State of the Science Workshop: Low Dose-Response Extrapolation for Environmental Health Risk Assessment
advertisement

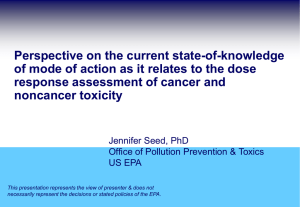
State of the Science Workshop: Low Dose-Response Extrapolation for Environmental Health Risk Assessment Mary Fox, PhD, MPH Ronald White, MST Risk Sciences and Public Policy Institute Johns Hopkins Bloomberg School of Public Health Society of Toxicology Risk Assessment Specialty Section January 14, 2009 Contemporary Principles of Risk Assessment • Risk assessment involves a critical analysis of available scientific information – Chemical/pollutant toxicity (hazard identification) – Exposure assessment – Dose - response assessment – Risk Characterization (cancer/non-cancer risk metrics – “safe” levels) • Quantitative risk metrics are ideally – Biologically-based – Data-driven • When there is insufficient data, default methods are used that – Ensure scientific validity (i.e., scientifically plausible and extensively peer-reviewed) – Create an orderly and predictable process – Protect public health (account for uncertainties) EPA 2004; Preuss 2006 Dose - Response Assessment R e s p o n s e 0 Observable Range Range of Inference Dose State-of-the-Science Project on Low DoseResponse Extrapolation in EH Risk Assessment • Increasing biological knowledge and analytical capabilities are challenging existing dose-response assessment procedures • Project provides opportunity to: – Summarize the current body of science – Integrate multi-disciplinary expertise – Advance the field • Funded by U.S. Environmental Protection Agency Background Information Document • Prepared by Johns Hopkins Bloomberg School of Public Health • Literature review – 889 papers (1953 - 2006) compiled, covering broad scope of topics related to workshop issue. • Selected key studies annotated • Historical review of low dose extrapolation in EH risk assessment • Discussion of key concepts and approaches • Preliminary findings and conceptual approach • Case studies: ambient & diesel particulate matter, radon, naphthalene State-of-the-Science Workshop: Issues and Approaches in Low Dose–Response Extrapolation for Environmental Health Risk Assessment April 23 - 24, 2007 Baltimore, Maryland, U.S.A. Co-Chairs Ila Cote, U.S. Environmental Protection Agency Jonathan M. Samet, Johns Hopkins Bloomberg School of Public Health Participants Linda S. Birnbaum, U.S. Environmental Protection Agency Thomas A. Burke, Johns Hopkins Bloomberg School of Public Health Kenny S. Crump, Environ Corp Francesca Dominici, Johns Hopkins Bloomberg School of Public Health Elaine M. Faustman, University of Washington School of Public Health & Community Medicine Mary Fox, Johns Hopkins Bloomberg School of Public Health Seymour Garte, University of Pittsburgh Cancer Institute Dale B. Hattis, Clark University Ralph L. Kodell, University of Arkansas for Medical Sciences Frederick J. Miller, consultant Peter Preuss, U.S. Environmental Protection Agency Louise M. Ryan, Harvard School of Public Health Paul D. White, U.S. Environmental Protection Agency Ronald H. White, Johns Hopkins Bloomberg School of Public Health Lauren Zeise, California Environmental Protection Agency Provided by D. Hattis Outline • Where we’ve been – Current approaches and their origins • What we’re doing and learning – Mode of action – Refinements – Interindividual variability – Additivity to dose and on-going disease process • Workshop discussions Origins of ‘Linear No Threshold’ (1) • One ‘hit’ to DNA in one cell… • Studies of Japanese atomic bomb survivors in 1950’s • Marked differences in individual response to carcinogens (individual thresholds) are not a basis for predicting a no-effect level in other individuals (IRLG 1979) Origins of ‘Linear No Threshold’ (2) Additivity to Background • Under the assumption of additivity to background, even for dose-response models that do not exhibit linearity, the low-doseresponse will approximately linear at low-doses (Crump et al 1976,Hoel 1980,Krewski and Van Ryzin 1981). • That is true for any doseresponse model that is increasing in d, because its first derivative at the background dose will be positive and therefore the curve will be “locally” linear. Origins of the “Threshold” (Lehman and Fitzhugh 1954) • Biological resilience, adaptability, repair • When using animal data to set a human “safety” standard – Animals are more resistant to toxics – Considerable variations within a species; animals tested are homogeneous, healthy – Reviewed data supporting 10-fold difference for resistance and variability (a.k.a inter- and intra-species “uncertainty factors”) Definition: Mode of Action “A mode of action is composed of key events and processes starting from the interaction of an agent with a cell, and through operational and anatomical changes, resulting in cancer formation. “Mode” is contrasted to “mechanism” of action, which implies a more detailed understanding and description of events than is meant by mode of action.” EPA Guidelines for Carcinogen Risk Assessment, 2005 Advances in Understanding Mode of Action (MOA) Continuum of Practice: Mode of Action • Pharmacokinetic models to extrapolate dose across species • Pharmacodynamic understanding qualitatively evaluate effects across species • Well-developed biologically based doseresponse models (few) Refinements to Inputs: “Uncertainty Factors” Inter-individual Variability Hattis et al. 1999 Refinements to Procedures: Benchmark Dose A devil in the details Procedure (Crump 1984); Figure (Rodricks 2007) State of Practice: UF and Procedures • Pharmacokinetic or dynamic information used to determine UF when available • Benchmark dose approach applied moreor-less routinely but results not always used in risk assessment State of the Science: Statistical Research • Sources of uncertainty in extrapolation to low doses – Statistical (overwhelming majority of statistical literature) – Choice of model (most important uncertainty amenable to statistical investigation) – Uncertainty in mode of action – Uncertainty in additivity to background expo and biological processes – Uncertainty in animal to human extrapolation State of the Science: Quantitative Methods • Increasing interest in and application of – Probabilistic methods and simulations – Bayesian/Hierarchical models MOA, Additivity, Repair and Inter-individual Variability Conolly et al. 2005 Conclusions: State of the Science • Research and risk decision making should be based on a mode-ofaction hypothesis when possible • There is a growing body of evidence critical of the “threshold” doseresponse model as a population-protective default • Multiple dose-response shapes are to be expected in the population • There is recognition that better modeling requires more data and that biologically-based dose-response models for the majority of chemicals of regulatory concern will not be available for some time (ever?) • There are competing ideas on how to address dose-response modeling and extrapolation to low doses for risk assessment • Extrapolation (risk estimation) for all toxicities • Benchmark dose approach for all toxicities given the considerable uncertainties Workshop Discussions: Major Topics • How/if to do biologically based DR modeling • New/Alternative approaches to DR • Mode of action – Promise/Pitfalls – Evaluating evidence of MOA • Statistical methods • Research needs Debate: BIOLOGICAL DATA IN MODELS • TWO DIVERGENT VIEWS – INCORPORATION OF BIOLOGICAL DATA INTO RISK ASSESSMENT MODELS IS USEFUL AND/OR NECESSARY – SUCH USE OF BIOLOGICAL DATA IS HOPELESS FOR QUANTITATIVE LOW DOSE RISK ESTIMATION Approaches Discussed (1) • CATEGORICAL APPROACH TO A PRIORI - MODEL SELECTION BASED ON MECHANISM • HATTIS CATEGORIES 1. LOW DOSE REVERSIBLE MECHANISM 2. SMALL NUMBER OF IRREVERSIBLE EVENTS (MUTATIONS) 3. CHRONIC CUMMULATIVE LARGE NUMBER OF IRREVERSIBLE EVENTS Approaches Discussed (2) • USE OF LINEAR LOW DOSE NO THRESHOLD EXTRAPOLATION AS A DEFAULT WITH ADJUSTMENT OF SLOPE WITH MECHANISTIC DATA (CRUMP 1) • POINT OF DEPARTURE (eg. ANIMAL DATA) WITH UNCERTAINTY FACTORS BASED ON MECHANISM, SEVERITY ETC. TO ARRIVE AT AN ADVISORY LEVEL WITHOUT A RISK ESTIMATE (CRUMP 2) Approaches Discussed (3) :New Low Dose Linear Formulation (Zeise) RiskH = SlopeBMD × MS × FH-A × D where - RiskH is the low dose human risk. - SlopeBMD is the slope of the dose response curve at what would be chosen as the benchmark dose under the current practice - MS adjusts for the differences in slope at the high dose compared to low dose (0 MS 1) - D is the dose - FH-A adjusts for interspecies differences. Zeise 2007 Zeise Alternative: Base Model Incorporating Uncertainty and Variability RiskH = SlopeBMD × MS × FH-A × D × U Log Risk = log SlopeBMD + log MS + log FH-A + log D + e • where the random variable e is distributed normally with mean zero and variance 2. Thus, for this simplistic case, • 2 = 2 logSlope + 2 logM + 2 logF + 2logD RiskH yth = SlopeBMD × MS × FH-A × D × VH yth × U where VH yth is the yth quantile of the distribution that describes the ratio of the yth percentile individual to the median individual. Zeise 2007 The ultimate goal is to enable expressions such as “the risk of effect does not exceed x level for the yth percentile individual, stated with confidence z%” Additivity to Background Risk • IF THERE IS EVIDENCE FOR ADDITIVITY TO BACKGROUND, LINEAR NO THRESHOLD IS APPROPRIATE • THERE ARE IMPORTANT SITUATIONS IS WHICH ADDITIVITY DOES NOT OCCUR. Focus on Mode of Action • 1980s: Rationale for risk assessment based on additivity to ongoing processes (vs independence), population variability and statistical considerations lead to low dose linear modeling for carcinogens • Early 2000s: Emphasis on defining mode of action (MOA) with expectation that such information would answer dose-response questions • Challenge: How can considerations of MOA be combined with basic disease causation issues (population variability and background processes)? MOA: Promise and Pitfalls Determine human relevance (yes/no) Allows deviation from defaults Build unified models (all relevant processes) Diversity in human population complicates answer Lack of data (MOA research not addressing key info, e.g., additivity to ongoing processes) Not there yet Current Criteria for MOA Evidence Assessment • “Hill criteria”: temporality, strength of association, specificity, consistency, coherence—developed for consideration of observational evidence. • Hill criteria of uncertain relevance to evaluating evidence on mode or mechanism of action • Need for new criteria? Assessing Weight of Evidence for MOA • Formal and transparent process for gathering relevant evidence • Systematic approach for assessing the quality of the evidence • Approaches for combining evidence, e.g., metaanalysis • Criteria for evaluating the informativeness of the evidence • Standard terminology for classifying the strength of evidence. An Example Classification Scheme • Evidence on MOA is sufficient to inform development of a biologically-based model; • Evidence on MOA is sufficient to support a particular dose-response model • Evidence on MOA is suggestive in supporting a particular dose-response model • Evidence on MOA is insufficient to inform the selection of the dose-response model/shape Discussion: Statistical Modeling • Model choice is challenging, even if MOA is known • Model averaging may avoid need to chose a single model • Models that combine data from multiple endpoints and/or multiple studies – Gain power/precision – Inform biology – Help quantify uncertainty • Research needed on how to incorporate biomarkers, especially high dimensional genomics data • Greater effort to understand mechanism may be needed if effects seen in animal studies are close to exposures seen in humans Discussion: Bayesian Model Averaging • Specify a set of suitable models, usually weighted equally a priori • Compute “posterior” model probabilities, reflecting the likelihood that a model holds, given the observed data • Average the results with respect to these posterior probabilities – “bad” models get downweighted, several “good” models can contribute. (Example presented used method of Carlin and Chib 1995.) Discussion: Epi vs Animal Studies • Epi studies avoid inter-species problem, but many other problems (Measurement error, confounding) • Default approaches developed for risk assessment based on animals may not work for epi data – Appropriate point of departure generally lower (10% typical for animal studies maybe at upper end of dose range for human studies) – Application of standard uncertainty factors may lead to infeasibly low exposure levels On Bioassays • Current bioassays – Expensive – Fewer being conducted – Generate limited data to support BBDR models and quantitative risk assessments – Provide limited insights on MOA Better Bioassays: Design Considerations • Serially kill animals • Include endpoints critical for BBDR models (cell proliferation, lesion location, toxicogenomics) • Incorporate endpoints likely to help identify, refine MOA • Preserve tissue for future research – So new methodologies can be applied or other endpoints can be assessed – Link to comparable human responses, e.g., proteomics Discussion Highlights • From MOA to risk (dose-response) model—how? – Families of MOA based models (Hattis) – New/refined default models, e.g., Crump and Zeise alternatives – Operational definition of MOA • Approach for evaluating and classifying evidence related to MOA – Need systematic approach – Relevance of Hill criteria for this purpose? • Statistical Methods – BMA is a tool for quantifying uncertainty in the shape of the dose-response for extrapolation of risk at low doses (that is, at dose levels below the observable ranges) – Averaged model may reflect true population heterogeneity – Methods for data integration, combined models • Considerations when extrapolating to low doses • Consider additivity (vs not) to background (exposure & bio process) • Consider population variability • Does this suggest a LNT default for non-cancer effects? A Controversial Topic • Linear No-Threshold Default Assumption for All Toxicities • Controversial but not new – See Biological Effects of Low Level Exposure (BELLE) newsletter vol. 6, no. 1, March 1997 • http://www.belleonline.com/newsletters/volume6/vol6-1.html – Useful for first pass screening (R. Wilson), reasonable for public health purposes where there is no evidence to the contrary (D. Hoel) – Does not mean that low-dose slope should be same as high-dose slope • Since then … – Results from population studies – Informative for this controversy? – Residential radon exposure, Criteria pollutants, ETS, Pb Residential Radon Exposure and Lung Cancer Krewski et al. 2006 Ozone and Mortality Bell et al. 2006 PM10 and Mortality 8 8 10 U.S. Cities (Schwartz and Zanobetti 2000) 8 Spanish Cities (Schwartz et al. 2001) b 6 % increase in deaths % increase in deaths a 4 2 0 6 4 2 0 0 20 40 60 80 100 0 20 40 3 80 100 BS (g/m ) 8 8 20 U.S. Cities (Daniels et al. 2000; Dominici et al. 2003) c 6 88 U.S. Cities (Dominici et al. 2002; Dominici et al. 2003) d % increase in deaths % increase in deaths 60 3 PM10 (g/m ) Selected PM10 concentrationresponse relationships from various multi-city daily timeseries studies. (Adapted from original publications and rescaled for comparison.) 4 2 0 6 • Schwartz and Zanobetti 2000 • Schwartz et al. 2001 4 • Daniels et al. 2000 2 0 0 20 40 60 80 100 0 20 40 3 60 80 100 3 PM10 (g/m ) PM10 (g/m ) • Dominici et al. 2002 • Dominici et al. 2003 8 22 European Cities (Samoli et al. 2005) % increase in deaths e • Samoli et al. 2005 6 4 2 0 0 20 40 60 80 100 120 140 160 180 200 220 1.4 1050 a 1000 b U.S. cross-sectional mortality Adjusted mortality relative risk 1980 adjusted mortality(deaths/yr/100,000) PM2.5 and Mortality, Children’s Lung Growth 950 900 850 800 750 700 650 1.3 Harvard Six-cities (Laden et al. 2006) Period 1 (upper case) 1.2 H L 1.1 h T 1.0 p P 10 15 20 25 W s t Period 2 (lower case) l 0.9 w 0.8 5 S 30 5 10 3 PM2.5 (g/m ) 15 20 25 30 25 30 3 PM2.5 (g/m ) 1.4 1.3 ACS cohort (Pope et al. 2002) Cardiopulmonary 1.2 1.1 All cause 1.0 All other 0.9 Children's Lung Growth (Gauderman et al. 2004) d 12 Lung Cancer FEV1 <80% of predicted (%) Adjusted mortality relative risk c 10 8 6 4 2 0 0.8 5 10 15 20 3 PM2.5 (g/m ) 25 30 5 10 15 20 3 PM2.5 (g/m ) Figure 2. Selected PM2.5 concentration-response relationships from studies of long-term exposure. (Adapted from original publications and rescaled for comparison.) (Pope et al. 2002; Gauderman et al. 2004; Laden et al. 2006) Tobacco Smoke, Lead Exposure and Multiple Outcomes • Report of the Surgeon General 2006 – “The scientific evidence indicates that there is no risk free level of exposure to second-hand smoke.” • CDC 2005 – “…data demonstrating that no “safe” threshold for blood lead levels in young children has been identified…” The Controversial Topic • An argument for a ‘no-threshold’ default for noncancer outcomes • Significant Implications – A change in risk assessment practice to reflect growing knowledge – A significant change in regulatory approach to identify protective exposure levels Workshop Recommendations: What We Can Do Now • Develop operational definition of MOA • Develop approaches for evaluating evidence on MOA • Incorporate variability, background incidence and background exposures to current doseresponse models • Adjust for severity with uncertainty factors • Use model averaging Workshop Recommendations: Research Needs • As information on MOA advances – translate into dose-response models • Attention to background risk in MOA-based research • Explore statistical approaches to model selection (e.g. model averaging) • What are the implications for risk assessment practice? • Develop hybrid modeling approaches to integrate data across multiple species and health endpoints/outcomes Workshop Report State-of-the-Science Workshop Report: Issues and Approaches in Low Dose–Response Extrapolation for Environmental Health Risk Assessment Ronald H. White (JHU), Ila Cote (EPA), Lauren Zeise (CA EPA), Mary Fox (JHU), Francesca Dominici (JHU), Thomas A. Burke (JHU), Paul D. White (EPA), Dale B. Hattis (Clark U), Jonathan M. Samet (JHU) Environmental Health Perspectives (On-line), 19 September, 2008. A Recent Development Science and Decisions: Advancing Risk Assessment (NAS 2008) – Unification of cancer and noncancer dose-response assessment approaches • Noncancer effects do not necessarily have a threshold, or lowdose nonlinearity, and the mode of action of carcinogens varies. • Background exposures and underlying disease processes contribute to population background risk and can lead to linearity at the population doses of concern. • Recommends a consistent, unified approach for doseresponse modeling that includes formal, systematic assessment of background disease processes and exposures, possible vulnerable populations, and modes of action that may affect a chemical’s dose-response relationship in humans. • RfD or RfC redefined as “risk-specific dose”