META-ANALYSIS OF TIME-SERIES STUDIES AND PANEL STUDIES OF PARTICULATE MATTER (PM) AND OZONE (O3)
Prepared by: H. Ross Anderson,
Richard W. Atkinson,
Janet L. Peacock,
Louise Marston and
Kostas Konstantinou
Meta-analysis of
time-series studies
and panel studies of
Particulate Matter (PM)
and Ozone (O3)
Report of a WHO task group
EUR/04/5042688
E82792
Original: English
Meta-analysis of time-series
studies and panel studies of
Particulate Matter (PM) and
Ozone (O3)
Report of a WHO task group
This report was prepared by: H. Ross Anderson, Richard W. Atkinson, Janet
L. Peacock, Louise Marston and Kostas Konstantinou, all at the Department of
Community Health Sciences, Epidemiology, St. George’s Hospital Medical School,
London, United Kingdom as part of the WHO project "Systemic Review of Health
Aspects of Air Quality in Europe"
ABSTRACT
Quantitative health impact assessment has become increasingly important in the development of air
quality policy. For such analysis it is important to have accurate information on the concentration-response
relationships for the effects investigated, for example on the relationship between changes in daily air
pollution and its impact on health. Therefore, a quantitative meta-analysis of peer reviewed studies was
conducted to obtain summary estimates for certain health effects linked to the exposure to particulate
matter (PM) and ozone. This work was done as part of the WHO project “Systematic review of health
aspects of air pollution in Europe”, which is funded by the European Commission and is intended to
provide input to the Clean Air For Europe (CAFE) programme. The data for these analyses came from a
database of time-series studies (ecological and individual) developed at St. George’s Hospital Medical
School at the University of London. The meta-analysis was also performed at St. George’s Hospital
according to a protocol that was agreed upon by a WHO Task Group in advance of the work. This analysis
confirmed statistically significant relationships between levels of PM and ozone in ambient air with
mortality, using data from several European cities. Updated risk coefficients in relation to ambient
exposure to PM and ozone were obtained for all-cause (relative risk for a 10 µg/m3 increase in PM10: 1.006
(1.004, 1.008) and ozone: 1.003 (1.001, 1.004), respectively) and cause-specific mortality and hospital
admissions for respiratory and cardiovascular causes. In addition, possible publication bias was
investigated and revised summary estimates were calculated. Also panel studies were analyzed to derive
summary estimates for coughs and medication use in individuals with underlying respiratory disease.
Keywords
META-ANALYSIS
AIR POLLUTANTS – adverse effects
ENVIRONMENTAL EXPOSURE
OZONE
RISK ASSESSMENT
Address requests about publications of the WHO Regional Office to:
• by e-mail
publicationrequests@euro.who.int (for copies of publications)
permissions@euro.who.int (for permission to reproduce them)
pubrights@euro.who.int (for permission to translate them)
• by post
Publications
WHO Regional Office for Europe
Scherfigsvej 8
DK-2100 Copenhagen Ø, Denmark
© World Health Organization 2004
All rights reserved. The Regional Office for Europe of the World Health Organization welcomes requests for permission to
reproduce or translate its publications, in part or in full.
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion
whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or
of its authorities, or concerning the delimitation of its frontiers or boundaries. Where the designation “country or area”
appears in the headings of tables, it covers countries, territories, cities, or areas. Dotted lines on maps represent approximate
border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or
recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and
omissions excepted, the names of proprietary products are distinguished by initial capital letters.
The World Health Organization does not warrant that the information contained in this publication is complete and correct
and shall not be liable for any damages incurred as a result of its use. The views expressed by authors or editors do not
necessarily represent the decisions or the stated policy of the World Health Organization.
CONTENTS
Page
1.
Background ................................................................................................................. 1
2.
Process ....................................................................................................................... 1
3.
Methods ...................................................................................................................... 2
4.
5.
3.1
Systematic review database ................................................................................ 2
3.2
Selection of studies for meta-analysis .................................................................. 2
3.3
Selection issues specific to panel studies.............................................................. 3
3.4
Meta-analysis ..................................................................................................... 3
Results ........................................................................................................................ 3
4.1
Summary estimates ............................................................................................ 3
4.2
Time-series results ............................................................................................. 5
4.3
Panel Results ..................................................................................................... 8
Discussion ................................................................................................................. 10
5.1
Exploration of heterogeneity ............................................................................. 11
5.2
Publication bias ................................................................................................ 12
References......................................................................................................................... 26
Annex 1. Members of the WHO task group........................................................................... 28
Annex 2. Minutes of the task group meeting in London ......................................................... 29
Annex 3. Use of bibliographic database for systemic review .................................................. 33
Annex 4. Tables of individual city results – time-series.......................................................... 36
Annex 5. Meta-analysis of PM2.5 results from non-European countries .................................. 68
EUR/04/5042688
page 1
1.
Background
The WHO project “Systematic Review of Health Aspects of Air Quality in Europe”, which is
financially supported by the European Commission, aims to provide the Clean Air for Europe
(CAFE) programme of the Commission’s DG Environment with a systematic, periodic and
scientifically independent review of the health aspects of air pollution in Europe.
As part of this review process WHO/Europe convened a working group to provide answers to a
set of twelve questions in relation to the health effects of particulate matter, ozone and nitrogen
dioxide. The report from this working group provided a comprehensive description of the
hazards related to these pollutants, but no detailed guidance on risk assessment (WHO 2003).
Therefore, the working group recommended conducting a quantitative meta-analysis of existing
studies which could be used subsequently for health impact assessments. The data for these
analyses came from a database of time-series studies (ecological and individual) developed at St.
George’s Hospital Medical School at the University of London. The meta-analysis of these data
will be used to update risk coefficients for selected health endpoints in relation to ambient
exposure to particulate matter and ozone.
2.
Process
A WHO task group was established to perform the meta-analysis. The analysis was carried out at
St. George’s Hospital Medical School at the University of London. The members of the task
group are listed in Annex 1.
This report describes the work undertaken for this meta-analysis and presents both the summary
estimates and the raw data used in their calculation. It details the assumptions made in order to
select the studies for inclusion in the calculation of the summary estimates. The Task Group
agreed on these assumptions at a meeting in London on 8 April 2003. The minutes from this
meeting are attached as Annex 2. At this meeting it was decided to investigate a number of
different health outcomes and to conduct sensitivity analyses. However, because of the large
number of permutations of health outcomes and exposure measures, a core set of analyses was
subsequently agreed with the task group: According to this agreement, meta-analytical estimates
for the effects of particles (PM10, PM2.5, black smoke (BS) and coarse fraction) and ozone were
estimated for the following health outcomes:
•
daily number of deaths from all causes (excluding accidents), from respiratory causes and
from cardiovascular causes as categorised by the WHO International Classification of
Diseases;
•
daily number of hospital admissions (incl. emergency department and emergency room
admissions) for respiratory diseases (subdivided by ages 0–14, 15–64 and 65+ years) and
for cardiovascular disease (for ages 65+);
•
cough in individuals with underlying respiratory disease (for children and adults
separately);
•
respiratory medication use in individuals with underlying respiratory disease (for children
and adults separately).
EUR/04/5042688
page 2
3.
Methods
3.1 Systematic review database
As part of a project to assist the Department of Health in the United Kingdom in their evaluation
of the evidence of the adverse health effects of air pollution, a series of databases containing
details of published studies was set up at St. George’s Hospital Medical School. Search criteria
were developed to identify the relevant studies indexed in the peer-reviewed literature. They
aimed to identify time-series studies (both ecological and individual) of the short-term health
effects of air pollution. Original numerical estimates of these effects, together with other relevant
information were extracted from these studies and entered into the ACCESS databases. The
APED (Air Pollution Epidemiology Databases) contain estimates of the effects of particles,
nitrogen dioxide, sulphur dioxide, ozone and carbon monoxide. The outcomes studied were
mortality, hospital admissions, use of medical services, respiratory symptoms and lung function.
Results for subdivisions by diagnosis, age and season and for various lags were also recorded.
Procedures for the validation and analysis of these data have been developed and periodic
reviews of the literature are carried out to update the databases. Further details are given in
Annex 3.
3.2 Selection of studies for meta-analysis
Studies can vary in many ways, for example in their definition of the health outcome, their
choice of pollutant metric and their reporting of results. When more than one study has been
conducted using the same population, further consideration of the study characteristics are
required. They may have been published at different times and may have used different statistical
methods. It was considered desirable that, for the purposes of health impact assessment, the
results were not dominated by multiple analyses of single locations. Also, it was important that
study selection was unbiased by knowledge of the result. Hence, guidelines for study selection
were discussed and determined at a meeting of the WHO Task Group in London on 8 April 2003
(see also Annex 2). The minutes of the meeting outline the decisions taken and therefore only the
key points are summarized below.
1.
The number of estimates available for meta-analysis should not be a determining factor in
selecting studies – that is, there should be no compromises on any of the criteria for study
selection in order to raise the number of studies included in the analysis
2.
It was decided to concentrate upon European studies. If there were insufficient studies to
perform a meta-analysis then it may be necessary to consider the inclusion of studies from
other parts of the world. However, this issue would need further consideration by the
whole task group should it occur.
3.
Only one estimate from each city should be used in a meta-analysis. A number of cities
have been studied more than once and therefore a mechanism for selecting the appropriate
estimate was needed. It was decided to select the latest study published or, if the study
participated in a large multicity study, to use the multicity study result.
4.
The initial analysis will focus upon single-pollutant model results based upon an all-year
analysis.
5.
The “selected” lag from the database would be used rather than specific lags or
combinations of lags.
EUR/04/5042688
page 3
3.3 Selection issues specific to panel studies
For panel studies the same protocol was followed. In particular, summary estimates were only
calculated where there were four or more individual estimates, and the analysis was confined to
European studies.
As will be seen, the results were dominated by the PEACE study, which was a multicentre study
conducted in 14 centres using a common protocol. Each centre had an urban and rural panel of
symptomatic children, giving 28 panels (and estimates) in all. It must be pointed out that there is
a degree of correlation between these panel studies because all were carried out during the same
winter period when air pollution levels were correlated over a wide area of Europe. Also, the
studies coincided with an influenza epidemic which could not be accounted for in the analysis
(Roemer et al., 2000).
3.3.1 Patient group
The requirement was to include studies among individuals with chronic respiratory disease.
Studies varied in their definitions of patient group and the following were included for children:
asthmatic (mild, moderate, severe, on and not on medication), and chronic respiratory symptoms.
In adults, the same two categories were included plus panels with chronic obstructive pulmonary
(airway) disease or bronchial hyperresponsiveness. No subgroup analyses within asthmatic
panels were used.
3.3.2 Outcomes
The task group wished to have one or two outcomes that reflected an exacerbation in asthmatic
patients. Panel studies have recorded a large variety of symptoms and lung function measures. It
was agreed to use “cough” and “medication use” as indicators of a worsening of respiratory
health in symptomatic individuals. The following measures of cough were used: unspecified
cough, cough in combination with wheeze and tight chest and night cough. Both incidence and
prevalence measures were analysed and where both were reported, incidence estimates were
used. Measures of medication use were bronchodilator or specific use of ß agonists.
3.4 Meta-analysis
Fixed- and random-effects summary estimates for each pollutant-outcome pair were calculated
for an effect of 10 µg/m3 increase in the pollutant (Der Simonian & Laird, 1986).
4.
Results
Using studies catalogued in bibliographic databases up to February 2003, 629 ecological timeseries studies and 160 individual or panel studies have been identified. 286 time-series and 124
panel studies have provided usable data. The two databases contain over 11 700 and 6400 effect
estimates, respectively.
4.1 Summary estimates
Tables 1–4 show the random-effects summary estimate for each pollutant/outcome combination.
The tables also give the number of estimates available for analysis. For some outcome/pollutant
EUR/04/5042688
page 4
combinations there were insufficient numbers of studies for meta-analysis (a minimum of four
estimates were required for meta-analysis) and therefore, no summary estimates are given in the
tables. Individual city results are given in the Annex 4.
Table 1. Summary relative risk estimates (and 95% confidence intervals) for a 10 µg/m3 increase
in pollutant for all-cause and cause specific mortality
Outcome/
Disease
Age
All-Cause
All age
Respiratory
All age
Cardiovascular
All age
PM10
PM2.5
CF
1.006 (1.004, 1.008) NA 3
331
1.013 (1.005, 1.020) NA 1
18
1.009 (1.005, 1.013) NA 1
17
NA 1
BS
Ozone (8-hour)
1.006 (1.004, 1.008) 1.003 (1.001, 1.004)
26
15
1.006 (0.998, 1.015) 1.000 (0.996, 1.005)
18
12
1.004 (1.002, 1.007) 1.004 (1.003, 1.005)
18
13
NA 1
NA 2
Notes:
1. Numbers in bold indicate number of European studies available.
2. NA – insufficient numbers available for meta-analysis (<4).
Table 2. Summary relative risk estimates (and 95% confidence intervals) for a 10 µg/m3 increase
in pollutant for respiratory and cardiovascular hospital admissions
Outcome/
Disease
Age in
years
Respiratory
Respiratory
0–14
15–64
Respiratory
65+
Cardiovascular
65+
PM10
PM2.5
CF
BS
NA 3
NA 3
NA 1
NA 1
NA 1
NA 1
1.007 (1.002, 1.013) NA 1
8
NA 2
NA 0
NA 1
NA 0
Ozone (8-hour)
NA 2
NA 3
1.006 (1.001, 1.010) 1.001 (0.991, 1.012)
5
5
1.001 (0.993, 1.010) 1.005 (0.998, 1.012)
6
5
NA 2
NA 1
Notes:
1. Numbers in bold indicate number of European studies available.
2. NA – insufficient numbers available for meta-analysis (<4).
Table 3. Summary odds ratios (95% confidence intervals) for a 10 µg/m3 increase
in pollutant for cough
Patient group
Age
in
years
PM10
PM2.5
CF
Symptomatic
children
Symptomatic
adults
5–15
0.999 (0.987, 1.011)
34
NA
3
NA 1
NA 1
1.001 (0.982, 1.021) 33 NA 1
No
studies
No
studies
NA 2
16–70
BS
Notes:
1. Numbers in bold indicate number of European studies available.
2. NA – insufficient numbers available for meta-analysis (<4).
Ozone
NA 1
EUR/04/5042688
page 5
Table 4. Summary odds ratio estimates (and 95% confidence intervals) for a 10 µg/m3 increase
in pollutant for medication use
Patient
group
Symptomatic
children
Symptomatic
adults
Age
in
years
5–15
16+
PM10
PM2.5
CF
BS
Ozone
1.005 (0.981, 1.029)
31
NA 3
NA 1
NA 1
1.008 (0.970, 1.049) 31
NA 1
No
studies
NA 1
NA 2
NA 1
Notes:
1. Numbers in bold indicate number of European studies available.
2. NA – insufficient numbers available for meta-analysis (<4).
4.2 Time-series results
Mortality and particles
Estimates of the effect of PM10 on all-cause mortality were taken from 33 separate European
cities or regions (Table A1, Appendix). The random-effects summary relative risk for these 33
results was 1.006 (95% CI: 1.004, 1.008) for a 10 µg/m3 increase in PM10. 21 of theses estimates
were taken from the APHEA 2 (Air Pollution and Health: a European Approach 2) study
(Katsouyanni et al, 2001) and hence the summary estimate derived from this review is dominated
by this multicity study.
Cause-specific results for mortality are yet to be published from the APHEA 2 project. Hence,
the numbers of estimates for cardiovascular and respiratory mortality are smaller than for allcause mortality, 17 and 18 respectively. The corresponding summary estimates were 1.009
(1.005, 1.013) and 1.013 (1.005, 1.020) for a 10 µg/m3 increase in PM10 (Tables A2 and A3).
The majority of the estimates in these two categories come from multicity studies conducted in
France, Italy and Spain.
The estimates for all-cause mortality and cause-specific mortality are comparable to those
originally reported from the National Mortality, Morbidity and Air Pollution Study (NMMAPS)
based upon the 20 largest cities in the United States (Samet et al., 2000). For a 10 µg/m3 increase
in PM10 they reported a 0.51% (0.07, 0.93) increase in daily mortality from all causes and for
cardio-respiratory mortality the corresponding percentage change was slightly larger at 0.68%
(0.2, 1.16). A recent re-analysis of the NMMAPS data, organized by the US Health Effects
Institute (HEI) because of concern over the statistical procedures used in the original analyses,
revised the NMMAPS summary estimates downwards to 0.21% for all-cause mortality and
0.31% for cardio-respiratory mortality (HEI, 2003). A similar re-analysis of the APHEA 2
mortality data revealed that the European results were more robust to the method of analysis.
Depending upon the method of smoothing adopted, the summary estimate for PM10 and all-cause
mortality reduced by 4% when “loess” smoothing with more stringent convergence criteria were
used, reduced by 34% when natural splines were used instead of “loess” smoothing and reduced
by 11% when penalized splines were used to smooth the time-series. The actual effect estimates,
expressed as an increase in mortality associated with a 10 µg/m3 increase in PM10, under these
three scenarios were: 0.6% using “loess”, 0.4% using natural splines and 0.6% using penalized
splines.
Very few European studies of all-cause and cause-specific mortality and fine particles were
found. All-cause mortality and PM2.5 were reported from Erfurt, Germany (Wichmann et al.,
EUR/04/5042688
page 6
2000), the Czech Republic (Peters et al., 2000) and the West Midlands conurbation in the United
Kingdom (Anderson et al., 2001) (Table A9). Evidence from Europe of an effect of fine particles
on daily mortality is therefore sparse. Of the five estimates from three studies available, none
showed a statistically significant positive association and one was significantly negative. The
West Midlands study was a systematic study of both mortality and hospital admissions with the
specific aim of investigating associations between health outcomes and different particle
measures and sizes. It covered a population in excess of 2 million. The health data were from the
mid-1990s and the analysis followed the APHEA 2 methodology, which included an a priori
hypothesis of lag0+1. It therefore seems an appropriate study from which to take the health
effect estimates for fine particles. These estimates are listed in Table A9. For all-cause mortality
the relative risk for an effect of PM2.5 was 1.0034 (0.9915, 1.0154). This compares with 1.0057
(0.9980, 1.0136) and 0.9837 (0.9677, 0.9999) from studies in the Czech Republic and Erfurt
respectively. For cause-specific mortality only the West Midlands study provides effect
estimates (Tables A9).
In view of the paucity of data on PM2.5 effects in Europe, and following the decisions of the task
group on the meta-analysis protocol, we also looked for studies conducted outside of Europe.
This analysis is fully described in Annex 5. The estimates for North American cities were larger
than those for Europe and their summary estimates were statistically significant. While the
transferability of the North American coefficients to Europe will increase the uncertainty and
requires proper consideration of the differences and similarities of the two regions, these results
also give confidence that the results from the large West Midlands study are likely to represent a
positive association with daily mortality. In general it is difficult to be confident that three
estimates are sufficient to characterize the European situation. Whatever estimate is chosen for
Europe, it seems clear that any health impact assessment analysing effects of short term exposure
to PM2.5 will need to consider these as a source of uncertainty.
Black smoke (BS) is a measure of the blackness of particles with diameter under 4.5 µm. It is
probably a reasonable indicator of primary fine particles originating from combustion sources.
There are numerous studies of black smoke and mortality from the European Region. Twenty-six
estimates of the effect of black smoke on all-cause mortality were extracted from the database
and they show an overall summary relative risk of 1.006 (1.004, 1.008) per 10 µg/m3 increase in
BS (Table A5). As for PM10, estimates from APHEA 2 study dominate this group of results.
Also, since it was the larger cities in Europe that participated in the APHEA 2 programme, the
results from this meta-analysis closely match those from APHEA 2. The summary estimate
derived from this review was 1.006 (1.004, 1.009) slightly larger than that calculated from the
meta-analysis of the 14 APHEA 2 estimates at 1.005 (1.004, 1.006). The re-analysis of the black
smoke results by Katsouyanni and colleagues found little change in the size and precision of the
summary BS estimate from the APHEA 2 data (Katsouyanni et al., 2001).
For cause-specific mortality, 18 estimates were available for both cardiovascular mortality and
respiratory mortality (Tables A5 and A6), most estimates deriving from multicity studies
conducted in France, Poland and Spain. The summary relative risks per 10 µg/m3 increase in BS
for cardiovascular and respiratory mortality were 1.004 (1.002, 1.007) and 1.006 (0.998, 1.015)
respectively. Cause-specific results for BS from the APHEA 2 project were not in print at the
time of the review.
EUR/04/5042688
page 7
The evidence for an effect of coarse fraction particles in Europe is even less substantive than for
fine particles. Only two European studies, the West Midlands study described above, and a study
of cardiovascular admissions from Krakow 1979–1989, have examined the effect of coarse
particles (PM10–2.5) on daily mortality. The only study to show a statistically significant adverse
effect of particles in the range PM10–2.5 was conducted in Poland (Krzyzanowski & Wojtyniak,
1991). At this stage, no summary relative risks for health impact assessments of coarse particles
can be given.
Hospital admissions and particles
Sufficient numbers of estimates (>3) of the effect of PM10 were available only for respiratory
admissions in the 65+ age group. The relative risk for a 10 µg/m3 increase in PM10 was 1.007
(1.002, 1.013) (Table 2) and was based upon 8 estimates (Table A4). Six of these eight estimates
were provided by the APHEA 2 project (Atkinson et al., 2001). As for mortality, a re-analysis of
the APHEA 2 data confirmed the robustness of the original results (HEI, 2003). Unfortunately,
we were unable to use much of the recent published data on particles and daily admissions for
respiratory disease from APHEA 2 because this study did not report all respiratory admissions in
the younger age groups.
For the other two age categories, ages 0–14 and 15–64 years, results were available from three
studies conducted in London (Atkinson et al., 1999), West Midlands (Bremner et al., 1999) and
Rome (Michelozzi et al., 2000) (Tables A4). Together these cities represent a population in
excess of 10 million people. A meta-analysis of results from these three cities gave summary
estimates of 1.010 (0.998, 1.021) and 1.008 (1.001, 1.015) per 10 µg/m3 increases in PM10 for
respiratory admissions, ages 0–14 and 15–64 years respectively. It may be appropriate to
reconsider the guideline on the number of estimates required for a meta-analysis given the small
numbers available for some combinations of health outcome and pollutant.
For fine and coarse particles only the West Midlands study provided results for the respiratory
outcomes. The relative risks for PM2.5 for each of the three age categories, 0–14, 15–64 and 65+
years were 1.091 (0.9994, 1.0391), 0.9881 (0.9633, 1.0135) and 0.9926 (0.9732, 1.0125)
respectively (Table A10). There were no estimates available from the 65+ years, cardiovascular
admissions group. Results for coarse particles were similar to those for fine particles.
Results for BS and respiratory admissions in the over 65 were dominated by the APHEA 2
programme (Atkinson et al., 2001), all bar one of the six results coming from that project. Hence
the summary estimate of the relative risk of 1.001 (0.993, 1.010) was almost identical at 1.001
(0.993, 1.009). The slightly wider confidence interval in the meta-analytical estimate reflected
the addition of the result from Edinburgh (Prescott et al., 1998), a relatively small city. For
respiratory admissions in adults aged 15–64 years the summary estimate was based upon the
original APHEA 1 analysis of four cities (Amsterdam, London, Paris and Rotterdam) (Spix et
al., 1998) together with the result from the West Midlands study. The summary relative risk was
1.006 (1.001, 1.010) per 10 µg/m3 increase in BS. For admissions for respiratory disease in
children aged 0–14 years only two results were available, one from London and one from the
West Midlands (Table A8). A meta-analysis of these two results gave an estimate slightly closer
to the London estimate because of the larger weight London has in the analysis due to its larger
population. The choice of estimate for this group needs further consideration.
Two studies of BS and cardiovascular admissions in the elderly (65+ years) have been published
– from London and Edinburgh. Because of the larger population in London the summary
EUR/04/5042688
page 8
estimate from the London study would be appropriate – relative risk 1.017 (1.008, 1.026),
compared to 1.023 (0.981, 1.069) for Edinburgh. We were unable to use the recently published
results from APHEA 2 (Le Tertre et al., 2002) because these described cardiac rather than
cardiovascular admissions. The present analysis includes cerebrovascular disease in addition to
cardiac disease. Most European evidence suggests that there is no relationship between air
pollution and cerebrovascular disease, so in retrospect, it might have been better to choose this
diagnostic group.
Mortality and ozone
Table 1 shows the summary estimates for the three mortality outcomes and ozone. There were
15, 13 and 12 estimates available for meta-analysis for all-cause, cardiovascular and respiratory
mortality. Details of the individual estimates are given in Tables A11–A13. The relative risks per
10 µg/m3 increases in ozone were 1.003 (1.001, 1.004), 1.004 (1.003, 1.005) and 1.000 (0.996,
1.005) for all-cause, cardiovascular and respiratory mortality respectively. In each group the
estimates are based upon studies in France, Italy, the Netherlands, Spain and the United
Kingdom. Results from the APHEA 2 project are not yet published.
Hospital Admissions and ozone
The numbers of available estimates were limited for respiratory and cardiovascular admissions.
The original APHEA programme provided summary estimates for respiratory admissions in age
ranges 15–64 and 65+ years. Combining these results with those from the West Midlands study
gave summary relative risks of 1.001 (0.991, 1.012) and 1.005 (0.998, 1.012) respectively. Three
estimates were available for respiratory admissions in children aged 0–14 years. A meta-analysis
of these estimates gave a summary relative risk of 0.999 (0.987, 1.012). Only one estimate, from
a study in London, was available for cardiovascular admissions. It showed a positive and
statistically significant association with ozone, relative risk 1.007 (1.002, 1.011) per 10 µg/m3
increase in mean 8-hour ozone.
The lack of matching of outcomes chosen for this meta-analysis with those for which published
data are available – discussed above for particles – was also a problem for ozone. A further
problem was that some studies reported only results for maximum one-hour ozone, not eighthour ozone.
4.3 Panel Results
Cough and particles in symptomatic children
Thirty-four estimates were available for PM10 and cough in children (Table A15). Many of the
estimates used for European panel studies are from the PEACE study. PEACE is a multicity
panel study conducted in 14 centres using a common protocol. Each PEACE centre studied an
urban and a rural panel of symptomatic children. Hence, for most outcome/pollutant
combinations, PEACE provided 28 estimates.
The dominance of the results by the PEACE study deserves special mention. This study was
carried out in children in 14 centres (one urban and one rural panel per centre) throughout
Europe in one winter. This will have reduced the potential for heterogeneity because the
exposure of the panels will tend to have been more similar than if they had been conducted in
different years or seasons. There was a concurrent influenza epidemic which could not be
accounted for in the analysis and the study period was somewhat too short to make adequate
adjustment for time trends (Roemer et al., 2000).
EUR/04/5042688
page 9
The pooled odds ratio estimate is close to 1.0 with 95% confidence limits indicating nonstatistical significance. There was only one estimate for PM2.5. This was from Finland where
49 children aged 8–13 were followed for six weeks (OR 1.091 (95%CI 1.007, 1.182) (Table
A16). There was a complementary estimate for coarse particles from the same study (OR 1.086
(1.023, 1.152) (Table A16). There were 33 studies of effects of black smoke. Once again, these
included 28 estimates from the PEACE studies and so provide a wide representation of European
cities. The pooled estimate was close to 1.0 and was not significant (Table A17).
Cough and ozone in symptomatic children
Only one estimate was available for this. This came from a Parisian study which included
82 children aged 7–15 years followed for three months. The odds ratio was 1.040 (0.920, 1.176)
(Table A16).
Cough and particles in symptomatic adults
There were six estimates of PM10 available in total but only three were usable. Of the usable
estimates, two were from the Netherlands and one was from Paris and the pooled estimate was
1.043 (1.005, 1.084). One further study from the Netherlands could not be combined with the
others since the estimate was a relative risk rather than an odds ratio. This estimate was not
significant, (Table A18). For a relatively common outcome such as cough, odds ratios and
relative risks cannot be considered to be equivalent. The two remaining studies of PM10 were
also Dutch studies and were not usable since the results had simply been quoted as “not
significant” in the text with no estimates of effect size presented (Table A18).
No studies were found which examined effects of PM2.5 or coarse particles on cough in adults.
There were five estimates of effects of black smoke, of which two were usable. These included
one Dutch and one Parisian study in 52 and 40 subjects followed respectively for three and six
months. The pooled estimate was 1.05 (1.011, 1.101). Three further Dutch studies had to be
excluded from meta-analysis due to the use of a relative risk estimate (one estimate, not
significant, Table A18) and results simply presented as “not significant” with no effect sizes (two
estimates, Table A18).
Cough and ozone in symptomatic adults
There were only two studies which estimated effects of ozone on cough in adults. One was a
study from the United Kingdom with 75 subjects followed for one month and gave an odds ratio
of 1.050 (0.910, 1.212). The other was a Dutch study in 60 subjects followed for three months
which reported a significant protective effect as a relative risk (Table A18), making it not
combinable with the odds ratio estimate.
Medication use and particles in symptomatic children
There were 31 studies analysing PM10 in children including 27 estimates from the PEACE
studies, thus providing a wide representation of European cities. (One PEACE centre [Poland]
only reported an estimate for the rural panel and hence there were 27 and not 28 PEACE
estimates, Table A19). The pooled estimate was 1.005 and the 95% CI spanned 1.00. No studies
were found for PM2.5 or coarse fraction. As for PM10, there were 31 studies that analysed black
smoke in children including 27 estimates from the PEACE studies and so again, these provide a
reasonable representation of European cities. The pooled estimate was 1.008 which was nonsignificant as for PM10 (Table A20).
EUR/04/5042688
page 10
Medication use and ozone in symptomatic children
Only one study was found for ozone in children. This was from a Parisian study in 82 children
followed for three months and gave an odds ratio of 1.410 (1.050, 1.890) (Table A21).
Medication use and particles in symptomatic adults
There were four estimates for PM10, all from the Netherlands. One estimate could not be
combined with the odds ratios as it was a relative risk. The pooled estimate for the remaining
three was 1.010 (0.990, 1.031). The three studies comprised 138, 128 and 32 subjects who were
all followed for about three months. The unusable estimate was non-significant (Table A22).
There were no studies found of PM2.5 and only one study of coarse fraction. This was from
Germany and involved 67 subjects who were followed for six months and gave an odds ratio of
1.008 (0.958, 1.061). There were three estimates of black smoke and these all came from Dutch
studies. There were two usable estimates from studies of 138 and 128 subjects followed for
about three months. The pooled estimate was 0.993 (0.956, 1.031). The third estimate was from a
study in 60 subjects followed for three months where the relative risk indicated a non-significant
protective effect (Table A22).
Medication use and ozone in symptomatic adults
Two studies looked at ozone in relation to medication use. One was a study performed in the
United Kingdom in 75 subjects followed for one month and gave an odds ratio of 1.440 (1.140,
1.810). The other was a Dutch study in 60 subjects followed for three months and which reported
a non-significant relative risk (Table A22).
5.
Discussion
There are sufficient European studies of the health effects of particulate matter measured as
PM10 and BS, and of ozone on all-cause and cause-specific mortality to perform a meta-analysis
and derive summary relative risks. The APHEA 2 project investigated cause-specific mortality
also for ozone (in relation to both all-cause and cause-specific mortality) and results are likely to
be published shortly. It may be appropriate to take consideration of the findings of this study
independently of this review – the results are already published in a technical report to the
European Commission.
There are insufficient studies of the health effects of fine and coarse particles on daily mortality
from Europe to fulfil the criteria to calculate summary estimates agreed by the Task Group. The
West Midlands study (Anderson et al., 2001) was designed specifically to study the health
effects of size-fractionated particulate matter and would provide a consistent and uniform set of
results for health impact assessment calculations. An alternative method to address the paucity of
results is to include non-European studies. The applicability of results from non-European
studies to European populations needs consideration however.
There are few studies generally of particulate matter and ozone and hospital admissions. Certain
age groups tend to be more frequently studied than others. For example sufficient studies of
admissions for respiratory diseases in those aged 65 years and over exist but not for younger age
groups. This is mainly because admissions for specific respiratory causes tend to be studied in
younger subjects, for example asthma. There may be little advantage in looking outside Europe
EUR/04/5042688
page 11
for further evidence as in the United States data on hospital admissions are routinely available
only for individuals older than 65 years. Other countries may, however provide usable results.
There is a surprising lack of estimates for the diagnostic group of all cardiovascular admissions
(ICD 9 390–459). There are a number of options to consider in seeking additional evidence. First
admissions for cardiac disease, ICD 9 codes 390–429, could be included in the study selection
protocol, thus enabling the inclusion of APHEA 2 published results for cardiac admissions.
Furthermore, studies of cardiac/cardiovascular admissions for all ages, rather than just for those
over 64 years of age, may be considered. Cardiovascular diseases are less common in children
and early adult life and so little may be lost in combining these two age groups.
There were sufficient studies of effects of PM10 and BS on cough and medication use in
symptomatic children to calculate overall pooled estimates. There were very few studies of
effects on cough of fine particles, coarse particles or ozone in children and few studies overall
for any pollutant in symptomatic adults. Summary values have been calculated in these
situations. However although it would seem reasonable to accept these as best available
estimates, they cannot be used with the same degree of confidence as those summary estimates
based on larger numbers of studies.
5.1 Exploration of heterogeneity
This meta-analysis aimed at producing summary estimates for chosen pollutants and outcomes. It
did not attempt to explain any heterogeneity in the estimates. Although there is the theoretical
potential to use information about the causes of heterogeneity to tailor estimates to subregions of
Europe, our knowledge is insufficient at present for this to be based on a solid foundation.
However, because the database contains information on the annual mean level of pollutant for
the cities concerned, it is relatively simple to produce a ranking of estimates according to the
mean level of pollution (shown in the tables of individual city data). A relationship would be
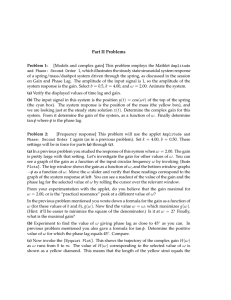
expected if a there was a threshold, or if another pollutant was an effect modifier. Fig. 1 gives an
example by ranking estimates for all-cause mortality and PM10, by the annual levels of PM10.
It is seen that there is no apparent relationship, indicating that the relative risk estimates apply to
a wide range of levels of PM10.
EUR/04/5042688
page 12
Fig. 1. Ranking of PM10 estimates for all-cause mortality by annual average levels of PM10 (left yaxis: mean PM10 levels in µg/m3; right y-axis: RR in total mortality of a 10 µg/m3 increase of PM10)
6.0
70
mean PM10
RR
5.0
mean PM10 level in µg/m3
60
50
40
3.0
2.0
1.0
30
20
0.0
-1.0
RR increase per 10 µg/m3
4.0
-2.0
10
-3.0
-4.0
Bir
mi
ng
ha
m,
S
We tock
h
st
Mi olm
dla
n
P ds
He aris
ls
Lo inki
nd
Ro o n
ue
Ba n
se
Str Zuri l
as ch
b
Le ourg
Ha
Ge vre
ne
v
Am Mad a
ste rid
rda
m
Ne
the Koln
r la
nd
Ly s
Ath on
Bu en
da s
p
Hu est
Flo elva
re
Bo nce
lo
Te gna
pl
S e i ce
Pa ville
ler
Cz
m
ec Tel o
h R Av
e p iv
u
Mi blic
la n
Er o
Cr furt
ac
ow
Ba Rom
rce e
lo
To na
r
Pr ino
ag
ue
0
5.2 Publication bias
Publication bias arises because there are more rewards for publishing positive or at least
statistically significant findings. It is a common if not universal problem in our research culture
(Sterling, 1959; Mahoney, 1977; Simes, 1986; Begg & Berlin, 1988 and 1989; Dickersin, 1997).
In the case of time-series studies using routine data there are particular reasons why publication
bias might occur. One is that the data are relatively cheap to obtain and analyse, so that there
may be less determination to publish “uninteresting” findings. The other is that each study can
generate a large number of results for various outcomes, pollutants and lags and there is quite
possibly bias in the process of choosing amongst them for inclusion in a paper. In the field of air
pollution epidemiology, the question of publication bias has only recently begun to be formally
addressed (Anderson et al., 2002 and Peacock et al., 2002). A related source of bias is lag
selection bias. These sources of bias are overcome by planned multicity studies (such as APHEA
and NMMAPS) which have a commitment to publish and which may adopt an a priori lag
specification.
There are methods of detecting publication bias but it should be noted that these are not without
problems. One method is the “funnel plot” in which estimates are plotted against their standard
error. If there is no publication bias, the resulting scatter should be symmetrically shaped like a
funnel (Light & Pillemer, 1984). Evidence of asymmetry in the funnel plot can be tested by
regressing the standardised effect size against the inverse of the standard error (Egger et al.,
1997).
EUR/04/5042688
page 13
It is important to distinguish two different implications of publication bias. The first relates to
hazard detection. Publication bias could lead to a false conclusion being drawn as to the
association between air pollution and a health outcome, i.e. that there is an association when in
fact there is none. The other implication is for health impact assessment because the publication
bias could lead to inflation of the estimated magnitude of the health impacts. Therefore, it might
be necessary to adjust for the bias before using the estimates in health impact assessments.
5.2.1 Time-series studies
The study results used in the calculation of the summary estimates in Tables 1 and 2 were
investigated for evidence of asymmetry and therefore the possibility of publication bias.
Asymmetry was assessed using both statistical procedures, Beggs test (Begg & Mazumdar,
1994) and Eggers test (Egger et al., 1997) and by graphical techniques using the funnel plot
(Light & Pillemer, 1984). The “trim and fill” technique (Duval & Tweedie, 2000) was also
applied both to further assess evidence for asymmetry and, where found, to calculate adjusted
summary estimates.
For those pollutant-outcome pairs having sufficient numbers of estimates, the original and
revised summary estimates are given in Tables 5 and 6. In all but one case there was evidence for
asymmetry and possible publication bias. In some cases the evidence was strong with the
graphical evidence concurring with the results of the significance tests. In others, e.g. PM10 and
respiratory mortality, the evidence was less conclusive. In such cases the number of estimates
“generated” by the trim and fill technique were small and the revised summary estimates little
different to the originals.
Table 5. Original and revised summary relative risk estimates (for a 10 µg/m3 increase) for
selected pollutants and all-cause and cause-specific mortality. Revised estimates are calculated
using the “trim and fill” technique. The total number of estimates used in the meta-analysis is
indicated in bold.
1
Outcome/ Age
Disease
Summary
Estimate
PM10
BS
Ozone (8-hour)
All-Cause
All
Age
Original
(No. Estimates)
Revised
(No. Estimates)
1.006 (1.004, 1.008)
33
1.006 (1.004, 1.008)
33
1.006 (1.004, 1.008)
26
1.004 (1.002, 1.007)
33
1.003 (1.001, 1.004)
15
1.002 (1.000, 1.003)1
20
Respiratory
All
Age
Original
(No. Estimates)
Revised
(No. Estimates)
1.013 (1.005, 1.020)
18
1.010 (1.001, 1.018)
20
1.006 (0.998, 1.015)
18
0.999 (0.990, 1.008)
24
1.000 (0.996, 1.005)
12
0.999 (0.995, 1.004)
15
Cardiovascular
All
Age
Original
(No. Estimates)
Revised
(No. Estimates)
1.009 (1.005, 1.013)
17
1.005 (1.001, 1.010)
23
1.004 (1.002, 1.007)
18
1.004 (1.001, 1.006)
22
1.004 (1.003, 1.005)
13
1.004 (1.003, 1.005)
17
1.0020 (1.0005, 1.0035).
EUR/04/5042688
page 14
Table 6. Original and revised summary relative risk estimates (for a 10 µg/m3 increase) for
selected pollutants and respiratory hospital admissions. Revised estimates are calculated
using the “trim and fill” technique. The total number of estimates used in the
meta-analysis is indicated in bold.
Outcome/
Disease
Respiratory
Age
65+
Summary
Estimate
Original (No. Estimates)
Revised (No. Estimates)
PM10
1.007 (1.002, 1.013) 8
1.006 (1.000, 1.011) 10
BS
1.001 (0.993, 1.010) 6
1.001 (0.993, 1.009) 7
Figures 2–12 show the funnel plots for each of the eleven pollutant-outcome pairs. These plots
show the individual estimates plotted, as filled circles, against the reciprocal of the standard error
(measure of estimate precision). The estimates “generated” by the “trim and fill” technique are
shown as open diamonds. The original (long-dash line) and revised (short-dash line) summary
estimates are also shown.
As previously noted the detection and adjustment for asymmetry and possible publication bias is
not without its problems. There is evidence of asymmetry in most cases and that adjustment for
this asymmetry leads to smaller summary effect estimates. However, the overall conclusions
remain unaltered – that of small but statistically significant associations between air pollution
measures and indicators of daily mortality and morbidity.
Fig. 2. Funnel plot of estimates for all-cause mortality and PM10
Solid circles indicate original effect estimates plotted against the reciprocal of the standard error
(precision of the estimates). Open diamonds are the study estimates generated by the trim and fill
technique to make the funnel plot symmetrical. The long-dash line is the original summary
estimate and the short-dash line the revised (including the generated estimates) summary
estimate.
EUR/04/5042688
page 15
Fig. 3. Funnel plot of estimates for all-cause mortality and black smoke
Solid circles indicate original effect estimates plotted against the reciprocal of the standard error
(precision of the estimates). Open diamonds are the study estimates generated by the trim and fill
technique to make the funnel plot symmetrical. The long-dash line is the original summary
estimate and the short-dash line the revised (including the generated estimates) summary
estimate.
EUR/04/5042688
page 16
Fig. 4. Funnel plot of estimates for all-cause mortality and ozone
Solid circles indicate original effect estimates plotted against the reciprocal of the standard error
(precision of the estimates). Open diamonds are the study estimates generated by the trim and fill
technique to make the funnel plot symmetrical. The long-dash line is the original summary
estimate and the short-dash line the revised (including the generated estimates) summary
estimate.
EUR/04/5042688
page 17
Fig. 5. Funnel plot of estimates for respiratory mortality and PM10
Solid circles indicate original effect estimates plotted against the reciprocal of the standard error
(precision of the estimates). Open diamonds are the study estimates generated by the trim and fill
technique to make the funnel plot symmetrical. The long-dash line is the original summary
estimate and the short-dash line the revised (including the generated estimates) summary
estimate.
EUR/04/5042688
page 18
Fig. 6. Funnel plot of estimates for respiratory mortality and black smoke
Solid circles indicate original effect estimates plotted against the reciprocal of the standard error
(precision of the estimates). Open diamonds are the study estimates generated by the trim and fill
technique to make the funnel plot symmetrical. The long-dash line is the original summary
estimate and the short-dash line the revised (including the generated estimates) summary
estimate.
EUR/04/5042688
page 19
Fig. 7. Funnel plot of estimates for respiratory mortality and ozone
Solid circles indicate original effect estimates plotted against the reciprocal of the standard error
(precision of the estimates). Open diamonds are the study estimates generated by the trim and fill
technique to make the funnel plot symmetrical. The long-dash line is the original summary
estimate and the short-dash line the revised (including the generated estimates) summary
estimate.
EUR/04/5042688
page 20
Fig. 8. Funnel plot of estimates for cardiovascular mortality and PM10
Solid circles indicate original effect estimates plotted against the reciprocal of the standard error
(precision of the estimates). Open diamonds are the study estimates generated by the trim and fill
technique to make the funnel plot symmetrical. The long-dash line is the original summary
estimate and the short-dash line the revised (including the generated estimates) summary
estimate.
EUR/04/5042688
page 21
Fig. 9. Funnel plot of estimates for cardiovascular mortality and black smoke
Solid circles indicate original effect estimates plotted against the reciprocal of the standard error
(precision of the estimates). Open diamonds are the study estimates generated by the trim and fill
technique to make the funnel plot symmetrical. The long-dash line is the original summary
estimate and the short-dash line the revised (including the generated estimates) summary
estimate.
EUR/04/5042688
page 22
Fig. 10. Funnel plot of estimates for cardiovascular mortality and ozone
Solid circles indicate original effect estimates plotted against the reciprocal of the standard error
(precision of the estimates). Open diamonds are the study estimates generated by the trim and fill
technique to make the funnel plot symmetrical. The long-dash line is the original summary
estimate and the short-dash line the revised (including the generated estimates) summary
estimate.
EUR/04/5042688
page 23
Fig. 11. Funnel plot of estimates for respiratory hospital admissions and PM10
Solid circles indicate original effect estimates plotted against the reciprocal of the standard error
(precision of the estimates). Open diamonds are the study estimates generated by the trim and fill
technique to make the funnel plot symmetrical. The long-dash line is the original summary
estimate and the short-dash line the revised (including the generated estimates) summary
estimate.
EUR/04/5042688
page 24
Fig. 12. Funnel plot of estimates for respiratory hospital admissions and black smoke
Solid circles indicate original effect estimates plotted against the reciprocal of the standard error
(precision of the estimates). Open diamonds are the study estimates generated by the trim and fill
technique to make the funnel plot symmetrical. The long-dash line is the original summary
estimate and the short-dash line the revised (including the generated estimates) summary
estimate.
5.2.2 Panel studies
For the panel studies, there were seven pollutant-outcome pairs investigated, all of these relate to
children. The original and revised estimates as a result of “trim and fill” are given in Table 7.
There was no evidence of publication bias using either Begg’s or Egger’s test for any of the
combinations. The only combination where there was asymmetry which resulted in the “trim and
fill” technique “generating” new estimates was for black smoke and cough. This generated two
estimates that changed the random effects estimate from 1.001 (95% confidence interval 0.982,
1.021) to 0.999 (95% confidence interval 0.980, 1.019). However, for this outcome the
publication bias p-values for Begg’s and Egger’s tests are 0.975 and 0.650 respectively giving no
evidence to suspect publication bias.
There are only three significant outcome-pollutant combinations, two indicating adverse effects
of air pollution – lower respiratory symptoms and PM10 and peak expiratory flow rate (PEFR)
and PM10, the other being beneficial effects of air pollution, with upper respiratory symptoms
and PM10.
In conclusion there is no evidence of publication bias within the pollutant-outcome combinations
studied within the panel studies.
EUR/04/5042688
page 25
Table 7. Original and revised summary Odds ratio (beta for PEFR) estimates for a 10 µg/m3
increase for selected pollutants and child lung function and symptoms
Lung function/
symptom
Peak expiratory flow
rate
Cough
Lower respiratory
symptoms
Upper respiratory
symptoms
Medication use
Summary
Estimate
PM10
BS
Original
(No. Estimates)
Revised
(No. Estimates)
-0.085 (-0.136, -0.033) 41
NA
-0.085 (-0.136, -0.033) 41
NA
Original
(No. Estimates)
Revised
(No. Estimates)
0.999 (0.987, 1.011)
34
0.999 (0.987, 1.011)
34
1.001 (0.982, 1.021) 33
Original
(No. Estimates)
Revised
(No. Estimates)
1.008 (1.000, 1.016)
39
1.008 (1.000, 1.016)
39
NA
Original
(No. Estimates)
Revised
(No. Estimates)
0.997 (0.994, 0.999)
39
0.997 (0.994, 0.999)
39
NA
Original
(No. Estimates)
Revised
(No. Estimates)
1.005 (0.981, 1.029)
31
1.005 (0.981, 1.029)
31
1.008 (0.970, 1.049) 31
0.999 (0.980, 1.019) 35
NA
NA
1.008 (0.970, 1.049) 31
Revised estimates are calculated using the “trim and fill” technique. The total number of
estimates used in the meta-analysis is indicated in bold.
NA – Not Applicable – publication bias not conducted due to small numbers of studies
EUR/04/5042688
page 26
References
ANDERSON, H.R. ET AL. Particulate matter and daily mortality and hospital admissions in the
west midlands conurbation of the United Kingdom: associations with fine and coarse
particles, black smoke and sulphate. Occupational and Environmental Medicine, 58: 504–
510 (2001).
ANDERSON, H.R. ET AL. Publication bias in studies of ambient particulate pollution and daily
mortality. Epidemiology, 13: 394 (2002).
ATKINSON, R. W. ET AL. Short-term associations between emergency hospital admissions for
respiratory and cardiovascular disease and outdoor air pollution in London. Archives of
environmental health, 54: 398–411 (1999).
ATKINSON, R. W. ET AL. Acute effects of particulate air pollution on respiratory admissions –
Results from APHEA 2 project. American Journal of Respiratory and Critical Care
Medicine, 164: 1860–1866 (2001).
BEGG, C.B. & BERLIN, J.A. Publication bias: a problem in interpreting medical data. Journal of
the royal statistical society, 151: 419–463 (1988).
BEGG, C.B. & BERLIN, J.A. Publication bias and dissemination of clinical research. Journal of the
National Cancer Institute, 81:107–15 (1989).
BEGG, C.B. & MAZUMDAR M. Operating characteristics of a rank correlation test for Publication
Bias. Biometrics, 50: 1088–1101 (1994).
BREMNER, S.A. ET AL. Associations between various measures of particles and daily mortality in
the west midlands conurbation, United Kingdom. Epidemiology, 10: 257 (1999).
DER SIMONIAN, R. & LAIRD N. Meta-analysis in clinical trials. Controlled Clinical Trials, 7:
177–188 (1986).
DICKERSIN K. How important is publication bias? A synthesis of available data. AIDS education
and prevention, 9: 15–21 (1997).
DUVAL, S. & TWEEDIE, R. Trim and fill: A simple funnel-plot-based method of testing and
adjusting for publication bias in meta-analysis. Biometrics, 56(2): 455–463 (2000).
EGGER, M. ET AL. Bias in meta-analysis detected by a simple, graphical test. British medical
journal, 315: 629–634 (1997).
HEALTH EFFECTS INSTITUTE. Revised analyses of time-series studies of air pollution and health.
Special report. Health Effects Institute (2003).
KATSOUYANNI, K. ET AL. Confounding and effect modification in the short-term effects of
ambient particles on total mortality: Results from 29 European cities within the APHEA2
project. Epidemiology, 12: 521–531 (2001).
EUR/04/5042688
page 27
KRZYZANOWSKI, M. & WOJTYNIAK, B. Air pollution and daily mortality in Cracow. Public
Health Review, 19: 73–81 (1991).
LE TERTRE, A. ET AL. Short-term effects of particulate air pollution on cardiovascular disease in
eight European cities. Journal of epidemiology and community health, 56: 773–779 (2002).
LIGHT, R. J. & PILLEMER, D.B. Summing up: the science of reviewing research. Cambridge:
Harvard University Press, 1984.
MAHONEY, M.J. Publication predjudices: an experimental study of confirmatory bias in the peer
review system. Cognitive Therapy and Research, 1: 161–175 (1977).
Michelozzi, P. et al. [Acute effects of air pollution in Rome]. [Italian]. Annali dell’Istituto
superiore di sanita, 36: 297–304 (2000).
PEACOCK, J.L. ET AL. Publication bias in studies of PM10 and children’s lung function.
Epidemiology, 13: 391 (2002).
PETERS, A. ET AL. Associations between mortality and air pollution in Central Europe.
Environmental Health Perspectives, 108: 283–287 (2000).
PRESCOTT, G.J. ET AL. Urban air pollution and cardiopulmonary ill health: a 14.5 year time series
study. Occupational and environmental medicine, 55: 697–704 (1998).
ROEMER, W. ET AL. Pollution effects on asthmatic children in Europe, the PEACE study. Clinical
and experimental allergy, 30: 1067–1075 (2000).
SAMET, J.M. ET AL. Fine particulate air pollution and mortality in 20 US Cities, 1987-1994. New
England Journal of Medicine. 343: 1742–1749 (2000).
SIMES, R. J. Publication bias: the case for an international registry of clinical trials. Journal
clinical oncology, 4: 1529–1541 (1986).
SPIX, C. ET AL. Short-term effects of air pollution on hospital admissions of respiratory diseases
in Europe: a quantitative summary of APHEA study results. Air Pollution and Health: a
European Approach. Archives of environmental health, 53: 54–64 (1998).
STERLING, T.D. Publication decisions and their possible effects on inferences drawn from tests of
significance – or vice versa. Journal of the American statistical association. 54: 30–34
(1959).
WHO, Health aspects of air pollution with particulate matter, ozone and nitrogen dioxide.
Report on a WHO working group. WHO, Bonn, Germany, EUR/03/5042688,
http://www.euro.who.int/document/e79097.pdf. (2003).
WICHMANN, H. E. ET AL. Daily mortality and fine and ultrafine particles in Erfurt, Germany. Part
I: Role of particle number and particle mass. Health Effects Institute (2000).
EUR/04/5042688
page 28
Annex 1
MEMBERS OF THE WHO TASK GROUP
(AUTHORS ARE MARKED WITH AN ASTERIX)
Ben Armstrong
London School of Hygiene and Tropical Medicine, London, United
Kingdom
H. Ross Anderson*
St. George’s Hospital Medical School, London, United Kingdom
Richard Atkinson*
St. George’s Hospital Medical School, London, United Kingdom
Bert Brunekreef
Institute for Risk Assessment Sciences, University of Utrecht, Utrecht,
the Netherlands
Aaron Cohen
Health Effects Institute, Boston, United States of America
Klea Katsouyanni
Department of Hygiene and Epidemiology, University of Athens,
Athens, Greece
Kostas Konstantinou*
St. George’s Hospital Medical School, London, United Kingdom
Morton Lippmann
New York University School of Medicine Tuxedo, United States of
America
Louise Marston*
St. George’s Hospital Medical School, London, United Kingdom
Janet Peacock*
St. George’s Hospital Medical School, London, United Kingdom
Jordi Sunyer
Institut Municipal d’Investigacio Mèdica, Barcelona, Spain
Leendert van Bree
National Institute for Public Health and the Environment, Bilthoven,
the Netherlands
H. Erich Wichmann
GSF Institute of Epidemiology, Neuherberg, Germany
WHO Secretariat
Michal Krzyzanowski
WHO European Centre for Environment and Health, Bonn, Germany
Jürgen Schneider
WHO European Centre for Environment and Health, Bonn, Germany
EUR/04/5042688
page 29
Annex 2
MINUTES OF THE TASK GROUP MEETING IN LONDON
Background
The WHO project “Systematic Review of Health Aspects of Air Quality in Europe” aims to
provide the Clean Air for Europe (CAFE) programme of the European Commission (DG
Environment) with a systematic, periodic, scientifically independent review of the health aspects
of air quality in Europe.
As part of this review process WHO convened a working group, which reviewed specific
answers to a set of twelve questions in relation to the health effects of particulate matter, ozone
and nitrogen dioxide. The report of this working group provides a comprehensive description of
the hazards related to these pollutants, but no detailed guidance on risk assessment. Therefore,
the working group also recommended conducting as a follow up of this work a quantitative
meta-analysis of existing studies, which could subsequently inter alia be used for health impact
assessments. The analysis will use the bibliographic database developed at the St George’s
Hospital Medical School as the main framework, and will be performed by a small task group of
invited experts.
The meta-analysis will be used to update risk coefficients for selected health endpoints in
relation to the exposure to ozone and particulate matter.
The experts from St. George’s Hospital have prepared an interim report of their work. This
report was distributed among the members of the task group at the end of March and highlighted
a number of important questions to be answered by the task group in relation to the metaanalysis. Bert Brunekreef, Jordi Sunyer and Erich Wichmann, all members of the task group,
provided written comments to the questions in advance, since they could not attend the meeting
in London. The purpose of this meeting was therefore to review the progress of the metaanalysis, discuss any specific methodological issues identified by the task group members. The
meeting was also supposed to discuss approaches to risk assessment. As a basis for this
discussion, a proposal by IIASA on a methodology to perform an impact assessment of PM
related mortality was also forwarded to the members of the working group.
Summary of discussion; its conclusions and recommendations
Discussion of the purpose of the meta-analysis
It was emphasized that the purpose of the meta-analysis was to provide updated concentration
response (CR) functions for selected health outcomes for ozone and PM. These CR functions
should be available for subsequent health impact assessments (calculation of attributable cases),
but the process should also deepen the understanding of the relationship between exposure and
the health outcomes, including aspects such as heterogeneity of effects, uncertainties and effect
modifiers.
Discussion of meta-analysis of time-series and panel studies
Preliminary remark: The discussions of the task group were mainly focused on questions posed
in a preliminary report by St. George’s Hospital group. In answering the questions, the task
group tried to take into account time and capacity constraints. Therefore, some of the
EUR/04/5042688
page 30
recommendations do not only reflect the scientific judgement of the group, but also reflects the
priorities identified by the task group. (As a general approach, it was recommended to start with
a rather inclusive approach, and to subsequently classify input and to perform sensitivity
analyses.)
Is the number of estimates for a meta-analysis a relevant criterion in selecting studies for the
purpose of the health impact assessment?
No, but there is a minimum number to justify the meta-analysis (as a rule of thumb: this number
should be > 3).
Is the availability of base-rates relevant to the selection of the outcomes?
Yes, if the outcomes are to be used for subsequent health impact assessment. No, if the outcome
will be used for other applications.
Which outcomes should be included?
Daily number of deaths from all causes (excluding accidents, murders, etc.), all respiratory
disease and all cardiovascular disease. Calculations will be made for all ages; if a mortality study
does not provides an estimate for all ages but does for an elderly group (defined as 65+ or other
suitable age group) then they will be used instead.
Daily number of hospital admissions (incl. ED and ER admissions) for all respiratory diseases
(All ages; 0–14; 15–65; 65+) and for all cardiovascular disease (All ages; 65+); Asthma (0–14,
15–64) and COPD (65+). Sensitivity analysis will be included to test the potential influence of
ER and ED admissions compared to hospital emergency admissions (involving over night stay).
The other sensitivity analysis involved an assessment of a study’s ability to differentiate between
emergency and elective hospital admissions – do you get different relative risks from studies of
emergency hospital admissions compared to all hospital admissions (i.e. including elective
admissions).
ER/ED/A&E visits for respiratory causes (All ages; 0–14; 15–65; 65+).
Symptom exacerbations in asthmatics: Analysis of cough in children and adults separately,
medication use (both only to asthmatic subgroup applicable).
Sensitivity analyses would investigate effect of including estimates from what appeared to be
post-hoc subgroup analyses within studies.
Which pollutants should be included?
PM measured as PM10, PM2.5, black smoke, and coarse particles.
Ozone.
Which lags should be chosen?
It was decided to use the “selected” lag for the analyses and to conduct a sensitivity analysis to
assess the effect of using single-day lag versus a cumulative measure.
Which averaging time should be chosen?
For ozone, 8-hour average will be used at a first stage. The results from studies using 1 hour and
24 hours will be compared.
EUR/04/5042688
page 31
From which geographical areas should studies be selected?
It was decided to restrict the analysis to European studies. If not enough studies are available
(e.g. for PM2.5 or coarse fraction), these will be supplemented by studies from northern America.
If more than one study is available for a city/region, which one should be used?
Generally, the study that was published most recently should be used. However, exceptions to
this rule might be warranted, but have to be justified case by case.
To what extent can differing definition of a disease category, in terms of ICD codes, be
combined?
It was decided to allow all combinations, but to perform sensitivity analysis using more specific
diagnosis.
To what extent should different seasons be analysed?
Analysis should be performed for the entire year and in addition, summer only and winter only
(both ozone and PM).
Should results from multi-pollutant models be considered?
The group recommended to focus on single-pollutant models.
In addition, the Task Group added some more advice.
•
It was recommended to investigate the potential publication bias in estimates derived from
single-city studies. However, interpretation would have to be done very cautiously.
•
The level of heterogeneity should be assessed, taking into account expected variations and
calculating random-effect estimates. It was decided to dispense with the calculation of
fixed-effect estimates and to go straight to the calculation of random-effects estimates.
•
Unit risks should be used as intervals for summary estimates.
•
Some studies have been re-analyzed recently using different statistical methods to derive
effect estimates. Klea Katsouyanni was invited to prepare a proposal on how to handle
these studies by 23 April.
Approaches to risk assessment
The group reiterated the usefulness of both long-term and short-term studies for risk
assessments. There are currently no long-term studies on ozone showing convincing effects on
mortality. In addition, short-term studies are needed to identify the health impacts on PM- and
ozone-related morbidity. In contrast, PM-related mortality can be assessed more
comprehensively based on results from cohort studies (for a more detailed discussions see:
http://www.euro.who.int/document/e74256.pdf).
The outline of a methodology to estimate reduction of life expectation provided by IIASA was in
general welcomed and regarded as appropriate. However, there are a number of points that
would require a more deep discussion, including the following.
•
The treatment of uncertainty described in the report was regarded as not sufficient.
•
The motivation for the choice of the risk estimates should be discussed in more detail. Also
the consequences of this choice have to be made transparent (for example, the finding that
individuals with less than college education have an increased risk).
EUR/04/5042688
page 32
•
The consequences of the use of a different method for the calculation life expectancy than
the method described by Miller et al. should be investigated.
•
Secondary organic aerosols should be included in the atmospheric modelling, since they
can contribute significantly to the overall PM2.5 mass and there are indications that this part
is also critical from a health point of view.
WHO will get in contact with IIASA and propose a procedure for dealing with the issues
mentioned above.
In addition, the need was identified to develop a comprehensive approach to the estimation of
impacts using the concentration-response functions from time-series studies comparable to the
one IIASA has developed for the estimation of impacts on survival.
Follow-up
The St. George’s group is going to assess the work and prepare detailed plans for the work. The
plan will be forwarded to WHO. Depending on the plan, it might be necessary to further
prioritize the work. This will be done in close collaboration with WHO.
EUR/04/5042688
page 33
Annex 3
USE OF BIBLIOGRAPHIC DATABASE FOR SYSTEMATIC REVIEW
By Richard Atkinson, St. George’s Hospital Medical School, London, United Kingdom
METHOD
1.
Identification of time-series and panel studies
Three bibliographic databases were searched: Medline, Embase and Web of Science. Separate
search strings for each study type, time-series and panel, were used. These were tested against
known literature until we were satisfied that the search strings were sensitive enough to pick up
all relevant studies. The full reference and abstract for each of the citations identified by the
searches were downloaded from the source bibliographic databases into Reference Manager
(RM) databases, one for potential time-series studies and one for potential panel studies. Within
each of the RM databases the studies were assigned unique identification codes.
Papers already available to the academic department were checked for inclusion in the RM
databases. Citations in reviews of the published literature (such as the recent consultation
document on particles published by the United States Environmental Protection Agency) were
also checked to ensure that no relevant papers were missed.
The process of identifying time-series or panel studies from those selected by the search strings
comprised two stages. First, the abstracts of all studies were reviewed and obvious non-time
series and non-panel studies (e.g. clinical, mechanistic, exposure assessment) were removed
from the RM databases. In the second stage, copies of the remaining studies were obtained and
the time-series and panel studies identified.
Once the time-series and panel studies had been identified they were assigned a code within RM
indicating whether or not they provided usable numerical estimates of the effects of air pollution.
If they did not provide usable estimates then the reason(s) was also recorded. Studies were
classified as follows:
•
studies providing usable numerical estimates of the effects of air pollution;
•
studies providing numerical estimates that were unusable (e.g. because of inappropriate
statistical methods or insufficient data provided in the paper);
•
studies which did not provide numerical estimates for the effects of air pollution (e.g.
where the association between air pollution and health is assessed using a correlation
coefficient);
•
those studies which reviewed published literature;
•
those studies using existing data or simulated data to develop new analytical techniques;
•
others (letters, editorials, errata, meeting abstracts, case crossover and case control study
designs).
EUR/04/5042688
page 34
2.
Studies providing usable numerical estimates
For all time-series and panel studies providing usable regression estimates a number of items of
data were identified, recorded on a coding sheet and then entered into Access databases, one
containing details of results for all time-series studies and the other containing similar
information for all panel studies. These data described basic features of each study as well as
recording the regression coefficients, standard errors and the information necessary to calculate
standardized estimates of the health effects of each pollutant. Variables were also included that
described relevant elements of the analysis such as the length of the study period, year of study,
continent, average pollution levels, etc. General information about each study contained in the
RM databases (title, authors, journal reference, etc.) was also downloaded into the Access
databases. These study specific data were linked to the result specific data using the relational
features of the Access software.
3.
Studies providing unusable numerical estimates
A number of studies contained numerical estimates but were not included in the Access
databases. The reason(s) for their exclusion were coded in the RM databases and fell largely into
two categories, statistical method and data quality. The former included studies that did not
control for seasonality and other confounders adequately and the latter included studies that were
of a very limited period or a very small population (e.g. a single hospital).
4.
Presentation of results
In time-series studies, relative risks, regression estimates and percentage changes in the mean
number of events per day were all used to assess the association between the pollutants and
health outcomes. In order to make results comparable estimates from Poisson and log-linear
models (relative risks, regression estimates and percentage changes) were converted into a
standard metric: percentage change in the mean number of daily events associated with a
10 µg/m3 increase in the pollutant (100 mg/m3 increase for CO). Access queries were written to
calculate these adjusted estimates. Estimates from linear models were standardized to the change
in the number of events associated with 10 µg/m3 increases in the pollutant (100 mg/m3 increases
for CO). Where the logarithm of the pollutant was used in the model, the results were quoted for
a unit change in the pollutant level on the logarithmic scale – in other words, the number of
health events or percentage change in the number of health events associated with a doubling of
the pollutant level.
A similar process was undertaken for panel study results. Most studies using binary outcomes
used logistic regression and presented odds ratios. These have been converted to represent
10 µg/m3 increases in the pollutant. The results for continuous outcomes were usually given as
betas, sometimes as percentage change. These have been converted to betas for 10 µg/m3
increases in the pollutant. Results recorded as percentage change have been converted to betas
where this was possible (only a few cases). Units for lung function were standardized to litres (L)
or L/min as appropriate.
Access forms provide a user interface to the databases. They allow the user to select a set of the
results defined by outcome, disease, age group, pollutant etc. The standardized regression
estimates are calculated and then displayed using a “forest” plot. The estimates are assumed to
come from Poisson or log-linear models with linear terms for the pollutants. Results from other
model specifications or where a non-linear term for the pollutant was used are highlighted on the
plot.
EUR/04/5042688
page 35
5.
Selection of lags
Many studies investigated and reported results for a number of pollutant lags or days prior to the
health events. Some studies specified an a priori lag for investigation whilst others investigated a
number of lags and reported only those that had the largest (or largest positive) effect or were
statistically significant. It was desirable to be able to specify the lag for specific analyses but also
it was essential that a result for each outcome/pollutant combination from each study could be
easily selected for presentation without reference to a specified lag. For a given outcome defined
by event type (mortality/admission, etc.), disease group and age group and a given pollutant, a
single result was extracted and denoted as the “selected” result for that combination of outcome
and pollutant. The selection was made in priority order as follows:
Only one lag measure presented (this may be because only one was examined or only one was
presented in the paper).
Results for more than one lag presented. The lag selected was chosen as:
2.1
2.2
2.3
Lag focused on by author OR
Most statistically significant OR
Largest estimate.
In addition to this selected lag, results for lag 0 and lag 1 were recorded (if different to “selected”
lag from above process). A result for a cumulative lag (mean of pollution measures over 2 or
more days), chosen by criteria 2.1–2.3 above was also recorded when cumulative results were
available.
Some studies only provided results by season, that is, if no all-year analyses were undertaken. In
these cases the selection process described above applied to each season analysed. Where only
results from multi-pollutant models (two, three, four pollutants in a single statistical model) were
given then the results from the model with the most pollutants in it was selected for inclusion in
the Access database.
For panel studies a similar approach was used.
6.
Multicity studies
A number of recent studies have presented meta-analyses of results from several locations. As
well as presenting results from each location, summary estimates have been calculated. Where
such studies have used previously published data only the summary estimates have been
recorded. Where previously unpublished city-specific results are presented they have been
recorded separately.
7.
Summary estimates
Regression estimates and standard errors for each group of studies were transferred into STATA
where standard procedures within STATA were used to calculate fixed- and random-effects
summary estimates.
EUR/04/5042688
page 36
Annex 4
TABLES OF INDIVIDUAL CITY RESULTS – TIME-SERIES
Table A1. All-cause mortality, PM10
Reference
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
City
Country
Study period
ICD
group
Lag
%∆
%LCL
%UCL
Beta
SE
RR ∆
RR LCL
RR UCL
mean/
median
Athens
Greece
1992–1996
<800
lag 0–1
1.55
0.98
2.11
0.01534
0.00284
1.01546
1.00982
1.02114
40
Barcelona
Spain
1991–1996
<800
lag 0–1
0.93
0.57
1.30
0.00928
0.00185
1.00932
1.00567
1.01299
60
Basel
Switzerland
1990–1995
<800
lag 0–1
0.41
–0.44
1.28
0.00412
0.00436
1.00413
0.99558
1.01275
28
Birmingham, West
Midlands
United
Kingdom
1992–1996
<800
lag 0–1
0.28
–0.23
0.80
0.00282
0.00262
1.00282
0.99768
1.00799
21
Budapest
Hungary
1992–1995
<800
lag 0–1
0.29
–0.61
1.20
0.00289
0.00462
1.00289
0.99385
1.01201
40
Cracow
Poland
1990–1996
<800
lag 0–1
0.13
–0.54
0.82
0.00135
0.00346
1.00135
0.99458
1.00816
54
Erfurt
Germany
1991–1995
<800
lag 0–1
–1.33
0.21
0.00394
0.99438
0.98673
1.00208
48
Geneva
Switzerland
1990–1995
<800
lag 0–1
–1.01
0.82
0.00468
0.99897
0.98986
1.00817
33
Helsinki
Finland
1993–1996
<800
lag 0–1
0.32
–0.51
1.17
0.00324
0.00427
1.00324
0.99488
1.01167
23
London
United
Kingdom
1992–1996
<800
lag 0–1
0.69
0.35
1.04
0.00691
0.00175
1.00694
1.00349
1.01040
25
Lyon
France
1993–1997
<800
lag 0–1
1.36
0.31
2.42
0.01353
0.00531
1.01362
1.00313
1.02423
39
Madrid
Spain
1992–1995
<800
lag 0–1
0.53
0.07
1.00
0.00531
0.00238
1.00532
1.00065
1.01002
33
Milan
Italy
1990–1996
<800
lag 0–1
1.17
0.79
1.54
0.01160
0.00189
1.01167
1.00794
1.01542
47
Paris
France
1991–1996
<800
lag 0–1
0.43
–0.02
0.88
0.00427
0.00230
1.00428
0.99976
1.00881
22
Prague
Czech
Republic
1992–1996
<800
lag 0–1
0.12
–0.24
0.48
0.00122
0.00183
1.00122
0.99763
1.00482
66
Rome
Italy
1992–1996
<800
lag 0–1
1.29
0.76
1.83
0.01283
0.00270
1.01292
1.00757
1.01829
57
–
0.56
–
0.10
–
0.00564
–
0.00103
EUR/04/5042688
page 37
Reference
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Zeghnoun et
al. 2001
Zeghnoun et
al. 2001
Zeghnoun et
al. 2001
Biggeri et al.
2001
Biggeri et al.
2001
Biggeri et al.
2001
Roemer et al.
2001
Peters et al.
2000
Daponte et al.
1999
Spix et al.,
1996
Hoek et al.,
2000
Ocana–Riola
et al. 1999
City
Country
Study period
ICD
group
Lag
%∆
%LCL
%UCL
Beta
SE
RR ∆
RR LCL
RR UCL
mean/
median
Stockholm
Sweden
1990–1996
<800
lag 0–1
0.39
–1.29
2.10
0.00389
0.00863
1.00390
0.98706
1.02102
14
Tel Aviv
Israel
1991–1996
<800
lag 0–1
0.64
0.13
1.15
0.00641
0.00259
1.00643
1.00134
1.01154
43
Teplice
Slovakia
1990–1997
<800
lag 0–1
0.64
–0.03
1.32
0.00641
0.00344
1.00643
0.99966
1.01325
42
Torino
Italy
1990–1996
<800
lag 0–1
1.05
0.72
1.39
0.01046
0.00169
1.01052
1.00717
1.01388
65
Zurich
Switzerland
1990–1995
<800
lag 0–1
0.43
–0.30
1.16
0.00424
0.00370
1.00425
0.99701
1.01155
28
Le Havre
France
1990–1995
<800
lag 1
0.79
–0.34
1.93
0.00788
0.00573
1.00791
0.99664
1.01929
30.8
Rouen
France
1990–1995
<800
lag 1
0.24
–0.54
1.03
0.00242
0.00397
1.00242
0.99464
1.01026
27.7
Strasbourg
France
1990–1995
<800
lag 2
0.60
–0.50
1.71
0.00596
0.00561
1.00598
0.99499
1.01710
29
Bologna
Italy
1996–1998
<800
lag 0–1
0.90
–0.10
1.91
0.00896
0.00508
1.00900
0.99900
1.01910
41.2
Florence
Italy
1996–1998
<800
lag 0–1
1.00
–0.30
2.32
0.00995
0.00661
1.01000
0.99700
1.02317
40.3
Palermo
Italy
1997–1999
<800
lag 0–1
3.30
2.20
4.41
0.03247
0.00546
1.03300
1.02200
1.04412
42.9
Amsterdam
Netherlands
1987–1998
lag 1
0.27
–0.13
0.67
0.00266
0.00203
1.00267
0.99869
1.00666
34
Czech Republic
Czech
Republic
1982–1994
<800
lag 1
0.94
0.07
1.82
0.00935
0.00441
1.00939
1.00070
1.01816
45
Huelva
Spain
1993–1996
<800
lag 0
2.49
–0.21
5.26
0.02460
0.01362
1.02490
0.99790
1.05263
40
Koln
Germany
1975–1985
lag 1
0.36
–0.02
0.75
0.00361
0.00196
1.00362
0.99978
1.00747
34
Netherlands
Netherlands
1986–1994
<800
lag 1
0.18
0.03
0.33
0.00178
0.00076
1.00179
1.00030
1.00327
34
Seville
Spain
1992–1996
<800
lag 5
–
1.99
–3.23
–0.74
–
0.02013
0.00650
0.98007
0.96766
0.99264
42.68
EUR/04/5042688
page 38
Table A2. Cardiovascular mortality, PM10
Reference
Biggeri et al.
2001
Biggeri et al.
2001
Biggeri et al.
2001
Biggeri et al.
2001
Biggeri et al.
2001
Biggeri et al.
2001
Ocana–Riola
et al. 1999
Galan et al.
1999
Daponte et al.
1999
Zeghnoun et
al. 2001
Zeghnoun et
al. 2001
Zeghnoun et
al. 2001
Zeghnoun et
al. 2001
Anderson et
al. 2001
Bremner et al.
1999
Wichmann et
al. 2000
Hoek et al.
2001
City
Country
Study period
ICD
group
Lag
%∆
%LCL
%UCL
Beta
SE
RR ∆
RR LCL
RR UCL
mean/
media
n
Bologna
Italy
1996–1998
390–459
lag 0–1
1.30
–0.30
2.93
0.0129162
0.008123
1.013
0.997
1.0292568
41.2
Florence
Italy
1996–1998
390–459
lag 0–1
1.50
–0.50
3.54
0.0148886
0.010154
1.015
0.995
1.035402
40.3
Milan
Italy
1995–1997
390–459
lag 0–1
0.40
–0.70
1.51
0.003992
0.005621
1.004
0.993
1.0151219
45.2
Palermo
Italy
1997–1999
390–459
lag 0–1
3.50
1.80
5.23
0.0344014
0.00845
1.035
1.018
1.0522839
42.9
Rome
Italy
1995–1997
390–459
lag 0–1
1.80
0.70
2.91
0.0178399
0.005543
1.018
1.007
1.0291202
59
Turin
Italy
1995–1998
390–459
lag 0–1
0.70
0.00
1.40
0.0069756
0.003559
1.007
1
1.014049
63.8
–3.31
0.55
–0.01409
0.01
0.98601
0.966871
1.0055252
42.68
Seville
Spain
1992–1996
390–459
lag 5
–
1.40
Madrid
Spain
1992–1995
390–459
lag 0
0.91
0.15
1.68
0.0090588
0.003857
1.0091
1.0015
1.0167577
32.8
Huelva
Spain
1993–1996
390–459
lag 5
3.05
–1.15
7.43
0.0300441
0.02123
1.0305
0.9885
1.0742845
40
Le Havre
France
1990–1995
390–459
lag 1
2.55
0.04
5.12
0.025169
0.012628
1.02549
1.000418
1.0511868
30.8
Paris
France
1990–1995
390–459
lag 2
0.86
0.13
1.60
0.0086108
0.003714
1.00865
1.001333
1.0160165
22
Rouen
France
1990–1995
390–459
lag 1
1.06
–0.29
2.43
0.0105638
0.00688
1.01062
0.997083
1.0243406
27.7
Strasbourg
France
1990–1995
390–459
lag 3
2.37
0.25
4.54
0.0234418
0.010688
1.02372
1.002497
1.0453898
29
1994–1996
390–459
lag 0–1
0.41
–0.78
1.61
0.004078
0.006092
1.00409
0.992169
1.0161468
20
1992–1994
390–459
lag 1
0.55
–0.07
1.17
0.0054909
0.003134
1.00551
0.999348
1.0117019
24.8
lag 0
0.79
–0.69
2.29
0.0078561
0.007541
1.00789
0.993099
1.0228956
31
lag 0–6
0.15
–0.20
0.50
0.0014911
0.001789
1.00149
0.997986
1.0050108
West Midlands
London
United
Kingdom
United
Kingdom
Erfurt
Germany
1995–1998
Netherlands
Netherlands
1986–1994
390–448
EUR/04/5042688
page 39
Table A3. Respiratory mortality, PM10
Reference
Biggeri et al.
2001
Biggeri et al.
2001
Biggeri et al.
2001
Biggeri et al.
2001
Biggeri et al.
2001
Biggeri et al.
2001
Daponte et al.
1999
Galan et al.
1999
Ocana–Riola
et al. 1999
Zeghnoun et
al. 2001
Zeghnoun et
al. 2001
Zeghnoun et
al. 2001
Zeghnoun et
al. 2001
Wichmann et
al. 2000
Krzyzanowski
et al. 1991
Bremner et al.
1999
Zmirou et al.,
1996
Anderson et
al. 2001
RR LCL
RR UCL
mean/m
edian
0.02012
–0.05300 –0.09000
–0.01451
41.2
–0.01207
0.02541
–0.02200 –0.07000
0.02845
40.3
6.77
0.04018
0.01290
0.03100
0.00500
0.05767
45.2
5.00
12.53
0.08342
0.01767
0.07700
0.04000
0.11530
42.9
3.10
0.10
6.19
0.03053
0.01507
0.02100
–0.00900
0.05190
59
lag 0–1
1.50
–0.20
3.23
0.01489
0.00862
0.00500
–0.01200
0.02229
63.8
460–519
lag 3
7.65
–0.64
16.63
0.07372
0.04089
0.06650
–0.01640
0.15632
40
1992–1995
460–519
lag 1
0.80
–0.56
2.18
0.00797
0.00693
–0.00200 –0.01560
0.01179
32.8
Spain
1992–1996
460–519
lag 2
–2.53
–6.37
1.46
–0.02565
0.02050
–0.03532 –0.07371
0.00464
42.68
Le Havre
France
1990–1995
460–519
lag 2
2.02
–1.82
6.02
0.02002
0.01959
0.01022
–0.02822
0.05016
30.8
Paris
France
1990–1995
460–519
lag 1
0.07
–1.40
1.56
0.00067
0.00756
–0.00933 –0.02405
0.00560
22
Strasbourg
France
1990–1995
460–519
lag 3
2.32
–1.87
6.69
0.02296
0.02133
0.01323
–0.02867
0.05692
29
Rouen
France
1990–1995
460–519
lag 0–1
1.78
–0.58
4.20
0.01764
0.01199
0.00779
–0.01584
0.03199
27.7
Erfurt
Germany
1995–1998
lag 0
2.92
0.61
5.28
0.02879
0.01158
0.01920
–0.00390
0.04283
31
Krakow
Poland
1977–1989
lag 1–4
0.58
–0.10
1.26
0.00576
0.00346
–0.00422 –0.01102
0.00258
London
United Kingdom
1992–1994
460–519
lag 3
1.29
0.29
2.29
0.01278
0.00503
0.00286
–0.00708
0.01289
24.8
Lyon
France
1985–1990
460–519
lag 0
0.79
0.00
1.58
0.00784
0.00400
–0.00213 –0.01000
0.00581
38.1
West Midlands
United Kingdom
1994–1996
460–519
lag 0–1
–0.58
–2.50
1.39
–0.00578
0.00999
–0.01576 –0.03504
0.00390
20
City
Country
Study period
ICD group
Lag
%∆
%LCL
%UCL
Beta
SE
Bologna
Italy
1996–1998
460–519
lag 0–1
–4.30
–8.00
–0.45
–0.04395
Florence
Italy
1996–1998
460–519
lag 0–1
–1.20
–6.00
3.85
Milan
Italy
1995–1997
460–519
lag 0–1
4.10
1.50
Palermo
Italy
1997–1999
460–519
lag 0–1
8.70
Rome
Italy
1995–1997
460–519
lag 0–1
Turin
Italy
1995–1998
460–519
Huelva
Spain
1993–1996
Madrid
Spain
Seville
RR ∆
EUR/04/5042688
page 40
Table A4. Admissions, PM10
Reference
City
All respiratory, ages 65+
Atkinson et
Barcelona
al. 2001
Atkinson et
Birmingham, West
al. 2001
Midlands
Atkinson et
London
al. 2001
Atkinson et
Netherlands
al. 2001
Atkinson et
Paris
al. 2001
Atkinson et
Stockholm
al. 2001
Prescott et
Edinburgh 1
al. 1998
Michelozzi
Rome
et al. 2000
All respiratory, ages 15–64
Atkinson et
London
al. 1999
Anderson et
West Midlands
al. 2001
Michelozzi
Rome
et al. 2000
All respiratory, ages 0–14
Atkinson et
London
al. 1999
Anderson et
West Midlands
al. 2001
Michelozzi
Rome
et al. 2000
Country
Study period
ICD group
Lag
%∆
%LCL
%UCL
Beta
SE
RR ∆
RR LCL
RR UCL
mean/
median
Spain
1994–1996
460–519
lag 0–1
2.00
0.80
3.21
0.01980
0.00604
1.02000
1.00800
1.03214
53.3
1992–1994
460–519
lag 0–1
0.90
–0.30
2.11
0.00896
0.00610
1.00900
0.99700
1.02114
21.5
1992–1994
460–519
lag 0–1
0.40
–0.30
1.10
0.00399
0.00357
1.00400
0.99700
1.01105
24.9
Netherlands
1992–1995
460–519
lag 0–1
1.20
0.70
1.70
0.01193
0.00253
1.01200
1.00700
1.01702
33.4
France
1992–1996
460–519
lag 0–1
–
0.10
–1.30
1.11
–
0.00100
0.00617
0.99900
0.98700
1.01115
20.1
Sweden
1994–1996
460–519
lag 0–1
1.70
–1.20
4.69
0.01686
0.01476
1.01700
0.98800
1.04685
13.6
United
Kingdom
1981–1995
480–487,
490–496
lag 1–3
2.10
–3.80
8.36
0.02078
0.03037
1.02100
0.96200
1.08362
20.7
–0.95
0.70
–
0.00130
0.00423
0.99871
0.99046
1.00702
United
Kingdom
United
Kingdom
1992–1997
460–519
lag 0
–
0.13
1992–1994
460–519
lag 2
1.36
0.41
2.32
0.01353
0.00482
1.01362
1.00409
1.02324
24.8
1994–1996
460–519
lag 0–1
0.04
–1.66
1.77
0.00041
0.00874
1.00041
0.98341
1.01770
20
1992–1997
460–519
lag 0
0.47
–0.56
1.52
0.00472
0.00528
1.00473
0.99438
1.01519
1992–1994
460–519
lag 1
1.55
0.67
2.45
0.01543
0.00447
1.01555
1.00670
1.02447
24.8
1994–1996
460–519
lag 0–1
1.58
0.25
2.93
0.01568
0.00675
1.01580
1.00245
1.02933
20
Italy
1992–1997
460–519
lag 0
–
0.22
–1.39
0.97
–
0.00216
0.00605
0.99784
0.98608
1.00974
Italy
United
Kingdom
United
Kingdom
Italy
United
Kingdom
United
Kingdom
Cardiovascular, ages 65+
Prescott et
al. 1998
Edinburgh 1
United
Kingdom
1981–1995
410–414,
426–429,
434–440
lag 1–3
4.80
0.90
8.85
0.04688
0.01935
1.04800
1.00900
1.08851
20.7
Atkinson et
al. 1999
London
United
Kingdom
1992–1994
390–459
lag 0
0.50
–0.04
1.04
0.00495
0.00274
1.00496
0.99958
1.01037
24.8
EUR/04/5042688
page 41
Table A5. All–cause mortality, black smoke
Reference
Arribas et al.
1999
Perez Boillos
et al. 1999
Taracido et al.
1999
Aguinaga et
al. 1999
Bellido Blasco
et al. 1999
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Katsouyanni
et al., 2001
Roemer et al.
2001
City
Country
Study
period
ICD
group
Lag
%∆
%LCL
%UCL
Beta
SE
RR ∆
RR LCL
RR UCL
mean/
median
Saragossa
Spain
1991–1995
<800
lag 1
2.80
0.60
5.05
0.02762
0.01104
1.02800
1.00600
1.05048
44
Vitoria–
Gasteiz
Spain
1990–1994
<800
lag 1
0.63
–0.32
1.59
0.00628
0.00484
1.00630
0.99680
1.01589
45
Vigo
Spain
1991–1994
<800
lag 5
–0.40
–1.06
0.26
–0.00401
0.00339
0.99600
0.98940
1.00264
98.13
Pamplona
Spain
1991–1995
<800
lag 0
2.98
–1.88
8.09
0.02941
0.02470
1.02985
0.98119
1.08092
21.67
Castellon
Spain
1991–1995
<800
lag 2
1.51
–0.50
3.56
0.01499
0.01020
1.01510
0.99500
1.03561
20.3
Athens
Greece
1992–1996
<800
lag 0–1
0.66
0.43
0.89
0.00655
0.00117
1.00657
1.00426
1.00888
64
Barcelona
Spain
1991–1996
<800
lag 0–1
1.58
1.04
2.13
0.01570
0.00273
1.01583
1.01040
1.02129
39
Bilbao
Spain
1992–1996
<800
lag 0–1
0.82
–0.67
2.32
0.00813
0.00757
1.00817
0.99331
1.02324
23
Birmingham,
West
Midlands
United
Kingdom
1992–1996
<800
lag 0–1
0.34
–0.59
1.28
0.00342
0.00475
1.00342
0.99413
1.01280
11
Cracow
Poland
1990–1996
<800
lag 0–1
–0.21
–0.62
0.21
–0.00207
0.00212
0.99793
0.99379
1.00209
36
Dublin
Ireland
1990–1996
<800
lag 0–1
1.04
0.09
2.00
0.01038
0.00483
1.01043
1.00092
1.02004
10
Ljubljana
Slovenia
1992–1996
<800
lag 0–1
–0.09
–1.27
1.11
–0.00087
0.00609
0.99913
0.98728
1.01113
13
Lodz
Poland
1990–1996
<800
lag 0–1
–0.06
–0.47
0.36
–0.00058
0.00211
0.99942
0.99530
1.00356
30
London
United
Kingdom
1992–1996
<800
lag 0–1
0.93
0.34
1.53
0.00929
0.00300
1.00933
1.00341
1.01529
11
Marseille
France
1990–1995
<800
lag 0–1
1.08
0.37
1.80
0.01073
0.00361
1.01078
1.00365
1.01796
34
Paris
France
1991–1996
<800
lag 0–1
0.38
0.10
0.67
0.00383
0.00146
1.00383
1.00096
1.00672
21
Poznan
Poland
1990–1996
<800
lag 0–1
0.63
0.16
1.10
0.00624
0.00239
1.00626
1.00156
1.01098
23
Valencia
Spain
1994–1996
<800
lag 0–1
1.35
0.36
2.35
0.01342
0.00499
1.01351
1.00364
1.02348
40
Wroclaw
Poland
1990–1996
<800
lag 0–1
0.28
–0.16
0.73
0.00282
0.00228
1.00283
0.99835
1.00732
33
Amsterdam
Netherlands
1987–1998
lag 1
3.30
1.43
5.19
0.03243
0.00928
1.03296
1.01434
1.05192
9
EUR/04/5042688
page 42
Reference
Hoek et al.
2000
Hoek et al.
1997
Prescott et al.
1998
Le Tertre et al.
2002
Le Tertre et al.
2002
Le Tertre et al.
2002
City
Country
Study
period
ICD
group
Lag
%∆
%LCL
%UCL
Beta
SE
RR ∆
RR LCL
RR UCL
mean/
median
Netherlands
Netherlands
1986–1994
<800
lag 1
0.40
0.20
0.59
0.00396
0.00101
1.00397
1.00199
1.00595
10
Rotterdam
Netherlands
1983–1991
all
lag 2
0.90
0.00
1.80
0.00891
0.00455
1.00895
1.00000
1.01799
13
Edinburgh 1
United
Kingdom
1981–1995
<900
lag 1–3
1.50
0.50
2.51
0.01489
0.00505
1.01500
1.00500
1.02510
8.7
Bordeaux
France
1990–1995
<800
lag 0–1
1.53
0.00
3.09
0.01521
0.00776
1.01532
1.00000
1.03088
Le Havre
France
1990–1995
<800
lag 0–1
0.24
–1.46
1.97
0.00239
0.00873
1.00239
0.98538
1.01969
Rouen
France
1990–1995
<800
lag 0–1
0.14
–1.00
1.29
0.00140
0.00584
1.00140
0.99000
1.01292
EUR/04/5042688
page 43
Table A6. Cardiovascular mortality, black smoke
Reference
Le Tertre et
al. 2002
Le Tertre et
al. 2002
Le Tertre et
al. 2002
Le Tertre et
al. 2002
Le Tertre et
al. 2002
Wojtyniak
et al. 1996
Wojtyniak
et al. 1996
Wojtyniak
et al. 1996
Wojtyniak
et al. 1996
Bremner et
al. 1999
Anderson et
al. 2001
Hoek et al.
2001
Aguinaga et
al. 1999
Bellido
Blasco et
al. 1999
Cambra et
al. 1999
Arribas–
Monzon et
al. 2001
Garcia–
Aymerich et
al. 2000
Tenias
Burillo et al.
1999
City
Country
Study
period
ICD group
Lag
%∆
%LCL
%UCL
Beta
SE
RR ∆
RR LCL
RR UCL
Bordeaux
France
1990–1995
390–459
lag 0–1
1.76
–0.73
4.31
0.01742
0.01263
1.01757
0.99269
1.04307
Le Havre
France
1990–1995
390–459
lag 0–1
1.40
–1.61
4.50
0.01391
0.01538
1.01400
0.98389
1.04504
Marseille
France
1990–1995
390–459
lag 0–1
0.92
–0.24
2.10
0.00919
0.00592
1.00923
0.99759
1.02100
Paris
France
1990–1995
390–459
lag 0–1
0.40
–0.24
1.04
0.00396
0.00325
1.00397
0.99759
1.01039
Rouen
France
1990–1995
390–459
lag 0–1
0.98
–1.06
3.07
0.00976
0.01043
1.00981
0.98938
1.03066
Krakow
Poland
1977–1989
390–459
lag 0
0.14
–0.19
0.47
0.00143
0.00168
1.00144
0.99814
1.00474
73.3
Lodz
Poland
1977–1990
390–459
lag 2
0.13
–0.20
0.45
0.00128
0.00165
1.00128
0.99804
1.00452
57.3
Poznan
Poland
1983–1990
390–459
lag 2
–0.20
–0.79
0.39
–0.00198
0.00302
0.99802
0.99212
1.00395
34
Wroclaw
Poland
1979–1989
390–459
lag 1
0.13
–0.36
0.63
0.00133
0.00252
1.00133
0.99641
1.00628
54.3
1992–1994
390–459
lag 1
1.18
–0.12
2.49
0.01169
0.00660
1.01176
0.99876
1.02493
10.8
1994–1996
390–459
lag 0–1
0.90
–0.90
2.72
0.00892
0.00917
1.00896
0.99099
1.02725
10.9
London
West Midlands
United
Kingdom
United
Kingdom
mean/
median
Netherlands
Netherlands
1986–1994
390–448
lag 0–6
0.72
0.32
1.11
0.00715
0.00200
1.00717
1.00323
1.01113
Pamplona
Spain
1991–1995
390–459
lag 5
–2.32
–9.94
5.93
–0.02351
0.04140
0.97676
0.90064
1.05931
21.67
Castellon
Spain
1991–1995
390–459
lag 2
3.48
0.50
6.55
0.03421
0.01491
1.03480
1.00500
1.06548
20.3
Bilbao
Spain
1992–1996
390–459
lag 4
–1.65
–3.64
0.38
–0.01664
0.01043
0.98350
0.96360
1.00381
23.09
Zaragoza
Spain
1991–1995
390–459
lag 1
0.66
–0.49
1.82
0.00658
0.00586
1.00660
0.99510
1.01823
Barcelona
Spain
1985–1989
390–459
lag 0–3
1.15
0.38
1.94
0.01147
0.00393
1.01153
1.00377
1.01935
42.4
Valencia
Spain
1994–1996
lag 1
0.95
–0.51
2.43
0.00946
0.00743
1.00950
0.99490
1.02431
44.2
EUR/04/5042688
page 44
Table A7. Respiratory mortality, black smoke
Reference
Le Tertre et al.
2002
Le Tertre et al.
2002
Le Tertre et al.
2002
Le Tertre et al.
2002
Le Tertre et al.
2002
Wojtyniak et
al. 1996
Wojtyniak et
al. 1996
Wojtyniak et
al. 1996
Wojtyniak et
al. 1996
Garcia–
Aymerich et
al. 2000
Bremner et al.
1999
Tenias Burillo
et al. 1999
Arribas–
Monzon et al.
2001
Aguinaga et
al. 1999
Bellido Blasco
et al. 1999
Cambra et al.
1999
Prescott et al.
1998
Anderson et
al. 2001
City
Country
Study
period
ICD group
Lag
%∆
%LCL
%UCL
Beta
SE
RR ∆
RR LCL
RR UCL
Bordeaux
France
1990–1995
460–519
lag 0–1
2.00
–3.63
7.96
0.01979
0.02899
1.01999
0.96365
1.07961
Le Havre
France
1990–1995
460–519
lag 0–1
2.56
–3.31
8.80
0.02533
0.03011
1.02565
0.96688
1.08800
Marseille
France
1990–1995
460–519
lag 0–1
2.64
0.18
5.16
0.02603
0.01237
1.02637
1.00179
1.05155
Paris
France
1990–1995
460–519
lag 0–1
–0.22
–1.50
1.08
–0.00221
0.00661
0.99779
0.98495
1.01079
Rouen
France
1990–1995
460–519
lag 0–1
0.67
–3.24
4.74
0.00669
0.02024
1.00671
0.96756
1.04744
Krakow
Poland
1977–1989
460–519
lag 1
–0.21
–1.34
0.94
–0.00209
0.00583
0.99791
0.98658
1.00938
73.3
Lodz
Poland
1977–1990
460–519
lag 1
–0.84
–1.89
0.21
–0.00849
0.00539
0.99155
0.98113
1.00208
57.3
Poznan
Poland
1983–1990
460–519
lag 0
–0.98
–2.76
0.83
–0.00984
0.00925
0.99021
0.97242
1.00833
34
Wroclaw
Poland
1979–1989
460–519
lag 1
–1.88
–3.39
–0.34
–0.01899
0.00793
0.98119
0.96605
0.99657
54.3
Barcelona
Spain
1985–1989
460–519
lag 0–3
1.00
–0.51
2.53
0.00995
0.00766
1.01000
0.99495
1.02527
42.4
London
United
Kingdom
1992–1994
460–519
lag 3
1.91
0.25
3.61
0.01896
0.00841
1.01914
1.00248
1.03608
10.8
Valencia
Spain
1994–1996
lag 3
–1.89
–4.81
1.12
–0.01908
0.01542
0.98110
0.95190
1.01120
44.2
Zaragoza
Spain
1991–1995
460–519
lag 1
2.89
0.62
5.21
0.02849
0.01138
1.02890
1.00620
1.05211
Pamplona
Spain
1991–1995
460–519
lag 1
13.36
–3.87
33.67
0.12540
0.08410
1.13360
0.96133
1.33674
21.67
Castellon
Spain
1991–1995
460–519
lag 4
3.64
–2.57
10.25
0.03575
0.03153
1.03640
0.97430
1.10246
20.3
Bilbao
Spain
1992–1996
460–519
lag 1
2.98
–1.11
7.24
0.02936
0.02068
1.02980
0.98890
1.07239
23.09
1981–1995
480–487,
490–496
lag 1–3
3.90
1.10
6.78
0.03826
0.01394
1.03900
1.01100
1.06778
8.7
1994–1996
460–519
lag 0–1
0.06
–2.90
3.11
0.00060
0.01533
1.00060
0.97097
1.03113
10.9
Edinburgh 1
West
Midlands
United
Kingdom
United
Kingdom
mean/
median
EUR/04/5042688
page 45
Table A8. Admissions, black smoke
Reference
City
Country
Study period
ICD group
Lag
%∆
%LCL
%UCL
Beta
SE
RR ∆
RR LCL
RR UCL
mean/
median
All respiratory, ages 65+, hospital admissions
Prescott et
al. 1998
Atkinson et
al. 2001
Atkinson et
al. 2001
Atkinson et
al. 2001
Atkinson et
al. 2001
Atkinson et
al. 2001
Edinburgh 2
United Kingdom
1992–1995
480–487,
490–496
lag 1–3
3.10
–3.50
10.15
0.03053
0.03375
1.03100
0.96500
1.10151
8.7
Barcelona
Spain
1994–1996
460–519
lag 0–1
–
0.70
–2.30
0.93
–0.00702
0.00829
0.99300
0.97700
1.00926
36.2
Birmingham,
West Midlands
United Kingdom
1992–1994
460–519
lag 0–1
2.90
0.60
5.25
0.02859
0.01153
1.02900
1.00600
1.05253
11.5
London
United Kingdom
1992–1994
460–519
lag 0–1
–
1.10
–2.40
0.22
–0.01106
0.00675
0.98900
0.97600
1.00217
11.3
Netherlands
Netherlands
1989–1995
460–519
lag 0–1
0.00
–0.70
0.70
0.00000
0.00358
1.00000
0.99300
1.00705
9.1
Paris
France
1992–1996
460–519
lag 0–1
0.50
–0.40
1.41
0.00499
0.00459
1.00500
0.99600
1.01408
18.6
460–519
single
0.55
0.12
0.99
0.00552
0.00221
1.00554
1.00120
1.00990
1994–1996
460–519
lag 0–1
0.72
–1.87
3.37
0.00714
0.01327
1.00717
0.98132
1.03370
10.9
All respiratory, ages 15–64, hospital admissions
Spix et al.
1998
Amsterdam,
London, Paris,
Rotterdam
Europe
Anderson,
et al. 2001
West Midlands
United Kingdom
All respiratory, ages 0–14, hospital admissions
Atkinson, et
al. 1999
Anderson,
et al. 2001
London
United Kingdom
1992–1994
460–519
lag 0
1.08
–0.35
2.52
0.01071
0.00725
1.01077
0.99652
1.02523
10.8
West Midlands
United Kingdom
1994–1996
460–519
lag 0–1
2.32
0.42
4.25
0.02291
0.00956
1.02317
1.00419
1.04252
10.9
Cardiovascular, ages 65+, hospital admissions
Prescott et
al. 1998
Edinburgh 2
United Kingdom
1992–1995
410–414,
426–429,
434–440
lag 1–3
2.30
–1.90
6.68
0.02274
0.02139
1.02300
0.98100
1.06680
8.7
Atkinson, et
al. 1999
London
United Kingdom
1992–1994
390–459
lag 0
1.67
0.76
2.60
0.01661
0.00463
1.01675
1.00756
1.02602
10.8
EUR/04/5042688
page 46
Table A9. Mortality and Admissions, PM2.5
Reference
City
Country
Study period
ICD group
Lag
%∆
%LCL
%UCL
Beta
SE
RR ∆
RR LCL
RR UCL
mean/
median
0.98367
0.96766
0.99994
31
1.00575
0.99798
1.01358
All cause, all ages, mortality
Wichmann
et al. 2000
Peters et al.
2000
Anderson,
et al. 2001
Erfurt
Czech
Republic (coal
basin)
West
Midlands
Germany
1995–1998
<800
lag 3
–1.63
–3.234
–0.006
–0.01646
0.00837
Czech Republic
1982–1994
<800
lag 1
0.575
–0.202
1.358
0.00573
0.00396
United Kingdom
1994–1996
<800
lag 0–1
0.339
–0.85
1.542
0.00338
0.00608
1.00339
0.99150
1.01542
11.7
1994–1996
460–519
lag 0–1
–0.06
–3.088
3.069
–0.00057
0.01571
0.99943
0.96912
1.03069
11.7
1994–1996
390–459
lag 0–1
0.507
–1.192
2.236
0.00506
0.00870
1.00507
0.98808
1.02236
11.7
1994–1996
460–519
lag 0–1
–0.74
–2.68
1.25
–0.00739
0.01010
0.99263
0.97317
1.01249
11.7
1994–1996
460–519
lag 0–1
–1.19
–3.67
1.35
–0.01199
0.01295
0.98808
0.96332
1.01348
11.7
1994–1996
460–519
lag 0–1
1.91
–0.06
3.91
0.01889
0.00993
1.01907
0.99943
1.03909
11.7
32
All respiratory, all ages, mortality
Anderson,
et al. 2001
West
Midlands
United Kingdom
Cardiovascular, all ages, mortality
Anderson,
et al. 2001
West
Midlands
United Kingdom
All respiratory, ages 65+, hospital admissions
Anderson,
et al. 2001
West
Midlands
United Kingdom
All respiratory, age 15 – 64, hospital admissions
Anderson,
et al. 2001
West
Midlands
United Kingdom
All respiratory, ages 0–14, hospital admissions
Anderson,
et al. 2001
West
Midlands
United Kingdom
Cardiovascular, age 65+, hospital admissions
No
estimates
EUR/04/5042688
page 47
Table A10. Admissions, Coarse Fraction
City
Country
Study
period
ICD
group
Lag
%∆
%LCL
%UCL
Beta
SE
RR ∆
RR LCL
RR UCL
mean/
median
West Midlands
United
Kingdom
1994–1996
<800
lag 0–1
–0.53
–3.73
2.77
–
0.00533
0.01666
0.99469
0.96274
1.02770
8
United
Kingdom
1994–1996
460–
519
lag 0–1
–6.76
–
12.40
–0.74
–
0.06995
0.03188
0.93244
0.87595
0.99257
8
West Midlands
United
Kingdom
1994–1996
390–
459
lag 0–1
–0.71
–4.26
2.97
–
0.00711
0.01858
0.99292
0.95740
1.02975
8
Krakow
Poland
1977–1989
lag 1–4
0.30
0.10
0.50
0.00300
0.00104
1.00301
1.00097
1.00505
Reference
All cause, all ages mortality
Anderson, et al.
2001
All respiratory, all ages, mortality
Anderson, et al.
2001
West Midlands
Cardiovascular, all ages, mortality
Anderson, et al.
2001
Krzyzanowski et al.
1991
All respiratory, ages 65+, hospital admissions
Anderson, et al.
2001
West Midlands
United
Kingdom
1994–1996
460–
519
lag 0–1
–1.68
–5.33
2.10
–
0.01698
0.01928
0.98317
0.94672
1.02102
8
1994–1996
460–
519
lag 0–1
–4.35
–8.81
0.33
–
0.04446
0.02439
0.95651
0.91187
1.00334
8
1994–1996
460–
519
lag 0–1
3.88
–0.27
8.21
0.03811
0.02080
1.03884
0.99734
1.08206
8
All respiratory, age 15 – 64, hospital admissions
Anderson, et al.
2001
West Midlands
United
Kingdom
All respiratory, ages 0 – 14, hospital admissions
Anderson, et al.
2001
West Midlands
United
Kingdom
Cardiovascular, ages 65+, hospital admissions
No estimates
EUR/04/5042688
page 48
Table A11. All–cause mortality, ozone
Reference
Saez et al.
2002
Saez et al.
2002
Saez et al.
2002
Le Tertre et
al. 2002
Le Tertre et
al. 2002
Le Tertre et
al. 2002
Le Tertre et
al. 2002
Le Tertre et
al. 2002
Le Tertre et
al. 2002
Anderson, et
al. 2001
Bremner et al.
1999
Hoek et al.
2000
Roemer et al.
2001
Michelozzi et
al. 1998
Cadum et al.
1999
City
Country
Study period
ICD
group
Lag
%∆
%LCL
%UCL
Beta
SE
RR ∆
RR LCL
RR UCL
mean/
median
Barcelona
Spain
1990–1996
<800
single
0.13
–0.17
0.43
0.00129
0.00155
1.00129
0.99826
1.00433
67.5
Madrid
Spain
1990–1996
<800
single
0.29
–0.06
0.64
0.00292
0.00179
1.00292
0.99941
1.00644
42.1
Valencia
Spain
1990–1996
<800
single
2.25
0.47
4.07
0.02228
0.00897
1.02253
1.00471
1.04067
45.5
Le Havre
France
1990–1995
<800
lag 0–1
0.69
–0.46
1.86
0.00688
0.00588
1.00690
0.99536
1.01858
Lyon
France
1990–1995
<800
lag 0–1
0.73
–0.04
1.50
0.00727
0.00391
1.00729
0.99960
1.01505
Paris
France
1990–1995
<800
lag 0–1
0.42
0.04
0.79
0.00416
0.00192
1.00417
1.00040
1.00794
Rouen
France
1990–1995
<800
lag 0–1
1.04
–0.02
2.11
0.01033
0.00537
1.01038
0.99980
1.02108
Strasbourg
France
1990–1995
<800
lag 0–1
0.57
–0.08
1.23
0.00572
0.00333
1.00573
0.99920
1.01231
Toulouse
France
1990–1995
<800
lag 0–1
0.26
–0.83
1.36
0.00258
0.00559
1.00259
0.99166
1.01363
1994–1996
<800
lag 0–1
0.50
–0.02
1.02
0.00500
0.00264
1.00501
0.99983
1.01022
48
1992–1994
<800
lag 2
–0.14
–0.45
0.18
–0.00137
0.00161
0.99863
0.99548
1.00180
32
<800
lag 1
0.22
0.13
0.31
0.00223
0.00046
1.00223
1.00132
1.00314
47
lag 2
–0.17
–0.52
0.18
–0.00171
0.00180
0.99829
0.99478
1.00181
41
West Midlands
London
United
Kingdom
United
Kingdom
Netherlands
Netherlands
1986–1994
Amsterdam
Netherlands
1987–1998
Rome
Italy
1992–1995
<800
lag 1
0.38
–0.03
0.79
0.00379
0.00209
1.00380
0.99970
1.00792
21
Turin
Italy
1991–1996
<800
lag 0
0.32
–0.12
0.76
0.00317
0.00223
1.00318
0.99880
1.00758
73.7
EUR/04/5042688
page 49
Table A12. Cardiovascular mortality, ozone
Reference
Le Tertre et
al. 2002
Le Tertre et
al. 2002
Le Tertre et
al. 2002
Le Tertre et
al. 2002
Le Tertre et
al. 2002
Le Tertre et
al. 2002
Saez et al.
2002
Saez et al.
2002
Saez et al.
2002
Cadum et al.
1999
Bremner et al.
1999
Anderson, et
al. 2001
Hoek et al.
2001
Peters et al.
2000
Wietlisbach et
al. 1996
Wietlisbach et
al. 1996
City
Country
Study period
ICD
group
Lag
%∆
%LCL
%UCL
Beta
SE
RR ∆
RR LCL
RR UCL
Le Havre
France
1990–1995
390–459
lag 0–1
0.28
–1.80
2.40
0.00278
0.01071
1.00278
0.98196
1.02405
Lyon
France
1990–1995
390–459
lag 0–1
0.38
–1.59
2.38
0.00376
0.01010
1.00377
0.98410
1.02383
Paris
France
1990–1995
390–459
lag 0–1
0.42
–0.34
1.18
0.00416
0.00387
1.00417
0.99658
1.01181
Rouen
France
1990–1995
390–459
lag 0–1
1.38
–0.63
3.43
0.01372
0.01021
1.01381
0.99372
1.03431
Strasbourg
France
1990–1995
390–459
lag 0–1
0.22
–0.83
1.28
0.00219
0.00539
1.00219
0.99166
1.01283
Toulouse
France
1990–1995
390–459
lag 0–1
1.00
–0.85
2.89
0.00995
0.00945
1.01000
0.99146
1.02889
Barcelona
Spain
1990–1996
390–459
single
0.55
–0.03
1.14
0.00552
0.00297
1.00554
0.99971
1.01140
67.5
Madrid
Spain
1990–1996
390–459
single
0.54
–0.04
1.13
0.00540
0.00298
1.00541
0.99955
1.01130
42.1
Valencia
Spain
1990–1996
390–459
single
3.14
0.35
6.00
0.03089
0.01397
1.03137
1.00352
1.05999
45.5
Italy
1991–1996
390–459
lag 0
0.67
–0.02
1.37
0.00669
0.00351
1.00671
0.99980
1.01367
73.7
1992–1994
390–459
lag 2
0.67
0.10
1.25
0.00669
0.00292
1.00672
1.00097
1.01249
32
1994–1996
390–459
lag 0–1
0.16
–0.60
0.92
0.00157
0.00388
1.00157
0.99397
1.00922
48
Turin
London
West Midlands
United
Kingdom
United
Kingdom
mean/me
dian
Netherlands
Netherlands
1986–1994
390–448
lag 1
0.36
0.21
0.51
0.00357
0.00075
1.00358
1.00210
1.00505
Germany (Rural)
Germany
1982–1994
390–459
lag 0
0.59
–0.38
1.57
0.00592
0.00494
1.00594
0.99624
1.01574
38
–0.81
0.76
–0.00030
0.00400
0.99970
0.99189
1.00757
26.9
–3.83
0.65
–0.01630
0.01160
0.98383
0.96172
1.00646
23.9
Zurich
Switzerland
1984–1989
390–459
lag 1
Basle
Switzerland
1984–1989
390–459
lag 1
–
0.03
–
1.62
EUR/04/5042688
page 50
Table A13. Respiratory mortality, ozone
Reference
Saez et al.
2002
Saez et al.
2002
Saez et al.
2002
Le Tertre et
al. 2002
Le Tertre et
al. 2002
Le Tertre et
al. 2002
Le Tertre et
al. 2002
Le Tertre et
al. 2002
Le Tertre et
al. 2002
Bremner et
al. 1999
Anderson, et
al. 2001
Cadum et al.
1999
City
Country
Study period
ICD
group
Lag
%∆
%LCL
%UCL
Beta
SE
RR ∆
RR LCL
RR UCL
mean/
median
Barcelona
Spain
1990–1996
460–519
single
0.40
–0.58
1.39
0.00398
0.00500
1.00399
0.99420
1.01388
67.5
Madrid
Spain
1990–1996
460–519
single
0.10
–0.98
1.20
0.00104
0.00554
1.00104
0.99022
1.01198
42.1
Valencia
Spain
1990–1996
460–519
single
1.85
–3.83
7.88
0.01836
0.02931
1.01853
0.96167
1.07875
45.5
Le Havre
France
1990–1995
460–519
lag 0–1
–2.02
–6.54
2.72
–0.02041
0.02411
0.97980
0.93458
1.02721
Lyon
France
1990–1995
460–519
lag 0–1
1.72
–1.00
4.51
0.01705
0.01383
1.01720
0.99000
1.04514
Paris
France
1990–1995
460–519
lag 0–1
–0.38
–1.87
1.13
–0.00384
0.00767
0.99617
0.98131
1.01125
Rouen
France
1990–1995
460–519
lag 0–1
2.07
–2.06
6.38
0.02051
0.02110
1.02072
0.97937
1.06383
Strasbourg
France
1990–1995
460–519
lag 0–1
0.02
–2.41
2.51
0.00020
0.01257
1.00020
0.97586
1.02514
Toulouse
France
1990–1995
460–519
lag 0–1
1.00
–3.18
5.36
0.00995
0.02154
1.01000
0.96825
1.05355
London
United Kingdom
1992–1994
460–519
lag 2
–0.71
–1.55
0.13
–0.00713
0.00431
0.99289
0.98453
1.00132
32
West
Midlands
United Kingdom
1994–1996
460–519
lag 0–1
0.38
–0.97
1.75
0.00380
0.00689
1.00381
0.99034
1.01746
48
Turin
Italy
1991–1996
480–519
lag 0
0.51
–1.48
2.55
0.00513
0.01024
1.00515
0.98517
1.02553
73.7
EUR/04/5042688
page 51
Table A14. Admissions, ozone
Reference
City
Country
ICD
group
Lag
%∆
%LCL
%UCL
Beta
SE
RR ∆
RR LCL
RR UCL
460–519
single
0.75
0.36
1.14
0.00746
0.00199
1.00749
1.00357
1.01141
460–519
lag 0–1
0.03
–0.73
0.80
0.00035
0.00391
1.00035
0.99271
1.00805
460–519
single
0.61
0.26
0.97
0.00611
0.00180
1.00612
1.00259
1.00967
1994–1996
460–519
lag 0–1
–0.50
–1.39
0.41
–0.00496
0.00461
0.99505
0.98609
1.00409
48
Study period
mean/
median
All respiratory, ages 65+, hospital admissions
Spix et al.
1998
Anderson et
al. 2001
Amsterdam,
London,
Paris,
Rotterdam
West
Midlands
Europe
United Kingdom
1994–1996
48
All respiratory, ages 15–64, hospital admissions
Spix et al.
1998
Anderson et
al. 2001
Amsterdam,
London,
Paris,
Rotterdam
West
Midlands
Europe
United Kingdom
All respiratory, ages 0–14, hospital admissions
Atkinson et al.
1999
Fusco et al.
2001
Anderson et
al. 2001
London
United Kingdom
1992–1994
460–519
lag 0
–0.32
–1.13
0.50
–0.00318
0.00416
0.99683
0.98873
1.00499
32
Rome
Italy
1995–1997
460–519
lag 1
2.22
0.08
4.41
0.02201
0.01080
1.02225
1.00084
1.04412
27
West
Midlands
United Kingdom
1994–1996
460–519
lag 0–1
–0.93
–1.77
–0.08
–0.00934
0.00434
0.99071
0.98232
0.99917
48
1992–1994
390–459
lag 2
0.65
0.22
1.08
0.00647
0.00219
1.00649
1.00217
1.01083
32
Cardiovascular, ages 65+, hospital admissions
Atkinson et al.
1999
London
United Kingdom
EUR/04/5042688
page 52
References of time-series studies
AGUINAGA, O. ET AL. [The short-term effects of air pollution on mortality: the results of the
EMECAM project in the city of Pamplona, 1991–1995. Estudio Multicentrico Espanol
sobre la Relacion entre la Contaminacion Atmosferica y la Mortalidad]. [Spanish] Revista
Espanola De Salud Publica, 73 (2): 253–258 (1999).
ANDERSON, H. R. ET AL. Particulate matter and daily mortality and hospital admissions in the
west midlands conurbation of the United Kingdom: associations with fine and coarse
particles, black smoke and sulphate. Occupational and environmental medicine, 58: 504–
510 (2001).
ARRIBAS, M. F. ET AL. The short-term effects of air pollution on mortality. The results of the
EMECAM project in Saragossa, 1991–1995. Estudio Multicentrico Espanol sobre la
Relacion entre la Contaminacion Atmosferica y la Mortalidad]. [Spanish], Revista
Espanola De Salud Publica, 73 (2): 293–302 (1999).
ARRIBAS, M. F. ET AL. Effects of air pollution on daily mortality in Zaragoza, Spain, 1991–1995.
Salud Publica de Mexico, 43: 289–297 (2001).
ATKINSON, R. W. ET AL. Acute effects of particulate air pollution on respiratory admissions –
Results from APHEA 2 project. American Journal of Respiratory and Critical Care
Medicine, 164: 1860–1866 (2001).
BELLIDO BLASCO, J. B. ET AL. The short-term effects of air pollution on mortality: the results of
the EMECAM project in Castellon, 1991–1995. [Estudio Multicentrico Espanol sobre la
Relacion entre la Contaminacion Atmosferica y la Mortalidad]. [Spanish]. Revista
Espanola De Salud Publica, 73: 225–231 (1999).
BIGGERI, A. ET AL. Meta-analysis of the Italian studies on short-term effects of air pollution].
[Italian], Epidemiologia e Prevenzione, 25: l–71 (2001).
BREMNER, S.A. ET AL. Short-term associations between outdoor air pollution and mortality in
London 1992–1994. Occupational and environmental medicine, 56: 237–244 (1999).
CADUM, E. ET AL. Air pollution and daily mortality in Turin, 1991–1996. Epidemiologia e
prevenzione, 23: 268–276 (1999).
CAMBRA, C. K. & ALONSO, F. E. [The short-term effects of air pollution on mortality: the results
of the EMECAM project in greater Bilbao. Estudio Multicentrico Espanol sobre la
Relacion entre la Contaminacion Atmosferica y la Mortalidad]. [Spanish]. Revista
Espanola De Salud Publica, 73: 209–214 (1999).
DAPONTE, C. A. ET AL. [The short-term effects of air pollution on mortality: the results of the
EMECAM project in the city of Huelva, 1993–1996. Estudio Multicentrico Espanol sobre
la Relacion entre la Contaminacion Atmosferica y la Mortalidad]. [Spanish]. Revista
Espanola De Salud Publica, 73: 233–242 (1999).
FUSCO, D. ET AL. Air pollution and hospital admissions for respiratory conditions in Rome, Italy.
European respiratory journal, 17: 1143–1150 (2001).
EUR/04/5042688
page 53
GALAN, L. I. ET AL. The short-term effects of air pollution on mortality: the results of the
EMECAM project in the municipality of Madrid, 1992–1995. Revista espanola de salud
publica, 73: 243–252 (1999).
GARCIA-AYMERICH, J. ET AL. Air pollution and mortality in a cohort of patients with chronic
obstructive pulmonary disease: a time series analysis. Journal of epidemiology and
community health, 54: 73–74 (2000).
HOEK G. ET AL. The association between air pollution and heart failure, arrhythmia, embolism,
thrombosis, and other cardiovascular causes of death in a time series study. Epidemiology:
12: 355–357 (2001).
HOEK G. ET AL. Daily mortality and air pollution in the Netherlands. Journal of the air and waste
management association, 50: 1380–1389 (2000).
HOEK G. ET AL. Effects of ambient particulate matter and ozone on daily mortality in Rotterdam,
The Netherlands. Archives of environmental health, 52: 455–463 (1997).
KATSOUYANNI, K. ET AL. Confounding and effect modification in the short-term effects of
ambient particles on total mortality: Results from 29 European cities within the APHEA 2
project. Epidemiology, 12: 521–531 (2001).
KRZYZANOWSKI, M. & WOJTYNIAK, B. Air pollution and daily mortality in Cracow. Public
Health Review, 19: 73–81 (1991).
LE TERTRE, A. ET AL. Short-term effects of air pollution on mortality in nine French cities: A
quantitative summary. Archives of environmental health, 57: 311–319 (2002).
MICHELOZZI, P. ET AL. [Acute effects of air pollution in Rome]. [Italian]. Annali dell Istituto
Superiore di Sanita, 36: 297–304 (2000).
MICHELOZZI, P. ET AL. Air pollution and daily mortality in Rome, Italy. Journal of occupational
and environmental medicine, 55: 605–610 (1998).
OCANA-RIOLA, R., ET AL. [The short-term effects of air pollution on mortality. The results of the
EMCAM project in the city of Seville, 1992-1996. Estudio Multicentrico Espanol sobre la
Relacion entre la Contaminacion Atmosferica y la Mortalidad]. [Spanish]. Revista
Espanola De Salud Publica, 73: 259–265 (1999).
PEREZ BOILLOS, M. J. ET AL. [The short-term effects of air pollution on mortality. The results of
the EMECAM project in Vitoria-Gasteiz, 1990–1994. Estudio Multicentrico Espanol sobre
la Relacion entre la Contaminacion Atmosferica y la Mortalidad]. [Spanish]. Revista
Espanola De Salud Publica, 73: 283–292 (1999).
PETERS, A. ET AL. Associations between mortality and air pollution in Central Europe.
Environmental Health Perspectives, 108: 283–287 (2000).
PRESCOTT, G.J. ET AL. Urban air pollution and cardiopulmonary ill health: a 14.5 year time series
study. Occupational and environmental health, 55: 697–704 (1998).
EUR/04/5042688
page 54
ROEMER, W. H. & VAN WIJNEN J. H. Daily mortality and air pollution along busy streets in
Amsterdam, 1987–1998. Epidemiology, 12: 649–653 (2001).
SAEZ, M. ET AL. A combined analysis of the short-term effects of photochemical air pollutants on
mortality within the EMECAM project. Environmental health perspectives, 110: 221–228
(2002).
SPIX, C. ET AL. Short-term effects of air pollution on hospital admissions of respiratory diseases
in Europe: a quantitative summary of APHEA study results. Air Pollution and Health: a
European Approach. Archives of environmental health, 53: 54–64 (1998).
SPIX, C. & WICHMANN, H. E. ET AL. Daily mortality and air pollutants: findings from Koln,
Germany. Journal of epidemiology and community health, 50: 52–58 (1996).
TARACIDO, T. M. ET AL. The short-term effects of air pollution on mortality. The results of the
EMECAM project in the city of Vigo, 1991–1994. Estudio Multicentrico Espanol sobre la
Relacion entre la Contaminacion Atmosferica y la Mortalidad]. [Spanish]. Revista
Espanola De Salud Publica,. 73: 275–282 (1999).
TENIAS BURILLO, J. M. ET AL. The short-term effects of air pollution on mortality. The results of
the EMECAM project in the city of Valencia, 1994–1996. Revista espanola de salud, 73:
267–274 (1999).
WICHMANN, H. E. ET AL. Daily mortality and fine and ultrafine particles in Erfurt, Germany part
I: Role of particle number and particle mass. Health Effects Institute (2000).
WIETLISBACH, V. ET AL. Air pollution and daily mortality in three Swiss urban areas. Sozial- und
Praventivmedizin, 41: 107–115 (1996).
WOJTYNIAK, B. & PIEKARSKA, T. Short term effect of air pollution on mortality in Polish urban
populations – What is different? Journal of epidemiology and community health, 50: 36–41
(1996).
ZEGHNOUN, A. ET AL. Surveillance des effets à court terme de la pollution atmosphérique sur la
mortalité en milieu urbain. Résultats d’une étude de faisabilité dans 9 villes françaises.
Revue d' epidemiologie et de sante publique, 49: 3–12 (2001).
ZMIROU, D. ET AL. Short term effects of air pollution on mortality in the city of Lyon, France,
1985–1990. Journal of epidemiology and community health, 50: 30–35 (1996).
EUR/04/5042688
page 55
Tables of individual city results – panel studies
Table A15. Cough in symptomatic children, PM10
Reference
City
Country
Study period
Outcome
Ages
Lag
OR
OR LCL
OR UCL
Forsberg et
al.1998
4 Northern Swedish villages
Sweden
03/01/1994–27/03/1994
cough
5–11
1
0.753
0.547
1.037
Nielsen et al.
1998
Almhult, Olofstrom
Sweden
1993–1994
cough
7–12
0
1.235
0.980
1.556
van der Zee
et al. 1998
Amsterdam
Netherlands
20/11/1993–28/02/1994
cough
7–11
1
0.866
0.786
0.954
Kalandidi et
al. 1998
Athens
Greece
10/01/1994–10/03/1994
cough
6–11
2
1.056
1.009
1.105
Vondra et et
al. 1998
Benesov
Czech Republic
17/01/1994–12/04/1994
cough
6–13
2
1.013
0.957
1.072
Englert et al.
1998
Berlin
Germany
27/01/1994–25/03/1994
cough
7–11
1
0.937
0.842
1.043
Englert et al.
1998
Berlin suburb
Germany
27/01/1994–25/03/1994
cough
7–11
2
1.033
0.940
1.135
Rudnai et al.
1998
Budapest
Hungary
02/1994–04/1994
cough
6–12
1
1.016
0.966
1.069
Nielsen et al.
1998
Burlov, Malmo
Sweden
1993–1994
cough
7–12
2
1.077
0.936
1.239
van der Zee
et al. 1998
Drenthe
Netherlands
20/11/1993–28/02/1994
cough
8–12
1
1.036
0.983
1.092
Beyer et al.
1998
Hettstedt
Germany
10/1993–03/1994
cough
6–11
2
1.047
0.959
1.143
Niepsuj et al.
1998
Katowice
Poland
17/01/1994–10/04/1994
cough
7–12
0
0.930
0.864
1.001
Haluszka et
al. 1998
Krakow
Poland
10/01/1994–01/04/1994
cough
7–11
0
0.947
0.901
0.995
Timonen et
al. 1998
Kuopio
Finland
08/02/1994–05/04/1994
cough
7–12
1
0.868
0.751
1.003
Tiittanen et
al. 1999
Kuopio
Finland
13/03/1995–23/04/1995
cough
8–13
2
1.046
1.010
1.084
Timonen et
al. 1998
Kuopio suburb
Finland
08/02/1994–05/04/1994
cough
7–12
2
0.927
0.728
1.180
van der Zee
et al. 1999
Netherlands, rural
Netherlands
1992–1995
cough
7–11
1
1.009
0.998
1.019
EUR/04/5042688
page 56
Reference
City
Country
Study period
Outcome
Ages
Lag
OR
OR LCL
OR UCL
van der Zee
et al. 1999
Netherlands, urban
Netherlands
1992–1995
cough
7–11
2
1.005
0.991
1.019
Clench–Aas
et al. 1998
Oslo
Norway
01/12/1993–14/02/1994
cough
6–12
1
0.965
0.811
1.148
Clench–Aas
et al. 1998
Oslo suburb
Norway
01/12/1993–14/02/1994
cough
6–12
1
1.176
0.908
1.523
Segala et al.
1998
Paris
France
15/11/1992–09/05/1993
nocturnal cough
7–15
3
1.116
1.032
1.207
Just et al.
2002
Paris
France
01/04/1996 – 30/06/1996
nocturnal cough
7–15
0
1.100
0.880
1.375
Baldini et al.
1998
Pisa
Italy
1993–1994 (2 months)
cough
6–11
1
0.975
0.947
1.004
Kotesovec et
al. 1998
Prachatice
Czech Republic
01/1994–03/1994
cough
7–11
0
1.025
0.938
1.120
Vondra et et
al. 1998
Prague
Czech Republic
17/01/1994–12/04/1994
cough
6–13
1
1.029
0.958
1.105
Niepsuj et al.
1998
Pszczyna
Poland
17/01/1994–10/04/1994
cough
7–12
0
0.997
0.979
1.015
Haluszka et
al. 1998
Rabka
Poland
10/01/1994–01/04/1994
cough
6–12
1
0.983
0.947
1.020
Peters et al.
1997
Sokolov
Czech Republic
01/09/1991–31/03/1992
cough
6–14
0
1.002
0.993
1.011
Kalandidi et
al. 1998
Southern Greek villages
Greece
10/01/1994–10/03/1994
cough
5–12
0
0.891
0.815
0.974
Rudnai et al.
1998
Szentendre
Hungary
02/1994–04/1994
cough
6–12
0
0.935
0.868
1.007
Kotesovec et
al. 1998
Teplice
Czech Republic
01/1994–03/1994
cough
7–13
1
1.021
0.977
1.067
Baldini et al.
1998
Torre del Lago Puccini
Italy
1993–1994 (2 months)
cough
6–11
2
0.977
0.957
0.997
Forsberg et
al. 1998
Umea
Sweden
03/01/1994–27/03/1994
cough
5–11
2
0.766
0.577
1.017
Beyer et al.
1998
Zerbst
Germany
10/1993–03/1994
cough
6–11
0
0.952
0.847
1.070
EUR/04/5042688
page 57
Table A16. Cough in symptomatic adults, PM10, black smoke and ozone
Reference
City
Country
Study period
Outcome
Ages
Lag
OR
OR LCL
OR UCL
1.001
1.041
0.963
1.008
Cough in symptomatic adults, PM10
Boezen et al.
1998
Amsterdam, Meppel
Netherlands
1993–1994
cough
16+
0
1.021
van der Zee
et al. 20001
Amsterdam, Rotterdam
Netherlands
1992–1995
cough
50–70
1
1.000
Hiltermann
et al. 19982
Leiden
Netherlands
03/07/1995–06/10/1995
cough/phlegm
18–55
0
0.986
van der Zee
et al. 20001
Meppel, Nunspeet
Netherlands
1992–1995
cough
50–70
1
1.000
Neukirch et
al. 1998
Paris
France
15/11/1992–09/05/1993
nocturnal cough
16–70
6
1.116
1.052
1.183
Dusseldorp
et al. 1995
Vijk aan Zee
Netherlands
11/10/1993–22/12/1993
cough
16+
0
1.027
0.997
1.059
0.969
1.098
0.900
1.067
Cough in symptomatic adults, black smoke
Boezen et al.
1998
Amsterdam, Meppel
Netherlands
1993–1994
cough
16+
0
1.031
van der Zee
et al. 20001
Amsterdam, Rotterdam
Netherlands
1992–1995
cough
50–70
1
1.000
Hiltermann
et al. 19982
Leiden
Netherlands
03/07/1995–06/10/1995
cough/phlegm
18–55
0
0.980
van der Zee
et al. 20001
Meppel, Nunspeet
Netherlands
1992–1995
cough
50–70
1
1.000
Neukirch et
al. 1998
Paris
France
15/11/1992–09/05/1993
nocturnal cough
16–70
6
1.077
1.016
1.143
Cough in symptomatic adults and ozone
Hiltermann
et al. 19982
Leiden
Netherlands
03/07/1995–06/10/1995
cough/phlegm
18–55
1
0.987
0.975
0.999
Higgins et al.
1995
Runcorn & Widnes
United Kingdom
28 days
cough
16+
0
1.050
0.910
1.212
Note:
Estimate not given; results reported as “not significant” only.
2
Estimate expressed as a relative risk and 95% confidence interval.
1
EUR/04/5042688
page 58
Table A17. Cough in symptomatic children, coarse fraction, PM2.5 and ozone
Reference
City
Country
Study period
Outcome
Ages
Lag
OR
OR LCL
OR UCL
Finland
13/03/1995–23/04/1995
cough
8–13
2
1.086
1.023
1.152
Finland
13/03/1995–23/04/1995
cough
8–13
2
1.091
1.007
1.182
France
01/04/1996 – 30/06/1996
nocturnal cough
7–15
0
1.040
0.920
1.176
Cough in symptomatic children, coarse fraction
Tiittanen et
al. 1999
Kuopio
Cough in symptomatic children, PM2.5
Tiittanen et
al. 1999
Kuopio
Cough in symptomatic children and ozone
Just et al.
2002
Paris
EUR/04/5042688
page 59
Table A18. Cough in symptomatic children, black smoke
Reference
City
Country
Study period
Outcome
Ages
Lag
OR
OR LCL
OR UCL
Forsberg et
al. 1998
4 northern Swedish villages
Sweden
03/01/1994–27/03/1994
cough
5–11
0
1.185
0.764
1.838
Nielsen et al.
1998
Almhult, Olofstrom
Sweden
1993–1994
cough
7–12
1
1.334
0.676
2.632
van der Zee
et al. 1998
Amsterdam
Netherlands
20/11/1993–28/02/1994
cough
7–11
1
0.780
0.644
0.945
Kalandidi et
al. 1998
Athens
Greece
10/01/1994–10/03/1994
cough
6–11
2
1.048
1.005
1.093
Vondra et al.
1998
Benesov
Czech Republic
17/01/1994–12/04/1994
cough
6–13
1
0.893
0.756
1.055
Englert et al.
1998
Berlin
Germany
27/01/1994–25/03/1994
cough
7–11
0
0.840
0.704
1.002
Englert et al.
1998
Berlin suburb
Germany
27/01/1994–25/03/1994
cough
7–11
0
1.113
0.942
1.315
Rudnai et al.
1998
Budapest
Hungary
02/1994–04/1994
cough
6–12
2
1.022
0.961
1.087
Nielsen et al.
1998
Burlov, Malmö
Sweden
1993–1994
cough
7–12
0
0.981
0.757
1.271
van der Zee
et al. 1998
Drenthe
Netherlands
20/11/1993–28/02/1994
cough
8–12
1
1.128
0.954
1.334
Beyer et al.
1998
Hettstedt
Germany
10/1993–03/1994
cough
6–11
0
0.963
0.913
1.016
Niepsuj et al.
1998
Katowice
Poland
17/01/1994–10/04/1994
cough
7–12
2
0.982
0.956
1.009
Haluszka et
al. 1998
Krakow
Poland
10/01/1994–01/04/1994
cough
7–11
1
0.961
0.893
1.034
Timonen et
al. 1998
Kuopio
Finland
08/02/1994–05/04/1994
cough
7–12
1
0.845
0.711
1.004
Timonen et
al. 1998
Kuopio suburb
Finland
08/02/1994–05/04/1994
cough
7–12
2
0.882
0.707
1.100
van der Zee
et al. 1999
Netherlands, rural
Netherlands
1992–1995
cough
7–11
1
1.026
1.000
1.054
van der Zee
et al. 1999
Netherlands, urban
Netherlands
1992–1995
cough
7–11
0
1.026
0.987
1.067
Clench–Aas
et al. 1998
Oslo
Norway
01/12/1993–14/02/1994
cough
6–12
1
1.009
0.890
1.144
EUR/04/5042688
page 60
Reference
City
Country
Study period
Outcome
Ages
Lag
OR
OR LCL
OR UCL
Clench–Aas
et al. 1998
Oslo suburb
Norway
01/12/1993–14/02/1994
cough
6–12
1
1.058
0.906
1.236
Segala et al.
1998
Paris
France
15/11/1992–09/05/1993
nocturnal cough
7–15
2
1.041
0.963
1.124
Segala et al.
1998
Paris
France
15/11/1992–09/05/1993
nocturnal cough
7–15
4
1.132
1.047
1.224
Just et al.
2002
Paris
France
01/04/1996–30/06/1996
nocturnal cough
7–15
0
1.220
0.990
1.503
Baldini et al.
1998
Pisa
Italy
1993–1994 (2 months)
cough
6–11
2
0.947
0.871
1.030
Kotesovec et
al. 1998
Prachatice
Czech Republic
01/1994–03/1994
cough
7–11
0
1.131
0.976
1.311
Vondra et et
al. 1998
Prague
Czech Republic
17/01/1994–12/04/1994
cough
6–13
1
1.047
0.927
1.183
Niepsuj et al.
1998
Pszczyna
Poland
17/01/1994–10/04/1994
cough
7–12
2
1.008
0.985
1.032
Haluszka et
al. 1998
Rabka
Poland
10/01/1994–01/04/1994
cough
6–12
0
1.009
0.963
1.057
Kalandidi et
al. 1998
Southern Greek villages
Greece
10/01/1994–10/03/1994
cough
5–12
0
0.896
0.800
1.004
Rudnai et al.
1998
Szentendre
Hungary
02/1994–04/1994
cough
6–12
0
0.880
0.802
0.966
Kotesovec et
al. 1998
Teplice
Czech Republic
01/1994–03/1994
cough
7–13
1
1.013
0.968
1.060
Baldini et al.
1998
Torre del Lago Puccini
Italy
1993–1994 (2 months)
cough
6–11
1
0.980
0.942
1.020
Forsberg et
al. 1998
Umea
Sweden
03/01/1994–27/03/1994
cough
5–11
0
1.145
0.877
1.495
Beyer et al.
1998
Zerbst
Germany
10/1993–03/1994
cough
6–11
2
0.968
0.875
1.071
EUR/04/5042688
page 61
Table A19. Medication use in symptomatic children, PM10
Reference
City
Country
Study period
Outcome
Ages
Lag
OR
OR LCL
OR UCL
Forsberg et
al. 1998
4 Northern Swedish villages
Sweden
03/01/1994–27/03/1994
bronchodilator use
5–11
0
1.275
0.702
2.316
Nielsen et al.
1998
Almhult, Olofstrom
Sweden
1993–1994
bronchodilator use
7–12
2
0.785
0.583
1.057
van der Zee
et al. 1998
Amsterdam
Netherlands
20/11/1993–28/02/1994
bronchodilator use
7–11
0
1.154
0.953
1.397
Kalandidi et
al. 1998
Athens
Greece
10/01/1994–10/03/1994
bronchodilator use
6–11
0
0.940
0.830
1.065
Vondra et et
al. 1998
Benesov
Czech Republic
17/01/1994–12/04/1994
bronchodilator use
6–13
1
1.095
0.969
1.237
Englert et al.
1998
Berlin
Germany
27/01/1994–25/03/1994
bronchodilator use
7–11
0
0.872
0.692
1.099
Englert et al.
1998
Berlin suburb
Germany
27/01/1994–25/03/1994
bronchodilator use
7–11
1
1.092
0.872
1.368
Rudnai et al.
1998
Budapest
Hungary
02/1994–04/1994
bronchodilator use
6–12
2
0.832
0.703
0.985
Nielsen et al.
1998
Burlov, Malmo
Sweden
1993–1994
bronchodilator use
7–12
1
1.306
1.015
1.680
van der Zee
et al. 1998
Drenthe
Netherlands
20/11/1993–28/02/1994
bronchodilator use
8–12
2
1.062
0.991
1.138
Beyer et al.
1998
Hettstedt
Germany
10/1993–03/1994
bronchodilator use
6–11
1
0.744
0.490
1.130
Haluszka et
al. 1998
Krakow
Poland
10/01/1994–01/04/1994
bronchodilator use
7–11
1
0.890
0.707
1.120
Timonen et
al. 1998
Kuopio
Finland
08/02/1994–05/04/1994
bronchodilator use
7–12
2
1.067
0.955
1.192
Timonen et
al. 1998
Kuopio suburb
Finland
08/02/1994–05/04/1994
bronchodilator use
7–12
0
1.039
0.971
1.112
van der Zee
et al. 1999
Netherlands, rural
Netherlands
1992–1995
bronchodilator use
7–11
0
0.980
0.952
1.010
van der Zee
et al. 1999
Netherlands, urban
Netherlands
1992–1995
bronchodilator use
7–11
2
1.005
0.991
1.019
Clench–Aas
et al. 1998
Oslo
Norway
01/12/1993–14/02/1994
bronchodilator use
6–12
1
0.910
0.784
1.056
EUR/04/5042688
page 62
Reference
City
Country
Study period
Outcome
Ages
Lag
OR
OR LCL
OR UCL
Clench–Aas
et al. 1998
Oslo suburb
Norway
01/12/1993–14/02/1994
bronchodilator use
6–12
0
1.069
0.959
1.192
Segala et al.
1998
Paris
France
15/11/1992–09/05/1993
B2 agonist
7–15
0
1.145
0.852
1.539
Baldini et al.
1998
Pisa
Italy
1993–1994 (2 months)
bronchodilator use
6–11
0
0.866
0.700
1.071
Kotesovec et
al. 1998
Prachatice
Czech Republic
01/1994–03/1994
bronchodilator use
7–11
2
1.520
1.064
2.171
Vondra et et
al. 1998
Prague
Czech Republic
17/01/1994–12/04/1994
bronchodilator use
6–13
2
0.931
0.814
1.065
Niepsuj et al.
1998
Pszczyna
Poland
17/01/1994–10/04/1994
bronchodilator use
7–12
1
0.961
0.925
0.998
Haluszka et
al. 1998
Rabka
Poland
10/01/1994–01/04/1994
bronchodilator use
6–12
1
1.016
0.913
1.131
Peters et al.
1997
Sokolov
Czech Republic
01/09/1991–31/03/1992
B agonist
6–14
0
1.011
0.974
1.049
Kalandidi et
al. 1998
Southern Greek villages
Greece
10/01/1994–10/03/1994
bronchodilator use
5–12
2
0.882
0.650
1.197
Rudnai et al.
1998
Szentendre
Hungary
02/1994–04/1994
bronchodilator use
6–12
1
0.861
0.695
1.067
Kotesovec et
al. 1998
Teplice
Czech Republic
01/1994–03/1994
bronchodilator use
7–13
0
1.035
0.998
1.073
Baldini et al.
1998
Torre del Lago Puccini
Italy
1993–1994 (2 months)
bronchodilator use
6–11
1
1.050
0.925
1.192
Forsberg et
al. 1998
Umea
Sweden
03/01/1994–27/03/1994
bronchodilator use
5–11
0
1.498
0.899
2.496
Beyer et al.
1998
Zerbst
Germany
10/1993–03/1994
bronchodilator use
6–11
1
0.567
0.311
1.034
EUR/04/5042688
page 63
Table A20. Medication use in symptomatic children, black smoke
Reference
City
Country
Study period
Outcome
Ages
Lag
OR
OR LCL
OR UCL
Forsberg et
al. 1998
4 northern Swedish villages
Sweden
03/01/1994–27/03/1994
bronchodilator use
5–11
1
0.480
0.155
1.486
Nielsen et al.
1998
Almhult, Olofstrom
Sweden
1993–1994
bronchodilator use
7–12
1
0.495
0.226
1.084
van der Zee
et al. 1998
Amsterdam
Netherlands
20/11/1993–28/02/1994
bronchodilator use
7–11
2
1.618
1.104
2.371
Kalandidi et
al. 1998
Athens
Greece
10/01/1994–10/03/1994
bronchodilator use
6–11
0
0.922
0.811
1.048
Vondra et et
al. 1998
Benesov
Czech Republic
17/01/1994–12/04/1994
bronchodilator use
6–13
0
0.932
0.649
1.338
Englert et al.
1998
Berlin
Germany
27/01/1994–25/03/1994
bronchodilator use
7–11
1
0.736
0.486
1.115
Englert et al.
1998
Berlin suburb
Germany
27/01/1994–25/03/1994
bronchodilator use
7–11
1
1.163
0.830
1.630
Rudnai et al.
1998
Budapest
Hungary
02/1994–04/1994
bronchodilator use
6–12
1
0.847
0.700
1.025
Nielsen et al.
1998
Burlov, Malmo
Sweden
1993–1994
bronchodilator use
7–12
1
1.497
1.008
2.223
van der Zee
et al. 1998
Drenthe
Netherlands
20/11/1993–28/02/1994
bronchodilator use
8–12
0
0.775
0.536
1.121
Beyer et al.
1998
Hettstedt
Germany
10/1993–03/1994
bronchodilator use
6–11
1
0.679
0.458
1.007
Haluszka et
al. 1998
Krakow
Poland
10/01/1994–01/04/1994
bronchodilator use
7–11
0
1.223
1.048
1.427
Timonen et
al. 1998
Kuopio
Finland
08/02/1994–05/04/1994
bronchodilator use
7–12
0
0.933
0.842
1.034
Timonen et
al. 1998
Kuopio suburb
Finland
08/02/1994–05/04/1994
bronchodilator use
7–12
2
1.036
0.971
1.105
van der Zee
et al. 1999
Netherlands, rural
Netherlands
1992–1995
bronchodilator use
7–11
2
0.952
0.880
1.029
van der Zee
et al. 1999
Netherlands, urban
Netherlands
1992–1995
bronchodilator use
7–11
0
1.090
1.029
1.154
Clench–Aas
et al. 1998
Oslo
Norway
01/12/1993–14/02/1994
bronchodilator use
6–12
1
0.941
0.848
1.044
EUR/04/5042688
page 64
Reference
City
Country
Study period
Outcome
Ages
Lag
OR
OR LCL
OR UCL
Clench–Aas
et al. 1998
Oslo suburb
Norway
01/12/1993–14/02/1994
bronchodilator use
6–12
2
0.993
0.942
1.047
Segala et al.
1998
Paris
France
15/11/1992–09/05/1993
B2 agonist
7–15
0
1.105
0.856
1.427
Segala et al.
1998
Paris
France
15/11/1992–09/05/1993
B2 agonist
7–15
4
1.071
0.952
1.206
Baldini et al.
1998
Pisa
Italy
1993–1994 (2 months)
bronchodilator use
6–11
2
1.495
0.716
3.122
Kotesovec et
al. 1998
Prachatice
Czech Republic
01/1994–03/1994
bronchodilator use
7–11
2
1.416
1.082
1.853
Vondra et et
al. 1998
Prague
Czech Republic
17/01/1994–12/04/1994
bronchodilator use
6–13
2
0.852
0.679
1.069
Niepsuj et al.
1998
Pszczyna
Poland
17/01/1994–10/04/1994
bronchodilator use
7–12
1
0.975
0.938
1.013
Haluszka et
al. 1998
Rabka
Poland
10/01/1994–01/04/1994
bronchodilator use
6–12
2
1.063
0.935
1.209
Kalandidi et
al. 1998
Southern Greek villages
Greece
10/01/1994–10/03/1994
bronchodilator use
5–12
2
1.054
0.970
1.145
Rudnai et al.
1998
Szentendre
Hungary
02/1994–04/1994
bronchodilator use
6–12
1
0.763
0.568
1.025
Kotesovec et
al. 1998
Teplice
Czech Republic
01/1994–03/1994
bronchodilator use
7–13
1
1.042
0.996
1.090
Baldini et al.
1998
Torre del Lago Puccini
Italy
1993–1994 (2 months)
bronchodilator use
6–11
0
0.923
0.730
1.167
Forsberg et
al. 1998
Umea
Sweden
03/01/1994–27/03/1994
bronchodilator use
5–11
0
1.800
1.120
2.893
Beyer et al.
1998
Zerbst
Germany
10/1993–03/1994
bronchodilator use
6–11
1
0.947
0.668
1.343
Table A21. Medication use in symptomatic children and ozone
Reference
City
Country
Study period
Outcome
Ages
Lag
OR
OR LCL
OR UCL
Just et al.
2002
Paris
France
01/04/1996 – 30/06/1996
B2 agonist
7–15
0
1.410
1.052
1.890
EUR/04/5042688
page 65
Table A22. Medication use in symptomatic adults, black smoke, PM10, coarse fraction and ozone
Reference
City
Country
Study period
Outcome
Ages
Lag
OR
OR LCL
OR UCL
Medication use in symptomatic adults, black smoke
van der Zee
et al. 2000
Amsterdam, Rotterdam
Netherlands
1992–1995
bronchodilator use
50–70
2
0.971
0.937
1.007
Hiltermann
1
et al. 1998
Leiden
Netherlands
03/07/1995–06/10/1995
bronchodilator use
18–55
0
0.970
0.910
1.034
van der Zee
et al. 2000
Meppel, Nunspeet
Netherlands
1992–1995
bronchodilator use
50–70
1
1.010
0.987
1.033
Medication use in symptomatic adults, PM10
van der Zee
1
et al. 2000
Amsterdam, Rotterdam
Netherlands
1992–1995
bronchodilator use
50–70
2
0.993
0.977
1.009
Hiltermann
2
et al. 1998
Leiden
Netherlands
03/07/1995–06/10/1995
bronchodilator use
18–55
0
1.003
0.993
1.013
van der Zee
1
et al. 2000
Meppel, Nunspeet
Netherlands
1992–1995
bronchodilator use
50–70
1
1.005
0.997
1.013
Dusseldorp
et al. 1995
Vijk aan Zee
Netherlands
11/10/1993–22/12/1993
bronchodilator use
16+
1
1.034
1.018
1.051
Germany
29/10/1996 – 30/03/1997
B2 agonist
16+
0
1.008
0.958
1.061
Medication use in symptomatic adults, coarse fraction
von Klot et
al. 2002
Erfurt
Medication use in symptomatic adults, ozone
Hiltermann
2
et al. 1998
Leiden
Netherlands
03/07/1995–06/10/1995
bronchodilator use
18–55
1
1.009
0.997
1.020
Higgins et al.
1995
Runcorn & Widnes
United Kingdom
28 days
bronchodilator use
16+
1
1.440
1.140
1.819
Note:
Estimate not given; results reported as “not significant” only
2
Estimate expressed as a relative risk and 95% confidence interval
1
EUR/04/5042688
page 66
References panel studies
BALDINI, G. ET AL. Air pollution and respiratory health of children: The PEACE panel study in
Pisa, Italy. European Respiratory Review, 8 (52): 108–116 (1998).
BEYER, U. ET AL. Air pollution and respiratory health of children: The PEACE panel study in
Hettstedt and Zerbst, Eastern Germany. European Respiratory Review, 8 (52): 61–69
(1998).
BOEZEN, M. ET AL. Peak expiratory flow variability, bronchial responsiveness, and susceptibility
to ambient air pollution in adults. American Journal of Respiratory & Critical Care
Medicine, 158 (6): 1848–1854 (1998).
CLENCH-AAS, J. ET AL. Air pollution and respiratory health of children: The PEACE study in
Oslo, Norway. European Respiratory Review, 8 (52): 36–43 (1998).
DUSSELDORP, A. ET AL. Associations of PM10 and airborne iron with respiratory health of adults
living near a steel factory. American Journal of Respiratory & Critical Care Medicine,
152: 1932–1939 (1995).
ENGLERT, N. ET AL. Air pollution and respiratory health of children: The PEACE panel study in
Berlin, Germany. European Respiratory Review, 8: 53–60 (1998).
FORSBERG, B. ET AL. Air pollution and respiratory health of children: The PEACE panel study in
Umea, Sweden. European Respiratory Review, 8: 12–19 (1998).
HALUSZKA, J., ET AL. Air pollution and respiratory health in children: The PEACE panel study in
Krakow, Poland. European Respiratory Review, 8: 94–100 (1998).
HIGGINS, B. G. ET AL. Effects of air pollution on symptoms and peak expiratory flow
measurements in subjects with obstructive airways disease. Thorax, 50: 149–155 (1995).
HILTERMANN, T. J. ET AL. Asthma severity and susceptibility to air pollution. European
Respiratory Journal, 11: 686–693 (1998).
JUST, J. ET AL. Short-term health effects of particulate and photochemical air pollution in
asthmatic children. European Respiratory Journal, 20: 899–906 (2002).
KALANDIDI, A. ET AL. Air pollution and respiratory health of children: The PEACE panel study
in Athens, Greece. European Respiratory Review, 8: 117–124 (1998).
KOTESOVEC, F. ET AL. Air pollution and respiratory health of children: The PEACE panel study
in Teplice, Czech Republic, European Respiratory Review, 8: 70–77 (1998).
NEUKIRCH, F. ET AL. Short-term effects of low-level winter pollution on respiratory health of
asthmatic adults. Archives of Environmental Health, 53: 320–328 (1998).
EUR/04/5042688
page 67
NIELSEN, J. ET AL. Air pollution and respiratory health of children: The PEACE panel study in
urban and rural locations in southern Sweden European Respiratory Review, 8: 20–26
(1998).
NIEPSUJ, G. ET AL. Air pollution and respiratory health of children: The PEACE panel study in
Katowice, Poland. European Respiratory Review, 8: 86–93 (1998).
PETERS, A. ET AL. Short-term effects of particulate air pollution on respiratory morbidity in
asthmatic children. European Respiratory Journal, 10: 872–879 (1997).
RUDNAI, P. ET AL. Air pollution and the respiratory health of children: The PEACE study in
Hungary. European Respiratory Review, 8: 101–107 (1998).
SEGALA, C. ET AL. Short-term effect of winter air pollution on respiratory health of asthmatic
children in Paris. European Respiratory Journal, 11: 677–685 (1998).
TIITTANEN, P. ET AL. Fine particulate air pollution, resuspended road dust and respiratory health
among symptomatic children. European Respiratory Journal, 13: 266–273 (1999).
TIMONEN, K. L. ET AL. Air pollution and respiratory health of children: The PEACE panel study
in Kuopio, Finland. European Respiratory Review, 8: 27–35 (1998).
ZEE, S. ET AL. Air pollution and respiratory health of children: The PEACE study in
Amsterdam, The Netherlands. European Respiratory Review, 8: 44–52 (1998)
VAN DER
ZEE, S. ET AL. Acute effects of air pollution on respiratory health of 50-70 year old
adults. European Respiratory Journal, 15: 700–709 (2000).
VAN DER
VAN DER ZEE, S. ET AL.
Acute effects of urban air pollution on respiratory health of children with
and without chronic respiratory symptoms. Occupational and Environmental Medicine, 56:
802–812 (1999).
VON
KLOT, S. ET AL. Increased asthma medication use in association with ambient fine and
ultrafine particles. European Respiratory Journal, 20: 691–702 (2002).
VONDRA, V. ET AL. Air pollution and respiratory health of children: The PEACE panel study in
Prague, Czech Republic. European Respiratory Review, 8: 78–85 (1998).
EUR/04/5042688
page 68
Annex 5
META-ANALYSIS OF PM2.5 RESULTS FROM NON-EUROPEAN COUNTRIES
This Annex presents the results of an analysis of PM2.5 and daily mortality estimates extracted
from time-series studies in the Air Pollution Epidemiology Database held at St. George’s
Hospital Medical School. This was done because there were insufficient studies of PM2.5 in
Europe and consideration was given to taking studies from other countries, mainly North
America into account.
Studies from North America, Canada, South America and other parts of the world have been
identified in the database. Meta-analysis of North American and Canadian studies and all regions
together (including European studies) were carried out for each mortality group. As in the
original review, three main groups of mortality were investigated. These were all cause,
cardiovascular and respiratory mortality. The details of the studies included are shown in Tables
A, B and C for all-cause, respiratory and cardiovascular mortality respectively, together with
those that were excluded on geographical or other grounds.
Table D provides fixed- and random-effects summary estimates for PM2.5 and each of the causes
of death, for American and Canadian studies and for all studies. The estimates are the relative
risks associated with 10 µg/m3 increases in PM2.5. The European estimates have been added for
comparison. Figures A5.1–A5.3 present these estimates graphically using forest plots.
The summary estimates for North America are larger than for any of the three European studies.
This meta-analysis does not in itself answer the question of whether it is better to use a summary
estimate based on the more numerous North American Studies or choose a single estimate from
among the European studies. What is clear is that the estimates for the largest city studied in
Europe (West Midlands Conurbation), are within the range of those from North America, and
this indicates that although this estimate is not statistically significant (lower 95% confidence
interval 0.992), it is likely that effects of PM2.5 on mortality in Europe do exist. Whether or not
these are smaller than in North America cannot be determined from the present analysis, and
would require consideration of factors such as the source and composition of PM2.5 in the
respective regions and the differences in other potential effect modifiers. One reason for the
larger estimate for North America may be positive publication bias, since a funnel plot of these
estimates demonstrates some clear asymmetry (Figure A5.4). This bias was not significant
however (P=0.08), so this is not likely to be a major reason for the regional differences. The plot
does however emphasize the importance of not relying on small numbers of less statistically
powerful individual studies.
EUR/04/5042688
page 69
Table A. All cause mortality and PM2.5
Study
period
Beta
SE
RR
RR LCL
RR UCL
Montreal
8 Canadian Cities
Toronto
Canada
Canada
Canada
1984–1993 <800
1986–1996 <800
1980–1994 <800
lag 1
lag 1
lag 0–1
0.0115
0.0119
0.0187
0.006
0.0038
0.0029
1.012
1.012
1.019
1.000
1.004
1.013
1.024
1.020
1.025
Coachella Valley
Georgia
Pittsburgh
Boston
Knoxville
Portage
St Louis
Steubenville
Topeka
United States
United States
United States
United States
United States
United States
United States
United States
United States
1989–1998
1998–1999
1989–1991
1979–1986
1980–1987
1979–1987
1979–1987
1979–1987
1979–1988
lag 4
lag 1
lag 0
lag 0–1
lag 0–1
lag 0–1
lag 0–1
lag 0–1
lag 0–1
0.0436
0.0251
0.0059
0.0218
0.0139
0.0119
0.0109
0.01
0.008
0.0222
0.0164
0.0094
0.0035
0.0061
0.0076
0.0035
0.0056
0.0144
1.045
1.025
1.006
1.022
1.014
1.012
1.011
1.010
1.008
1.000
0.993
0.988
1.015
1.002
0.997
1.004
0.999
0.980
1.091
1.059
1.025
1.029
1.026
1.027
1.018
1.021
1.037
Los Angeles
Eastern Tennessee
United States
United States
1980–1986 <800
1985–1986 <800
lag 0
lag 1
0.0011
0.0228
0.002
0.0186
1.001
1.023
0.997
0.986
1.005
1.061
Wayne County
Santiago
United States
Chile
1992–1994 <800
1988–1996 <800
lag 3
lag 1–2
0.0122
0.0071
0.0075
0.0011
1.012
1.007
0.997
1.005
1.027
1.009
Mexico City
Chongqing
Melbourne
Sydney
Mexico
China
Australia
Australia
1993–1995
1995–1995
1991–1996
1989–1993
<800
<800
<800
<800
lag 1–5
lag 3
lag 0
lag 0
0.0147
–0.004
0.008
0.0153
0.0075
0.0034
0.0087
0.006
1.015
0.996
1.008
1.015
1.000
0.989
0.991
1.004
1.030
1.003
1.025
1.027
West Midlands
United Kingdom
1994–1996 <800
lag 0–1
0.0034
0.0061
1.003
0.991
1.015
Czech Republic (coal basin)
Erfurt
Excluded studies
St Louis
Mexico City
Santiago
Mexico City
Czech Republic
Germany
1982–1994 <800
1995–1998 <800
lag 1
lag 3
0.0057
–0.0165
0.004
0.0084
1.006
0.984
0.998
0.968
1.014
1.000
USA
Mexico
Chile
Mexico
1985–1986
1993–1995
1988–1993
1993–1995
lag 1
lag 4
0.0171
0.0135
0.004
0.0469
0.0096
0.0059
0.0011
0.019
1.017
1.014
1.004
1.048
0.998
1.002
1.002
1.010
1.037
1.025
1.006
1.088
City
Country
ICD
<800
<800
<800
<800
<800
<800
<800
<800
<800
<800
<800
<800
<800
Lag
lag 3
EUR/04/5042688
page 70
Table B. Cardiovascular mortality and PM2.5
City
Country
Study
period
ICD group
Lag
Beta
SE
RR D
RR LCL
RR UCL
Montreal
Canada
1984–1993 390–459
lag 1
0.0133
0.0092
1.013
0.995
1.032
Coachella Valley
United States
1989–1998 393–440
lag 4
0.0328
0.0282
1.033
0.978
1.092
Phoenix
United States
1995–1997 390–448
lag 1
0.0685
0.0236
1.071
1.022
1.122
Wayne County
United States
1992–1994 390–459
lag 1
0.0125
0.0111
1.013
0.991
1.035
Mexico City
Mexico
1993–1995
lag 1–5
0.0154
0.0143
1.016
0.988
1.044
Melbourne
Australia
1991–1996 390–459
lag 0
0.003
0.0123
1.003
0.979
1.027
Sydney
Australia
United
Kingdom
1989–1993 390–459
lag 0
0.0158
0.0083
1.016
1.000
1.033
1994–1996 390–459
lag 0–1
0.0051
0.0087
1.005
0.988
1.022
0.0217
0.0111
1.022
1.000
1.044
West Midlands
Excluded studies
Mexico City
Santa Clara County,
California
Mexico
390–398,
401–417,
420, 430–
1993–1995 438, 440–448 lag 4
United States
1989–1996 390–459
lag 0
0.0242
1.024
Montreal
Canada
1984–1993 390–459
lag 0–2
0.0104
1.010
EUR/04/5042688
page 71
Table C. Respiratory mortality and PM2.5
Country
Study
period
Montreal
Coachella Valley
Canada
United States
1984–1993
1989–1998
Los Angeles
United States
1980–1986
Wayne County
United States
1992–1994
Mexico City
Mexico
1993–1995
Melbourne
Australia
1991–1996
460–519
lag 0
–0.007
0.0297
0.993
0.937
1.053
Sydney
West Midlands
Australia
1989–1993
United Kingdom 1994–1996
460–519
460–519
lag 1
lag 0–1
0.0231
–0.0006
0.0183
0.0157
1.023
0.999
0.987
0.969
1.061
1.031
Mexico
1993–1995
460–466, 480–487,
490–496, 500–508
lag 4
0.0247
0.0183
1.025
0.989
1.063
1984–1993
460–519
lag 1
0.0451
1.046
1991–1995
460–519
11, 35, 472–519,
710.0, 710.2, 710.4
lag 0–1
0.0058
1.006
lag 0
0.0436
1.045
City
ICD group
460–519
460–519
460–519
Beta
SE
RR
lag 1
lag 4
Lag
0.0492
–0.057
0.0212
0.0834
1.050
0.945
RR LCL RR UCL
1.008
0.802
1.095
1.112
lag 0
0.0082
0.0056
1.008
0.997
1.019
lag 0
0.009
0.0268
1.009
0.957
1.063
lag 1–5
0.0354
0.0235
1.036
0.989
1.085
Excluded studies
Mexico City
Montreal
Canada
Philadelphia Pennsylvania
United States
Counties NJ counties
Santa Clara County,
United States
California
1989–1996
EUR/04/5042688
page 72
Table D. Relative risk summary estimates (FE Fixed–Effects, RE Random–Effects) for PM2.5
and daily mortality. Relative risks are for a 10 µg/m3 increases in PM2.5
All Cause
1.010 (1.008, 1.013) FE
1.013 (1.008, 1.018) RE
United
States and
Canada
1.008 (1.006, 1.009) FE
Global
Europe*
1.009 (1.006, 1.013) RE
1.003 (0.992, 1.015) WM
1.006 (0.998, 1.014) CR
0.984 (0.968, 1.000) ER
Cardiovascular
Respiratory
1.019 (1.005, 1.032) FE
1.023 (1.003, 1.044) RE
1.011 (1.000, 1.021) FE
1.016 (0.994, 1.038) RE
1.013 (1.005, 1.021) FE
1.013 (1.005, 1.022) RE
1.005 (0.998, 1.022) WM
1.011 (1.002, 1.020) FE
1.011 (1.002, 1.020) RE
0.944 (0.969,1.031) WM
*:WM – West Midlands
CR – Czech Republic
ER – Erfurt
Fig. A5.1. All cause mortality. Percentage change in mean number of deaths associated
with 10 µg/m3 increase in daily PM2.5
10
8
RR in percent
6
Summary
Estimate North
America
4
2
0
-2
8
C
an Mo
ad nt
ia re
n al
C
C
To ities
oa
ro
ch
nt
el
o
la
Va
G lle
Pi eor y
tts gi
bu a
Bo rgh
Kn ston
ox
Po vill
rt e
St St age
eu Lo
be uis
nv
Ea
st Lo To ille
er s pe
n A k
W Te nge a
ay nn le
ne es s
C see
ou
n
Sa ty
M nt
ex ia
g
C i co o
ho C
ng ity
qi
ng
M
el
bo
u
Sy rne
W
d
e
n
C st M ey
ze
ch idla
R nd
ep s
ub
Er lic
fu
rt
-4
EUR/04/5042688
page 73
Fig. A5.2. Cardiovascular mortality. Percentage change in mean number of deaths
associated with 10 µg/m3 increase in daily PM2.5
14
12
10
RR in percent
8
6
4
2
0
-2
W
es
t
M
id
l
an
ds
Sy
dn
ey
M
el
b
ou
rn
e
C
ity
co
ex
i
M
ix
oa
ch
el
la
Va
lle
W
ay
y
ne
C
ou
nt
y
Ph
oe
n
C
M
on
tre
al
-4
Fig. A5.3. Respiratory mortality. Percentage change in mean number of deaths associated
with 10 µg/m3 increase in daily PM2.5
15
10
0
-5
-10
-15
-20
id
la
nd
s
W
es
tM
M
el
bo
ur
n
Sy e
dn
ey
C
ity
M
ex
ic
o
An
ge
ay
le
s
ne
C
ou
nt
y
W
Lo
s
C
oa
ch
el
la
Va
lle
y
-25
M
on
tre
al
RR in percent
5