The Effect of Risk-Based Capital Formulae on South African Medical Scheme Solvency
advertisement

Centre for Actuarial Research
(CARe)
A Research Unit of the University of Cape Town
The Effect of Risk-Based Capital
Formulae on South African
Medical Scheme Solvency
CARe Discussion Paper
prepared for the Council for Medical Schemes
by John Kendal, supervised and edited by Heather McLeod
May 2004
Centre for Actuarial Research
University of Cape Town
Private Bag
Rondebosch
7701 SOUTH AFRICA
Telephone: +27 (21) 650-2475
Telephone for Professor McLeod : +27 (28) 572-1933
Fax: +27 (21) 689-7580
E-mail: care@commerce.uct.ac.za
E-mail for Professor McLeod : hmcleod@iafrica.com
Editor’s Note
John Kendal submitted this work as his Honours research project in the Actuarial
Science Department at the University of Cape Town in 2003. John obtained a first for
his project (a rarity in Actuarial Science) and his work was submitted as one of the
best national actuarial projects in that year.
The purpose of his research was to ‘compare and explain’ the Australian and USA
risk based capital (RBC) systems and investigate, using the 2000 statutory returns
from the Office of the Registrar of Medical Schemes, the impact of application of
these systems in South Africa.
The most valuable and long-lasting part of this work is the definition of the data items
in the statutory returns to the Registrar that should be used in the RBC formulae from
the USA and Australia. This mapping was no small feat and this diligent work will
provide a valuable platform for the development of recommendations on a possible
RBC formula for South Africa.
In areas where there was no equivalent data item in South Africa, the author has
suggested an appropriate definition or indicated whether it is a meaningful omission.
This work was placed in Appendices C, D and E but should probably have merited a
chapter in its own right.
This is a very useful research report which will lay the foundations for RBC work in
medical schemes in the years to come.
The most important research work now needed is to determine the required overall
level of solvency for South African medical schemes. Work also needs to be done on
how the solvency standard for healthcare funds differs from the standard for managed
care organisations (the NAIC formula) in the USA and how this might be applied in
South Africa.
Once agreement is reached on the overall solvency needed in South African medical
schemes and managed care organisations, it will then be possible to undertake further
research on the appropriate level of certain key parameters in the formulae, based on
South African evidence.
Professor Heather McLeod
May 2004
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page ii
Synopsis
Risk-based capital (RBC) is a level of capital that enables a medical scheme to
withstand certain adverse fluctuations in results. It is determined by the risks facing a
scheme. This report examines two foreign methods for calculating RBC requirements
and estimates the impact a RBC system would have on South African medical scheme
solvency.
The USA and Australian RBC systems
The USA RBC system for Managed Care Organisations (MCO’s) is incredibly
detailed, but remarkably simple. It is based on a certain probability of ruin and
determines the RBC for an MCO, known as risk-based capital after covariance, by
multiplying its various balance sheet and income statement items by risk factors. A
special feature of this system is its allowance for risk-transfer through managed care
arrangements and reinsurance contracts.
The Australian system requires insurers to hold capital to meet certain circumstances.
This system resembles the current RBC system for South African life insurers and
would probably be similar to any RBC system developed for South African medical
schemes. It requires insurers to hold an amount of capital (i.e. the solvency reserve)
that will enable the fund to meet its current obligations if the fund was closed to new
business and run-off. It also requires the fund to hold sufficient capital (i.e. the capital
adequacy reserve) to meet its obligations as a going concern. Special features of this
system are its interaction with the Australian risk-equalisation system and its
specification of a method to estimate outstanding claims.
Impact of RBC on South African medical scheme solvency
Since no RBC system has been developed specifically for the South African medical
scheme industry, the impact of RBC on South African medical scheme solvency was
estimated by calculating the USA and Australian RBC requirements for South African
medical schemes using 2000 statutory returns data.
At the industry level, it is unclear whether a RBC system would require the industry
to hold more or less capital than the current 25% of gross contributions rule. The USA
RBC after covariance is less than 25% of gross contributions, while the Australian
solvency and capital adequacy reserves straddle the current requirement.
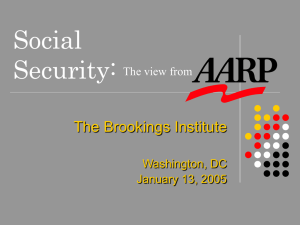
The figure below shows the USA and Australian RBC requirements as a percentage of
gross contributions for individual schemes.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page iii
70
Risk-based capital after covariance
Solvency reserve
60
Capital adequacy reserve
Accumulated funds
Number of schemes
50
40
30
20
10
0
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
55%
60%
65%
70%
75%
80%
85%
90%
95% 100% More
Percentage of gross contributions
Under both systems, some schemes are allowed to hold less than 25% of gross
contributions while others are required to hold significantly more. This implies that
some schemes would be strongly against a RBC system while others (especially the
larger schemes) would support it.
Conclusions
Despite the differences between the two foreign systems, they each have features that
could be useful in the South African environment. They also suggest what changes
should be made to the life insurance standards to make them applicable to medical
schemes. In addition, it appears that each RBC system will have a unique effect on
solvency at the industry level.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page iv
Table of Contents
Editor’s Note.................................................................................................................ii
Synopsis ........................................................................................................................iii
Table of Contents ......................................................................................................... v
Glossary .....................................................................................................................viii
1.
Introduction .......................................................................................................... 1
1.1
1.2
1.3
1.4
1.5
1.6
1.7
2.
Risk-Based Capital............................................................................................... 3
2.1
2.2
2.3
2.4
3.
Background to Research Project .................................................................... 1
Statement of Research Project ....................................................................... 1
Objectives of Research Project ...................................................................... 1
Sources of Information .................................................................................. 1
Scope and Limitations of Project ................................................................... 2
Plan of Development...................................................................................... 2
Acknowledgements ........................................................................................ 2
Introduction to Risk-Based Capital ................................................................ 3
Medical Scheme Risk .................................................................................... 4
Calculation of RBC Requirements................................................................. 5
Desirable Features of a RBC System ............................................................. 6
The USA RBC system for Managed Care Organisations ................................ 8
3.1
Introduction to the USA RBC System ........................................................... 8
3.2
Asset Risk – Affiliates ................................................................................... 9
3.3
Asset Risk – Other ....................................................................................... 10
3.3.1
Fixed income assets ............................................................................. 11
3.3.2
Replication transactions ...................................................................... 11
3.3.3
Equity ................................................................................................... 12
3.3.4
Property and equipment assets ............................................................ 12
3.3.5
Asset concentration .............................................................................. 13
3.4
Underwriting Risk ........................................................................................ 15
3.4.1
Base Underwriting risk RBC ............................................................... 15
3.4.2
Underwriting risk RBC after managed care discount ......................... 15
3.4.3
Alternative risk charge ......................................................................... 17
3.5
Credit Risk ................................................................................................... 18
3.6
Business Risk ............................................................................................... 21
3.7
Risk-Based Capital After Covariance .......................................................... 23
3.8
Transitional Arrangements........................................................................... 25
4.
The Australian RBC System for Private Health Insurers ............................. 27
4.1
4.2
4.3
4.4
CARE
Introduction to the Australian RBC System ................................................ 27
Solvency Liability ........................................................................................ 29
Expense Reserve .......................................................................................... 31
Inadmissible Assets Reserve ........................................................................ 32
Effect of RBC Formulae on Medical Scheme Solvency
Page v
4.5
4.6
4.7
4.8
4.9
4.10
4.11
4.12
5.
Resilience Reserve ....................................................................................... 34
Management Capital Amount ...................................................................... 35
Capital Adequacy Liability .......................................................................... 36
Renewal Option Reserve.............................................................................. 39
Business Funding Reserve ........................................................................... 40
Subordinated Debt Allowance ..................................................................... 40
Solvency and Capital Adequacy Reserves ................................................... 42
Transitional Arrangements........................................................................... 42
The effect of RBC on South African Medical Scheme Solvency ................... 44
5.1
Methodology ................................................................................................ 44
5.2
Industry Level .............................................................................................. 44
5.2.1
Aggregate solvency .............................................................................. 44
5.2.2
Aggregate solvency by scheme type ..................................................... 45
5.2.3
Aggregate solvency by scheme size...................................................... 47
5.3
Individual Scheme Level ............................................................................. 48
5.3.1
Range of individual scheme capital requirements ............................... 48
5.3.2
Individual scheme solvency by scheme type ........................................ 49
5.3.3
Individual scheme solvency by scheme size ......................................... 49
5.4
Summary ...................................................................................................... 50
6.
A Comparison of the Australian and USA RBC Systems .............................. 52
6.1
Conceptual Framework ................................................................................ 52
6.1.1
Probability of ruin................................................................................ 52
6.1.2
Capital to meet specific circumstances ................................................ 52
6.1.3
Suitable conceptual framework for a South African RBC system........ 53
6.2
Components of Each Formula ..................................................................... 53
6.2.1
Omissions from the USA formula ........................................................ 54
6.2.2
Omissions from the Australian formulae ............................................. 54
6.2.3
Relative sizes of the different components ........................................... 54
6.3
Special features of each formula .................................................................. 55
6.3.1
Special features of the USA formula .................................................... 55
6.3.2
Special features of the Australian formulae......................................... 57
6.4
Meeting the requirements ............................................................................ 57
6.5
Basis for intervention ................................................................................... 57
7.
Conclusions and Further Research .................................................................. 58
8.
References and Bibliography ............................................................................ 59
8.1
8.2
8.3
8.4
Australia ....................................................................................................... 59
United States of America ............................................................................. 60
South Africa ................................................................................................. 61
General ......................................................................................................... 62
Appendix A: Data Files Submitted to the Council for Medical Schemes ............. 63
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page vi
Appendix B: RBC Theory ......................................................................................... 64
B1. Calculation of RBC requirements using the EPD and probability of ruin
approaches................................................................................................................ 64
B1.1 Ruin Approach ............................................................................................. 64
B1.2 Expected policyholder deficit (EPD) approach .......................................... 65
B1.3 More complicated situations ....................................................................... 66
B2. Estimating factors by simulation ....................................................................... 66
B3. Solvency liability margin .................................................................................. 67
Appendix C: Method used to calculate the USA RBC Requirement .................... 69
C1. Statutory returns data used in the calculation.................................................... 69
C2. Treatment of the different types of guarantee ................................................... 71
C3. Assumptions and adjustments to the formula ................................................... 72
C3.1 Premium tiers .............................................................................................. 72
C3.2 Alternative risk charge ................................................................................ 73
Appendix D: Method used to calculate the Australian Solvency Reserve ............ 74
D1. Statutory returns data used in the calculation ................................................... 74
D2. Assumptions and adjustments to the formula ................................................... 75
D2.1 Asset concentration risk .............................................................................. 75
D2.2 Resilience reserve ....................................................................................... 75
D2.3 Management capital amount ....................................................................... 77
Appendix E: Method used to calculate the Australian Capital Adequacy Reserve
...................................................................................................................................... 78
E1. Statutory returns data used in the calculation .................................................... 78
E2. Assumptions and adjustments to the formula .................................................... 79
E2.1 General ........................................................................................................ 79
E2.2 Capital adequacy margin ............................................................................ 79
E2.3 Renewal option reserve ............................................................................... 81
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page vii
Glossary
Accumulated funds
The net asset value of a medical scheme, excluding funds set aside for specific
purposes and unrealised non-distributable reserves.
Affiliates
“A person or entity that directly, or indirectly through one or more other persons or
entities, controls, is controlled by, or is under common control with the reporting
entity.” (NAIC, 2001, 33)
Capital (also equity or net asset value)
For the purposes of this report, capital is defined to be total assets minus total
liabilities. Therefore, the terms capital, equity and net asset value will be used
interchangeably throughout this report.
Gross contributions
“Gross contributions are amounts (premiums) payable by members and/or employers,
in terms of the rules of the medical scheme, for the purchase of healthcare benefits.
Gross contributions include, savings plan contributions.” (SAICA, 2003, p.53)
Healthcare receivables
“Fee-for-service, coordination of benefits and subrogations, co-payments, and other
health balances.” (NAIC, 2001, p.34)
IBNR claims liability
This is the liability for future payments in respect of claims that have already been
incurred by the medical scheme but not yet reported in the scheme’s records, as well
as the expected future development on reported claims (ASSA, 2003).
Managed care
Refers to the use of management techniques to deliver appropriate healthcare in a
cost-effective manner, through the use of risk-sharing contractual arrangements with
healthcare providers and various other healthcare expenditure management
techniques.
Managed care healthcare benefits
This is the cost of healthcare services under payment systems such as capitations and
other contractual arrangements (SAICA, 2003)
Managed care management services expenses
This is the cost to the medical scheme of healthcare expenditure management services
such as disease and case management, pre-authorisation and bill review. This does not
include the cost of any healthcare services. (SAICA, 2003)
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page viii
Managed care organisation
“Any person, corporation or other entity which enters into arrangements or
agreements with licensed medical providers or intermediaries for the purpose of
providing, or offering to provide, a plan of health benefits directly to individuals or
employer groups in consideration for an advance periodic charge (premium) per
member covered.” (NAIC, 2001, p.34)
National Association of Insurance Commissioners
The regulator of, inter alia, USA MCO’s
Net contributions
“Net contributions represent contributions for which the medical scheme is at risk,
and are calculated as gross contributions less savings contributions, during the
accounting period.” (SAICA, 2003, p.54)
Outstanding claims
Outstanding claims consist of claims that have been:
Incurred but not reported (IBNR);
Reported but not yet settled or approved for payment;
Reported and administratively finalised but which may be reopened. (ASSA,
2002).
Private Health Insurance Administration Council
The regulator of Australian private health insurers
Probability of ruin
The probability of insolvency
Registered medical scheme
Any medical scheme that is or will be in full compliance with the Medical Schemes
Act of 1998, and is registered with the Council for Medical Schemes (Dreyer, 2001).
The Registrar
The Registrar of medical schemes, appointed under section 18 of the Medical
Schemes Act of 1998
Reinsurance
A contractual arrangement under which some of the risk of the medical scheme is
transferred to a reinsurer in return for some consideration (ASSA, 2002)
Risk
Risk is the possibility of adverse deviations in results.
Risk-Based Capital
Risk-based capital is the minimum amount of capital a medical scheme must hold to
ensure that the danger of insolvency is acceptably low. It is an amount of capital that
enables an entity to survive certain adverse fluctuations in results.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page ix
Risk charge
The amount of risk-based capital required by a risk element or collection of risk
elements.
Risk element
Distinct, quantifiable elements that differ in their level of risk are known as different
risk elements (Butsic, 1994). For example, bonds, equities and property are three
different risk elements.
Risk factor (also RBC factor)
The risk factor for a certain risk element is the ratio of its risk charge to the value of
that risk element. They are related to risk charges and the value of a risk element by
the following equation:
Risk charge = Value of Risk element Risk factor.
Technical insolvency (also insolvency or ruin)
Technical insolvency occurs when a scheme’s liabilities exceed its assets.
Abbreviations
ASC
ASO
ASSA
HBFCAR
HBFSR
IBNR
MCO
NAIC
PHIAC
RBC
RBCAC
RBCBC
SAICA
SEU
CARE
Administrative services contract
Administrative services only
Actuarial Society of South Africa
Health benefits fund capital adequacy requirement
Health benefits fund solvency requirement
Incurred But Not Received
Managed Care Organisation
National Association of Insurance Commissioners
Private Health Insurance Administration Council
Risk-Based Capital
Risk-Based Capital After Covariance
Risk-Based Capital Before Covariance
South African Institute of Chartered Accountants
Single Equivalent Unit
Effect of RBC Formulae on Medical Scheme Solvency
Page x
1. Introduction
1.1 Background to Research Project
A medical scheme is solvent if its assets exceed its liabilities. For the purpose of
regulation, a more stringent definition of solvency is used. This is meant to expose
schemes that might become insolvent or experience financial distress in the future so
that the regulator may take appropriate corrective action. In SA, for a scheme to be
solvent under the regulator’s definition of solvency, it must hold accumulated funds in
excess of 25% of gross contributions.
In a study of solvency requirements for medical schemes, Cooper (2001) points out a
number of problems with this regulatory solvency measure. For instance, it ignores
the transfer of risk through managed care contracts and reinsurance agreements. It
also ignores scheme size and variability in claims experience. In short, it makes no
allowance for the differing risk profiles of medical schemes. Cooper concluded that
the current solvency approach is inappropriate. He recommended the adoption of a
risk-based approach, which would consider the specific risks faced by each scheme.
He also recommended that the solvency definition allow for the transfer of risk.
1.2 Statement of Research Project
In light of Cooper’s recommendations, this project will examine two foreign riskbased capital systems and attempt to establish the effect a risk-based capital system
would have on South African medical scheme solvency.
1.3 Objectives of Research Project
The objectives of this project are to:
1. Explain and compare the RBC systems of Australian Health Insurers and USA
Managed Care Organisations.
2. Use 2000 statutory returns data to establish the effect a RBC system would
have on South African medical scheme solvency.
1.4 Sources of Information
Legislative and regulatory documents provided the basic detail of the Australian and
USA RBC systems, while journal articles on risk-based capital systems proved useful
in understanding the formulae and RBC in general.
Email was used to contact foreign RBC experts who were extremely helpful in
explaining certain parts of the formulae and providing reference papers.
The Registrar’s 2000 statutory returns provided the data to estimate the effect a RBC
system would have on South African medical scheme solvency.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 1
1.5 Scope and Limitations of Project
This report explains the Australian and USA RBC formulae and establishes the effect
those RBC systems would have on South African medical scheme solvency if
implemented without adaptation. It does not aim to develop a RBC system for South
African medical schemes or to adapt the foreign systems for use in the South African
medical scheme industry.
The project was limited in places by data availability and international differences.
Some of the data required by the Australian and USA RBC formulae was not
available from the Registrar’s 2000 returns, which meant that assumptions and
approximations were necessary. Furthermore, of the 146 schemes that were registered
in 2000, only 144 submitted their 2000 returns.
In addition, the report only considers the effect a RBC system would have on
Registered scheme solvency. It ignores Bargaining Council scheme solvency.
1.6 Plan of Development
The report begins with an introduction to risk-based capital in general. It then looks at
two foreign risk-based capital systems in detail. Chapter 3 gives an account of the
USA RBC formula for Managed Care Organisations, while Chapter 4 explains the
Australian solvency and capital adequacy standards for private health insurers. In
Chapter 5, data from the 2000 statutory returns is used to estimate the impact of RBC
on South African medical scheme solvency. This is achieved by calculating the USA
and Australian RBC requirements for South African medical schemes. Chapter 6 then
compares the Australian and USA systems. Finally, conclusions are reached and
recommendations are made for further research.
1.7 Acknowledgements
The author wishes to thank his supervisor, Professor McLeod of the University of
Cape Town, for her expertise, enthusiasm and supervision of this project.
Thanks must also go to:
Alan Ford of the American Academy of Actuaries;
David Watson of the Health Practice Committee of the Institute of Actuaries of
Australia;
Paul Groenewegen and Gayle Ginnane of the Australian Private Health Insurance
Administration Council;
Maggie Grobler of the Council for Medical Schemes; and
Mahesh Cooper
for their selfless assistance and valuable insights.
The author is also grateful to Yura Kaliazin for his comments on an earlier version of
this report.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 2
2. Risk-Based Capital
The aim of this chapter is to introduce the idea of risk-based capital. This will set the
scene for the next two chapters where two foreign RBC systems are discussed.
2.1 Introduction to Risk-Based Capital
Capital provides a cushion that allows a medical scheme to remain solvent through
certain adverse fluctuations in results. The more capital a scheme holds, the less likely
it is to go insolvent. The following diagram takes this relationship one step further by
introducing risk.
Capital
Risk
Probability of
ruin
Source: Van Den Heever (1998)
Figure 2.1: The relationship between capital, risk and probability of ruin
A medical scheme’s probability of ruin (or probability of insolvency) depends on the
risks that it faces as well as the amount of capital it holds. Two schemes facing the
same risks but holding different quantities of capital will have different ruin
probabilities. By changing the amount of risk and/or capital held, schemes can
influence their probability of ruin, making this a three-way relationship.
Under a risk-based capital (RBC) system, the relationship is simpler. The regulator
would choose the maximum probability of ruin and then, by examining a scheme’s
risk profile, determine the minimum amount of capital required by that scheme to
achieve that probability of ruin. The figure below shows the relationship from the
regulator’s point of view.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 3
Minimum
Capital
Requirement
Probability of
ruin
Risk
Figure 2.2: The relationship between risk, capital and probability of ruin from the regulator’s
point of view
Risk-based capital is the minimum amount of capital a medical scheme must hold to
ensure that the probability of ruin is acceptably low. This minimum amount of
capital is determined by the risks affecting the medical scheme.
Under a risk-based capital system, medical schemes would be required to hold capital
in excess of some minimum capital requirement (the RBC requirement) determined
by the regulator. If a scheme’s capital fell below the required level, it would be
subject to regulatory action of some kind.
2.2 Medical Scheme Risk
If each medical scheme were required to hold a minimum amount of capital
determined by its risk profile, it would be natural to ask: “what risks should be taken
into account when setting these minimum capital requirements?” This section looks at
the various risks affecting medical schemes and will provide a point of reference for
the risks considered by the foreign RBC formulae in the coming chapters. Hooker
(1996), Cooper (2001) and the Council For Medical Schemes (2003) provided
valuable input to this section.
The main risks affecting medical schemes are:
Uncertainty in claims costs; and
Asset risk.
Uncertainty in claims costs relates to the potential error in estimates of incurred
claims for business already written and the potential error in estimates of future claims
used to price new business. For instance, the outstanding claims liability on the
balance sheet may be understated because incurred claims have been underestimated.
Restating the liabilities will reduce the scheme’s capital and may result in insolvency.
Also, new business may be under-priced because actual claims turn out to be higher
than was expected when contributions were set. The resulting losses will reduce the
scheme’s capital and could, if severe enough, cause insolvency.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 4
Asset risk is another major risk for a medical scheme. The scheme assets are invested
in the financial markets, so their capital values and income returns (e.g. dividends) are
likely to fluctuate. A decline in capital value will reduce the equity on a scheme’s
balance sheet and may lead to insolvency. Also, if the income from the assets is lower
than expected, the scheme may have to sell other assets to meet claim payments. This
will also reduce the scheme’s equity and could potentially cause insolvency.
Poor liquidity of assets, caused by poor asset structure, may render the scheme unable
to pay claims as they arise. Asset risk is intensified by excessive concentration of
assets in particular asset classes or with particular issuers.
Apart from the main risks already mentioned, medical schemes face many other risks,
including:
The risk of catastrophic losses;
Expense risk;
Managed care risk;
Reinsurance risk;
Credit risk;
Management risk; and
Growth risk.
The first two risks are self-explanatory. Managed care risk is the risk that a Managed
Care Organisation (MCO) defaults on its obligations to the scheme. This could
happen if the scheme paid capitations to an MCO which went insolvent before
providing the agreed care to the scheme members.
Reinsurance risk relates to the possibility that the reinsurer will not pay future
reinsurance claims in full. It includes the risk that the reinsurer may not pay those
claims currently outstanding in full. Credit risk is similar and refers to the risk of other
creditors defaulting on their obligations to the scheme.
Management risk relates to the possibility that a scheme’s management is incompetent
to run the scheme effectively. Areas that could be mismanaged include claims
processing, investment, benefit design and financial reporting.
Growth risk is present when a scheme grows quicker than its resources. In the UK
general insurance context, Hooker (1996) highlights inadequate infrastructure and
expertise as possible consequences of rapid growth into a new geographical area.
2.3 Calculation of RBC Requirements
Once the regulator has identified the risks affecting a particular scheme, that
information can be used to calculate its RBC requirement. The next two chapters will
describe exactly how this is done in the United States and Australia.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 5
At a theoretical level, there are three possible approaches:
The probability of ruin approach (used by the USA RBC system);
The expected policyholder deficit approach; and
The approach whereby schemes are required to hold capital to meet certain
circumstances (used by the Australian RBC system).
Appendix B1 gives an example of how the first two methods work. Section 2.1
introduced the idea of RBC using the probability of ruin approach for ease of
explanation.
2.4 Desirable Features of a RBC System
Hooker (1996) and Cummins et al (1992) suggest that a RBC system should be:
An incentive for weak companies to hold more capital and/or reduce risks without
distorting the behaviour of financially sound schemes;
Comprehensive;
Based on a solid theoretical foundation;
Free of unnecessary complexity;
Robust; and
Unlikely to cause adverse behavioural changes such as manipulation of financial
results.
They also acknowledge that some of these qualities are conflicting. The coming
paragraphs will expand on these points.
The main aim of a risk-based capital system is to give financially weak schemes an
incentive to reduce the danger of insolvency. It should encourage those schemes for
which market incentives are insufficient, to reduce risk and/or hold more capital.
More often than not this will cause the schemes to increase contribution rates.
To avoid distorting the behaviour of financially sound insurers, the level of the RBC
requirement must be set carefully. A high requirement will reduce insolvencies, but
distort the behaviour of financially sound insurers and cause large increases in
contribution rates. If the requirement is set too low, it will have no impact on
insolvencies.
The formula should be “comprehensive” or complete in that it includes as many
different risks as possible. It should allow for the various steps schemes can take to
mitigate risks, such as reinsurance arrangements and managed care arrangements.
Likewise, the formula should recognise how schemes can exacerbate these risks, such
as excessive concentration of assets in a certain asset class or with a certain issuer.
Examples of solid theoretical foundations are the probability of ruin approach and the
newer expected policyholder deficit approach. These approaches were both mentioned
in the previous section.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 6
Any RBC formula should be free from complexity that only marginally increases the
accuracy of the formula. This will make the formula easier to explain, understand and
use. Cummins et al (1993) point out that the more complex the formula, the more
difficult it will be for schemes to determine the effect of their actions on their required
capital. A complex formula could also lead to unintended side effects when the
formula is put into practice, since it is harder to predict the effect of a complicated
formula than the effect of a simple formula. Practically speaking, the benefits and
costs of additional data reporting under a complex system need to be evaluated.
The formula should also be “robust” in the sense that a minor change in a firm’s risk
profile should cause no more than a minor change to that firm’s RBC requirement.
Robustness helps ensure that the RBC system does not cause undesirable changes to
scheme behaviour by creating incentives to manipulate financial results. Furthermore,
the RBC requirement should not cause schemes to take unnecessary additional risks.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 7
3. The USA RBC system for Managed Care
Organisations
This chapter explains the USA RBC system for Managed Care Organisations
(MCO’s).
3.1 Introduction to the USA RBC System
The USA RBC system calculates the amount of capital an MCO needs to ensure its
probability of ruin is sufficiently low. This capital will enable the MCO to withstand
certain adverse fluctuations in results. Although quite detailed, the formula is
conceptually simple. The following example (ASSA, n.d.) will give an initial feel.
Suppose an MCO invests all its assets in bonds and that the current value of this
investment is $100 million. Next, assume that there is a 5% probability that the value
of this investment will be less than $75 million in one year’s time and that the MCO
has liabilities of $75 million. This implies that the MCO must hold at least $25
million in capital to have a 95% probability of remaining solvent over the coming
year (assuming asset risk is the only risk faced by the scheme). If capital requirements
are based on a 5% probability of ruin, the MCO will have a $25 million RBC
requirement.
In this example, a risk factor of 0.25 (i.e. 25/100) would be appropriate for bonds. In
other words, the risk charge for bonds equals 0.25 multiplied by the value of the
MCO’s bond portfolio.
The USA RBC formula uses this risk factor approach to specifying the various risk
charges. Most risk charges in the USA formula are of the form:
Risk charge = Value of Risk element Risk factor.
Risk elements are items that differ in their riskiness. In the above example, bonds are
the risk element. Common stock, preferred stock and equities are other risk elements
that would each require a different factor, the riskier the risk element, the larger the
risk factor. Appendix B2 explains how these factors would be estimated in practice.
The formula is divided into five sections, each one corresponding to a different risk.
This structure is illustrated below.
RBC requirement
Asset risk
H0: Asset risk - affiliates
Liability risk
H1: Asset risk - other
H2: Underwriting risk
Other risks
H3: Credit risk
H4: Business risk
Source: NAIC (2001)
Figure 3.1: Structure of USA RBC formula
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 8
Each section contains the various risk elements relating to that risk. These risk
elements require different risk factors to determine their risk charges.
The total risk charges for each section of the formula are combined to give the riskbased capital after covariance (RBCAC) for an MCO. If an MCO’s total equity
exceeds its RBCAC, the MCO is not subject to any regulatory action. However, if an
MCO’s equity falls below one of four thresholds, the organisation will be subject to
regulatory action. These different thresholds and their corresponding regulatory
actions are shown in the table below. Authorised Control Level (ACL) is defined as
50% of an organisation’s RBCAC.
Table 3.1: RBC thresholds and their corresponding regulatory actions
RBC level
Company Action Level
(CAL=200% ACL)
Regulatory action
The company must notify the insurance commissioner of the corrective
actions it plans to take to increase capital.
Regulatory Action Level
(RAL=150% ACL)
The company must submit or resubmit a corrective plan of action to remedy
the situation. After examining the company, the insurance commissioner will
issue an order specifying the corrective actions to be taken.
The insurance commissioner is authorised to take whatever regulatory action
Authorised Control Level
is necessary to protect the interests of the policyholders, including taking
(ACL)
control of the company.
Mandatory Control Level The insurance commissioner is required to place the company under
regulatory control.
(MCL=70% ACL)
Source: Milliman (1998, p.2)
The following sections will explain each of the five sections of the USA formula; the
calculation of risk-based capital after covariance; and the transitional arrangements
used to phase in this RBC requirement. Data from South African medical schemes’
2000 statutory returns are used throughout these sections to give a feel for how much
RBC the formula would have required registered South African medical schemes to
hold at 31 December 2000. This will also demonstrate the relative importance of the
different sections.
3.2 Asset Risk – Affiliates
This section of the RBC formula allows for the risk that the value of investments in
affiliates will decrease. Therefore, this section only affects MCO’s that have
ownership in affiliates. South African medical schemes are essentially mutual
organisations, so they cannot have a parent. They could however have a subsidiary,
but this is rare.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 9
The risk charge for ownership in affiliated entities depends on whether those entities
are themselves subject to a RBC requirement. For affiliates that are not subject to
RBC, holdings in non-USA insurance subsidiaries receive a risk factor of 1.0, while
other affiliates have a risk factor of 0.3. For affiliates that are subject to RBC, the risk
charge is more complicated. Since it has little relevance to the South African
environment, its full detail will not be set out here and the reader is referred to NAIC
(2001, pp.1-6). Suffice it to say, the aim of the risk charge for investment in affiliated
entities is to ensure that the assets held in respect of the affiliate’s capital requirements
are not counted in meeting the capital requirements of its owner.
The asset risk – affiliates section also makes allowance for off balance sheet risk such
as contingent liabilities that are disclosed in the notes to the financial statements. It
calculates the risk charge by applying a 0.01 factor to the value of the contingent
liability. By holding extra capital in respect of these contingent liabilities it reduces
the risk of the MCO going insolvent, were it required to make any payments in terms
of these contingent liabilities.
The estimated value of the asset risk – affiliates charge for registered South African
medical schemes is shown below.
Table 3.2: Estimate of asset risk – affiliates RBC
Rands
Off-balance sheet items
189,718
H0: Asset risk - affiliates RBC
189,718
Gross contributions
29,884,077,939
% of gross contributions
0.001%
Clearly, the asset risk – affiliates charge would not impose a significant capital
requirement on South African medical schemes.
3.3 Asset Risk – Other
Figure 3.2 shows the structure of the Asset risk – other section.
Asset risk - other
Fixed income assets
Replication transactions
Equity
Property and equipment
Asset concentration
Source: NAIC (2001)
Figure 3.2: Structure of asset risk – other charge
This section reserves against reductions in the market value of assets as well as the
possibility of default of principal or interest. It only deals with unaffiliated
investments. This part of the formula is very detailed because it differentiates between
many different types of assets. For instance, it recognises seven different bond classes,
and assigns each one a different risk factor.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 10
This can make the formula appear more complex than it actually is. It also makes
estimation of these risk factors (i.e. calibrating the formula) time consuming and
expensive.
Despite the level of detail in this section, all the risk charges are of the form:
Risk charge = Value of Risk element Risk factor.
The total risk charge for the asset risk – other section of the RBC formula is found by
summing the risk charges for each of its five subsections.
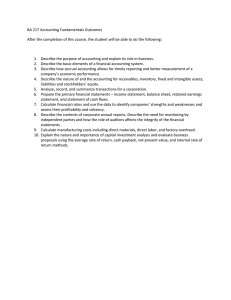
3.3.1 Fixed income assets
The NAIC Security Valuations Office (SVO) classifies bonds into six different classes
based on their risk of default of principal and interest. These bond ratings are used in
the formula. The riskier bonds are allocated to the higher classes, so the higher the
bond class, the higher the risk factor for that bond. The figure below shows the risk
factors used for fixed income assets.
0.35
0.300
0.3
0.25
Risk factor
0.200
0.2
0.15
0.100
0.1
0.045
0.05
0.020
0.000
0.003
0.010
0.003
0.003
Cash
Other short
term
investments
0
Government Class 1 bonds Class 2 bonds Class 3 bonds Class 4 bonds Class 5 bonds Class 6 bonds
bonds
Other long
term
investments
Risk element
Source: NAIC (2001)
Figure 3.3: Fixed income asset risk factors
3.3.2 Replication transactions
The formula recognises that some assets are held for the purposes of replicating the
payoffs from derivatives. It handles these assets differently from normal holdings. The
reader is referred to NAIC (2001, p.9) for the detail of this part of the formula.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 11
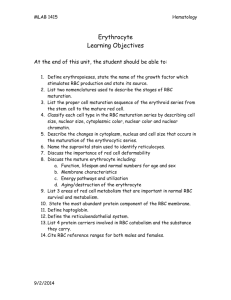
3.3.3 Equity
The formula distinguishes between common stock and preferred stock. As for bonds,
preferred stock is divided into six categories. Because there was no experience data
available to determine the preferred stock factors, they were set at the bond factor
level plus 2%, subject to a maximum of 30%. This was based on the assumption that
preferred stocks are more likely to default than bonds and that the losses on preferred
stock default would be higher than that on bonds (NAIC, 2001). Problems such as
lack of data to estimate factors are made more likely by the level of detail in the
formula. The resulting preferred stock and common stock factors are shown in the
figure below.
0.35
0.300
0.3
Risk factor
0.25
0.2
0.150
0.15
0.120
0.1
0.065
0.05
0.040
0.023
0.030
0
Class 1 preferred
stock
Class 2 preferred
stock
Class 3 preferred
stock
Class 4 preferred
stock
Class 5 preferred
stock
Class 6 preferred
stock
Common stock
Risk element
Source: NAIC (2001)
Figure 3.4: Equity risk factors
The factor for common stock lies between the factors for class five and six preferred
stock. On the whole, the formula recognises that common stock is more risky than
preferred stock, as one would expect
3.3.4 Property and equipment assets
Milliman (1998) state that one of the unique characteristics of MCO’s is investment in
property, such as hospitals, that are used for the provision of care and may give the
MCO greater control over healthcare costs. The formula appears to take this into
account by dividing properties into:
“Properties occupied by the company;
Properties held for the production of income; and
Properties held for sale.” (NAIC, 2001, p.12)
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 12
However, each category has a risk factor of 0.1, so for asset risk RBC purposes, it
doesn’t matter which category the MCO’s property falls into. Furthermore, the
underwriting risk section of the formula (see section 3.4) is unaffected by these
property categories. This implies that the formula ignores any increased control over
healthcare costs that an MCO enjoys from owning property.
Furniture and equipment are divided into:
Heath care delivery assets and
Other furniture and equipment.
Vehicles would be included in the second category (A. Ford, personal
communication, May 2, 2003).
As for property, both categories have a risk factor of 0.1. It is surprising that this risk
factor is lower than the common stock factor (0.150). This seems to suggest that
investment in furniture and equipment is less risky than investment in common stock.
At first glance it may seem pointless to distinguish between different types of assets
and then treat them in the same way. It is the author’s opinion that the NAIC plan to
assign different risk factors to the various equipment and property types in the future,
but have not yet decided what these factors should be (perhaps due to lack of data).
3.3.5 Asset concentration
The asset concentration section of the formula imposes an additional charge for high
concentrations of certain types of assets with single issuers. This is because there is
increased risk of insolvency if one of these issuers should default. An issuer is “a
single entity, such as IBM or Ford Motor Company” (NAIC, 2001, p.13).
Concentrated investments in certain types of assets are not expected to increase the
risk of insolvency significantly. Such assets are exempt from the asset concentration
charge. Assets subject to the concentration charge include:
Bonds (class 2-5);
Preferred stock (class 1-5);
Other long-term invested assets; and
Common stock.
The asset concentration charge effectively doubles the risk factor (up to a maximum
of 0.3) for assets held with the ten largest issuers. The ten largest issuers are
determined based on the total value of the assets that are subject to the concentration
charge invested with each issuer. By doubling the risk charge for these issuers, we
decrease the probability that reductions in the value of these assets will cause
insolvency.
Estimated values of the different components of the asset risk – other charge for
registered South African medical schemes are shown below.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 13
Table 3.3: Estimate of asset risk – other RBC
Fixed income assets
Equity
Property and equipment
Asset concentration
H1: Asset risk - other RBC
Gross contributions
% of gross contributions
Rands
465,973,565
350,013,388
26,262,894
512,443,800
1,354,693,647
29,884,077,939
4.5%
The contributions of the different subsections of the asset risk – other charge are
shown in Figure 3.5.
1.9%
25.8%
37.8%
Asset concentration
Fixed income assets
Equity
Property and equipment
34.4%
Figure 3.5: Components of asset risk – other charge
The asset concentration charge is the largest contributor to asset risk – other. This is
because many schemes were not invested across more than ten issuers, so the asset
concentration charge made up almost half of their asset – risk other charges. Fixed
income assets and equity assets are the other main contributors. Schemes hold very
little property and equipment, so these components were not significant.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 14
3.4 Underwriting Risk
The underwriting risk charge is usually the largest single component of the RBC
requirement and it is based on the risk that incurred claims may be higher than
expected. The underwriting risk charge is the maximum of the underwriting risk RBC
after managed care discount and the alternative risk charge.
3.4.1 Base Underwriting risk RBC
Base underwriting risk RBC is calculated separately for each line of business. It is
determined by the following equation:
Underwriting risk revenue Claims ratio Risk factor.
Underwriting risk revenue is essentially contributions net of reinsurance premiums, so
the formula allows for the transfer of risk through reinsurance. The credit risk (H3)
section of the formula allows for the possibility that the reinsurer may default on its
obligations to the MCO.
The claims ratio has the effect of reducing the underwriting risk charge for schemes
with better claims experience than others. Furthermore, it separates out the part of
premiums that are meant to cover claims from the part meant to pay expenses (ASSA,
n.d.). Expenses are dealt with separately in the business risk (H4) section of the
formula.
The risk factor is a premium weighted average of 0.15 and 0.09. The first $25 million
of premiums are used to weight the 0.15 factor while the rest apply to the 0.09 factor.
Other things equal, the risk factor and consequently the risk charge is lower for
schemes with larger total premiums. Barth (1999) suggested this tiered approach in
his article “Applying the Law of Large Numbers to P&C Risk-Based Capital”. He
argued that the variability of a loss ratio is lower for insurers with larger risk pools.
He quantified this relationship by regressing loss ratio standard deviation on earned
premium. The tiered factors were then chosen based on this relationship.
3.4.2 Underwriting risk RBC after managed care discount
This section of the formula adjusts the base underwriting risk RBC for the transfer of
risk from the MCO to the healthcare provider through managed care contracts.
Underwriting risk RBC after managed care discount is:
Base Underwriting Risk RBC Managed care discount factor.
The following table shows the different managed care categories and discount factors.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 15
Table 3.4: Managed care credit categories
Category
Description
Fee-for-service, discounted fee-for-service and other non-managed care
0
arrangements.
Factor
0.00
1
Payments made under contractual arrangements such as hospital per diems,
physician fee schedules, DRG-based payments, case rates, and other
contractual arrangements that would not apply to category 0.
0.15
2
Payments made subject to withholds and bonuses. The managed care credit
factor is presented as a range based on the proportion of withholds and bonuses
paid. The minimum factor is the managed care credit factor for category 0 or 1,
depending on the reimbursement method to which the withholds pertain. The
maximum managed care credit factor is 0.25.
0.00-0.25
3
Capitation payments made directly to providers of medical care and capitations
paid to intermediaries, such as an IPA, who, in turn, make payments to
providers who contract independently with the intermediary (not including
employment contracts). This includes payments to physicians and nurses for
utilisation review.
0.60
4
Owned facility expenses and salaries paid directly to medical care providers and
noncontingent salaries or aggregate cost payments to licensed providers.
0.75
Source: Milliman (1998, p.6)
The total paid claims in each category are used as weights to determine the weighted
average of the discount factors in the third column. Paid claims are used instead of
incurred claims because of the variability in estimates of outstanding claims included
in incurred claims as well as the difficulty in allocating estimated outstanding claims
to the different managed care categories. The managed care discount factor is then
defined as one minus this weighted average. It lies between zero and one.
It is important to realise that this reduction in the risk charge is based on a reduction in
the variability of claim payments caused by risk sharing agreements. It is not due to
any reduction in the size of claims. Notice how the managed care arrangements that
pass on more risk to the providers are assigned higher factors, which imply a smaller
underwriting risk charge. As with reinsurance, the credit risk section allows for the
possibility that the counter-parties to these contracts default on their obligations to the
MCO.
The figure below shows the breakdown of registered South African medical schemes’
paid claims between managed care and non-managed care arrangements.
The 99% of paid claims that were paid under non-managed care arrangements would
be grouped into category zero. Most of the 1% of paid claims made under managed
care arrangements would probably be grouped into categories zero or one.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 16
1.0%
Non-managed care claims
Managed care claims
99.0%
Figure 3.6: Managed care claims as a percentage of paid claims
Many of the managed care initiatives used by South African schemes have been found
not to transfer any risk at all. Doherty and McLeod (2002) found that in 2001, only
13% of medical schemes used risk-sharing managed care arrangements. All this
suggests that the managed care discount would currently have very little effect on
South African medical schemes at present.
[Editor’s Note: the use of risk-sharing arrangements is changing rapidly and the
conclusion above is made too lightly. An allowance for managed care risk transfer
makes sense IF managed care organisations in South Africa become regulated for
solvency. They could be required to hold reserves using a similar RBC approach.]
3.4.3 Alternative risk charge
The other component of the underwriting risk section of the formula is the alternative
risk charge. This reduces the probability that an MCO will be ruined by large
individual claims. The alternative risk charge is twice the maximum after reinsurance
payout on any individual claim.
The underwriting risk section of the formula also makes allowance for many different
types of business that USA MCO’s write that fall under the umbrella of medical
insurance and are not the business of a medical scheme.
An estimate of the underwriting risk charge for registered South African medical
schemes is shown below.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 17
Table 3.5: Estimate of underwriting risk RBC
Base underwriting risk RBC
Base underwriting risk RBC after
managed care discount
Alternate risk charge
H2: Underwriting risk RBC
Gross contributions
% of gross contributions
Rands
2,700,546,872
2,695,639,592
247,160,000
2,713,030,121
29,884,077,939
9.1%
Notice how small the effect of the managed care discount is. The underwriting risk
charge would impose a capital requirement of 9.1% of gross contributions on medical
schemes.
One of the author’s initial, but incorrect, criticisms of the USA RBC formula was that
it did not allow for the risk of misestimating outstanding claims. Mr. Alan Ford, one
of the creators of the formula, explained via email that the underwriting risk charge
implicitly includes a reserve against misestimating outstanding claims. An extract
from that email is included below.
“The answer to your question is that the H2 Factor includes
provision for the misestimating of outstanding claims.
RBC represents a level of capital that indicates a MCO's ability to
withstand adverse fluctuation in results. For MCO's the H2 risk is
primarily for the adverse deviation of incurred claims, which
includes the change in estimates for outstanding claims over the
valuation period as well as paid claims. Generally, outstanding
claims are estimated as a function of the paid claims over the
valuation period, adjusted for changes in claim backlog and other
known factors. The estimates of outstanding claims and the paid
claims are intimately related, so providing separate risk factors for
the components would introduce unnecessary complexity into the
determination of RBC.”
Alan Ford, personal communication, 27 February, 2003
3.5 Credit Risk
The credit risk section of the formula is divided into three subsections as shown in
Figure 3.7.
Credit risk
Reinsurance
Capitations
Other receivables
Source: NAIC (2001)
Figure 3.7: Structure of credit risk charge
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 18
Reinsurance risk is the possibility that the reinsurer will not pay the amounts it
currently owes the MCO, as well as the possibility that it will not provide the future
cover already paid for by the portion of the reinsurance premium that is currently
unearned. The reinsurance risk factor is 0.005, which is applied to amounts due from
reinsurers and premiums paid in advance to reinsurers. This risk factor is only
marginally higher than the cash factor of 0.003, suggesting that banks and reinsurers
have similar security. As for property, the reinsurance section divides reinsurance
receivables into various categories, but then assigns them all the same 0.005 factor.
Presumably, the NAIC intends to assign different factors to these different receivables
in future.
Capitation risk is present when an MCO pays capitations to providers or
intermediaries. It is possible that the provider or intermediary will not provide the
agreed upon services and the MCO will be forced to pay other providers to provide
these services. Withholds and letters of credit from providers can mitigate this risk.
The formula takes this into account by making some capitations exempt from the risk
charge when these measures are in place. The example in the table below shows how
the risk charge is calculated for capitations paid directly to providers. The risk charge
for capitations paid to intermediaries is calculated similarly.
Table 3.6: Example of calculation of capitation credit risk charge
Name of provider
Dr. A
Dr. B
Dr. C
Dr. D
Total risk charge
A
B
C
D=(B+C)/A E=A*Min(1,D/8%)
F=A-E
G=F*0.02
Paid
Capitation to
capitations Letter of
providers
during the
credit
Funds Protection
Exempt
subject to risk
Risk
year
amount witheld percentage
capitations
charge
charge
125,000
5,000
0
4%
62,500
62,500
1,250
50,000
5,000
0
10%
50,000
0
0
750,000
5,000
50,000
7%
687,500
62,500
1,250
25,000
0
0
0%
0
25,000
500
3,000
Source: NAIC (2001, p.26)
If the capitations are secured by letters of credit and withholds equal to 8% of paid
capitations, the entire capitation is exempt. Where less protection is provided, the
exempt capitation is prorated. A risk factor of 0.02, which is equivalent to one week’s
paid capitations, is applied to the remaining capitations. This seems to imply that
some mixture of withholds and letters of credit equal to 8% of the paid capitation
provides similar security to capital equal to 2% of the paid capitation. It is the author’s
opinion that this risk charge and its concessions are based more on experience and
judgement than statistics and data analysis.
The other receivables risk charge reserves against the risk that certain receivables will
be irrecoverable. It applies a 0.01 factor to investment income receivable and a 0.05
factor to health care receivables and amounts due from affiliates. A notable omission
from this section is any allowance for arrear contributions. When questioned on this,
Mr. Ford gave the following response.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 19
“Due and unpaid (arrear) premiums are not included in the RBC
calculation. Generally speaking, (in my opinion) this is not a large
risk. The aging of this receivable item is included in a separate
exhibit on the blank, so the regulator can readily discern where
assets are ‘optimistic’ with respect to the aging. Also, this
receivable is only admitted if it is under 90 days.”
Alan Ford, personal communication, 2 May, 2003
In the year 2000, some of the arrear contributions included in South African medical
schemes accounts receivable were more than 120 days in arrears. This suggests that
South African medical schemes are more exposed to this risk than are USA MCO’s.
Estimates of the different components of the credit risk charge for registered South
African medical schemes are shown in the table below.
Table 3.7: Estimate of credit risk RBC
Rands
Reinsurance RBC
1,774,818
Other receivables RBC
14,080,589
H3: Credit risk RBC
15,855,407
Gross contributions
29,884,077,939
% of gross contributions
0.1%
The credit risk charge is only 0.1% of gross contributions, so it would not impose a
significant capital requirement on medical schemes. The pie chart below shows the
relative importance of its two components.
11.2%
Other receivables RBC
Reinsurance RBC
88.8%
Figure 3.8: Components of credit risk charge
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 20
The other receivables charge, based mainly on co-payments due from members,
dominates the credit risk charge. Capitation risk is absent since this data was
unavailable. Since only 13% of medical schemes used risk sharing managed care
arrangements in 2001 (Doherty & McLeod, 2002) it is not expected to be significant.
3.6 Business Risk
The business risk section of the formula is divided into three subsections as illustrated
below.
Business risk
Administrative expense risk
Non-underwritten and limited risk
Excessive growth risk
Source: NAIC (2001)
Figure 3.9: Structure of business risk section
When premiums are set they include an assumption about the level of future
administrative (i.e. non-claims) expenses. These expenses are unknown at the time
premiums are set, so their variability leads to a risk charge.
The administrative expense charge is of the form:
Previous year’s administrative expenses Risk factor.
The risk factor is a tiered factor, similar to the underwriting risk factor. It is a
weighted average of 0.07 and 0.04, where the first $25 million of premiums is used to
weight the 0.07 factor while premiums in excess of $25 million weight the 0.04 factor.
The effect of this is to reduce the administrative expense risk charge for larger
schemes, which are expected to have less fluctuation in their administration expenses.
USA MCO’s can act as administrators for third parties, performing administrative
services such as claims processing. This type of business is known as “nonunderwritten and limited-risk business”. In this regard, the RBC formula differentiates
between administrative services only (ASO) and administrative services contracts
(ASC). Under an ASO contract, the MCO only pays claims once the third party has
paid the MCO enough money to fully cover the claims. Under an ASC contract, the
MCO would pay claims first and seek reimbursement from the third party afterwards.
Administrative expenses relating to ASC and ASO contracts are assigned a risk factor
of 0.02. This is lower than the factor for the MCO’s own administrative expenses.
This is probably because the MCO is only concerned with claims administration
under these contracts, allowing less scope for variability in expenses. Furthermore, a
0.01 factor is applied to total claims payments made under ASC contracts on behalf of
third parties. This risk charge stems from the risk that the counter party to the ASC
contract may be unable or unwilling to reimburse the MCO for claims payments made
under the contract.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 21
This risk charge has implications for South African medical scheme administrators. If
a RBC formula similar to the USA formula were introduced in South Africa, third
party administrators, as well as MCO’s and medical schemes, would be obliged to
hold minimum amounts of capital.
The final part of the business risk section is the excessive growth charge, which aims
to penalise uncontrolled growth. It does this by comparing the underwriting risk RBC
to a notional “safe level”. The formula sets the maximum safe level of underwriting
risk RBC by growing the previous year’s underwriting risk RBC for one year at the
one-year growth rate in premiums plus 10%. The excessive growth charge is then
defined as 50% of the difference between the current underwriting risk RBC and the
maximum safe level, subject to a minimum of zero.
Professor McLeod pointed out a problem with this method of reserving against
excessive growth (personal communication, April 3, 2003). If a scheme has a large
increase in membership shortly before the date on which the RBC requirement is
calculated, the extra premiums from these new members will not be fully visible at the
calculation date. Therefore, the underwriting risk RBC will not have increased
sufficiently to generate an excessive growth charge.
An estimate of the business risk charge for registered South African medical schemes
is shown in the table below.
Table 3.8: Estimate of business risk RBC
Administrative expense RBC
Excessive growth RBC
H4: Business risk RBC
Gross contributions
% of gross contributions
Rands
124,379,325
177,549,064
301,928,389
29,884,077,939
1.0%
The business risk charge would impose a capital requirement of roughly one percent
of gross contributions. The relative sizes of the different subsections of the business
risk charge are shown below.
The excessive growth charge and administrative expense charge both contribute
significantly to the business risk charge. The non-underwritten and limited risk
business charge was not applicable to South African medical schemes. Such risk
charges relate more to the business of scheme administrators than medical schemes.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 22
41.2%
Excessive growth RBC
Administrative expense RBC
58.8%
Figure 3.10: Components of business risk charge
3.7 Risk-Based Capital After Covariance
The risk-based capital after covariance (RBCAC) is a level of capital that allows the
MCO to withstand various adverse circumstances, as defined by the earlier five
sections of the formula. Since it is unlikely that these five circumstances coincide, the
RBCAC is less than the sum of these five sections.
RBCAC is determined by the following formula:
RBCAC H 0 H12 H 2 2 H 32 H 4 2 .
It assumes that the H1, H2, H3 and H4 risks are uncorrelated, while the H0 (affiliates)
risk is highly correlated with the other four risks. The following example (ASSA, n.d.)
will show how these assumptions are used.
Suppose an MCO has two risk elements, A and B, with risk charges of R3 million and
R4 million respectively. Assume that the risk charge for a given element is set so that
if the MCO faced only that risk and held exactly that amount of capital it would have
a 5% probability of ruin. Therefore, if an MCO had risk element A only and exactly
R3 million in capital, it would have a 5% probability of ruin.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 23
For a scheme with both risk elements, the capital requirement for a 5% probability of
ruin would be
3 2 4 2 2 Correlatio n( RiskA, RiskB ) 3 4 .
Case 1: If A and B are perfectly positively correlated, the capital requirement for a
5% probability of ruin is R7million (i.e. 3+4).
Case 2: If A and B are uncorrelated, the capital requirement is R5 million (i.e.
32 4 2 ).
The covariance adjustment is the cause of much debate. Van den Heever (1998) wrote
that there should be a covariance adjustment but that this square root rule is somewhat
arbitrary. On the other hand, Butsic (1994) has derived this square root rule exactly by
assuming that the values of the risk elements are normally distributed. In addition,
Hooker (1996) recommended that there should be no overall covariance adjustment,
but there should be an adjustment for covariance within the asset risk charge. Hooker
based this recommendation on his opinion that the absolute level of a RBC
requirement is a political decision based on what the market can handle.
The table below shows the total RBC after covariance and its components for
registered South African medical schemes.
Table 3.9: Analysis of estimated RBCAC
Risk category
Risk charge
H0: Asset risk - affiliates
H1: Asset risk - other
H2: Underwriting risk
H3: Credit risk
H4: Business risk
RBC before covariance
189,718
1,354,693,647
2,713,030,121
15,855,407
301,928,389
4,385,697,281
% of RBC before RBCAC' excluding
covariance
Hx as % of RBCAC'
0.0%
30.9%
61.9%
0.4%
6.9%
100.0%
RBC after covariance
Gross contributions
% of gross contributions
3,338,115,241
29,884,077,939
11.2%
RBC after covariance'
3,047,670,556
Source: Based on ASSA (n.d.)
100.0%
89.6%
45.5%
100.0%
99.5%
The total RBCAC for registered medical schemes was estimated at 11.2% of gross
contributions. To arrive at this figure, the covariance adjustment was applied
separately to each scheme, giving each individual scheme’s RBCAC, which were
summed to get the total RBCAC for registered schemes.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 24
The covariance adjustment increases the importance of larger risk charges and
decreases the importance of smaller sections (ASSA, n.d.). To illustrate this effect, the
RBC after covariance’ was calculated by applying the covariance adjustment to the
total H0-H4 components, as if the registered schemes were one big scheme. This is
merely for explanatory purposes and doesn’t represent any extension to the formula.
The total figures were used to avoid introducing a second set of numbers. The effect
of the covariance adjustment can be seen by comparing the sum of the different
sections of the formula i.e. risk-based capital before covariance to the RBCAC’.
It is clear that the RBCAC’ is less than the RBCBC. In addition, the risk categories
that form a large proportion of RBCBC have even greater influence on the RBCAC’.
The opposite is true of risk categories that form a small proportion of RBCBC.
Figure 3.11 shows the relative importance of the different risk charges.
0.4%
6.9%
0.0%
H2: Underwriting risk
H1: Asset risk - other
H4: Business risk
H3: Credit risk
H0: Asset risk - affiliates
30.9%
61.9%
Figure 3.11: Components of RBCBC
The underwriting risk charge is the largest risk charge, followed by the asset risk –
other charge. The business risk charge is the third largest charge while the other
charges are negligible.
3.8 Transitional Arrangements
The RBC requirement was phased in over the calendar years 1998, 1999 and 2000.
Figure 3.12 illustrates the transitional arrangements.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 25
55%
Full ACL
50%
50%
50%
Transitional ACL
50%
2000
2001
50%
45%
Percentage of RBCAC
45%
40%
40%
35%
30%
25%
20%
1998
1999
Calendar year
Source: NAIC (2001)
Figure 3.12: Transitional arrangements
When fully implemented, the ACL is set at 50% of RBCAC. During the phase-in
period, it is set lower than that. In 1998 the ACL was 40% of RBCAC, in 1999 it was
45% of RBCAC and from 2000 onwards, ACL is set at 50% of RBCAC. Since all the
other RBC thresholds are defined in terms of the ACL, this has the desired effect of
slowly raising the capital requirements to their full levels.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 26
4. The Australian RBC System for Private Health
Insurers
This chapter explains the Australian RBC system for Private Health Insurers.
4.1 Introduction to the Australian RBC System
The Australian RBC system for Private Health Insurers (“insurers”) requires insurers
to hold capital to meet certain circumstances. The solvency standard requires insurers
to hold an amount of capital (i.e. the solvency reserve) that will enable the fund to
meet its current obligations if the fund was closed to new business and run-off. The
capital adequacy standard requires the fund to hold sufficient capital (i.e. the capital
adequacy reserve) to continue to meet its obligations as a going concern. The capital
adequacy reserve is expected to exceed the solvency reserve.
PHIAC (2001) sets out the likely steps that the PHIAC would take in the event of a
breach of one of the standards. The RBC thresholds and regulatory responses in the
table below are based on Torrance (2001), who gives an interpretation of the PHIAC
paper.
Table 4.1: RBC thresholds and their corresponding regulatory actions
Capital level
Capital Adequacy Reserve
Solvency Reserve
Regulatory action
Increased PHIAC monitoring and potential direction to
the insurer to improve its position.
Direct PHIAC action to protect the insurer's obligations
to its policyholders.
Source: Torrance (2001)
An insurer with capital in excess of the capital adequacy requirement is likely to
suffer no intervention from the regulator.
Before looking at the detail of the solvency and capital adequacy formulae, it is
helpful to understand their logic. Figure 4.1 illustrates the method used to calculate
the solvency reserve; the capital adequacy reserve is calculated similarly.
The solvency reserve is not calculated directly; a figure called the solvency
requirement is calculated first. The difference between the solvency requirement and
the reported liabilities of the fund is the solvency reserve, which is the minimum
amount of capital an insurer is required to hold under the solvency standard.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 27
Solvency
Reserve
Solvency
Requirement
Reported
Liabilities
Total Assets
Capital and
Liabilities
Figure 4.1: Relationship between the solvency reserve and the solvency requirement
The structure of the solvency requirement is illustrated below.
Solvency requirement
Liability risk
Solvency
liability
Asset risk
Inadmissible
assets
reserve
Resilience
reserve
Additional obligations
Expense
reserve
Management
capital
amount
Source: PHIAC (2000a, p.6)
Figure 4.2: Structure of solvency requirement
The solvency requirement ensures that the insurer can meets its obligations in a runoff situation under a range of adverse circumstances affecting assets as well as
liabilities.
The solvency liability is the value of the insurer’s liabilities on a conservative basis
(this basis is specified in the standards). The inadmissible assets reserve; resilience
reserve; expense reserve and management capital amount can be thought of as risk
charges that require the insurer to hold extra capital on top of the solvency liability as
a buffer against adverse circumstances. The sum of these five components is called
the health benefits fund solvency requirement (HBFSR). The HBFSR less
subordinated debt is the solvency requirement. The logic behind this subordinated
debt allowance will be made clear in Section 4.10.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 28
The structure of the capital adequacy requirement is illustrated in Figure 4.3.
Capital adequacy requirement
Liability risk
Capital
adequacy
liability
Asset risk
Renewal
option
reserve
Inadmissible
assets
reserve
Ongoing fund
Resilience
reserve
Business
funding
reserve
Management
capital
amount
Source: PHIAC (2000b, p.6)
Figure 4.3: Structure of capital adequacy requirement
As with the solvency requirement, summing the six components at the bottom of the
diagram and making an adjustment for subordinated debt will generate the capital
adequacy requirement for a given scheme.
The rest of this chapter will describe the workings of each section of the solvency and
capital adequacy standards. At the time of writing, the standards were being changed.
The changes come into effect on 1 July 2003. Where relevant, the detail of these
changes will be included. Furthermore, data from South African medical schemes’
2000 statutory returns will be used throughout these sections to estimate how much
RBC the formula would have required registered South African medical schemes to
hold at 31 December 2000. This will also show the relative importance of the different
sections of the standards.
4.2 Solvency Liability
The solvency liability is equal to the reported liabilities of the insurer plus a loading
for those components of the insurer’s liabilities that are unknown and had to be
estimated. The structure of the solvency liability is illustrated below.
Solvency liability
Solvency net claims
liability
Solvency reinsurance
accrued liability
Solvency other
liabilities
Source: PHIAC (2000c, p.9)
Figure 4.4: Structure of solvency liability
The solvency net claims liability is the sum of two quantities:
1) 1.1 (Outstanding claims)
2) The maximum of
a) 1.1 (Contributions received in advance) (Loss ratio)
b) Contributions received in advance.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 29
The first quantity allows for the risk of underestimating outstanding claims. It adds a
ten percent margin in recognition of that risk, ensuring that in a run-off situation it is
likely that the insurer would be able to pay outstanding claims already incurred. The
basis for this 10% margin is outlined in Appendix B3.
The second quantity recognises that the insurer may be required to make claims (and
other) payments in excess of the contributions received in advance when providing
the cover paid for by those contributions. It requires the insurer to hold enough capital
to absorb such payments. The loss ratio is the ratio of expected claims and expenses to
contributions. Therefore, the product in line 2a is the value of the expected payments
relating to the contributions received in advance plus a ten percent loading for adverse
experience.
David Watson of the Australian Institute of Actuaries confirmed via email that any
reference to “reinsurance” in the Australian standards actually refers to their riskequalisation system. An extract from that email is given below.
“Reinsurance is a retrospective benefit equalisation arrangement,
administered by PHIAC. Its primary purpose is to support the
community rating system that is in place by virtue of the legislation
governing the operations of health insurers.”
David Watson, personal communication, 22 March, 2003
The parts of the solvency liability relating to these “reinsurance” arrangements will be
ignored in this report as they would involve a rather lengthy detour into the Australian
risk-equalisation system. The reader is referred to PHIAC (2000c, p.9 & pp.45-48) for
the details of this part of the calculation. However, with a South African risk
equalisation system currently being developed, it should be noted that such a system
would interact with a health RBC system.
Solvency Other Liabilities is the total balance sheet value of all other liabilities.
The solvency liability is the sum of the three components in Figure 4.4. It provides a
cushion of capital over and above the value of liabilities in recognition of the
possibility that liabilities are understated. This increases the likelihood that an insurer
can meet its obligations in a run-off situation.
The table below shows the solvency liability for registered South African medical
schemes.
The solvency liability turns out to be 5.4% larger than balance sheet total liabilities.
Therefore, the solvency liability alone generates a solvency reserve of 5.4% of
liabilities.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 30
Table 4.2: Estimate of solvency liability
Rands
Solvency net claims liability
Solvency other liabilities
Solvency liability
Less: Total liabilities
"Contribution" to solvency reserve
Gross contributions
As % of gross contributions
3,650,978,408
3,152,775,597
6,803,754,005
6,453,059,082
350,694,923
29,884,077,939
1.2%
As % of total
liabilities
105.4%
Contribution to the solvency reserve is the difference between the solvency liability
and total liabilities. It shows how much of the solvency reserve is generated by the
solvency liability section. The solvency liability generates a solvency reserve of 1.2%
of gross contributions.
4.3 Expense Reserve
In a run-off situation, contributions will cease, but the insurer will continue to incur
certain expenses. These expenses could erode the resources of the insurer, leaving it
unable to meet its obligations to policyholders and other creditors. The solvency
standard requires insurers to hold capital to meet these expenses and prevent such an
outcome.
The formula for this reserve is
Expense reserve 0.5 (Total expenses – Allowable deductions).
The reasoning behind it is quite straightforward. It starts off with the fund’s total nonclaims expenses for the year prior to the valuation date and subtracts those expenses
that the fund can immediately terminate (such as marketing and broker commissions)
without extra cost to the fund. Then, under the assumption that the leftover expenses
decrease to zero linearly over the course of one year, it multiplies the leftover
expenses by 0.5.
Regulation 6(1)(a) in terms of the Medical Schemes Act of 1998 holds that South
African medical schemes are not obligated to pay claims that are reported over four
months after the date on which the last medical service was rendered to the member or
dependant. This implies that a South African medical scheme, which is closed to new
business, will have few claims to process four to five months after its closure.
Therefore, a South African medical scheme’s expenses may decrease to zero in less
than one year, and a factor of less than 0.5 could be used in the South African
environment.
At the time of writing, the PHIAC were adjusting this part of the formula. From 1 July
2003, the expense reserve will be 40% of total non-claims expenses (with no
deductions) for the year prior to the valuation date (P. Groenewegen, personal
communication, May 2, 2003). This is equivalent to the old requirement with 20% of
non-claims expenses being deductible.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 31
Table 4.3 shows the expense reserve for registered South African medical schemes.
Table 4.3: Estimate of expense reserve
Total expenses
Total allowable deductions
Expense reserve
Gross contributions
As % of gross contributions
Rands
As % of total
expenses
3,705,122,360
1,209,641,858
1,247,740,251
29,884,077,939
4.2%
33.7%
The expense reserve equals 33.7% of total expenses and generates a solvency reserve
of 4.2% of gross contributions.
4.4 Inadmissible Assets Reserve
The inadmissible assets reserve has three components as illustrated below.
Inadmissible assets
reserve
Assets used in
conduct of business
Holdings in prudentially
regulated institutions
Asset concentration
reserve
Source: PHIAC (2000c)
Figure 4.5: Structure of inadmissible assets reserve
If the inadmissible assets reserve is being calculated as a component of the solvency
requirement, it equals the sum of all three components in Figure 4.5. However, for
inclusion in the capital adequacy requirement it should not include the reserve in
respect of assets used in the conduct of business.
If a fund closes to new business, it may need to sell some of its assets to fund its
expenses during the run-off period. For some assets, it will be difficult to recover their
full balance sheet value on sale. On a run-off basis, these assets are effectively worth
less than their normal balance sheet values. Therefore, the solvency standard requires
the insurer to hold reserves to the extent that these assets are over valued.
It defines the size of this reserve by specifying the value to be assigned to various
assets in a run-off situation. For instance, arrear contributions, computer software, and
prepaid expenses are all assigned zero values. So, the insurer must hold reserves equal
to these assets’ balance sheet values.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 32
If an insurer has holdings in an entity that is required to hold a minimum quantity of
capital (i.e. a prudentially regulated entity), that insurer will be required to hold a
reserve to the extent that the balance sheet value of that holding includes part of the
entity’s capital requirement. This ensures that the assets supporting the capital
requirement of the subsidiary entity are not used to meet the capital requirement of the
insurer that owns it. Similar allowances were made for affiliates subject to RBC in the
USA formula. In general, the assets supporting the capital requirements of one entity
cannot be used to meet the capital requirements of another entity at the same time.
The asset concentration reserve imposes a capital requirement based on the risk from
excess concentration of assets with one obligor. It does this by defining an acceptable
level of investment with each obligor and then imposing a capital requirement to the
extent that investment with each obligor exceeds the acceptable level. For most assets,
the maximum acceptable level of investment with a particular obligor is 10% of the
total assets of the insurer. An example of an exception to this rule is investment in
government bonds where the maximum acceptable investment is 100% of the
insurer’s total assets.
Although the 10% limit seemed rather harsh to the author, the Australian Government
Actuary has indicated that it may be too lenient and that a 5% limit may be more
appropriate (P. Groenewegen, personal communication, May 2, 2003). If this were
implemented, insurers would have to hold over 20 different assets to avoid an asset
concentration charge.
Table 4.4 shows the value of the inadmissible assets reserve for registered South
African medical schemes.
Table 4.4: Estimate of inadmissible assets reserves
Rands
As % of total
assets
Total assets
12,972,132,222
Assets used in conduct of business
Asset concentration risk
Inadmissible assets reserve (solvency)
Gross contributions
As % of gross contributions
1,523,412,290
2,579,028,277
4,102,440,567
29,884,077,939
13.7%
11.7%
19.9%
31.6%
Asset concentration risk
Inadmissible assets reserve (capital adequacy)
Gross contributions
As % of gross contributions
2,579,028,277
2,579,028,277
29,884,077,939
8.6%
19.9%
19.9%
For solvency purposes, 31.6% of total assets were inadmissible, while 19.9% of total
assets were inadmissible for capital adequacy purposes. This can be interpreted as
imposing a solvency reserve of 31.6% of assets and a capital adequacy reserve of
19.9% of assets. The inadmissible assets reserve generates a solvency reserve of
13.7% of gross contributions and a capital adequacy reserve of 8.6% of gross
contributions.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 33
4.5 Resilience Reserve
The resilience reserve establishes a reserve against adverse movements in asset values
relative to liability values. In other words, the resilience reserve is that quantity of
capital that ensures an insurer’s assets still exceed its liabilities after an economic
shock that decreases the value of the insurer’s assets relative to its liabilities.
The explanation of this reserve requires some notation, as used in PHIAC (2000c,
p.23). Let:
RR be the resilience reserve;
A and A’ be the value of the insurer’s assets before and after the shock;
L and L’ be the value of the insurer’s liabilities before and after the shock.
Assets that are worth one rand before the shock will be worth A’/A rand after the
shock.
The resilience reserve is defined so that assets worth RR+L before the shock are
worth L’ after the shock. In other words, the assets supporting liabilities and the
capital cushion provided by the resilience reserve before the shock, should be enough
to meet liabilities after the shock. Therefore the resilience reserve satisfies
RR L A' L' .
A
This implies that
RR L'
A
L.
A'
The prescribed economic changes that determine A’ are listed in Table 4.5.
Table 4.5: Economic shocks assumed in resilience reserve
Shock for
Shock for capital
solvency
adequacy
Fall in capital value Fall in capital value
of (25% times DF) of (35% times DF)
Asset class
Equities
Fall in capital value Fall in capital value
of (15% times DF) of (25% times DF)
Property
Interest bearing Rise in yield of
(1.5% times DF)
securities
Rise in yield of
(2.5% times DF)
Rise in yield of
Rise in yield of
(0.5% times DF)
(1.5% times DF)
Source: PHIAC (2000c, p. 23)
Indexed bonds
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 34
In the above table, DF is the diversification factor as defined in PHIAC (2000c, p.24).
It reduces the severity of the economic shocks (and hence the resilience reserve) for
insurers that spread their assets across the different asset classes. With effect from 1
July 2003, the fall in capital value of property for solvency purposes will be increased
to 25% times DF (P. Groenewegen, personal communication, May 2, 2003). This is
because of the difficulty in determining the value of properties in a wind-up situation.
Table 4.6 shows an estimate of the resilience reserve for registered South African
medical schemes.
Table 4.6: Estimate of resilience reserves
Rands
As % of total
assets
Total assets
12,972,132,222
Resilience reserve (solvency)
Gross contributions
As % of gross contributions
307,614,756
29,884,077,939
1.0%
2.4%
Resilience reserve (capital adequacy)
Gross contributions
As % of gross contributions
739,138,071
29,884,077,939
2.5%
5.7%
The resilience reserve imposes a solvency reserve of 2.4% of assets and a capital
adequacy reserve of 5.7% of assets. Furthermore, the resilience reserve adds 1.0% of
gross contributions to the solvency reserve and 2.5% of gross contributions to the
capital adequacy reserve.
4.6 Management Capital Amount
At a practical level, the management capital amount imposes a fixed dollar minimum
on both the solvency and capital adequacy reserves. The minimum solvency reserve is
$1.0 million while the minimum capital adequacy reserve is $1.5 million.
Torrance (2001) explains that many of the other components of the solvency and
capital adequacy requirements are proportional to the sizes of the insurer’s balance
sheet items or the size of the insurer. In contrast, management risks are often not
proportional to the size of the fund and are best handled by imposing a minimum
capital requirement. The minimum capital requirement also gives the public a
minimum assurance of the financial soundness of health insurers.
Table 4.7 shows the management capital amounts for registered South African
medical schemes. [Editor’s Note: in future work, this should be contrasted with the
capital needed to start a medical scheme in South Africa.]
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 35
Table 4.7: Estimate of management capital amounts
Management capital amount (solvency)
Gross contributions
As % of gross contributions
Rands
89,465,276
29,884,077,939
0.3%
Management capital amount (capital adequacy)
Gross contributions
As % of gross contributions
67,034,376
29,884,077,939
0.2%
It seems clear that the management capital amount is small, adding 0.3% of gross
contributions to the solvency reserve and 0.2% of gross contributions to the capital
adequacy reserve.
4.7 Capital Adequacy Liability
The capital adequacy liability is very similar to the solvency liability. It has the
following structure.
Capital adequacy
liability
Capital adequacy net
claims liability
Capital adequacy
reinsurance accrued
liability
Capital adequacy
other liabilities
Source: PHIAC (2000c, p.30)
Figure 4.6: Structure of capital adequacy liability
Capital adequacy other liabilities is the value of all other liabilities at their balance
sheet values. It is identical to solvency other liabilities.
The capital adequacy net claims liability is the sum of the following two quantities:
1) {1+Margin} (Outstanding claims)
2) The maximum of
a) {1+Margin} (Contributions received in advance) (Loss ratio)
b) Contributions received in advance.
With effect from 1 July 2003, the “Margin” will be removed from part 2a, making it
contributions received in advance times the loss ratio (P. Groenewegen, personal
communication, May 2, 2003). This will reduce the capital adequacy liability for
some insurers.
The capital adequacy net claims liability is essentially the solvency net claims liability
with the 10% figure replaced by “Margin”. “Margin” is the “capital adequacy margin”
and it is determined by the characteristics of the insurer in question.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 36
It has a minimum value of 12.5% to which two additions are made, namely:
The fund size addition and
The membership and claims experience stability addition.
The additions for various fund sizes are shown in the figure below.
8%
4,000 SEU's
7%
Fund size addition
6%
5%
4%
3%
20,000 SEU's
2%
1%
200,000 SEU's
0%
0
50,000
100,000
150,000
200,000
250,000
Number of SEU's
Source: PHIAC (2000c)
Figure 4.7: Fund size addition to capital adequacy margin
The standards use “Single Equivalent Units” (SEU’s) as the measure of insurer size.
This measure has its origins in the Australian risk-equalisation system (PHIAC,
2000c). Parkin (2001) explains that a single member is classified as one SEU, while
all other classes of membership (married, family etc) are classified as two SEU’s. The
relative sizes of the additions suggest that risk is reduced more by growth from 4,000
SEU’s to 20,000 SEU’s, than growth from 20,000 SEU’s to 200,000 SEU’s.
The addition for membership and claims stability requires judgement from the person
completing the calculations. It cannot be negative and 5% would be a large addition.
The more the following conditions exist, the closer the addition should be to 5%:
Membership numbers vary significantly;
Incurred claims vary significantly;
Loss ratios have been increasing over recent years; and
A new product has been introduced which is expected to affect the fund’s finances
significantly, but about which little is known.
Walker (2003) suggests a way to determine the capital adequacy margin for a given
insurer based on stability of past claims only. He proposes calculating the incurred
claims per SEU per day for each month over some sufficiently long period (18 months
in his example).
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 37
He then recommends a capital adequacy margin based on the standard deviation of
these monthly figures divided by ten. If this statistic exceeds 5%, a margin of 5% is
recommended. If it lies between 4.5% and 5%, a margin of 4.5% is recommended,
etc.
Walker argues that it is sufficient to base the margin on this standard deviation only,
because it picks up membership variability, claims variability and changing loss
ratios. The results of his calculations support this argument. The margins
recommended using this approach were similar to the margins that the insurers
participating in the study had recommended independently using their own
judgement. In response to Walker’s paper, Watson (2003) comments that the
determination of the stability addition requires judgement and can never be reduced to
a formula alone. However, Watson believes that Walker’s method does give a good
indication of experience stability.
A histogram of the capital adequacy margins for registered South African medical
schemes is shown below.
70
120%
Frequency
Cumulative %
60
100%
50
Frequency
80%
40
60%
30
40%
20
20%
10
0
12%
14%
16%
18%
20%
22%
24%
26%
0%
More
Capital adequacy margin
Figure 4.8: Histogram of capital adequacy margins
The histogram shows that 70% of the margins are between 16% and 22%.
Furthermore, none of the margins exceed 26%. Due to the 12.5% minimum, all the
margins exceed the 10% value used in the solvency liability.
The capital adequacy liability for registered South African medical schemes is shown
in Table 4.8.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 38
Table 4.8: Estimate of capital adequacy liability
Rands
Capital adequacy net claims liability
Capital adequacy other liabilities
Capital adequacy liability
Less: Total liabilities
"Contribution" to capital adequacy reserve
Gross contributions
As % of gross contributions
As % of total
liabilities
3,820,566,610
3,152,775,597
6,973,342,207
6,453,059,082
520,283,125
29,884,077,939
1.7%
108.1%
As expected, the capital adequacy liability (108.1% of liabilities) was found to be
greater than the solvency liability (105.4% of liabilities). The capital adequacy
liability added 1.7% of gross contributions to the capital adequacy reserve.
4.8 Renewal Option Reserve
Current contribution levels may be insufficient to cover claims and expenses over the
coming year. It may take some time for the insurer to realise this and adjust
premiums. In the mean time, the insurer will need sufficient capital to absorb the
losses from this under pricing and/or adverse experience if it is to avoid insolvency.
The renewal option reserve requires insurers to hold a quantity of capital to absorb
such losses.
The renewal option reserve is the NPV of cash outflows less cash inflows over the
twelve months following the valuation date, subject to a minimum value of zero.
These cash flows are based on a conservative projection of results and the insurer’s
current business plan.
More specifically, this conservative projection uses:
Contributions as in the current business plan;
Expected benefits increased by the capital adequacy margin;
Expected expenses increased by half the capital adequacy margin; and
Investment income on contributions received in advance and projected net cash
flows equal to the return on one-year Government treasury bonds less 1%. This
rate is also used as the discount rate to calculate the NPV.
From 1 July 2003, investment income on outstanding claims provision must also be
recognised (P. Groenewegen, personal communication, May 2, 2003).
The table below shows the value of the renewal option reserve for registered South
African medical schemes.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 39
Table 4.9: Estimate of renewal option reserve
Renewal option reserve
Gross contributions
As % of gross contributions
Rands
4,551,783,444
29,884,077,939
15.2%
The renewal option reserve contributes significantly to the total capital adequacy
reserve, imposing a capital adequacy reserve of 15.2% of gross contributions.
4.9 Business Funding Reserve
The insurer’s future business plan may (say) aim to grow the business by attracting
new policyholders through increased advertising and/or by expanding into new
markets. This strategy will impose marketing and advertising expenses on the insurer,
which will reduce the scheme’s capital. This expansion should not reduce the security
of existing policyholders’ claims against the insurer. Therefore, the insurer must hold
extra capital, to the value of the business funding reserve, if its business plan is likely
to reduce the scheme’s current level of capital.
The business funding reserve is basically the extra quantity of capital required to
ensure that the fund will meet the solvency requirement over the three years following
the valuation date, less any capital that the insurer has entered into binding
arrangements to raise externally in the future.
It was not possible to calculate this reserve using data from the South African medical
schemes’ 2000 statutory returns. Each scheme’s business plan for the three years
following the valuation date, as well as the expected impact of that business plan on
the scheme’s capital would be needed to calculate the business funding reserve.
4.10 Subordinated Debt Allowance
Throughout this chapter we have focused on the solvency (capital adequacy) reserves
as quantities of capital that the scheme is required to hold. To understand the
subordinated debt allowance, we need to focus on the solvency (capital adequacy)
requirements as quantities of assets that the scheme is required to hold. The coming
paragraphs will explain the subordinated debt allowance as it applies to the solvency
requirement. The allowance works similarly for the capital adequacy requirement.
The subordinated debt allowance allows the insurer to use subordinated debt as well
as equity to fund its solvency requirement. This allowance leads to the difference
between the HBFSR and the solvency requirement. That is
HBFSR Subordinat ed debt Solvency requirement .
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 40
The following example should clarify this.
Table 4.10: Balance sheet of a hypothetical insurer under various scenarios ($ millions)
Scenario A: Base case
Assets
40 Capital
Liabilities
40
HBFSR
Less: Subordinated debt
Solvency requirement
Scenario B: Equity issue
5
35
40
Assets
50 Capital
Liabilities
50
50
0
50
HBFSR
Less: Subordinated debt
Solvency requirement
15
35
50
50
0
50
Scenario C: Subordinated debt issue
(with subordinated debt allowance)
Assets
50 Capital
5
Liabilities
45
50
50
Scenario D: Subordinated debt issue
(without subordinated debt allowance)
Assets
50 Capital
5
Liabilities
45
50
50
HBFSR
Less: Subordinated debt
Solvency requirement
HBFSR
Less: Subordinated debt
Solvency requirement
60
10
50
60
10
60
Suppose an insurer with a HBFSR of $50 million has total assets of $40 million
(Scenario A in Table 4.10). There are various options to fund the extra $10 million of
assets that it needs: debt, equity or some combination of the two. If it uses equity
(Scenario B), the insurer’s total assets will increase by $10 million, its solvency
requirement will remain at $50 million and its solvency requirement will be met. If it
uses subordinated debt (Scenario C), its total assets will increase by $10 million. Its
HBFSR will increase by $10 million, since solvency other liabilities increases by $10
million, but its solvency requirement will remain the same, thanks to the subordinated
debt allowance. Therefore, the scheme will have met its solvency requirement.
If the solvency standard had no subordinated debt allowance (Scenario D), the insurer
in the above example could not have used subordinated debt to fund the extra $10
million of assets and meet the solvency requirement. The $10 million of subordinated
debt would increase assets by $10 million, to a total of $50 million. However, it
would increase the solvency requirement to $60 million. Any increase in assets
funded by subordinated debt would lead to an equal increase in the solvency
requirement. Therefore, subordinated debt could not be used to meet the insurer’s
solvency requirement.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 41
4.11 Solvency and Capital Adequacy Reserves
The first section of this chapter explained how the solvency and capital adequacy
reserves are calculated. The table below shows their values for registered South
African medical schemes.
Table 4.11: Estimate of solvency and capital adequacy reserves
Rands
Solvency liability
Expense reserve
Inadmissible assets reserve
Resilience reserve
Management capital amount
HBFSR
Less: Subordinated debt
Solvency requirement
Less: Reported liabilities
Solvency reserve
Gross contributions
As % of gross contributions
6,803,754,005
1,247,740,251
4,102,440,567
307,614,756
89,465,276
12,551,014,854
0
12,551,014,854
6,453,059,082
6,097,955,772
29,884,077,939
20.4%
As % of
reserve
5.8%
20.5%
67.3%
5.0%
1.5%
Rands
Capital adequacy liability
Renewal option reserve
Business funding reserve
Inadmissible assets reserve
Resilience reserve
Management capital amount
HBFCAR
Less: Subordinated debt
Capital adequacy requirement
Less: Reported liabilities
Capital adequacy reserve
Gross contributions
As % of gross contributions
6,973,342,207
4,551,783,444
0
2,579,028,277
739,138,071
67,034,376
14,910,326,375
0
14,910,326,375
6,453,059,082
8,457,267,293
29,884,077,939
28.3%
As % of
reserve
6.2%
53.8%
0.0%
30.5%
8.7%
0.8%
The solvency and capital adequacy reserves were estimated to be 20.4% and 28.3% of
gross contributions respectively. The “percentage of reserve column” shows how
much each component contributes to the final reserve. For the solvency and capital
adequacy liabilities, reported liabilities were subtracted first before evaluating their
contributions to the reserves.
The inadmissible assets reserve and the expense reserve together make up nearly 90%
of the solvency reserve. Similarly, the renewal option reserve and the inadmissible
assets reserve together make up nearly 85% of the capital adequacy reserve. These
components appear to be the critical parts of each formula.
4.12 Transitional Arrangements
The Australian solvency requirement is being phased in over the calendar years 2001
to 2005. As for the subordinated debt allowance, the solvency requirement must be
interpreted as a minimum quantity of assets to understand the transitional
arrangements. Figure 4.9 shows how this transition is taking place.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 42
100%
100%
HBFSR
83%
67%
50%
Transitional
requirements
33%
17%
0%
Old
requirement
2000
2001
2002
2003
2004
2005
2006
2006
Source: PHIAC (2000a)
Figure 4.9: Transitional arrangements
In 2001, insurers were required to hold assets in excess of the old capital requirement
plus 17% of the difference between the HBFSR and the old requirement. Over the
years 2002 to 2006, this 17% will increase by 17% each year until the full HBFSR is
reached and the new solvency requirement is fully implemented. The health benefits
fund capital adequacy requirement (HBFCAR) is being phased in similarly.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 43
5. The effect of RBC on South African Medical
Scheme Solvency
This chapter will estimate the effect of RBC on South African medical scheme
solvency both at the industry level and at the individual scheme level. In doing so it
will also compare the size and effect of the USA and Australian RBC requirements.
5.1 Methodology
Ideally, to estimate the effect a RBC system would have on South African medical
scheme solvency, a RBC system developed for South African medical schemes
should be applied to South African data. Since no such RBC system existed at the
time of writing, foreign RBC systems were applied to South African data. The results
of these calculations were used to estimate the effect a RBC system would have on
South African medical scheme solvency.
More precisely, the USA and Australian RBC requirements were estimated for South
African medical schemes at 31 December 2000, using data from their 2000 statutory
returns. Some of the results of these calculations have already appeared in the
previous two chapters.
Appendices C, D and E set out exactly what data was used to calculate each part of
the USA RBC requirement, the Australian solvency reserve, and the Australian capital
adequacy reserve respectively. International differences and data availability meant
that approximations and assumptions were sometimes necessary. These
approximations and assumptions are also recorded in the relevant appendices.
5.2 Industry Level
This section estimates the impact of a RBC system on South African medical scheme
solvency at the industry level. It does this by comparing the RBC requirements of
different aggregates of schemes to the accumulated funds of those aggregates.
5.2.1 Aggregate solvency
Figure 5.1 shows the total value of the four different capital requirements for
registered schemes.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 44
9,000
8,457
8,000
7,471
7,000
6,098
6,000
R millions
5,127
5,000
4,000
3,338
3,000
2,000
1,000
0
Risk-based capital after
covariance
Solvency reserve
25% of gross contributions
Capital adequacy reserve
Accumulated funds
Figure 5.1: Accumulated funds and capital requirements for registered schemes
Comparing the capital requirements to accumulated funds, we see that the USA RBC
system finds the industry adequately capitalised. However, both the Australian
solvency standard and the South African 25% rule suggest that registered schemes
should be holding more accumulated funds.
The capital requirements can also be compared to one another. Both the USA RBC
requirement and the Australian solvency reserve are lower than the current 25% of
gross contributions requirement, whereas the capital adequacy reserve is R1 billion
higher than the 25% requirement. This implies that the USA system would allow
registered medical schemes to hold less capital than the current requirement. On the
other hand, the Australian system would require registered medical schemes to hold
more reserves than the current requirement.
5.2.2 Aggregate solvency by scheme type
Figure 5.2 shows the total capital requirements, as a percentage of gross contributions,
for different scheme types. The capital requirements are expressed as a percentage of
gross contributions for ease of comparison.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 45
45%
Registered
Registered - open
40%
38.2%
Registered - restricted
Percentage of gross contributions
35%
30%
28.3%
25.0%
25%
25.3%
23.7%
20.4%
20%
18.3%
17.2%
15.6%
15%
13.3%
11.2%
10%
9.1%
5%
0%
Risk-based capital after covariance
Solvency reserve
Capital adequacy reserve
Accumulated funds
Figure 5.2: Capital requirements as a percentage of gross contributions (by scheme type)
Comparing the capital requirements to accumulated funds, we see that the USA RBC
system would find that both scheme types are holding sufficient accumulated funds.
The Australian system would find that neither scheme type is adequately capitalised,
since neither scheme type satisfies the capital adequacy reserve. Only the restricted
schemes meet the Australian solvency requirement.
Comparing the capital requirements for different scheme types, we see that both the
USA and Australian systems require restricted schemes to hold a larger percentage of
gross contributions as reserves than open schemes. This implies that the RBC systems
find the restricted schemes “riskier” than the open schemes. The restricted schemes
tend to have lower membership than the open schemes, so this is probably a scheme
size effect rather than a scheme type effect. In reality, open schemes face a greater
risk of adverse claims fluctuations due to their open enrolment and restricted
underwriting (ASSA, 2002). This suggests that a South African RBC system may
need to include an indicator that somehow increases the requirement for open
schemes (Professor McLeod, personal communication, April 10, 2003). Another way
to handle this would be to set up different requirements for open and restricted
schemes. In other words, use different RBC factors for open and restricted schemes
respectively.
The horizontal black line shows the current 25% of gross contributions requirement.
On the whole, the USA system would allow registered schemes to hold less than 25%
of gross contributions as reserves, while the Australian system would require
registered schemes to hold more than 25% of gross contributions as reserves.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 46
5.2.3 Aggregate solvency by scheme size
Figure 5.3 shows the total RBC requirements, as a percentage of gross contributions,
for registered schemes by scheme size.
50%
47.0% 46.8%
Small
Medium
Large
45%
40.0%
Percentage of gross contributions
40%
34.9%
34.0%
35%
31.3%
30%
24.3%
25%
20%
18.5%
19.4%
17.7%
15%
10%
12.7%
9.5%
5%
0%
Risk-based capital after covariance
Solvency reserve
Capital adequacy reserve
Accumulated funds
Figure 5.3: Capital requirements as a percentage of gross contributions (by scheme size)
The size classifications small (<6000 members), medium (>6000 members and
<30000 beneficiaries) and large (>30000 beneficiaries) are based on the Annual
Report of the Registrar of Medical Schemes (2001).
Comparing the capital requirements to accumulated funds shows that the small and
medium schemes meet the USA requirement and the Australian solvency reserve, but
not the capital adequacy reserve. Large schemes meet the USA RBC requirement but
neither of the Australian reserve requirements.
Comparing the capital requirements for different scheme sizes shows that the RBC
systems require small and medium schemes to hold roughly the same proportion of
gross contributions as reserves. However, they allow large schemes to hold a
significantly smaller percentage of gross contributions as reserves.
Both Australian reserves require small and medium schemes to hold more than 25%
of gross contributions as reserves. For large schemes, the Australian solvency reserve
is less than 25% while the capital adequacy reserve is approximately 25%. The USA
RBC requirement is lower than 25% for all three scheme sizes.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 47
5.3 Individual Scheme Level
This section estimates the effect of a RBC system on South African medical scheme
solvency at the individual scheme level. It does this by showing the range of capital
requirements that schemes would be required to hold under a RBC system and by
reporting the proportions of schemes that meet the various capital requirements.
5.3.1 Range of individual scheme capital requirements
Figure 5.4 shows the distribution of the different capital requirements, as well as the
distribution of accumulated funds.
70
Risk-based capital after covariance
Solvency reserve
60
Capital adequacy reserve
Accumulated funds
Number of schemes
50
40
30
20
10
0
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
55%
60%
65%
70%
75%
80%
85%
90%
95% 100% More
Percentage of gross contributions
Figure 5.4: Histogram of capital requirements for registered schemes
The main feature of this graph is the large range in capital requirements. If a RBC
system were introduced in South Africa, some schemes would be allowed to hold less
than the current 25% of gross contributions, while others would be required to hold
substantially more.
Schemes with very small annual contributions are often required to hold more than
25% of gross contributions. Under the Australian system, the inadmissible assets
charge (which makes up 67.3% of the solvency reserve and 30.5% of the capital
adequacy reserve, see Table 4.11) is often behind these large capital requirements.
Some schemes have large outstanding contributions, which add significantly to the
assets used in the conduct of business charge. Other schemes have large asset
concentration charges.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 48
5.3.2 Individual scheme solvency by scheme type
Figure 5.5 shows the percentages of each type of scheme that meet the various capital
requirements.
80%
Registered
70%
68.9% 68.1%
Registered - open
69.3%
Registered - restricted
Percentage of schemes that are solvent
61.4%
58.4%
60%
54.7%
52.0%
50%
40.4%
38.3%
40%
39.6%
37.8%
34.0%
30%
20%
10%
0%
US risk-based capital standard
Solvency standard
25% of gross contributions rule
Capital adequacy standard
Figure 5.5: Percentages of schemes that are solvent (by scheme type)
Comparing the RBC standards to the current requirement, we see that more schemes
are solvent under the USA RBC standard and the Australian solvency standard than
under the current 25% of gross contributions rule. On the other hand, a smaller
percentage of each scheme type is solvent under the Australian capital adequacy
standard than under the current 25% of gross contributions rule.
We can also compare the solvency of the different scheme types. Under each RBC
standard, the proportion of restricted schemes that are solvent is larger than the
proportion of open schemes that are solvent.
5.3.3 Individual scheme solvency by scheme size
Figure 5.6 shows the percentages of registered schemes that meet the various capital
requirements, by scheme size.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 49
80%
Small
73.3%
70%
Large
68.2%
65.1%
63.6%
Percentage of schemes that are solvent
Medium
60.0%
60%
59.3%
59.1%
50.0%
50%
40.0%
38.4%
40%
30.0%
30%
20.0%
20%
10%
0%
US risk-based capital standard
Solvency standard
25% of gross contributions rule
Capital adequacy standard
Figure 5.6: Percentages of schemes that are solvent (by scheme size)
More large schemes are solvent under the three RBC standards than under the current
25% of gross contributions rule. This suggests that the current capital requirement for
large schemes is quite conservative. A larger percentage of medium schemes are
solvent under the USA RBC standard and the Australian solvency standard than under
the current 25% of gross contributions rule. A larger percentage of small schemes are
solvent under the USA RBC standard than under the current 25% of gross
contributions rule.
Comparing the solvency of the different scheme types shows that under each of the
four solvency standards, the percentage of small and medium schemes that are solvent
is higher than the percentage of large schemes that are solvent.
5.4 Summary
This section summarises the estimated effect of the various RBC systems on South
African medical scheme solvency.
Industry level:
Registered schemes are solvent under the USA RBC system but insolvent under
all others.
The USA RBC system and Australian solvency standard allow registered schemes
to hold less than 25% of gross contributions, whereas the Australian capital
adequacy standard requires registered schemes to hold more than 25% of gross
contributions.
Restricted schemes are required to hold a larger percentage of contributions as
reserves than open schemes.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 50
Small and medium schemes are required to hold a larger percentage of
contributions as reserves than large schemes.
Individual scheme level:
Under a RBC system, some schemes are allowed to hold less than 25% of gross
contributions as reserves; others are required to hold significantly more.
More registered schemes are solvent under the USA RBC system and the
Australian solvency standard than under the current 25% of gross contributions
rule. In contrast, fewer registered schemes are solvent under the Australian capital
adequacy standard than under the current 25% of gross contributions rule.
A larger proportion of restricted schemes than open schemes are solvent.
A larger proportion of small and medium schemes than large schemes are solvent.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 51
6. A Comparison of the Australian and USA RBC
Systems
This chapter will compare the Australian and USA RBC systems. Where possible, it
will highlight issues that may be relevant to the development of a RBC system for
South African medical schemes.
6.1 Conceptual Framework
The USA and Australian RBC systems are based on different conceptual frameworks.
The USA system is based on a particular probability of ruin, while the Australian
system requires insurers to hold capital to meet certain circumstances. The following
paragraphs will discuss the merits of each framework.
6.1.1 Probability of ruin
The probability of ruin approach is closely related to the underlying stochastic model.
This enables the use of statistical techniques to estimate the risk factors in the USA
RBC formula. Such techniques support the level of detail and the number of different
factors in the standards.
6.1.2 Capital to meet specific circumstances
The Australian solvency and capital adequacy standards require insurers to hold
enough capital to meet their current obligations if the fund was closed to new business
and to continue to meet their obligations as a going concern. This form of capital
requirement is easily understood by a layperson, but it is more difficult to use
statistics to estimate this type of capital requirement.
The two-tier solvency and capital adequacy requirement is equivalent to Campagne’s
notion of static and dynamic solvency. Cooper (2001) explains that static solvency
refers to an insurer’s ability to meet current outstanding claims and existing
obligations in a run-off situation. Dynamic solvency requires the insurer to hold
sufficient capital to have a high probability of remaining solvent while it writes new
business and continues to grow.
The South African capital adequacy standard for life insurers also requires insurers to
hold capital to meet certain circumstances. The Actuarial Society of South Africa
(2001) explains that the insurer is required to hold the greater of the “termination
capital adequacy requirement” and the “ordinary capital adequacy requirement.” The
first of these requires the insurer to hold enough capital to pay the lapse and surrender
values on all its policies, while the second requires the insurer to hold sufficient
capital to withstand adverse experience and continue doing business as a going
concern
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 52
6.1.3 Suitable conceptual framework for a South African RBC system
In the USA and Australia, the health RBC systems were both based on RBC systems
already developed for other types of insurers in those countries. Therefore, one
possibility for a South African RBC system for medical schemes would be to consider
the RBC system currently in use for South African life offices. This implies requiring
schemes to hold capital to meet certain circumstances. The Australian system will
thus provide an understanding of this approach in the context of South African
medical schemes.
6.2 Components of Each Formula
The table below shows what risks the various sections of each RBC system reserve
against. A question mark indicates a possible omission from the RBC system.
Table 6.1: Risks and corresponding sections of RBC standards
Risk
Australian solvency
standard
US RBC standard
Australian capital
adequacy standard
Asset risk
Adverse systematic market
movements
Asset risk - affiliates and
other
Resilience reserve
Asset concentration and nonsystematic risk
Asset risk - other, asset
concentration
Inadmissible assets reserve, Inadmissible assets reserve,
asset concentration risk
asset concentration risk
Asset realisation/liquidity
NA
Inadmissible assets reserve,
assets used in the conduct NA
of business
Holdings in institutions
required to hold RBC
Inadmissible assets reserve, Inadmissible assets reserve,
Asset risk - affiliates, affiliates
holdings in prudentially
holdings in prudentially
subject to RBC
regulated institutions
regulated institutions
Resilience reserve
Liability risk
Reserve adequacy
Underpricing
Catastrophic losses
Underwriting risk, base
Solvency liability
underwriting risk RBC
Underwriting risk, base
NA
underwriting risk RBC
Underwriting risk, alternative
risk charge
Capital adequacy liability
Renewal option reserve
?
?
Other risks
Expense risk
Business risk, administration
expense charge
Expense reserve
Management and business
risk
Business risk
Management capital amount Management capital amount
Credit and counter party risk
Growth risk
Credit risk, reinsurance and
capitation risk
Business risk, excessive
growth charge
Renewal option reserve
Implied
Implied
NA
Business funding reserve
The Australian solvency standard is based on a run-off view of the fund, while the
USA RBC formula and the Australian capital adequacy standard view the fund as a
going concern. This is why some risks in Table 6.1 are not applicable to the various
capital requirements.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 53
Furthermore, although no explicit provision is made, the Australian standards take
credit risks and counter party risk into account implicitly. That is, they assume that the
balance sheet values of individual assets reflect the default risk of those assets.
Based on Table 6.1 and the developments of the earlier chapters, there appear to be
one or two minor omissions from the standards.
6.2.1 Omissions from the USA formula
The USA RBC formula makes no allowance for the risk that arrear contributions are
irrecoverable. As mentioned earlier, this is because USA MCO’s do not have
significant exposure to this risk (A. Ford, personal communication, May 2, 2003).
South African medical schemes do, however, face significant exposure to such bad
debts. In the calendar year 2000, registered medical schemes wrote off R80.2 million
in bad debts on their way to an overall net surplus of R242.3 million. Clearly, if a
system like the USA were implemented in South Africa, it would need to include an
allowance for bad debts.
6.2.2 Omissions from the Australian formulae
The Australian RBC formulae do not allow for
The risk of catastrophic claims or
Covariance between the different risks.
The USA formula, through its alternative risk charge, allows for the risk of
catastrophic claims, while the Australian formulae make no such allowance. Torrance
(2001) writes that the risk from large individual claims was identified as a risk to be
considered under the solvency and capital adequacy standards. It appears that this
never actually happened. A South African RBC standard built along the lines of the
Australian system should try to include such a risk charge.
The Australian formulae make no allowance for covariance between the different
risks. This is both a weakness and strength of the formula. Without a covariance
adjustment, the formula is simpler and less intimidating. However, including an
adjustment would be more theoretically correct.
Covariance adjustments, the USA covariance adjustment in particular, are the subject
of much debate (Section 3.7 touched on some of the different viewpoints). It is the
author’s opinion that any South African RBC formula would be better off without
such an adjustment. A complicated adjustment would make the industry suspicious of
the formula and less likely to support its implementation.
6.2.3 Relative sizes of the different components
Figure 6.1 shows the contribution of the different risk charges to each of the RBC
requirements.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 54
0.8%
100%
7.2%
90%
21.9%
80%
Proportion of capital requirement
5.8%
70%
60%
60.0%
61.9%
50%
40%
72.3%
30%
20%
39.2%
30.9%
10%
0%
Risk-based capital before covariance
Solvency reserve
Asset risk
Liability risk
Capital adequacy reserve
Other risk
Figure 6.1: Components of capital requirements for registered schemes
There is some similarity between the relative importance of the Australian capital
adequacy reserve’s constituent risk charges and those of the risk-based capital before
covariance. The liability risks are of very similar importance. The importance of the
components of the solvency reserve is quite different to the other two requirements.
This is because the solvency reserve is based on a run-off view of the fund while the
other requirements aim to secure the fund’s future as a going concern.
When a scheme is closed to new business and run-off, its only liability risk is that
technical reserves are insufficient. An ongoing operation faces this risk as well as the
risk that future claims are higher than expected. This suggests that liability risk is
more important for a going concern than for a scheme that is closed to new business.
A scheme that is closed to new business also faces the risk that its assets are not
realisable at their balance sheet values, as well as the risk of market fluctuations. An
ongoing operation would have less exposure to these asset realisation risks and would
be able to realise the value of its assets over their useful lives. This suggests that asset
risk is less important for an ongoing operation than for a scheme that is closed to new
business.
6.3 Special features of each formula
6.3.1 Special features of the USA formula
Special features of the USA formula are its allowance for transfer of risk through
Reinsurance and
Managed care.
The Australian formulae do not have these features.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 55
The transfer of risk through reinsurance is allowed for implicitly by basing the
underwriting risk charge on contributions and claims net of reinsurance premiums and
recoveries. Likewise, the alternative risk charge is based on claims after reinsurance
recoveries. The credit risk section of the formula allows for the risk that the reinsurer
will default on obligations to the MCO.
As explained in Section 3.4.2, the MCO’s underwriting risk charge is reduced where
the MCO shares risk with the providers of medical services. The reduction is larger
when more risk is transferred to the provider. As for reinsurance, the credit risk
section makes allowance for the possibility that the providers will default on their
obligations to the MCO.
Both of these features are based on the premise that reinsurance and managed care
arrangements actually transfer risk away from the scheme and that reinsurers and
MCO’s are also required to hold capital. In constructing a South African RBC system,
the need for such allowances will be determined by the types of reinsurance and
managed care arrangements in use, as well as the capital requirements of these other
organisations.
Section 20 of the Medical Schemes Act of 1998 (as amended) requires that all
reinsurance contracts need to be approved by the registrar. Furthermore, the Actuarial
Society of South Africa (2002) defines a reinsurance agreement as
“… any contractual arrangement whereby some element of risk
contained in the rules of the medical scheme is transferred to a
reinsurer in return for some consideration.” (ASSA, 2002, p.1)
This suggests that future medical scheme reinsurance arrangements are likely to
transfer risk to the reinsurer. In addition, South African long-term insurers are
required to hold minimum amounts of capital. Therefore, a South African RBC
system should incorporate an allowance for risk transfer through reinsurance.
Currently, South African medical schemes are obliged to hold 25% of gross
contributions with no allowance for the transfer of risk through reinsurance. 2004 is
the first full year of data that the Council for Medical Schemes will have on the effect
of reinsurance on medical schemes. Therefore, late 2005 is the earliest that the council
may consider incorporating a reinsurance offset in the current capital requirement
(Professor McLeod, personal communication, May 14, 2003).
The managed care allowance is a different story altogether. South African MCO’s are
not required to hold minimum amounts of capital, so to reduce a scheme’s capital
requirement because of contracts with an MCO would reduce the total amount of
capital in the industry (Professor McLeod, personal communication, April 3, 2003).
Furthermore, a managed care allowance would have little effect on the industry at
present. Therefore, a South African RBC formula should not include a managed care
allowance.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 56
6.3.2 Special features of the Australian formulae
Noteworthy features of the Australian formulae are their
Specification of a method to determine outstanding claims and
Interaction with the Australian risk-equalisation system.
The USA formula does not have these special features.
The specification of a method to determine outstanding claims attempts to reduce the
scope for an insurer to manipulate reserves in order to reduce its capital requirement
and increase the capital on its balance sheet.
The ASSA and the South African Institute of Chartered Accountants (2003) brought
out professional guidelines on the estimation of IBNR claim liabilities for South
African medical schemes, which list a number of factors that need to be considered
when estimating these liabilities. Since guidance is already available, it would be
unnecessary for a South African RBC system to specify a method for calculating
IBNR liabilities.
Although this report paid very little attention to the parts of the Australian standards
relating to their risk-equalisation system, it recognises that the two systems interact.
The standards treat amounts payable and receivable in terms of the risk-equalisation
system differently to other payables and receivables, see PHIAC (2000c, p.9 & pp.4748) for the details. A risk-equalisation system is currently being developed for South
African medical schemes. Any RBC system for medical schemes should be consistent
with this risk-equalisation system.
6.4 Meeting the requirements
The USA standard requires an MCO to hold a minimum quantity of equity. The
Australian standards require insurers to hold a quantity of assets, in addition to those
supporting the liabilities, which may be financed by either equity or subordinated
debt.
A South African RBC system would probably require schemes to hold a minimum
quantity of accumulated funds. A disadvantage of accumulated funds is that its
definition allows more scope for interpretation than equity or subordinated debt.
6.5 Basis for intervention
The USA standards are extremely clear on what action the regulator should take for
every possible level of MCO equity. This makes regulation transparent and brings
certainty to the industry, but it can be quite restrictive for the regulator.
The regulatory responses under the Australian standards are less prescriptive than
under the US. For instance, it is not clear on exactly what actions are to be taken in
the event of a breach of the standards. Furthermore, part VI, division 3 A & B of the
Australian National Health Act (1953) gives the PHIAC the right to issue directions to
insurers even if they meet the requirements of both the solvency standard and the
capital adequacy standard. Although this provides flexibility to the regulator, it does
not give insurers as much certainty as the USA system.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 57
7. Conclusions and Further Research
Based on the findings of this report, the following conclusions may be drawn:
1. Both the USA and Australian RBC systems have features that may be useful
in the South African environment.
The RBC systems studied in this report both have features that may be useful when
developing a RBC system for South African medical schemes. They give insight into
some of the adjustments that would need to be made to make them suitable for
medical schemes. The USA system’s allowance for risk transfer through reinsurance
contracts, as well as the Australian system’s interaction with the Australian riskequalisation system, suggests issues to be considered in the development of a RBC
system.
2. At the industry level, the effect of a RBC system on South African medical
scheme solvency is unclear.
It is unclear whether a RBC system would require the industry to hold more or less
capital than 25% of gross contributions. The USA system would allow the industry to
hold substantially less, while the Australian requirements straddle the 25% of gross
contributions requirement. It appears that each different RBC system would have a
different effect on medical scheme solvency.
3. Differing individual scheme capital requirements would lead to winners and
losers under a RBC system
Both RBC systems studied allowed some schemes to hold less than 25% of gross
contributions, while other schemes were required to hold substantially more than
25%. Schemes required to hold more than 25% may feel that the system is biased
against them and be opposed to the use of RBC. Schemes required to hold less than
25% of gross contributions, often the larger schemes, would probably support the
introduction of RBC.
It is recommended that the following be investigated:
1. Starting Points for a RBC system for South African Medical Schemes.
The USA and Australian RBC systems provide insight into the features a RBC system
for medical schemes could have. These systems and the current RBC system for
South African life insurers provide possible starting points for the construction of a
RBC system for South African medical schemes. The investment (asset) sections of
the life insurance formula may not need major changes, while the liability sections
will need to be reconstructed to suit medical schemes.
[See Editor’s Note for research now needed]
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 58
8. References and Bibliography
8.1 Australia
Cumpston, J. R. (1992). Margins for Prudence in Outstanding Claims Provisions.
Proceedings of Eighth General Insurance Seminar, Institute of Actuaries of Australia,
211-238.
Macquarie Bank Limited website. (n.d.). Retrieved April 18, 2003 from
http://www.macquarie.com.au.
Office of Legislative Drafting, Attorney-General’s Department, Canberra. National
Health Act (1953), [Online]. Available: http://scaleplus.law.gov.au. [2003, January 6].
Parkin, N. (2001). Risk Equalisation in practice. B.Bus.Sc. project. University of
Cape Town.
Private Health Insurance Administration Council. (2000a). Health Benefits
Organizations
–
Solvency
Standard
2000,
[Online].
Available:
http://www.phiac.gov.au. [2003, January 10]
Private Health Insurance Administration Council. (2000b). Health Benefits
Organizations – Capital Adequacy Standard 2000, [Online]. Available:
http://www.phiac.gov.au. [2003, January 10]
Private Health Insurance Administration Council. (2000c). Health Benefits
Organizations
–
Interpretation
Standard
2000,
[Online].
Available:
http://www.phiac.gov.au. [2003, January 10]
Private Health Insurance Administration Council. (2001). Managing Supervision and
Intervention March 2001 Guidelines, Received through personal communication with
P. Groenewegen. [2003, May 5].
Private Health Insurance Administration Council. (2002). Review of the Solvency and
Capital Adequacy Standards – Discussion Paper, August 2002, [Online]. Available:
http://www.phiac.gov.au. [2003, January 10]
Taylor, G. C. (1996). Risk, Capital and Profit in Insurance, University of Melbourne
research
paper
number
39.
[Online].
Available:
http://www.economics.unimelb.edu.au/actwww/. [2003, April 14]
The Institute of Actuaries of Australia. (2000). Comments on the solvency and capital
adequacy standards exposure draft for the private health insurance industry,
[Online]. Available: http://www.actuaries.asn.au. [2003, January 10].
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 59
The Institute of Actuaries of Australia. (1999). Guidance Note 650 – Actuarial reports
and advice on outstanding claims in health insurance, [Online]. Available:
http://www.actuaries.asn.au. [2003, January 10]
The Institute of Actuaries of Australia. (2002). Guidance Note 660 – Financial
projections for health insurers, [Online]. Available: http://www.actuaries.asn.au.
[2003, January 10]
The Institute of Actuaries of Australia. (n.d.). Submission on the draft solvency and
capital adequacy standards for the private health insurance industry, [Online].
Available: http://www.actuaries.asn.au. [2003, January 10].
Torrance, D. (2001). The Development of Prudential Requirements for Private Health
Insurers, Institute of Actuaries of Australia Biennial Convention, 2001. Received
through personal communication with D. Watson. [2003, March 23].
Walker, B. (2003). Health Insurance Membership and Claims Experience Stability
Margin, [Online]. Available: http://www.actuaries.asn.au. [2003, May 10].
Watson, D. (2003). Newsletter on Private Health Insurance in Australia, 107,
[Online]. Available:
http://www.actuaries.asn.au/PublicSite/about_us/hpcnewsletters.htm. [2003, June 11].
8.2 United States of America
Actuarial Society of South Africa Healthcare Committee. (n.d.). Demystifying the US
Risk-Based Capital formula, Unpublished document provided to the Financial
Soundness working group of the Council for Medical Schemes.
Barth, M. M. (2000). A Comparison of Risk-Based Capital Standards Under the
Expected Policyholder Deficit and the Probability of Ruin Approaches. The Journal
of Risk and Insurance, 67(3), 397-414.
Barth, M. M. (1999). Applying the Law of Large Numbers to P&C Risk-Based
Capital. Journal of Insurance Regulation, 17(4), 438-477.
Butsic, R. P. (1994). Solvency Measurement for Property-Liability Risk-based Capital
Applications. The Journal of Risk and Insurance, 61(4), 656-690.
Milliman & Robertson. (1998). Risk-Based Capital Requirements for Managed Care
Organisations. [Online]. Available: http://www.milliman.com. [2003, January 10].
National Association of Insurance Commissioners (NAIC). (2001). Risk-Based
Capital Report Including Overview and Instructions for Companies. Kansas City,
Mo.: NAIC.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 60
8.3 South Africa
Actuarial Society of South Africa (2001). PGN104: Life Offices – Financial
Soundness
Valuation,
[Online].
Available:
http://www.assa.organisation.za/guidance/pgn104.htm [2002, November 18]
Actuarial Society of South Africa Healthcare Committee. (2002). Draft professional
guidance note: Advice to South African Medical Schemes On Reinsurance, Circulated
electronically by Healthcare Committee.
Actuarial Society of South Africa and South African Institute of Chartered
Accountants. (2003). Professional Guidelines: IBNR Liability Valuations of South
African Medical Schemes, Circulated electronically to the Financial Soundness
Working Group of the Council for Medical Schemes.
Bodie, Z., Kane, A., & Marcus, A. (1999). Investments (4th ed.). Boston: McGrawHill.
Bond Exchange of South Africa website. (n.d.). Retrieved April 16, 2003, from
http://www.besa.org.za.
Cooper, M. (2001). Extracts from Solvency and Medical Schemes in South Africa,
Unpublished discussion document provided to the Financial Oversight Committee and
the staff of the Council for Medical Schemes.
Council for medical schemes. (2001). Annual report of the registrar of medical
schemes 2001. [Online]. Available: http://www.medicalschemes.com. [2003, April
18].
Council for medical schemes. (2003). Review of the factors that influence financial
soundness of medical schemes, [Online]. Available: http://www.medicalschemes.com.
[2003, April 30].
Doherty, J., & McLeod, H. (2002). Are medical schemes becoming more affordable?
In Health Systems Trust, South African Health Review 2002 (pp.41-66). Durban:
Health Systems Trust.
Dreyer, S. (2002). A study of the Exempt Medical Schemes. B.Bus.Sc. project.
University of Cape Town.
South African Government (1998) Medical Schemes Act, 1998 (Act No. 131 of 1998),
Government Gazette No. 19545, Vol. 402, 2 December 1998. Also, Medical Schemes
Amendment Act, 2001.
South African Government (1999) Regulations in terms of the Medical Schemes Act,
1998, Government Notice, Regulation Gazette No. 6652, Vol. 412, 20 October 1999.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 61
South African Government. (1998). Requirements & Guidelines to be complied with
for registration of a medical scheme in terms of the medical schemes act, 1998 (Act
No 131 of 1998), Government Gazette No. 19545, Vol. 402, 2 December 1998.
The South African Institute of Chartered Accountants. (2003). Audit and Accounting
Guide on Medical Schemes (Draft), [Online]. Available: http://www.saica.co.za.
[2003, April 7].
Van Den Heever, R. J. (1998). Risk Adjusted Capital in a General Insurance
Environment. Transactions of the Actuarial Society of South Africa, XII(1), 154-173.
8.4 General
Cummins, J., Harrington, S., & Niehaus, G. (1993). An Economic Overview of RiskBased Capital for the Property-Liability Insurance Industry. Journal of Insurance
Regulation, 11(4), 427-447.
Hooker, N. D., Bulmer, J. R., Cooper, S. M., Green, P. A. G., & Hinton, P. H. (1996).
Risk-Based Capital in General Insurance. British Actuarial Journal, 2(II), 265-323.
Kongsveldt, P. R. (1996). The Managed Health Care Handbook (3rd ed.). Maryland:
Aspen Publishers.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 62
Appendix A: Data Files Submitted to the Council
for Medical Schemes
Report.doc
Data/Australia.xls
Data/US.xls
Tables and figures/Tables and figures.xls
Tables and figures/Figures.ppt
Correspondence/Useful contacts.xls
Correspondence/Various emails
Electronic documents/…
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 63
Appendix B: RBC Theory
B1. Calculation of RBC requirements using the EPD
and probability of ruin approaches
Following the approach of Butsic (1994), a simplified version of a medical scheme is
used to explain the two approaches. The scheme is assumed to have assets with a
~
fixed value (A) and liabilities with a random value ( L ).
B1.1 Ruin Approach
~
As long as the value of assets exceeds the value of liabilities ( A L ) the scheme is
~
solvent. If the value of liabilities exceeds the value of assets ( A L ) the scheme is
insolvent or “ruined”. The ruin approach sets the minimum capital requirement for a
~
medical scheme by targeting a certain probability of ruin ( Pr[ A L ] ). The following
numerical example will illustrate the ruin approach. Assume the regulator sets the
minimum capital requirement to ensure a 5% probability of ruin.
Table B1: Balance sheet of a hypothetical medical scheme under various scenarios
Asset
Amount
0.20
12,000
0.60
12,000
0.15
12,000
0.05
12,000
12,000
Source: Butsic (1994)
Probability
Scenario 1
Scenario 2
Scenario 3
Scenario 4
Expectation
Loss
Amount
8,500
10,000
11,000
13,000
10,000
Capital
Amount
2,000
The scheme in Table B1 has assets of R12,000; liabilities with an expected value of
R10,000 and capital of R2,000. The scheme is solvent under the first three scenarios
but insolvent under the fourth. Since the probability of the fourth scenario is 5%, the
scheme has a 5% probability of ruin. If the scheme held less capital than R1,000 (i.e.
R11,000-R10,000), it would be insolvent under scenario three also, increasing its
probability of ruin to 20%. Therefore, R1,000 is the minimum amount of capital
required for this medical scheme to achieve a 5% ruin probability. R1,000 is this
scheme’s RBC requirement.
The scheme in Table B1 holds capital in excess of its RBC requirement, so it would
not suffer any regulatory action. This minimum capital requirement is equivalent to
10% of the balance sheet value of liabilities. Therefore, the regulator could express
the RBC requirement for the scheme as 0.1 Liabilitie s . This observation may seem
trivial, but it is crucial for understanding the USA RBC formula in Chapter 3The
factor of 0.1 is known as a risk-based capital factor. It is the ratio of the risk charge to
the value of the risk element. Here the risk element is the liability.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 64
B1.2 Expected policyholder deficit (EPD) approach
Butsic (1994) suggests that the probability of ruin approach is inappropriate and that
the severity of ruin needs to be taken into account too. For this reason he supports the
expected policyholder deficit approach to setting RBC requirements. He used a
numerical example similar to the one below to explain his point of view:
Table B2: Two schemes with the same balance sheets but different loss distributions
Scheme A
Probability
Scenario 1
Scenario 2
Scenario 3
Scenario 4
Expectation
0.20
0.60
0.15
0.05
Asset
Amount
12,000
12,000
12,000
12,000
12,000
Loss
Amount
8,500
10,000
11,000
13,000
10,000
Capital
Amount
Asset
Amount
12,000
12,000
12,000
12,000
12,000
Loss
Amount
8,000
10,000
11,000
15,000
10,000
Capital
Amount
2,000
Claim
Payment
8,500
10,000
11,000
12,000
9,950
Deficit
0
0
0
1,000
50
Scheme B
Probability
Scenario 1
Scenario 2
Scenario 3
Scenario 4
Expectation
0.20
0.60
0.15
0.05
2,000
Claim
Payment
8,000
10,000
11,000
12,000
9,850
Deficit
0
0
0
3,000
150
Source: Butsic (1994)
Schemes A and B both have R12,000 of assets, a R10,000 expected loss (liability) and
capital of R2,000. However, the distributions of their losses differ. Both schemes are
insolvent under scenario four and have a 5% probability of ruin, but scheme B’s
policyholders have more unpaid claims than scheme A’s when the schemes are
insolvent. Scheme A’s policyholders can expect R50 of unpaid claims while scheme
B’s policyholders can expect R150. The probability of ruin alone doesn’t capture the
full danger of insolvency for the policyholders; the severity of ruin needs to be
considered too.
This example suggests that the expected difference between the claims the insurer is
obliged to pay and the actual payments made (i.e. the expected policyholder deficit)
would be a good indication of the danger of insolvency. In fact, to adjust for different
liability sizes, the ratio of expected policyholder deficit to expected losses (i.e. the
EPD ratio) is used as the measure of the danger of insolvency.
Continuing with the example in Table B2, if the regulator required a 0.01 ratio of EPD
to expected loss (i.e. a 0.01 EPD ratio) the schemes would have to hold capital as in
the following table:
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 65
Table B3: Calculation of minimum capital requirement
(1) Required EPD ratio
(2) Expected loss
(3) Required expected deficit [(1)*(2)]
(4) Required deficit - scenario 4 [(3)/.05]
(5) Loss amount - scenario 4
(6) Required claim payment - scenario 4 [(5)-(4)]
(7) Required assets [(6)]
(8) Minimum capital requirement [(7)-(2)]
Source: Barth (2000)
Scheme A
0.01
10,000
100
2,000
13,000
11,000
11,000
1,000
Scheme B
0.01
10,000
100
2,000
15,000
13,000
13,000
3,000
Therefore, Scheme A has a RBC requirement of R1,000, while scheme B has a
R3,000 RBC requirement. The capital requirement can be expressed per unit of
liabilities (capital requirement/value of liabilities). That is, Scheme A is required to
hold 0.1 Liabilitie s , while scheme B is required to hold 0.3 Liabilitie s .
B1.3 More complicated situations
Clearly the examples used to illustrate the ruin and EPD approaches are unrealistic;
medical schemes face multiple risks – not just liability risk. Nevertheless, the
techniques used in these unrealistic examples are also of value in more complicated
situations involving multiple risks. This is because the capital requirement for a
scheme facing multiple risks is calculated by evaluating the capital needed for each
risk as if it was the only risk the scheme faced; and then combining the capital
required for each risk.
More precisely, to determine the total capital required for the entire scheme: calculate
the amount of capital required for each risk element (i.e. the risk charge for each risk
element) as if it was the only risk faced by the scheme and then combine the risk
charges for all risk elements to get the total capital requirement for the scheme. When
combining the capital for the different risk elements an allowance should be made for
the covariance between the different risk elements.
For further discussion of these approaches, see Butsic (1994) and Barth (2000). Butsic
describes the expected policyholder deficit approach in great detail, while Barth gives
a very readable comparison of the two approaches.
B2. Estimating factors by simulation
In practice the RBC factors in the USA formula are estimated using stochastic
simulation. ASSA (n.d.) explains this simulation approach in some detail. What
follows is merely an introduction to the approach based on ASSA (n.d.).
In essence, stochastic simulation is used to estimate the probability of ruin for a given
initial level of surplus. The initial level of surplus is then changed until the desired
probability of ruin is achieved. That optimal level of surplus determines the RBC
factor.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 66
The following (simplified) example shows how the underwriting risk section of the
formula could be estimated. Surplus is expressed as a percentage of contributions,
making it comparable to the loss ratio. The example uses a five-year modelling
period. The table below shows the results of one simulation.
Table B4: One simulation of end of year surplus
Loss ratio
deviate
Year
0
1
2
3
4
5
5%
7%
-17%
0%
16%
Premium basis
loss ratio
60%
65%
65%
65%
72%
65%
55%
65%
55%
65%
71%
65%
Source: ASSA (n.d.)
Actual loss ratio
End of year
surplus
10%
10%
3%
13%
23%
17%
The loss ratios (claims/contributions) for each of the five years are simulated first.
This is done by adding a randomly generated loss ratio deviate to the previous year’s
loss ratio. The distribution of this deviate could be based on medical schemes’ past
experience. Then, the end of year surplus is generated. Ending surplus is the previous
year’s ending surplus, plus the premium basis loss ratio minus the actual loss ratio.
The simulation in the above table is not a ruin at the 10% initial surplus level. By
running about 1,000 such simulations, the probability of ruin at the 10% surplus level
could be estimated. If 10% surplus corresponds to the desired probability of ruin, a 0.1
risk factor may be chosen for underwriting risk. That is, 0.1 times contributions equals
base underwriting risk RBC.
B3. Solvency liability margin
Torrance (2001) explains the basis for the 10% solvency liability margin. He uses the
risk structure below to estimate the standard deviation of outstanding claims
liabilities, which he then uses to derive the 10% solvency margin.
Variation in outstanding claims liability can be separated into two components.
Systemic variation (Sv) measures the impact of environmental factors, external to
individual insurers, which affect the industry as a whole.
Independent variation (Iv) refers to the impact of random claim variations on
individual insurers. This variation usually decreases with increasing size of the
insurer.
The total variation (standard deviation) of outstanding claims is then given by:
Sv 2 Iv 2 .
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 67
Quarterly health fund data for the 19 quarters ending on 30 September 1999 were then
analysed to estimate the above risk measures. The results of this analysis are shown
below.
Systematic variation = 1.5%
Independent variation = 4.3%
Total variation = 4.5%
Based on the results of his analysis, the standard deviation of the outstanding claims
liability of an insurer of average market share was estimated at 4.5%. Since PHIAC
required a reserve of roughly two standard deviations to ensure a 2.5% probability of
ruin, a margin of 10% was adopted.
Torrance didn’t fully explain how he arrived at these results but referred the reader to
Cumpston (1992) for an explanation. Cumpston carried out a similar analysis for
general insurers and his paper gives some insight into how these risk measures are
estimated. The reader is referred to Cumpston and Torrance’s articles for the details of
this analysis.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 68
Appendix C: Method used to calculate the USA
RBC Requirement
C1. Statutory returns data used in the calculation
The following table lists exactly what statutory returns data were used in the
calculation of the USA RBC formula’s various risk charges. If there is no data next to
a particular risk charge, that risk charge was not calculated.
Table C1: Data used to estimate RBCAC
Section of US RBC formula
Factor
Statutory returns data used (data is at
31/12/2000 unless otherwise stated)
0.010
Guarantees and suretyships for third parties. See
explanation of the different types of guarantees
below.
0.003
0.010
0.020
RSA government bonds
Transnet, Post office, Eskom bonds
Water board, Land bank bonds
0.100
0.300
0.003
0.200
Local government bonds
Other bonds e.g. company bonds
Cash and cash equivalents
All other investments
0.300
0.150
All preferred stock
All equities
0.100
0.100
0.100
0.100
0.100
Land and buildings
H0 - Asset risk - affiliates
Off-Balance Sheet Items
Directly Owned Insurer Subject to RBC
Indirectly Owned Insurer Subject to RBC
Directly Owned MCO Subject to RBC
Indirectly Owned MCO Subject to RBC
Directly Owned Alien Insurer
Indirectly Owned Alien Insurers
H1 - Asset risk - other
Investment Subsidiary
Holding Company Excess of Subsidiaries
Investment in Parent
Other Affiliates
Fair Value Excess Affiliate Common Stock
Fixed Income Assets
Bonds
Category 1
Category 2
Category 3
Category 4
Category 5
Category 6
Cash
Other long term invested assets
Replication & Mandatorily Convertible Securities
Unaffiliated Preferred Stock
Unaffiliated Common Stock
Property & Equipment
Properties occupied by the company
Properties held for the production of income
Properties held for sale
Furniture and equipment
EDP equipment and software
Asset Concentration
CARE
Investment property
Office equipment and fittings
Computer equipment and software
Effect of RBC Formulae on Medical Scheme Solvency
Page 69
H2 - Underwriting risk
Net Underwriting Risk (Basis 1)
Premium
Net incurred claims
Managed care claims payments
0.090-0.150
Gross contributions less reinsurance premiums
Gross claims less reinsurance claims
Category 0
0.000
Category 1
0.150
Direct benefits paid during the year for the period
and the previous period
Managed care benefits paid during the year for
the period and the previous period
Category 2
Category 3
Category 4
Rate Guaranty - 15-36 Months
Rate Guaranty - Over 36 Months
Assessment Risk (Non-Guaranty Fund)
Stop Loss
Disability Income
Long-Term Care
Limited Benefit Plans
Premium Stabilization Reserve
H3 - Credit risk
Total Reinsurance RBC
Reinsurance recoverables
Unearned premiums
Other reserve credits
Intermediaries Credit Risk RBC
Total Other Receivables RBC
Investment income receivable
Health care receivables
0.005
0.005
Reinsurance claims recoveries outstanding
Reinsurance premiums paid in advance
0.050
Arrear contributions plus recoveries from
members for co-payments plus advance
payments on savings plan
Amounts due from affiliates
Aggregate write-ins
H4 - Business risk
Administrative Expense RBC
General administrative expenses
0.040-0.070 Administration expenditure
Non-Underwritten and Limited Risk Business RBC
Premiums Subject to Guaranty Fund Assess
Excessive Growth RBC (Basis 1)
Gross contributions less reinsurance premiums
UW risk revenue, prior year
for the year ended 31/12/1999
Gross contributions less reinsurance premiums
UW risk revenue, current year
for the year ended 31/12/2000
As for H2 above, but using data for the year
Net UW risk RBC, prior year
ended 31/12/1999
As for H2 above, using data for the year ended
Net UW risk RBC, current year
31/12/2000
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 70
C2. Treatment of the different types of guarantee
The statutory returns data distinguishes between:
Guarantees supplied by a scheme to the registrar;
Guarantees for third parties; and
Suretyships for third parties.
To calculate the USA RBC requirement, it was necessary to know if any of these
guarantees and suretyships were contingent liabilities. For the avoidance of doubt, this
question was put to the Council for Medical Schemes. The Council’s response is
reproduced below.
“Legal basis supporting the different types of guarantees:
Per section 35(6)(d) - A medical scheme shall not by means of
suretyship or any other form of personal security, whether under a
primary or accessory obligation, give security in relation to
obligations between other persons without the prior approval of the
Council or subject to such directives as the Council may issue.
Per section 24(5) - The Registrar may demand from the person who
manages the business of a medical scheme which is in the process of
being established, such financial guarantees will in the opinion of
the Council ensure the financial stability of the medical scheme
Per Regulation 2(j) - the guarantees and the guarantee deposit
vouchers as the Registrar may require
Per section 33(3) - The Registrar may demand from the principal
officer such financial guarantees as will in the opinion of the
Council ensure the financial soundness of benefit options.
Per section 44(9)(b) - at any time demand from the medical scheme
such financial guarantees and guarantee deposits as will in the
opinion of the Registrar ensure the financial stability of the medical
scheme
Per Registration and accreditation two types of guarantees are
required upon registration of a new scheme - guarantee deposit in
to the bank account of the medical scheme and a guarantee with a
recognized reputable bank
Accounting treatment of the abovementioned:
1. Suretyship or guarantee provided by the scheme to a third party
Per AC 130.28 - an enterprise should not recognize a
contingent liability
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 71
Per AC 130.87 - unless the possibility of any outflow in
settlement is remote, an enterprise should disclose the following
for each contingent liability in a note to the financial
statements:
(a) a brief description of the nature;
(b) where practicable:
a. an estimate of its financial effect,
b. an indication of the uncertainties regarding the amount
or timing, and
c. the possibility of any reimbursement.
2. Guarantee deposit provided by the scheme to the Registrar
Per AC 000.49(a) - definition of an asset is complied with and
thus form part of the bank account
3. Guarantee provided by the scheme to the Registrar with a
recognized reputable bank
Per AC 130.32,90 - Contingent assets should not be
recognized. When an inflow of economic benefits is however
probable, disclose:
(a) a brief description of the nature;
(b) an estimate of the financial effect if possible.
Therefore it depends whether it is a guarantee deposit or just a
guarantee.”
Maggie Grobler, personal communication, 8 April 2003
Based on this response, it was concluded that only the guarantees and suretyships for
third parties are contingent liabilities, which should attract a risk charge in the off
balance sheet items section of the formula.
C3. Assumptions and adjustments to the formula
Two changes were made to the USA RBC formula when applying it to South African
medical schemes.
C3.1 Premium tiers
The premium tiers in the underwriting risk charge and business risk charge were
changed from $0 - $25 million to R0 - R135 million. This was an attempt to make the
results of the calculation more relevant to the South African environment. The figure
of R135 million is the average total gross contributions over the 2000 calendar year
for a scheme with 30,000 beneficiaries. The average contribution per beneficiary per
year in 2000 was R4,516. Therefore, the average annual contribution for 30,000
members was R135.48 million. This was rounded to R135 million for use in the
premium tiers. The table below examines the sensitivity of the calculation to the size
of the tier.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 72
Table C2: Premium tier sensitivity analysis
Underwriting risk RBC
Business risk RBC
RBCAC
% of gross contributions
R100 million R135 million R200 million
2,636,065,606 2,713,030,121 2,810,098,943
267,974,426 301,928,389 345,315,385
3,267,551,759 3,338,115,241 3,430,260,399
10.9%
11.2%
11.5%
RBCAC was calculated using a R100 million tier and a R200 million tier as well as
the R135 million tier. In all three cases the results were similar.
C3.2 Alternative risk charge
The alternative risk charge was set at R1,670,000. As mentioned earlier, the
alternative risk charge should be twice the maximum after reinsurance payout on an
individual claim. The maximum individual claim payout was taken to be R835,000,
which is the average of the top ten claims paid by medical schemes administered by
Medscheme during the 2001 calendar year. The top ten claims and a description of
their causes are shown below.
Table C3: Top ten claims
Description
Malignant neoplasm of oesophagus unspecified
Aneurysm of heart
Unspecified injury of head
Unspecified appendicitis
Chronic obstructive pulmonary disease, unspecified
Fracture of first cervical vertebra
Other acute renal failure
Injury of heart
Malignant neoplasm of pancreas, unspecified
Shock, unspecified
R
1,322,358
1,019,545
893,870
844,463
796,526
751,140
714,111
707,412
687,027
601,411
RBCAC was calculated using two other alternative risk charges to check the
sensitivity of the result to the alternative risk charge assumed. The table below shows
the results of this sensitivity analysis.
Table C4: Alternative risk charge sensitivity analysis
R1 million
R1.67 million R2 million
Underwriting risk RBC
2,702,486,167 2,713,030,121 2,720,318,957
RBCAC
3,328,928,065 3,338,115,241 3,344,681,637
% of gross contributions
11.1%
11.2%
11.2%
When the RBCAC was recalculated using R1 million and R2 million alternative risk
charges, the results differed by less than 0.1% of gross contributions respectively. The
result is robust because the base underwriting risk after managed care discount is
larger than the alternative risk charge for most schemes, so the alternative risk charge
has no impact on the RBCAC of most schemes.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 73
Appendix D: Method used to calculate the
Australian Solvency Reserve
D1. Statutory returns data used in the calculation
The following table lists exactly what statutory returns data were used in the
calculation of the Australian solvency reserve. If there is no data next to a particular
risk charge, that risk charge was not calculated.
Table D1: Data used to estimate Australian solvency reserve
Section of Australian solvency standard
Solvency Liability
Solvency net claims liability
Outstanding claims liability
Reinsurance outstanding claims liability
Unexpired risk liability
Contributions in advance
Solvency reinsurance accrued liability
Solvency other liabilities
Expense reserve
Total expenses
Allowable deductions
Inadmissible assets reserve
Assets used for the conduct of business
Holdings in associated prudentially regulated institutions
Asset concentration risks
CARE
Statutory returns data used (data is at
31/12/2000 unless otherwise stated)
Provision for outstanding claims plus reported
claims not yet paid
Relates to Australian risk equalisation system
Loss ratio*contributions received in advance
where
Loss ratio = (Gross contribution income - savings
contribution income + admin expenses + managed
care: management services + broker fees) / net
claims incurred
Contributions received in advance
Relates to Australian risk equalisation system
All liabilities not mentioned above
Admin expenditure + managed care: management
services + own facility staff costs and expenses
Legal fees; actuarial fees; consultancy fees (not
the contracted administrator) + penalties +
marketing expenses
Arrear contributions, recoveries from members for
advance payments on savings plan accounts,
reinsurance premiums paid in advance, loans to
members (capital and interest), computer equipment
and software, prepayments.
All assets
Effect of RBC Formulae on Medical Scheme Solvency
Page 74
Resilience reserve
Equities
Properties
Interest bearing
Preference shares, ordinary shares, units in
equity unit trust
Land and buildings, also investments: Immovable
property, units in unit trusts that invest in property
shares, shares in property companies, debentures
of property companies.
Cash and cash equivalents, also investments:
bonds, debentures (convertible, listed & unlisted),
units in unit trusts that invest mainly in income
generating securities
Indexed bonds
Management capital
No further data needed
D2. Assumptions and adjustments to the formula
It was necessary to make the following assumptions and adjustments to the formula to
apply it to South African data.
D2.1 Asset concentration risk
The maximum permissible investment in each asset type is listed below.
100% of scheme assets for SA government bonds.
The maximum of 50% of total scheme assets and R5 million for cash and cash
equivalents.
10% of total assets for all other assets.
D2.2 Resilience reserve
The statutory returns data only record the market value of each scheme’s bond
holdings. Since the prescribed change in bond values are specified in terms of a yield
increase, it was necessary to use an approximation to convert this yield increase into a
change in bond value.
After consultation with Professor McLeod (personal communication, 10 April 2003)
the following approximations and assumptions were used. Under the assumption that
schemes, on average, hold the All Bond Index (ALBI), or other pooled bond
investments that are benchmarked against the ALBI, the volatility of the ALBI was
used to make an approximation. The proportionate increase in bond value was
estimated using the equation below.
Proportionate increase in bond value -(Yield increase) (Volatility).
This equation comes from Bodie, Kane and Marcus (1999). The table below contains
average ALBI figures for the period 1 January 2003 to 16 April 2003. These figures
and the equation above were used in calculating the resilience reserve for bonds.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 75
Table D2: Average ALBI figures
ALBI quantity
Average modified duration (years)
Average yield
Average volatility
4.64
11.05%
4.40
The results were tested for sensitivity to the assumed volatility by calculating the
solvency and capital adequacy reserves using volatility of 4.00 and 5.00 as well as the
chosen 4.40. The table below shows the results of those calculations.
Table D3: ALBI volatility sensitivity analysis
Resilience reserve
Management capital amount
Solvency reserve
As % of gross contributions
4.00
4.40
5.00
287,093,068 307,614,756 338,663,328
89,920,974
89,465,276
88,773,306
6,077,889,782 6,097,955,772 6,128,312,375
20.3%
20.4%
20.5%
Resilience reserve
Management capital amount
Capital adequacy reserve
As % of gross contributions
688,929,035 739,138,071 815,593,690
67,706,812
67,034,376
66,025,322
8,407,730,693 8,457,267,293 8,532,713,858
28.1%
28.3%
28.6%
The capital adequacy reserve is more sensitive to the volatility than the solvency
reserve as the yield changes in the resilience reserve for capital adequacy are larger
than for solvency. Both the solvency and capital adequacy reserves show little
sensitivity to the volatility figure.
The diversification factor also required approximation, being a function of the average
term to maturity for the cash and fixed interest sectors combined. At 31 December
2000, 80% of Registered schemes’ cash and fixed interest investments were in cash
and cash equivalents while the other 20% were in fixed interest investments. Using 0
years as the term of a cash investment and the average modified duration of the ALBI
(4.64 years) as the average term of the fixed interest investments, gives a weighted
average term of 0.93 years for the two sectors combined. The table below shows the
value of the solvency and capital adequacy reserves when the fixed interest terms are
0 years, 0.93 years and 4.64 years.
Table D4: Average fixed interest term sensitivity analysis
Resilience reserve
Management capital amount
Solvency reserve
As % of gross contributions
0 years
0.93 years
4.64 years
183,863,860 307,614,756 302,419,552
93,935,440
89,465,276
89,442,413
5,978,675,040 6,097,955,772 6,092,737,705
20.0%
20.4%
20.4%
Resilience reserve
Management capital amount
Capital adequacy reserve
As % of gross contributions
474,334,908 739,138,071 728,222,230
76,958,876
67,034,376
67,139,224
8,202,388,630 8,457,267,293 8,446,456,299
27.4%
28.3%
28.3%
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 76
This appears to be the most significant assumption tested so far. The solvency reserve
differs by up to 0.4% while the capital adequacy reserve differs by up to 0.9% as the
assumption varies.
D2.3 Management capital amount
The management capital amount in the solvency standard imposes a minimum
solvency reserve of $1 million on Australian private health insurers. Professor
McLeod suggested the use of a R5 million minimum when calculating the solvency
reserve for South African schemes (personal communication, April 10, 2003). This is
based on the current rules for starting a medical scheme which require schemes to
hold a minimum balance of R2.5 million in their bank account and submit a guarantee
of R2.5 million to the registrar from a reputable bank (South African Government,
1998). The table below shows the value of the solvency and capital adequacy reserves
calculated using R0, R5 million and R10 million minima.
Table D5: Management capital amount sensitivity analysis
R0
Management capital amount
Solvency reserve
As % of gross contributions
R5 million
R10 million
0
89,465,276 325,757,543
6,008,490,497 6,097,955,772 6,334,248,040
20.1%
20.4%
21.2%
Management capital amount
Capital adequacy reserve
As % of gross contributions
0
67,034,376 239,996,044
8,390,232,917 8,457,267,293 8,630,228,961
28.1%
28.3%
28.9%
The solvency reserve was estimated to be 0.8% higher when a R10 million minimum
was used, but 0.3% lower when no minimum was imposed. The capital adequacy
reserve was slightly less sensitive to the assumed minimum.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 77
Appendix E: Method used to calculate the
Australian Capital Adequacy Reserve
E1. Statutory returns data used in the calculation
The following table lists exactly what statutory returns data were used in the
calculation of the Australian capital adequacy reserve. If there is no data next to a
particular risk charge, that risk charge was not calculated.
Table E1: Data used to estimate Australian capital adequacy reserve
Section of Australian capital adequacy
standard
Capital adequacy liability
Capital adequacy margin
Capital adequacy net claims liability
Outstanding claims liability
Reinsurance outstanding claims liability
Unexpired risk liability
Contributions in advance
Capital adequacy reinsurance accrued liability
Capital adequacy other liabilities
Renewal option reserve
Contribution income
Benefit claims
Reinsurance
Administration and other expenses
Statutory returns data used
(data is at 31/12/2000 unless otherwise stated)
Monthly scheme membership for the year 2000.
See comments below.
Provision for outstanding claims plus reported
claims not yet paid
Relates to Australian risk equalisation system
Loss ratio*contributions received in advance
where
Loss ratio = (Gross contribution income - savings
contribution income + admin expenses + managed
care: management services + broker fees) / net
claims incurred
Contributions received in advance
Relates to Australian risk equalisation system
All liabilities not mentioned above
Gross contributions
Gross claims
Administration expenses; managed care
management services; broker fees; own facility
staff costs; own facility expenses.
Investment earnings rate
Taxation
Business funding reserve
Inadmissible assets reserve
Holdings in associated prudentially regulated institutions
Asset concentration risks
CARE
All assets
Effect of RBC Formulae on Medical Scheme Solvency
Page 78
Resilience reserve
Equities
Properties
Interest bearing
Preference shares, ordinary shares, units in
equity unit trust
Land and buildings, also investments: Immovable
property, units in unit trusts that invest in property
shares, shares in property companies, debentures
of property companies.
Cash and cash equivalents, also investments:
bonds, debentures (convertible, listed & unlisted),
units in unit trusts that invest mainly in income
generating securities
Indexed bonds
Management capital
No further data needed
E2. Assumptions and adjustments to the formula
It was necessary to make the following assumptions and adjustments to the formula to
apply it to South African data.
E2.1 General
The assumptions and adjustments made when calculating the solvency reserve, as
outlined in Appendix D2, were also made when calculating the capital adequacy
reserve. In particular, the management capital amount was assumed to impose a
minimum capital adequacy reserve of R5 million, as for the solvency reserve. The
sensitivity to these assumptions was tested in Appendix D2.
E2.2 Capital adequacy margin
No adjustments were made to this part of the formula but assumptions were made
when calculating each scheme’s capital adequacy margin. The base (minimum) value
for the margin was 12.5%, as in the capital adequacy standard, to which a fund size
addition, as well as a membership and claims stability addition was added.
To calculate the fund size addition it was necessary to convert each scheme’s
membership at 31 December 2000 into a number of SEU’s. Each single member is
counted as one SEU while all other members (married etc) are counted as two SEU’s.
The marital status of each member was not in the data set so each member was
counted as 1.5 SEU’s. This is equivalent to assuming that half the members are single.
In evaluating the sensitivity of the results to this assumption, the results were
recalculated twice: firstly, counting each member as one SEU and secondly, counting
each member as two SEU’s i.e. assuming that all members are single and that no
members are single. The table below shows the results of those calculations.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 79
Table E2: SEU assumption sensitivity analysis
1 SEU
1.5 SEU's
2 SEU's
6,992,142,508 6,973,342,207 6,961,142,269
4,710,916,700 4,551,783,444 4,453,753,786
750,349,550 739,138,071 731,335,295
65,967,513
67,034,376
67,709,337
8,645,345,466 8,457,267,293 8,339,909,881
28.9%
28.3%
27.9%
Capital adequacy liability
Renewal option reserve
Resilience reserve
Management capital amount
Capital adequacy reserve
As % of gross contributions
Assuming one SEU gives the largest capital adequacy reserve while assuming two
SEU’s gives the minimum reserve. The capital adequacy reserve changes by about
0.5% of gross contributions as the assumption is changed.
No data on claims stability was available, but monthly membership for the year 2000
was included in the schemes’ 2000 returns. For each scheme the coefficient of
variation of its monthly membership was calculated and used to determine its
membership stability addition. The histogram below shows the distribution of those
coefficients of variation.
40
120%
Frequency
Cumulative %
35
100%
30
80%
Frequency
25
60%
20
15
40%
10
20%
5
0
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
10%
20%
30%
0%
More
Membership coefficient of variation
Figure E1: Histogram of membership coefficients of variation
Based on this diagram, it was decided to structure the membership variability addition
in the following way.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 80
Table E3: Membership and claims stability addition
Membership coefficient of variation (CV)
Additional margin
Less than 1%
Less than 20% but greater than 1%
Greater than 20%
0%
5%*(CV-0.01)/0.19
5%
Using the histogram to interpret this margin structure, one can see that the 20% of
schemes with the lowest CV get a 0% a margin, while the 10% of schemes with the
highest coefficient of variation get a 5% margin. The margin is allocated linearly
between these two extremes. Figure 4.8 is a histogram of the resulting capital
adequacy margins. The table below shows the results of using different methods to
deal with the stability addition: either setting it to 0.0%, 2.5% or 5.0% for all schemes
or using the coefficient of variation method described above.
Table E4: Stability addition sensitivity analysis
0.0%
Capital adequacy liability
Renewal option reserve
Resilience reserve
Management capital amount
Capital adequacy reserve
As % of gross contributions
6,946,022,061
4,364,702,554
726,161,330
70,532,571
8,233,387,711
27.6%
Coefficient of
2.5%
5.0%
variation
6,973,342,207 7,028,857,670 7,111,732,569
4,551,783,444 5,011,696,580 5,685,330,876
739,138,071 772,013,178 818,937,285
67,034,376
62,830,681
55,950,059
8,457,267,293 9,001,367,305 9,797,919,984
28.3%
30.1%
32.8%
Overall, the coefficient of variation method produces results which are a mixture of
the 0% and 2.5% approaches. However, it assigns a higher margin to schemes with
more membership variability (typically the open schemes) than to schemes with less
variability.
E2.3 Renewal option reserve
The basis used to calculate the renewal option reserve is taken from Torrance (2001,
p.42). Torrance was the lead consultant on the development of the standards. He used
this basis to approximate the renewal option reserve for the Australian private health
insurance industry using only past data.
Torrance assumed that:
Next years claims are expected to be the same as this year’s claims.
Next years contributions are expected to be the same as this year’s contributions.
Torrance’s basis ignores investment earnings. The author chose to allow for
investment earnings in the calculations in this report.
This made it necessary to make an assumption about the incidence of cash flows over
the year following the valuation date. It was assumed that all cash flows occur
halfway through the year. The table below shows how the results would differ if cash
flows were assumed to occur at the beginning and at the end of the year.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 81
Table E5: Cash flow incidence sensitivity analysis
Renewal option reserve
Resilience reserve
Management capital amount
Capital adequacy reserve
As % of gross contributions
Beginning
Middle
End
4,775,035,616 4,551,783,444 4,338,969,211
753,740,365
739,138,071 725,218,493
65,499,093
67,034,376
68,656,895
8,693,586,477 8,457,267,293 8,232,156,002
29.1%
28.3%
27.5%
The capital adequacy reserve differs by 0.8% either way if the cash flows are assumed
to occur at the beginning or end of the year instead of the middle.
In addition, the renewal option reserve uses the one-year yield on Commonwealth
Government Treasury Bonds at the start of the date of the projection, less 1% as the
rate of investment earnings. The yield on these bonds at 18 April 2003 was 4.64%. It
is pure coincidence that this yield looks so similar to the average modified duration on
the ALBI. The yield, and other information, on these bonds was found at the website
of Macquarie Bank Limited. However, for consistency with the assumptions made in
the resilience reserve and relevance to South African medical schemes, the average
yield on the ALBI (11.05% per annum, see Table D2) was used as the rate of
investment earnings. The table below shows the value of the capital adequacy reserve
for the two different rates of investment return.
Table E6: Investment return sensitivty analysis
Renewal option reserve
Resilience reserve
Management capital amount
Capital adequacy reserve
As % of gross contributions
4.64%
11.05%
4,712,422,307 4,551,783,444
750,202,725
739,138,071
65,817,221
67,034,376
8,627,753,655 8,457,267,293
28.9%
28.3%
The capital adequacy reserve is 0.6% higher when the lower 4.64% investment return
is used.
CARE
Effect of RBC Formulae on Medical Scheme Solvency
Page 82