pregnancy hypertension
advertisement

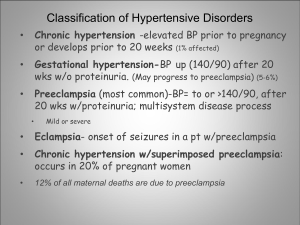
Pregnancy-induced Hypertension syndrome (Hypertensive disorders complicating pregnancy) Professor of obstetrics and gynecology Lin Qi De Term : PIHs is an acute or specific hypertension of pregnancy which is peculiar to pregnant or puerperal women .Diagnosis of PIHs is made on the basis of development of hypertension with or without proteinuria ,edema ,or both after the twentieth week of gestation ,although the signs and symptoms may appear earlier with hydatidiform moles . Classification : 1. Mild : Bp ≥140/90mmHg or Bp has a rise of 30mmHg systolic pressure or 15 mmHg diastolic pressure (4/2 Kpa ) over the prepregnant level,with or without trace proteinuria or edema. (= 1. gestational hypertension) 2. Moderate :Bp <160/110 mmHg (<21.3/14.6 Kpa ) ,with proteinuria “+” or edema . (= 2. preeclampsia/mild) 3. Severe : Bp ≥160/110 mmHg (21.3/14.6Kpa), with proteinuria “++” or edema . (= 2. preeclampsia/severe) (1) preeclampsia : above-described signs with headache ,visual disturbances and tightness of chest.(= 2. preeclampsia/severe) (2) Eclampsia : the signs and symptoms of pre-eclampsia with convulsion . (= 3. eclampsia) Etiology : 1. Utero-placental ischaemia : Abnormal development of the placental bed vessels / shallow trophoblast invision in spiral arteries / acute arterosis / 2. Endothelial cell activation/dysfunction: Cytotoxic factors : oxygen free raicals /lipid peroxidation / very low density lipoprotein(VLDL) /fibronection / platelet derived growth factor( PDGF) / tumor necrosis factor-a (TNF-a) /interleukins-6 (IL-6) / anti-vascular endothelial factor /endothelial inhibitive factor 3. Immunity ; (1) fail to express HLA-G mRNA or protein . (2) abnormal maternal immune situation such as Ts/Th decrease and Th1 function dominent . 4. Genetics : gene recessive trait . Pathophysiology : Basic pathophysiology changes : spasm of the arterioles --activation/damage of endothelium ---reduced organ perfusion :Hypertension / Proteinuria / Edema Pathology : hemorrhage /ischemia /necrosis/ 1. Placenta : (1) premature aging of villi (2) hemorrhage (3) necrosis 2. Kidney ----glomerular changes (1) swelling of endothelial cells (2) the deposition of amorphous materials in cytoplasm produce enlargement (3) swelling of the glomerular capillarities. 3. Liver : periportal areas 4. Brain :cortical /subcortical areas 5. Heart :increase of cardiac afterload , prelod may or . 6. Hematological changes: hypercoagulation status, HELLP(hemolysis, elevated liver enzymes,low count platelets) Clinical finding : (1) Hypertension is the most significant primary sign of PIHs. (2) Proteinuria is a very common finding in preeclampsia (3) Edema is a common first sign of impending or actual preeclampsia . classified into 4 degrees : Degree 1 : edema involves in shanks 2 : edema involve in thighs 3 : edema involves in vulva and abdomen 4 : edema involves face and fingers (4) Headache (5) Visual disturbances (6) The tightness of chest (7) Convulsion Diagnosis : 1. hypertension , with generalized edema or proteinuria or both . 2. Other than general physical examination : (1) check blood pressure repeatedly (2) opthalmoscopic examination (3) daily check body weight . (4) test tendon reflex. (5) monitor the obstetric condition (6) urinary examination (7) blood examination :hematocrit /hemoglobin / blood coagulation /electrolyes/ blood PH (8) determine of function of liver and kidney Treatment : 1. bed rest : 2. Sedation : (1) mild cases : phenobarbital 30-60mg tid p.o. or valium 2.5-5mg tid p.o. (2) moderate or severe cases : 250mg Phenobarbital given i.m. q6 hours ,or Valium 5mg i.v .or 10mg i.m. (3) eclamptogenic convulsion : Artificial hibernation mixture(Wintermin 50mg ,Phenergan 50mg ,Dolantin 100mg ) in 500ml of 5% glucose ivgtt. In emergency case ,1/3 dose of the mixture in 20ml of 25% glucose i.v. and 2/3 dose of it ivgtt. 3: Anti-convulsant –first choice :magnesium sulfate: contraindication as follow : (1) absent or very sluggish knee jerk (2) a respiratory rate below 16/min (3) a urinary output of less than 100ml in the preceding 4 hours (25ml/hr) 10ml vial of 10% calcium gluconate solution is necessary . Routes for giving magnesium sulfate : (1) Intravenous : (2) Intramuscular : 4. Termination of pregnancy : indication as follow : (1) severe case of PIHs or preeclampsia patient has no response following medical management for 24-48 hours .At same time she is at 36 weeks or more of gestation or she is before 36 weeks of gestation with impaired fetoplacental unit function and the L/S ratio is 2.0 or more or she is deteriorating despite of aggressive treatment . (2) In women with seizures ,when convulsion or coma is absent for a period of 6 ~12 hrs ,delivery by elective cesarean section may be considered . Methods of terminating pregnancy : (1) Induction of labor and vaginal delivery . (2) Cesarean section 5. Others : (1) Antihypertensive drugs :Hydralazine/Nifedipin /Methyldopa/ sodium nitroprusside the indication for its use : diastolic blood pressure≥ 120 mmHg or MAP ≥ 140 mmHg (2) Diuretics :generalized edema /cardiac failure /pulmonary edema / cerebral edema the indication for its use : generalized edema /cardiac failure /pulmonary edema/ cerebral edema Lasix 20-40mg i.v. 20% Mannitol 250 ml ivgtt. (in 30-60 min ) (3) plasma expanders : 5% glucose /plasma substitutes (dextran)/ whole blood /plasma /albumin the indication for its use : hematoconcentration / hypovolumia concrete index : Hemotocrit (HT)≥ 0.35 , blood viscosity odds ≥ 3.6 , plasma viscosity odds≥ 1.6 , uric specific gravity> 1.020 Prediction: 1. roll over test: increase of >20mmHg of distolic BP from left lateral position turn to supine position 2. MAP(mean arterial blood pressure): >85mmHg during 20-28 weeks of gestation. 3. Urinary calcium excretion:urinary calcium / blood creatinine ratio>0.04