Constriction of Human Umbillcal Arteries: Interaction between Oxygen and
Bradykinin
L. G. ELTHERINGTON, J. STOFF, T. HUGHES and KENNETH L. MELMON
Circ. Res. 1968;22;747-752
Circulation Research is published by the American Heart Association. 7272 Greenville Avenue, Dallas,
TX 72514
Copyright © 1968 American Heart Association. All rights reserved. Print ISSN: 0009-7330. Online ISSN:
1524-4571
The online version of this article, along with updated information and services, is located
on the World Wide Web at:
http://circres.ahajournals.org
Subscriptions: Information about subscribing to Circulation Research is online at
http://circres.ahajournals.org/subsriptions/
Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, 351 West Camden Street,
Baltimore, MD 21202-2436. Phone 410-5280-4050. Fax: 410-528-8550. Email:
journalpermissions@lww.com
Reprints: Information about reprints can be found online at
http://www.lww.com/static/html/reprints.html
Downloaded from circres.ahajournals.org at IOWA STATE UNIV on January 17, 2007
Constriction of Human Umbilical Arteries
INTERACTION BETWEEN OXYGEN AND BRADYKININ
By L. G. Eltherington, M.D., Ph.D., J. Stoff, B.S.,
T. Hughes, M.B., Ch.B., and Kenneth L. Melmon, M.D.
ABSTRACT
Experiments on perfused segments or isolated rings of human umbilical
artery showed that the magnitude of their contraction in response to bradykinin,
epinephrine, or serotonin depended on the P02 of the perfusing or bathing
solution. Constriction to bradykinin varied directly with the O2 tension and
was greatest when the Po2 was approximately that of umbilical arterial blood
during the transition from the fetal to the neonatal period. Catecholamine
beta-receptors were not demonstrated (not present or not functional) in the
umbilical artery, since there was no vascular response to either isoproterenol or
to propranolol. Alpha-receptors were not required for O2 or bradykinin constriction since these agents constricted the umbilical artery after enough
phentolamine had been given to block constriction by norepinephrine. Because
of the interaction between Oo and vasoconstrictor agents the O2 environment
of umbilical vessels must be rigidly controlled in experiments measuring
vascular reactivity. Sensitization by O2 to the effects of chemical substances
endogenous to the fetus or mother may play an important role in circulatory
adjustments essential for neonatal life.
ADDITIONAL KEY WORDS
beta-receptors
plethysmograpb
epinephrine
• Among the essential adjustments to extrauterine life are constriction of the ductus arteriosus and umbilical vessels and dilation of
pulmonary arterioles. Mechanical alterations
in the vessels and elevation of the oxygen tension (Po2) of arterial blood have been
thought to bring about the changes in the
pulmonary circulation of newborn lambs (1),
but these two factors are not sufficient to account for the total responses in the umbilical
vessels and the ductus arteriosus. For example, umbilical vessels of lambs are not constricted by oxygen in vivo (2). Attempts
have been made to discover possible mechanisms that would explain the circulatory
From the Departments of Medicine and Pharmacology, Division of Clinical Pharmacology, and the
Cardiovascular Research Institute, University of California San Francisco Medical Center, San Francisco,
California 94122.
This study was supported in part by U. S. Public
Health Service Research Grants HE-06285 and HE09964 from the National Heart Institute.
Accepted for publication April 15, 1968.
Orcidmion Risttrch, Vol. XXII, )mu 1968
oxygen sensitization
alpha-receptors
histamine
serotonin
perfusion
changes occurring at birth. With the exception
of histamine, vasoactive amines known to exist
in the fetus do not have pharmacologic properties which mimic the effects of birth on all
vessels critical to circulatory adaptation of
the newborn. Therefore a single substance
cannot account for all the vascular changes
measured at birth. Furthermore, reports that
summarize data on humoral mediators of
neonatal circulatory changes contain no information relating the release or action of
vasoactive substances, including polypeptides,
to either the circulatory changes at birth or
to the increase in the Po2 of arterial
blood (3, 4).
Bradykinin, a potent endogenous vasodilator in man (5), dilates the pulmonary arterioles of fetal lambs (6, 7); constricts the
ductus arteriosus of lambs, calves, and guinea
pigs (8); and constricts human umbilical
cord arteries (9). Because oxygen and bradykinin act qualitatively the same on the fetal
blood vessels that are affected most in the
747
748
ELTHERINGTON, STOFF, HUGHES, MELMON
TO RECORDER
PRESSURE
TRANSDUCERS
OUTFLOW
GAS M/X/A/6
RESERVO/RS
TO VACUUM PUMP
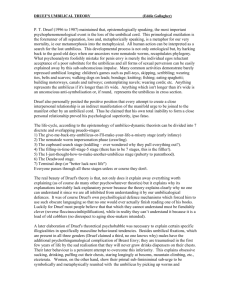
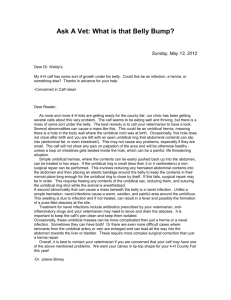
Apparatus used for perfusion of isolated umbilical cord segments. The reservoir bottles permit
changing the Pot of the perfusing solution while maintaining a constant Pcot. The vacuum
pump is used to apply a sudden increase in transmural pressure and hence to test the viability
of the preparation by its ability to contract when the artery is stretched. When a drug was
infused (rather than injected) a 30-cm length of tubing connected its pump to the T-tube.
circulatory adjustments of birth, we have
measured and evaluated the in-vitro relationships between oxygen and bradyldnin on human umbilical cord vessels. The results show
that (1) bradyldnin or oxygen elicits vasoconstricrion of human umbilical arteries and
that the response is directly proportional to
the Pou of the tissue bath or arterial perfusate; (2) of three drugs tested, bradykinin
(on either a milligram or molar basis) is the
most potent constrictor drug; and (3) the
oxygen and bradykinin receptor(s) of the
umbilical arteries may be identical and differ
from those for epinephrine and serotonin.
Such results provide the basis for studies to
determine whether bradykinin may be one of
the mediators of circulatory changes in the
fetal-neonatal period.
Methods
PERFUSION STUDIES
Eighty-seven human umbilical cords were
used within 3 hours of full-term vaginal delivery.
A 15-cm segment, free of gross irregularities, was
cut from the middle-to-placental portion of the
cord. This particular section of cord was used
because it is said to be nerve free (10). One ar-
tery was cannulated at each end and placed in a
glass plethysmograph (Fig. 1) filled with fluid.
This fluid and that used for perfusion of the artery
were a modified Krebs bicarbonate solution that
contained electrolytes in concentrations found by
Newman (11) to approximate most closely those
in maternal plasma during the third trimester. The
solution was composed of (in mEq/liter) Na + ,
139.5; K+, 3.97; Ca2 + , 4.69; Mg11 + , 1.47;
HCCV, 23.2; C1-, 104.2; and HPO4, 1.82. The
Vo2 of the plethysmograph solution was that of
room air and remained stable (by measurement)
throughout the perfusion period. The carbon
dioxide tension (Pco 2 ) of the solution was not
measured nor was any attempt made to keep this
constant. The inflow cannula to the arterial segment was connected to a constant-flow Sigma
motor pump; the outflow was discarded. Flow
was always in the direction of fetus to placenta.
The Pco2 of the perfusion solution (bubbled with
7% CO2) was measured with a Severinghaus electrode and ranged from 49.3 to 56.7 mm Hg. The
Po 2 of the fluid in the reservoirs varied from 15 to
approximately 720 mm Hg; it was monitored with
a Clark electrode. The temperature and pH of the
perfusion solution varied between 36.5 and
37.5°C and 7.17 and 7.24 respectively, approximating values reported in human umbilical artery blood (12). Inflow pressure to the cannulated artery was measured with a Statham pressure
transducer. Attachment of a vacuum pump to
CirctdMum Research, Vol. XXII, Jvtu 1968
SENSITIZATION OF UMBILICAL VESSELS BY OXYGEN
one of the tvvo side arms of the plethysmograph
allowed rapid and reproducible distention of the
arterial segment (9, 13). The amount of subatmospheric pressure necessary to produce a consistent vascular constriction varied from one
TO ISOTONIC TRANSDUCER
SOLUTION OUTFLOW
R/NGS OF UMBILICAL
ARTERY OR VEIN
GAS INFLOW
SOLUTION INFLOW
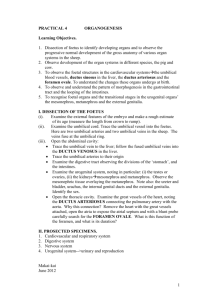
FIGURE 2
Apparatus used for perfusion of isolated rings of
umbilical artery or vein. The rings are attached in
tandem to an isotonic transducer. The 10-ml bath
empties by overflow.
200
r
i
100
0
FLOW 2Sml/min
02 120 mmHg
P
to
-
£: i
aM
&
i
• #
3
9
E
E
F
—i—|
•-
"I
1
"!•!•
1
'
7.64- n$ BRAOYK/N/N/snl PERFUSATE
I mm
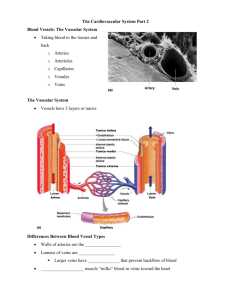
FIGURE 3
Record of inflow pressure to a perfused segment of
human umbilical artery. Continuous injection of
bradykinin resulted in a transient increase of inflow
pressure (representing constriction of the artery),
which returned to control values in spite of the continued infusion of bradykinin. Approximately 4 of the
5 minutes of delay time was transit time of the drug
from pump to segment of umbilical artery.
CircuUHcm Rtstmcb,
Vol. XXII, June 1968
preparation to another. A steady state was defined as a reproducible increase in the pressure
perfusing the umbilical artery in response to a
standard subatmospheric pressure. If a steady
state was not achieved within 4 hours of beginning perfusion, the preparation was discarded.
When it was obtained, drugs were administered
either as a single injection (Fig. 1) or as a constant infusion by a second pump; when a pump
was used, the volume of the tubing resulted in a
delay time of 4 minutes (transit time was measured by a blue dye).
Perfusion was begun with a solution whose
Po 2 was 15 mm Hg. As the artery gradually relaxed, flow was increased from 0 to 25 ml/min,
at which it was stable for the remainder of the
experiment.
RINGS OF UMBILICAL ARTERY
VALVE
INFLOW
PRESSURE
(mmHg)
749
Human umbilical arteries were gently and rapidly dissected free of connective tissue. Two rings
of artery 1.0 to 1.5 cm long were suspended, in
tandem, in a 10-ml muscle chamber (Fig. 2).
The rings gradually relaxed in the next 45 to 60
minutes. The rings were connected to a Phipps
and Bird linear motion transducer with a resting
load of 4 g. For 1 to 10 hours, each exposure to
increased Po2 or drugs resulted in increased response. Once reproducible responses were obtained to test stimuli, a steady state of sensitivity
was maintained for 5 to 10 additional hours, although 45 to 60 minutes were usually required
between drugs before reproducibility could be
achieved. The Krebs-Ringer bathing medium was
prepared according to the method of Umbreit et
al., modified to contain 5.5 instead of 11.0
mEq/liter calcium (14). We reduced the calcium concentration and changed from the perfusion solution to a Krebs-Ringer bathing medium in an unsuccessful attempt to shorten the
period of delay before reproducible responses
were obtained and to reduce spontaneous constrictor activity. The solution was maintained at a
pH of 7.35, and the temperature varied between
36.5 and 37.5°C. Throughout the experiment,
1% CO2 and 2% to 93* O2 bubbled through the
muscle chambers. Tn all experiments on rings and
on segments of arteries, peak responses were measured. All stimuli were applied in random order.
DRUGS
Bradykinin, epinephrine chloride, 5-hydroxytryptamine creatinine sulfate (serotonin), isoproterenol
hydrochloride, phentolamine methanesulfonate,
and propranolol hydrochloride were prepared
fresh for each experiment, and concentrations
were calculated as free base. The concentrations of the drugs are recorded later in the paper
750
ELTHERINGTON, STOFF, HUGHES, MELMON
CHANGE IN INFLOW
PRESSURE (mmHg)
250 r
600
200 -
500 -
15O -
4OO --
INFLOW PRESSURE
(mm Hg)
r
Hg
n • 4-
I
iI
3OO
IOO "
/ — BRAD YKrN/N
2OO
SEHO TQNIN
/
• s
{
100 -
O
-r^-''
30
60
90
120
PO! OF PERFUSION 60LUTI0N (mrnHg)
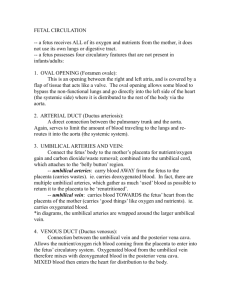
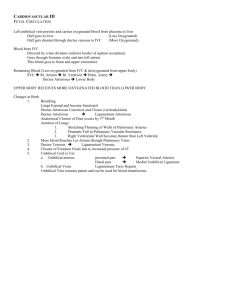
FIGURE 4
The direct relationship between Pot of the perfusion
solution and inflow pressure to the umbilical artery.
Magnitude of response (slope of the line) was greatest
over the Pot range of 15 mm Hg to 120 mm Hg,
even though a Pot of 700 mm Hg caused significantly
greater constriction (P < 0.05 by t-test) than 120 mm
Hg. The means ± 1 SD of 4 experiments are shown.
i
I
/—C&NCPHRINE
i tXrT i 11
i
i
i i i i ii
2
4- 6 6 10
20
40 6 0 100
MOLAR DRUG CONCENTRATION (x IO*9)
FIGURE 6
Dose-response curves of bradykinin, epinephrine, and
serotonin at a Pot of 120 mm Hg. Effects of epinephrine and serotonin at Pot of IS mm Hg are not
recorded because inordinately high ( > 10-} M) concentrations were needed to produce any recordable
changes in pressure. Means ± 1 SD are shown.
and in Figure 6. In addition, appropriate volumes of diluent or vehicle (as in the case of
phentolamine) were used as controls.
INFLOW PRESSURE
(mm Hg)
Results
6OO
PO2 A N D DRUG EFFECTS
5OO
40O
3OO
2OO
IOO
1
2
4
6 8 10
20
4O 6O 100
MOLAR DRUG CONCENTRATION (x IO' 9 )
FIGURE 5
Constriction by bradykinin of the perfused umbilical
artery at low and high Pot. At a Pot of IS mm Hg
the artery did not react to bradykinin as compared to
the higher Pot. At Pot 120 mm Hg, the artery ruptured at 450 mm Hg inflow pressure. Means ± 1 SD
are shoion.
Figure 3 shows the rise in inflow pressure
produced by a constant infusion of bradykinin through a segment of an umbilical artery. The pressure returned to control values
in spite of the continued injection of bradykinin.
Of particular interest was the response of
the umbilical artery to oxygen. Figure 4 shows
that inflow pressure increased as the P02
increased from 15 to 120 mm Hg. The peak
pressure was not sustained at any given Po2.
Increasing the Po2 of the perfusion solution
to approximately 700 mm Hg resulted in a
significantly greater increase in inflow pressure (P<0.05), over that obtained at a P02
of 120 mm Hg.
Bradykinin was much more effective in
constricting vessel segments perfused with a
solution at a Po2 of 120 mm Hg than with
one at 15 mm Hg (Fig. 5). Bradykinin was a
Circtdatian Resetrcb, Vol. XXII, ltm* 1968
SENSITIZATION OF UMBILICAL VESSELS BY OXYGEN
more potent constrictor on a molar basis than
epinephrine or serotonin (P < 0.001) tested on
the same arteries (Fig. 6).
In 125 experiments designed to characterize umbilical artery drug receptors, neither
phentolamine (5 X 1( H M ) nor propranolol
(1 X 10"3 M ) altered the response of 25 isolated umbilical artery rings to 9356 O2 or to
bradykinin (lxlO~ 8 M ) . This concentration
of phentolamine was sufficient to inhibit, but
not reverse, the response to epinephrine.
Propranolol, a beta-receptor blocking agent,
did not modify the epinephrine response.
Even when the artery rings were previously
constricted by O2 or bradykinin, they did not
respond to high concentrations of isoproterenol (1 X 10"3 M ) in the presence or absence
of a beta-receptor antagonist. No attempt was
made to block the serotonin effect.
Discussion
This study demonstrates that bradykinin
and O2 elicit in-vitro constriction of human umbilical arteries. The magnitude is
directly proportional to the Po2 of the
perfusion fluid. At a Po2 of 15 mm Hg,
which some authors state occurs in the
human umbilical arterial blood in vivo (12),
the vessels were relatively unresponsive to
all drugs tested. This evidence suggests that
the three vasoactive compounds tested in
these studies and that occur naturally in the
fetus (or may be administered to the mother
and cross the placenta) would be unlikely to
decrease fetal placental perfusion in vivo.
We have been unable to demonstrate vasodilation with isoproterenol but have not eliminated "silent" or functionless beta-receptors
capable of binding catecholamines (15). The
apparent absence of functioning beta-receptors
in human umbilical arteries suggests that any
release of epinephrine from the fetal adrenal
medulla during birth could act only to reduce fetal blood flow to the placenta, especially in the presence of gradually increasing oxygen tension in the umbilical arterial
blood. In the human, decreasing placental
blood flow as determined by umbilical vessel
constriction provides effective blood volume
Circulation Ktsetrcb, Vol. XXII. Junt 1968
751
homeostasis during the period between delivery of the baby and of the placenta. Whether bradykinin is involved in human umbilical
artery constriction remains for future studies.
An important limitation to the extension of
the in-vitro data to in-vivo conditions is implied by the very low flow rates obtained in
the perfusion studies. These vessels were obtained after they had become constricted during normal childbirth. They remained constricted, so that almost no umbilical blood
flow would have occurred if they were in
the same condition in vivo. Driving pressures
of 25 mm Hg were needed to cause a flow of
25 ml/min in a 15-cm segment of one artery.
This segment represents less than one-third
the usual cord length and of course does not
include resistances created by vessels in the
chorionic villi and fetal liver. Arterial pressure
in the fetus of 50 to 60 mm Hg may drive as
much as 500 ml blood (not saline)/min
through the fetal circulation. Therefore, the
in-vitro test system has \% to 22 of the "conductance" in vivo. At first glance, it might be
necessary to postulate another mechanism independent of increased P02 or bradykinin,
epinephrine, or serotonin release to produce
closure of umbilical arteries. However, such
substances may cause an initial and irreversible constriction of the vessels. Such constriction might even be independent of vascular
viability. Despite the limitations of an in-vitro
test system and the alteration and perhaps irreversible constriction, the vessels were responsive to the three drugs tested and to stretch.
The isolated rings also responded to drugs in
the same qualitative way as the vessels used
in perfusions. What physiologic importance
oxygen and bradykinin have in in-vivo constriction of cord vessels could only be assessed
in studies done in vivo or on unconstricted
vessels of species closely resembling the human.
There is no evidence that the response of
the umbilical artery to O2 and to bradykinin
is mediated by the same receptors. It is known
that extracts of human umbilical arteries free
from blood contain at least one vasoconstrictor substance (16). This substance has
752
ELTHERINGTON, STOFF, HUGHES, MELMON
not been identified, but does not appear to
be bradykinin. Whether bradykinin is produced
in the fetal-neonatal period and whether it
could be an important mediator in neonatal
vascular changes are discussed elsewhere
(17). Regardless of whether bradykinin is
a mediator of such changes, this study makes
it evident that the human umbilical vessels
in vitro are sensitized by O2 to the effects of
epinephrine, serotonin, and bradykinin. Sensitization may play an important in-vivo role
in the circulatory adjustments essential for
normal human newborn life.
Acknowledgment
Materials were provided by Dr. A. Margolis and
the Sandoz Pharmaceutical Company.
7. CAMBELL, A. G. M., DAWES, G. S., FISHMAK,
A. P., HYMAN, A. I., AND PERKS, A. M.: Re-
lease of a bradyldnin-lilce pulmonary vasodilator
substance in foetal and new-born lambs. J.
Physiol. (London) 198: 83, 1968.
8. KOVALCIK, V.: Response of the isolated ductus
arteriosus to oxygen and anoxia. J. Physiol.
(London) 169: 185, 1963.
9. DAVICNON, J., LORENZ, R. R., AND SHEPHERD,
J. T.: Response of human umbilical artery to
changes in transmural pressure. Am. J. Physiol.
209: 51, 1965.
10.
12.
References
Obstet. Gynecol. 84: 1634, 1962.
Effects of chemical mediators on the pulmonary and ductus arteriosus circulation in the
fetal lamb. Am. J. Obstet. Gynecol. 89: 252,
1964.
4. PANICEL, M.: Placenta! perfusion experiments.
Am. J. Obstet. Gynecol. 84: 1664, 1962.
DEFREITAS, F. M., FARACO, E. Z., AND D E -
AZEVEDO, D. F.: General circulatory alterations induced by intravenous infusion of synthetic bradykinin in man. Circulation 29: 66,
1964.
6. DAWES,
G.
S.:
Pulmonary
peculiarities
of
the
BARTELS,
H.,
MOLL, W., AND METCALF,
J.:
13. BURTON, A. C , AND STINSON, R. H.: Measure-
ment of tension in vascular smooth muscle. J.
Physiol. (London) 153: 290, 1960.
DAWES, G. S.: The umbilical circulation. Am. J.
3. SMITH, R. W., MORRIS, J. A., AND ASSALI, N. S.:
5.
Anatomical
human umbilical cord and their clinical significance. Am. J. Obstet. Gynecol. 52: 387,
1946.
11. NEWMAN', R. L.: Serum electrolytes in pregnancy, parturition and puerperium. Obstet.
Gynecol. 10: 51, 1957.
Physiology of gas exchange in the human placenta. Am. J. Obstet. Gynecol. 84: 1714, 1962.
1. DAWES, G. S.: Changes in the circulation at birth.
Anesthesiology 26: 522, 1965.
2.
SPIVACK, M.:
circulation
in
the
foetus and new-born. Brit. Med. Bull. 22: 61,
1966.
14.
UMBREIT, W. W., BURRIS, R. H., AND STAUFFER,
J. J.: Manometric Techniques and Tissue Metabolism, 3d ed. Minneapolis, Burgess, 1957, p.
149.
15. BURKS, T. F., AND COOPER, T.:
Enhancement
of peripheral alpha-receptor stimulation by
blockade of ''silent" beta-receptors. Circulation Res. 21: 703, 1967.
16. KARIM, S. M. M.: A smooth muscle contracting
substance in extracts of human umbilical cord.
Nature 211: 425, 1966.
17.
MELMON, K. L., RUDOLPH, A. M., HUGHES, T.,
NIES, A. S., AND CLINE, M. J.: Kinins—possi-
ble mediators of neonatal circulatory changes.
J. Clin. Invest., in press, May 1968.
€irc*lait(m RtJtarcb, Vol. XXII, ]u*t 1968