SHOCK & ASSESSMENT OF BURNS

SHOCK & ASSESSMENT OF BURNS
2
Lecture outline
This lecture deals about the Shock & Assessment of Burns;
1. Shock & its different forms
2. Burn assessment & its different forms
Lecture Objective
At the end of this lecture the students will be able to;
Define shock & explain the different types of shock.
Perform different types of burn assessment in a patient
SHOCK
The inability of the circulatory system to meet the needs of tissues for oxygen and nutrients and the removal of their metabolites' (Dietzman and Lillehei 1968; cited by Settle 1986).
Shock can last for 2-3 days, and longer in the elderly.
Within minutes of the burn being sustained, oedema gathers beneath the damaged areas, a result of increased capillary permeability of the affected tissues.
There is loss of protein and electrolytes from the blood.
PHYSIOLOGICAL CHANGES DUE TO SHOCK
Reduced plasma volume – hypovolemia
Increased ratio of red blood cells to plasma in the blood vessels resulting in increased blood viscosity and slowing of the circulation
Reduction of cardiac output
Increased heart rate.
During this stage the main dangers are from pulmonary edema, occlusion of arteries, cardiac failure, renal failure, liver failure, and permanent brain and vital organ damage
TYPES OF SHOCK
The cardiogenic shock:-
The cardiogenic shock is the inability of the heart to destined and fill before ejection.
Neurogenic shock:-
A primary shock caused by loss or decrease of the vascular tone = or due to decrease of the blood pressure via the increase of the vagal tone.
The secondary shock or the hypovolemic shock:-
It is the shock which is caused by the loss of the circulating blood volume , may occur with the loss of the whole blood or the loss of plasma as in cases of serious burn injuries.
TYPES OF SHOCK – Cont….
Septic shock:-
Acute or chronic bacterial inflammation as acute pyenephritis or pancreatitis lead to massive inflammation —> toxemia —> fever and fall in the vascular tone (peripheral resistance) via peripheral vasodilatation -> pooling of the blood —> decrease venous return —> decrease cardiac output -> fall of B.P -> syncope.
Clinical features of hypovolemic shock : are Apathy, Pallor, cyanosis, Sweating, tachycardia, hypertension, Shallow respiration,
Thirst, vomiting, subnormal temperature.
DURING SHOCK (UP TO 3 DAYS POST-BURN)
Restlessness and disorientation.
Coldness and paleness of the skin.
Collapsed veins and rapid pulse.
Sweating.
Thirst.
Hypotension.
Tachycardia.
Rapid breathing - later becoming gasping.
Cyanosis.
POST-SHOCK PHASE
Separation of the burned skin (eschar).
Formation of scar tissue.
Contraction of scar tissue, causing
(a) pain due to traction of the sensory nerve endings;
(b) limitation of joint movement;
(c) joint deformities;
(d) loss of function
Burn extent
% BSA involved morbidity
Burn extent is calculated only on individuals with second and third degree burns
Palmar surface = 1% of the BSA
Measurement charts
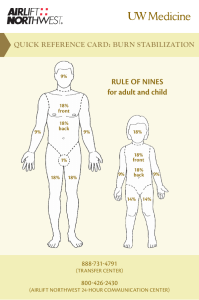
Rule of Nines:
Quick estimate of percent of burn
Lund and Browder:
More accurate assessment tool
Useful chart for children – takes into account the head size proportion.
Rule of Palms:
Good for estimating small patches of burn wound
Initial Depth Assessment
Assess depth of injuries:
Third degree (full thickness)
full thickness injury extending through all layers into subcutaneous fat
typically requires some degree of surgical closure
Fourth degree
third degree with extension into bone/joint/muscle
Note circumferential burns, compartment syndrome risk; consider escharotomy need.
Initial Management: Extent
Expressed as percentage of total BSA
Only 2 nd & 3 rd degree burns mapped
Once adult proportions attained (~15 yo), “rule of nines” may be used
For children less than 15 years of age, age adjusted proportions must be used
fluid replacement is based upon BSA estimates
Must rule out concomitant other injuries
RULE OF NINE
A method for gauging the total body surface area
*(Extend of burn injury)* is 'the rule of nines'.
This rule divides the body surface into 11 areas, each constituting 9% of the total . The perineum is counted as 1%.
Anatomic structure
Adult
Surface area
Anterior head 4.5%
Posterior head
Anterior torso
Posterior torso
Anterior leg , each
Posterior leg, each
Anterior arm , each
4.5%
18%
18%
9%
9%
4.5%
Posterior arm, each 4.5%
Genitalia / perineum 1%
Anterior head
Anatomic structure
Posterior head
Anterior torso
Posterior torso
Anterior leg, each
Posterior leg, each
Anterior arm, each
Posterior arm, each
Genitalia/perineum
Child
Surface area
9%
9%
18%
18%
6.75%
6.75%
4.5%
4.5%
1%
Assessing TBSA - Rule of Nines
This method divides the body into areas each of which equates to 9% of the total body surface area:
the whole of one arm (anterior and posterior surfaces including the hand) is 9%, therefore 2 arms
= 18%
the entire head including face, scalp and neck is 9%
anterior trunk is 18%
posterior trunk including buttocks is 18%
the whole lower limb (anterior and posterior surfaces, including the thigh, leg and foot) is 18%; therefore both lower limbs = 36%.
This totals 99% with the perineum making the final 1%.
Beware: this method is unreliable in young children.
Assessing TBSA in children
Why might the “rule of
9’s” be unreliable in children?
Body proportions change with age. In a child, the head represents a much greater proportion of the total body surface area.
Assessing TBSA - Lund and Browder charts
These take account of the patient’s age and provide a more detailed mapping system for the burnt area
AREA
A = ½ OF HEAD
B = ½ OF ONE THIGH
C = ½ OF ONE LEG
AGE 0
9 ½
2 ¾
2 ½
1
8 ½
3 ¼
2 ½
5
6 ½
4
2 ¾
10
5 ½
4 ½
3
15
4 ½
4 ½
3 ¼
ADULT
3 ½
4 ¾
3 ½
Burn Classification –
Extent Lund & Browder
Lund and Browder
More accurate
Divides body into small areas
Estimates proportion each area contributes
Takes more time and effort to calculate than Rule of Nines method
Burn Assessment Lund & Browder Chart
Assessing TBSA - Palm size
Another useful way, especially for small burns is to use the palm of the patient’s hand (with fingers extended). This equates to approximately 1% of the body surface area.
Assessing TBSA - Unburnt area
In very large burns, it is often easier to measure the area of skin that is unburnt and then subtract this from 100%.
Area of the body involved
Not only is the surface area or size of burn important, but also the specific part of the body affected
Eyes: Burns to the eyes (especially chemical) can cause blindness.
Feet: Mobility problems
Face: Facial oedema can lead to airway obstruction. Scarring can cause significant psychosocial problems
Perineum: problems with urogenital function and psychosexual
Hands: Problems with feeding and hygiene
Circumferential burns of the limbs can cause distal ischaemia; of the chest, can compromise breathing
American Burn Association severity classification[36]
Minor Moderate
Adult <10% TBSA Adult 10–20% TBSA
Young or old < 5% TBSA
<2% full thickness burn
Young or old 5–10% TBSA
2–5% full thickness burn
High voltage injury
Possible inhalation injury
Major
Adult >20% TBSA
Young or old >10% TBSA
>5% full thickness burn
High voltage burn
Known inhalation injury
Circumferential burn
Other health problems
Significant burn to face, joints, hands or feet
Associated injuries
PROGNOSIS OF BURNS PATIENT
•
AGE:
Burns in people aged over 60 years or under 5 years carry a poor Prognosis.
TOTAL BURN SURFACE AREA (TBSA)
The greater the total burn surface area, the poorer the prognosis.
A formula for gauging outcome is:
PERCENTAGE CHANCE OF SURVIVAL = [100 - (AGE IN YEARS +
PERCENTAGE TBSA)].
For example, a 60-year-old with 30% TBSA has a 10% chance of survival
[100 - (60 + 30)].
A 20-year-old with the same TBSA has a chance of survival of [100 - (20 +
30)], or 50%