hx of head or neck irradiation Strong family hx of thyroid cancer Case 44 y.o. woman, 2 cm nodule palpable in left lobe of thyroid gland at annual exam – smooth, non-tender. No lymphadenopathy TSH ordered – normal Thyroid u/s – confirms 2 cm nodule, solid FNA - benign Case Repeat U/S at 1 year – nodule now 2.5 cm in size Repeat FNA – benign Could consider suppression therapy, or continue to follow.