– The Heart Chap. 19 (Cardiology) 19-1
advertisement
 19-1")
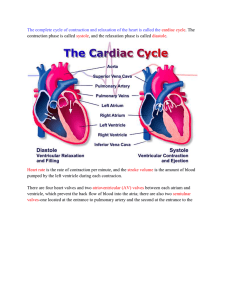
Chap. 19– The Heart (Cardiology) 19-1 Chap. 19 (Heart) Study Guide 1. Critically read Chapter 19 pp. 719-739 before 19.5 “Blood Flow” section 2. Comprehend Terminology (those in bold) 3. Study-- Figure questions, Think About It questions, and Before You Go On (sectionending) questions 4. Do Testing Your Recall— 1, 2, 4-8, 11-19 5. Do True or False– 1-4, 7, 9-10 6. Do Testing Your Comprehension-- #1 2 What are you going to do with your heart? ♥ “The best and most beautiful things in the world cannot be seen or even touched—they must be felt with the heart.” --Hellen Keller ♥ “Happiness comes only when we push our brains and hearts to the farthest reaches of which we are capable.” --Leo C. Rosten 19-3 I. Overview of cardiovascular system 19-4 § Introduction • The circulatory system— – Three component: the pump, the passageway, and the transport medium – What are they respectively? • The pump-• The passageway-• The transport medium-19-5 § Two circuits in the cardiovascular system (1) 1. Pulmonary circulation— – Function? – The route? • R. ventricle Pulmonary arteries Lungs Pulmonary veins L. atrium Figure 19.1 19-6 Lungs Pulmonary capillaries Pulmonary arteries = O2-poor blood Pulmonary circulation Pulmonary veins = O2-rich blood Right side of heart 19-7 § Two circuits in the cardiovascular system (2) 2. Systemic circulation— – Functions? – The route? (Students work on it.) • Starts which chamber of the heart? Major vessels? Destinations? Two major veins? Ends at which chamber of the heart? Fig. 19.1 19-8 Systemic circulation Left side of heart = O2-poor blood = O2-rich blood Systemic veins Systemic arteries Organ systems Systemic capillaries 19-9 II. Gross anatomy of the heart 19-10 § Shape and size of the heart • Base – broad superior portion • Apex - inferior end (a blunt point) • 3.5 in. wide at base, 5 in. from base to apex, and 2.5 in. anterior to posterior • weighs 10 oz (300 gram; size of your fist) Fig. 19.2 19-11 Aorta Superior vena cava Base of heart Apex of heart Next Topic 19-12 Diaphragm § Heart Position (1) 19-13 § Heart Position (2) 19-14 § Heart Position (3) 19-15 § Pericardial sac (pericardium) -1 • Def. the double-walled, membranous covering that encloses the heart • Function– Friction free • Peircardial fluid— Figure x Cardiac Disorders here (Table 19.3): • Pericarditis– inflammation here • Pericardial effusion– fluid in pericardial cavity • Cardiac tamponade– accumulation of fluid 16 here Figure x Pericardial cavity Heart 19-17 § Pericardial sac (pericardium) - 2 1. Parietal pericardium– 2 SUBLAYERS – A-outer, tough/fibrous layer (CT) + B-deep thin serous layer– turns inward . . . forms #2 below 2. Visceral pericardium (a.k.a. epicardium of heart wall) – INNER, thin, smooth, moist serous layer – covers heart surface 3. Pericardial cavity: between 1 + 2 above – filled with ____________________ Fig. 19.3 19-18 Functions? 3 1 2 19-19 § Heart Wall (from outermost layer) 1. Epicardium (a.k.a. visceral pericardium) – serous membrane covers heart 2. Myocardium – thick muscular layer – fibrous skeleton - network of collagenous and elastic fibers (special section for this one) 3. Endocardium - smooth inner lining – What type of epi.? Simple _________ epi. – Continuous with endothelium cells . . . Fig. 19.3 19-20 2 3 1 19-21 § Fibrous skeleton of the heart (1) – What is it? Four CT rings fuse with . . . – Structure details– Four fibrous rings, surrounds the 4 valves; in sheets of tissue that interconnect these rings – Location? In the walls between … Figure 19.8 19-22 (Rear) Right AV valve Fibrous skeleton including fibrous rings Left AV valve Aortic valve Pulmonary semilunar valve Ventricular myocardium (Front) 19-23 § Fibrous skeleton of the heart (2) Functions– – 1. Structure support-- firm base of the heart valves and openings of great vessels – 2. It anchors the cardiac muscle – 3. An electrical insulator: • Separate the atria from the ventricles and direct A.P. to specific pathways 19-24 Checkpoint Questions 1. Does most of the heart lie to the right or left of the median plane? 2. Name, in order, the three layers of the heart wall beginning with the outermost layer. 19-25 § Heart Chambers • 4 chambers— – A. right and left ATRIA – auricles? Ear-like structures . . . – B. right and left VENTRICLES • 3 sulci (grooves)— on the surface • Largely fat and coronary blood vessels – A. Atrioventricular (coronary) sulcus– B+C. Anterior and posterior interventricular sulci Figure 19.5 a+b 19-26 Coronary Anterior view sulcus? 19-27 Posterior view 19-28 § Heart Chambers – Internal (Fig. 19.7) 1. Interatrial septum – wall that separates atria 2. Pectinate muscles – internal ridges of myocardium in right atrium and both auricles; (@ absorber) 3. Interventricular septum – wall that separates ventricles Wave/sound absorber 4. Trabeculae carneae – internal ridges in both ventricles (@ absorber) 19-29 19-30 Checkpoint Questions 1. Which heart chamber has the thickest walls? What is the significance of this structural difference? 2. Do the atrial pectinate muscles more nearly resemble the ventricular papillary muscles or the trabeculae carneae? 19-31 § Heart valves (1) 1. Two atrioventricular (AV) valves— – A. Right AV valve– also called the tricuspid valve – B. Left AV valve– also called . . . • Function-blood from the atria to ventricles . .. Figure 19.8 (a,b) 19-32 Aorta Pulmonary artery Superior vena cava Pulmonary valve Pulmonary veins Right atrium Right AV valve Right ventricle Inferior vena cava Pulmonary veins Left atrium Left AV valve Aortic valve Chordae tendineae Papillary muscle Left ventricle Interventricular septum Superior views of these valves – next slide19-33 Right AV valve Left AV valve Aortic/pulmonary valve 19-34 Heart valves (2) 2. Chordae tendineae— – Structure– • Fibrous cords anchor the cusps to the ventricle walls via papillary muscles – Function– • Prevent valves from being _________ Figure 19.7, 19.8 19-35 Right atrium Chordae tendineae Right AV valve Direction of backflow of blood Septum Right ventricle Papillary muscle 19-36 Right AV valve seen from within the right ventricle 19-37 § Heart valves (3) 3.Semilunar valves include: One ______ valve and one __________ valve A. Where are they located respectively? • Major arteries leave the ventricles B. How to prevent them from everting? • Anatomical structure— leakproof “seam” C. Function– (of all valves) • Ensure unidirectional flow of blood Figure 19.7 and Fig. Z 19-38 Aorta Superior vena cava Pulmonary valve Pulmonary veins Right atrium Right AV valve Right ventricle Inferior vena cava Next slide Pulmonary artery Pulmonary veins Left atrium Left AV valve Aortic valve Chordae tendineae Papillary muscle Left ventricle Interventricular septum 19-39 (Pulmonary trunk or Aorta) Direction of backflow of blood Leakproof “seam” Aortic valve (Right or Left Ventricle) 19-40 § Valve Mechanics (Fig. 19.9, 19.19) Ventricles filling & isovolumetric contraction – AV valves open (semilunar valves close); blood flows from atria to ventricles (v. fillings) – AV valves open/closed (circle one)—S1 – ventricle pressure continues to rise – Momentarily before ventricle ejection Ventricles ejection & isovolumetric relaxation – semilunar valves open (AV valves close); – ventricle ejection; ventricle pressure drops – semilunar valves open/closed (circle one)—S2 – Isovolumetric relaxation 19-41 Operation of Atrioventricular Valves S1 19-42 Operation of Semilunar Valves S2 19-43 Before You Go On (p. 730) • Reminder: Remember to go over each question of Before You Go On in the text. • P. 730– Trace the flow of blood through the heart, naming each chamber, valve, and the great vessels in order (from the superior vena cava to the aorta). Do it yourself. Fig. 19.9 is a great figure to help you with this. 44 Fig. 19.9 Pathway of blood flow through the heart Figure 19.10 III. The Coronary Circulation 19-46 § Coronary arteries Right C.A. Left C.A. 19-47 § Coronary Arterial Supply • 1. Left coronary artery (LCA)– 2 branches – 1A--anterior interventricular branch • supplies blood to interventricular septum and anterior walls of both ventricles – 1B--circumflex branch (Fig. 19.10 a+b) • passes around left side of heart in coronary sulcus, supplies left atrium and posterior wall of left ventricle; it gives off a left marginal branch (1C) • 2. Right coronary artery (RCA)– 2 branches – 2A--right marginal branch • supplies lateral side of R atrium and ventricle – 2B--posterior interventricular branch • supplies posterior walls of ventricles 19-48 1B 2A 1A 19-49 1B 1C 2A 2B 19-50 § Anastomoses of coronary arteries 1. Definition (Anastomosis) – a point where two blood vessels join/merge; this is arterial anastomoses 2. Where? Anterior interventricular branch of LCA joins the posterior interventricular branch of RCA 3. Function– provide collateral (alternative) routes of blood supply to a tissue (the heart) Fig. x 19-51 Chest pain and Heart Attack • Angina pectoris-– partial obstruction of coronary blood flow can cause chest pain – pain caused by ischemia, often activity dependent • Myocardial infarction (heart attack)-– complete obstruction causes death of cardiac cells in affected area – pain or pressure in chest that often radiates down left arm 19-53 § Venous Drainage of Heart • 10% drains directly into right atrium and ventricle via multiple thebesian veins • 90% returns to right atrium via: (Fig. 19.10) – A. great cardiac vein • blood from anterior interventricular sulcus – B. middle cardiac vein (post. interventricular v.) • from posterior sulcus – C. left marginal vein The above three (A, B, C) empty into the coronary sinus before emptying into the ____________ (which chamber of the heart?) 19-54 A 19-55 A C B or posterior interventricular v. 19-56 IV. Cardiac conduction system 19-57 § 19.3 Cardiac muscle & conduction system Heart has its own pacemaker, nerves MODIFY the heart rate & contraction strength. • Beat rhythmically, _________beats per min. – Pacemaker? Where? (next slide) – Myogenic and autorhythmic – Regulation by autonomic nerve system 19-58 § Cardiac Conduction System (1) I. Properties – myogenic - heartbeat originates from within ____________________ – Originated from what cells (1% of heart cells)? cardiac muscles become specialized into autorhythmic cells (cardiac conduction system) – What do autorhythmic cells do?– regular, spontaneous depolarization II. Components – next slide 19-59 Cardiac Conduction System (2)– Autorhythmic cells 1. SA (sinoatrial) node: pacemaker, initiates heartbeat, sets heart rate; where? 2. AV node: electrical gateway to ventricles; where? • fibrous skeleton– insulates atria from ventricle 3. AV bundle: pathway for signals from AV node 4. Right and left bundle branches: divisions of AV bundle that enter interventricular septum 5. Purkinje fibers: upward from apex spread throughout ventricular myocardium Fig. 19.12 + X 19-60 Cardiac Conduction System 1 2 3 5 4 19-61 Students-- work on this one at home Interatrial pathway 3. Atrioventricular (AV) node 1. Sinoatrial (SA) node 4. Bundle of His or AV bundle Right atrium 5b. Left branch of bundle of His 2. Internodal pathway 5a. Right branch of bundle of His Left ventricle Right ventricle 6. Purkinje fibers 19-62 Checkpoint Question Which chamber of the heart is first to receive the electrical signal that induces the heart to contract? 63 V. Cardiac muscle 19-64 § Cardiac vs. skeletal m.(1) Skeletal M. Cardiac M. (cardiocyte) Fibers & their control •Fibers independent •Voluntary •Interlocking cells; (next) •Involuntary Nervous control by •Somatic motor • Autonomic neurons nervous sys. Initiation of contraction •Requires input • by from motor autorhythmic neurons cells in heart 65 § Cardiac vs. skeletal m.(2) 1. Cardiac myocytes—size, thickness etc. 2. T (transverse) tubules– smaller 3. Presence of intercalated discs– (see next slide) 4. Mitochondria— 5. Myoglobin and glycogen-66 § Intercalated discs (of cardiac muscle cells) • Def. specialized zigzag structures joining cardiac muscle cells end to end • Containing three distinctive features not found in skeletal muscle; what are they? Figure 19.11 a-c 67 Figure 19.11a light micrograph Next slide 19-68 One myocyte is shown (colored). 19-69 2 1 3 Structure of an intercalated disc 1-- interdigitating folds 2—mechanical junctions– two types; fascia adherens and desmosomes 3—electrical (gap) junctions-19-70 Plasma membranes of adjacent cardiac muscle fibers Desmosome Fascia adherens Gap junction Intercalated disc Action potential 19-71 § Intercalated discs 1. Function of interdigitating folds-- 2. Functions of fascia adherens and desmosome – • Types of adhering junction • Mechanically, hold cells together 72 § Intercalated discs 3. Functions of gap junction (connexons): • Allows action potentials to spread . . . • Therefore, cardiac cells form functional syncytia— cardiac cells excited and contract as a single unit Q--Does the atria and the ventricle each form a separate unit? 73 VI. Electrical activity of heart (autorhythmic cells) 19-74 § 19.4 Heart Autorhythmic Cells 1. Two types of cardiac muscle cells: A. 1% are autorhythmic cells (our focus on this section)– – Function? • AP— Yes • Contraction– No B. 99% --contractile cells – Function? • AP— No initiation of own Action Potential • Contraction– Yes 19-75 § Heart autorhythmic cells 2.Autorhythmic cells act as pacemaker: • How? Their m. potential slowly depolarizes (drifts) between AP, until . . .… Figure 19.13 19-76 B C A Pacemaker potentials & action potentials of the SA node 19-77 § Heart autorhythmic cells 3. Details of pacemaker activity: (vs. AP in nerve and skeletal m.): A. Slow depolarization: i. K+ voltage-gated channels slowly close ii. (No voltage-gated Na+ channels), instead sodium leak channels are used; So, sodium ions move in/out iii. Transient Ca+2 channels open—Calcium ions move inward All these make the inside becomes depolarized Thus, pacemaker p. toward 19-78 threshold § Heart autorhythmic cells B. Rising phase of the action potential: • Once, reach threshold p., longlasting Ca+2 channels open; . . . • Influx of calcium ions C. The falling phase: • as usual, potassium ions efflux 19-79 § Heart autorhythmic cells 4.Autorhythmic cells are self excitable: – Without nervous stimulation – They initiate AP cyclically, which trigger rhythmic beating – Each depolarization of SA node sets off one heartbeat (every 0.8 sec.) – They form the conduction system of the heart (see Figure 19.12) – It excites the other components in the system 19-80 § Heart autorhythmic cells 5. The spread of cardiac excitation: In a coordinated sequence: A-First, atrial excitation– From SA node to atria; How? through gap junctions; via internodal and interatrial pathways as well; Result– a single smooth contraction of the pair of atria (Fig. Y) B-Second, from the atria to the ventricles— AV node is the only point of electrical contact from the atria to the ventricles C-Finally, ventricular excitation-from AV node to the bundle of His, . . . Result– a single smooth contraction in 19-81 ventricles Interatrial pathway Right atrium Left atrium 1st beat SA node Internodal pathway Bundle of His AV node 2nd beat Purkinje fibers Right ventricle Left ventricle 19-82 VII. contractile activity of heart 19-83 Our focus 19-84 § Cardiac contractile cells 1. Action potential is initiated by: the pacemaker cells 3 phases: – Rising – Plateau –… 85 § Cardiac contractile cells 2.The detail of action potential: A.Rising phase • Massive sodium ions influx causes depolarization and AP B.Plateau phase • Primarily caused by opening of calcium channels • Also caused by temp. reduction in outflow of _____________ ions 86 § Cardiac contractile cells C.Falling phase • Primarily caused by ____________ outflow • Closing of calcium channels contribute to this as well 87 Review slide— ID A, B, C, D, E below B C A D E 19-88 § Cardiac contractile cells 3.Contractile response Compare to skeletal muscle: • Longer period of cardiac contraction • Longer refractory period How? Why? (next) Action potential Contractile response Refractory period 89 § Cardiac contractile cells A.Longer period of cardiac contraction – 3x longer compared to skeletal m. – Caused by entry of calcium ions which induce more calcium ions release from the sarcoplasmic reticulum – Purpose– this increased contractile time ensures emptying blood into ventricles and arteries Fig. 11.13 (skeletal muscle) 90 Latent period Contraction Relaxation time time In skeletal muscle Muscle twitch Contractile response Action potential 19-91 Stimulation § Cardiac contractile cells B.Longer refractory period • Caused chiefly by inactivation of the sodium ion channels • Consequences/Purpose– Cardiac muscle cannot be re-stimulated until contraction is almost over, therefore summation and tetanus of cardiac m. is impossible • This ensures . . . Compared to Fig. 11.13 (Shown previously; in skeletal m.) 92 § ECG (Electrocardiogram) 1. Def. A record of the overall electrical activity in all the cardiac muscle cells from the body surface – NOT a recording of a single action potential in a single cell – ECG recording represents . . .electrical activity detected by electrodes at 2 different points Figure 19.15 (ECG) 93 § ECG (Electrocardiogram) 2.Components of the ECG correlate to cardiac events (Fig. 19.16 in the next slide) • P wave— atrial depolarization when the electrical impulse spreads across the atria • QRS complex— • T wave— ventricular repolarization R T P P Q S 95 P T QRS 19-96