Staphylococcus
advertisement

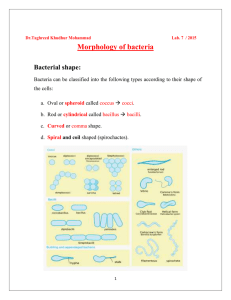
Staphyloccocci - derived from Greek “staphyl” (bunch of grapes) Gram positive cocci arranged in clusters but some, especially when examined in pathological specimens, may occur as single cells or pairs of cells. Include a major human pathogen and skin commensals Non motile Non spore forming Usually non-capsulate 32 species Catalase- positive distinguishing them from the genus streptococcus wich are catalsenegative Oxidase- negative 4 Staphylococcus species are generally nonfastidious They grow well on media without blood or other special supplements the genus Staphylococcus was separated from Micrococcus .differentiated the two genera depends mainly on the basis of their action on gelatin and on relation to their hosts. Staphylococci liquefied gelatin whereas micrococci were variable in their action on gelatin . The genera Staphylococcus, Micrococcus and Planococcus, containing Gram-positive, catalase-positive cocci, were later placed in the family Micrococcaceae Staphylococci are tolerate a high salt concentrations; they grow on media containing 5%-7.5% NaCl (e.g. Mannitol Salt Agar) pathogenic Staphylococci are commonly identified by their ability to produce coagulase, and thus clot. Staphylococcus aureus a major pathogen of increasing importance due to the rise its antibiotic resistance. Rothia can be differentiated from Staphylococcus and Micrococcus by its lack of growth on a high-salt medium, its negative catalase reaction, and its tendency to adhere firmly to an agar surface. Catalase POS Staphylococcus Catalase NEG Gram Positive Coccus Catalase + Salt Tolerant Yes Facultative Yes Staphylococcus No Rothia No Micrococcus _ Streptococcus Group Gram-positive spherical cells (0.5-1.5 mm) in singles, pairs, and clusters Appear as “bunches of grapes” Gram-stained smear of staphylococci from colony Scanning electron micrograph of staphylococci The genus Staphylococcus includes 3 species of medical importance; staph. aureus, staph.epidermidis and staph. Saprophyticus. Of the three, staph. aureus is the most important. Staph.aureus is distinguished from the others by being coagulase positive, manitol positive and by causing haemolysis of RBCs in vitro. Staph epidermidis and staph. Saprophyticus are coagulase negative and are usually commensals. However, they are considered to be potentially pathogenic. Nonmotile Non–spore-forming Nonencapsulated Catalase-producing Oxidase: negative Glucose fermenters Primarily aerobic, some facultatively anaerobic Bacitracin resistant Grow on agar that contains peptone Inhibited by media that has high bile salt concentration Some are ß-hemolytic Colony morphology: buttery looking, cream or white colored 1. Staphylococcus aureus 2. Coagulase positive Staphylococci Coagulase negative Staphylococci Staphylococcus epidermidis Staphylococcus saprophyticus Major human pathogen Habitat - part of normal flora in some humans and animals Source of organism - can be infected human host, carrier, fomite or environment Staph. aureus causes pyogenic infections which can be hospital acquired, food poisoning and toxic shock syndrome. Impetigo is a contagious superficial pyoderma, caused by Staphylococcus aureus and/or group A Differential Characteristics S. aureus Coagulase Fibrinogen Fibrin 1) All Staph group organisms that grow in air are catalase positive Rothia is catalase negative (or weakly positive). 2) Coagulase testi) Slide coagulase test- Positive. ii) Tube coagulase test- Positive. SLIDE COAGULASE TEST TUBE COAGULASE TEST Staphylococcus aureus Coagulase POS Coagulase NEG 3) Reduces nitrate to nitrite. 4) Ferments mannitol anaerobically with acid only. 5) Urea hydrolysis test- Positive. 6) Gelatin liquefaction test- Positive. 7) Produces Lipase. 8) Produces Phosphatase. 9) Produces Thermostable nuclease. Some virulence factor of Staphylococcus aureus A) CELL ASSOCIATED FACTORS: CELL WALL POLYMERS 1. Cell wall polysaccharide inhibits inflammatory response; endotoxin-like activity 2. Teichoic acid: Phage adsorption; reservior of bound divalent action 3. Capsular polysaccharide b) CELL SURFACE PROTEINS: 1. Protein A: reacts with Fsregion of Ig G 2. Clumping factor: binds to fibrinogen Structure of Staphylococcal cell wall B) EXTRACELLULAR FACTORS a) Enzymes b) Toxins a) Enzymes: 1. Free coagulase: converts fibrinogen to fibrin in plasma 2. Catalase 3. Lipase: degrades lipid 4. Hyaluronidase 5. DNAase: degrades DNA 6. Thermonuclease 7. Staphylokinase: degrades fibrin (Fibrinolysin) 8. Phosphatase b) Toxins: 1. Cytolytic toxins i) Haemolysins Alpha haemolysin Beta haemolysin Gamma haemolysin ii) Leucocidin (PantonValentine toxin) Impairment of membrane permeability; cytotoxic effects on phagocytic and tissue cells Staphylococcus toxins 1. Enterotoxin: commonly produced by up to 65% of S.aureus, these toxic proteins withstand Exposure to 100c for several minutes. When ingested as performed toxins in contaminated food microgam amount of toxin can induce within a few hours the symptoms of staphylococcal food poisoning: nausea, vomiting and diarrhoea. Resolves on its own within about 24 hours . 2. Toxic shock syndrome toxin (TSST): discovered in the early of 1980s, a multysystem disease caused by staphylococcal TSST-1. the absence of circulating antibodies to SST-1 is a factor in the pathogenesis of this syndrome Toxic shock syndrome: High fever, diarrhoea, shock and erythematous skin rash which desquamate Mediated via ‘toxic shock syndrome toxin’ 10% mortality rate Described in two groups of patients With young women using tampones during menstruation Described in young children and men 3. Exfoliative (epidermolytic toxin): the most dramati manifestation of epidermolytic toxin is Scalded skin syndrom where the toxin speeds systematically in individuals who lack neutrolizing antitoxin: extensive areas of skin are affected, wich after the development of painful rash, slough off; the skin surface resembles scalding. Such blistering lesions are seen mainly, but not exlusively, in small children. Disease of young children Mediated through minor Staphylococcal infection by ‘epidermolytic toxin’ producing strains Mild erythema and blistering of skin followed by shedding of sheets of epidermis Children are otherwise healthy and most eventually recover PATHOGENICITY: Source of infection: A) Exogenous: patients or carriers B) Endogenous: From colonized site Staphylococci do not grow outside the body except occationally in moist nutrient materials such as meat, milk and dirty water, and it is important to remember that the body surfaces of human beings and animals are the main reservoir. Although not spore forming, they may remain alive in a dormant state for several months when dried in pus, sputum, bed clothes or dust Mode of transmission: A) Contact: direct or indirect ( through fomites) B) Inhalation of air borne droplets Disease: Diseases produced by Staphylococcus aureus is studied under 2 groups: A) Infections B) Intoxications A) INFECTIONS: Mechanism of pathogenesis: Cocci gain access to damaged skin, mucosal or tissue site Colonize by adhering to cells or extracellular matrix Evade the host defense mechanisms and multiply Cause tissue damage Common Staphylococcal infections are: 1) Skin and soft tissue: Folliculitis, furuncle (boil), carbuncle, styes, abscess, wound infections, impetigo, paronychia and less often cellulitis. Folliculitis Folliculitis Furuncle (boil) Carbuncle Styes Abscess Impetigo Wound infection Paronychia Cellulitis 2) Musculoskeletal: Osteomyelitis, arthritis, bursitis, pyomyositis. osteomyelitis 3) Respiratory: Tonsillitis, pharyngitis, sinusitis, otitis, bronchopneumonia, lung abscess, empyema, rarely pneumonia. 4) Central nervous system: Abscess, meningitis, intracranial thrombophlebitis. 5) Endovascular: Bacteremia, septicemia, pyemia, endocarditis. Endocarditis 6) Urinary: Urinary tract infection. 1. In all pus forming lesions Gram stain and culture of pus 2. In all systemic infections Blood culture 3. In infections of other tissues Culture of relevant tissue or exudate 4. Faeces or vomit from patients with suspected food poisoning or remains of implicated food. 5. Blood from patients with suspected cystitis or pyelonephritis Staphylococci are inherntly sensitive to many antimicrobial agents, but 90% of strains found in hospitals are now resistant. Resistance of pencillin depends on production of the enzyme pencillinase. Antibiotic resistance can arise by various mechanisms. MRSA strains are an increasing infection control problome and therapeutic challenge. These strains, wich are resistant to all β- lactam agents, commonly colonize broken skin, but cause the full range of staphyolococcal infections. MRSA not a hospital pathogens with multiresistance , it also become more common in the community. Glycopeptides (Vancomycin or Teicoplanin) are the agents of choice in the treatment of systemmic infection. They are commonly found on the surface of healthy persons in whom they are rarely the cause of infection. More than 30 species are recognized, but few are commonly incriminated in human infection. Staph. epidermidis accounts for about 75% of all clinical isolates, probably reflecting its preponderance in the normal skin flora. Staph. epidermidis Staph. Haemolyticus Staph. Saprophyticus Staph.hominis Staph. capitis Opportunistic pathogens, often colonize biomedical device such as protheses, implants and intravascular lines, they cause particular probloms in Cardiac surgery Continuous ambolatory peritoneal dialysis Immunocompromised patients Skin commensal heart valves, Causes urinary tract infection in cathetarised patients Skin commensal Imp. Cause of UTI in sexually active young women Usually sensitive to wide range of antibiotics