Infectious Disease 11-ID-15
advertisement

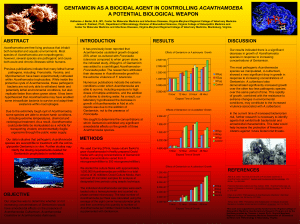
11-ID-15 Committee: Infectious Disease Title: Case Definitions for Non-notifiable Infections Caused by Free-living Amebae (Naegleria fowleri, Balamuthia mandrillaris, and Acanthamoeba spp.) I. Statement of the Problem Free-living amebae infections can cause corneal keratitis, blindness or severe, neurologic illnesses that commonly result in death. Although these infections are rare and not currently nationally notifiable, creating standardized case definitions would facilitate more systematic collection of clinical, epidemiologic, and laboratory data to assist in understanding the risk factors for infection with free-living amebae and increase the potential for development of future prevention recommendations. II. Background and Justification Infections caused by free-living amebae (Naegleria fowleri, Balamuthia mandrillaris, and Acanthamoeba [keratitis and non-keratitis infections]) have been well documented worldwide. These amebae can cause fatal or severe skin, eye, and neurologic infections (e.g., N. fowleri causes primary amebic meningoencephalitis [PAM]; B. mandrillaris and several species of Acanthamoeba cause granulomatous amebic encephalitis [GAE]; and Acanthamoeba can also cause keratitis). Annually, during 2005–2008, 3–6 fatal N. fowleri infections occurred underscoring that although these infections are rare, the outcomes are often severe and can undermine the public’s confidence in certain public recreational activities (e.g., swimming in fresh water lakes). A recent case in a Northern tier state (with no history of recent travel) indicates these organisms might be more geographically widespread than previously thought. Clusters of cases associated with organ transplantation occurred in 2009 and 2010, indicating the potential for multiple persons being affected by one source case. Currently, no standardized case definitions exist to facilitate collection of uniform clinical, epidemiologic, and laboratory data, or to serve as a guide for state and local health agencies to use in characterizing such severe illnesses. III. Statement of the desired action(s) to be taken 1. Establish standard reporting and case classification for non-notifiable diseases caused by N. fowleri, B. mandrillaris, and Acanthamoeba spp. (including keratitis) and recommend that any State or Territory conducting surveillance for these conditions using standard reporting and case classification. 2. CSTE recommends that State and Territories conducting surveillance according to these methods consider reporting case information to CDC. 3. CSTE recommends that CDC publish data on disease caused by N. fowleri, B. mandrillaris, and Acanthamoeba spp. (including keratitis) as appropriate. Page 1 of 10 In addition, CSTE calls upon CDC to 1) work with the American Medical Association and other partners to expand physician education regarding the diagnosis and treatment of PAM, GAE, Acanthamoeba keratitis, and other free-living amebic infections, and 2) increase public education about PAM, GAE, Acanthamoeba keratitis, and other free-living amebic syndromes to promote prevention and early recognition. IV. Goals of Surveillance Although free-living amebae infections are non-notifiable diseases, the purpose of this statement is to provide standardized case definitions to facilitate better understanding of these diseases and identify potential prevention measures. The goals of surveillance for free-living amebae infections are to monitor the geographic distribution and temporal trends in disease, and to collect standardized epidemiologic and clinical data to better characterize the illnesses to inform prevention measures. V. Methods for Surveillance: Surveillance for free-living amebae infections should use the following recommended sources of data and the extent of coverage listed in Table V. Table V. Recommended sources of data for case identification and extent of coverage for ascertaining cases of free-living amebae infections. Source of data for case identification Clinician reporting Laboratory reporting Reporting by other entities (e.g., hospitals, veterinarians, pharmacies) Death certificates Hospital discharge or outpatient records Extracts from electronic medical records Telephone survey School-based survey Other: media accounts Coverage Population-wide Sentinel sites X X X X X X VI. Criteria for case identification A. Narrative: A description of suggested criteria that may be for case ascertainment of a specific condition. Voluntary reporting of all illness to public health authorities that meets any of the following criteria: Page 2 of 10 1. Any person with clinical signs and/or symptoms consistent with primary amebic meningoencephalitis, granulomatous amebic encephalitis, or corneal keratitis who has a positive laboratory test for N. fowleri, Acanthamoeba spp., or Balamuthia spp. These tests may include any of the following: a. Isolation of free-living amebae in culture from a clinical specimen b. Detection of free-living amebae antigen or nucleic acid from a clinical specimen 2. Any person whose healthcare record or death certificate contains a diagnosis of primary amebic meningoencephalitis, granulomatous amebic encephalitis, or Acanthamoeba keratitis 3. Any person with ocular or neurologic manifestations consistent with free-living amebae infection after having receiving an organ or transplanted tissue from a person confirmed or suspected to have a free-living amebae infection Table VI-B. Table of criteria to determine whether a case should be reported to public health authorities. Criterion Reporting Clinical Evidence Primary amebic meningoencephalitis O Granulomatous amebic encephalitis O Acanthamoeba corneal keratitis O A person whose healthcare record contains a diagnosis of S primary amebic meningoencephalitis, granulomatous amebic encephalitis, or Acanthamoeba keratitis A person whose death certificate contains a diagnosis of S primary amebic meningoencephalitis, granulomatous amebic encephalitis, or Acanthamoeba keratitis Laboratory Evidence Isolation of N. fowleri, Acanthamoeba spp., or Balamuthia O spp. in culture from clinical specimen Detection of N. fowleri, Acanthamoeba spp., or Balamuthia O spp. antigen or nucleic acid from clinical specimen Epidemiological Evidence Any person with ocular or neurologic manifestations S consistent with free-living amebae infection after having receiving an organ or transplanted tissue from a person confirmed or suspected to have a free-living amebae infection Notes: S = This criterion alone is Sufficient to report a case. N = All “N” criteria in the same column are Necessary to report a case. O = At least one of these “O” (Optional) criteria in each category (e.g., clinical evidence and laboratory evidence) in the same column—in conjunction with all “N” criteria in the same column—is required to report a case. Page 3 of 10 C. Disease-specific data elements Disease-specific data elements to be included in the initial report are listed below. Basic demographics (e.g. age, sex, race, ethnicity, state of residence) Clinical Information Date of onset Reported symptoms of illness Recorded diagnoses Hospitalization Outcome Concurrent or pre-existing conditions (to include any recent trauma or immunosuppressing conditions) Medication and treatment Results of biopsies and cerebrospinal fluid studies (if applicable) Epidemiological Risk Factors Recreational or occupational water exposure in past 10 days (including type of water venue, location, and date[s] of exposure) Description of water-related activities (e.g., head submersion, diving, rough horseplay, water skiing, use of water slides, swings or other equipment at recreational water venue) or other outdoor activities (e.g., landscaping, gardening) Environmental conditions during period of water exposure if available (e.g., ambient air temperature, water temperature, water turbidity, presence of aquatic vegetation at recreational water venue, source of water) Travel in past 10 days Contact lens use (for corneal keratitis) Recent ill contacts Illness among coparticipants at recreational water venue Drinking untreated water Receipt of organs or tissues from persons having confirmed or suspected free-living amebae infection Laboratory Information Method(s) of laboratory testing (culture, PCR, antigen) Type of antigen testing Molecular characterization of organism (if available) VII. Case Definition for Case Classification A. Narrative: Description of criteria to determine how a case should be classified. Page 4 of 10 1) Naegleria fowleri Causing Primary Amebic Meningoencephalitis (PAM) Clinical description N. fowleri is a free-living ameboflagellate that invades the brain and meninges via the nasal mucosa and olfactory nerve to cause acute, fulminant hemorrhagic meningoencephalitis (primary amebic meningoencephalitis – PAM), primarily in healthy children and young adults with a recent history of exposure to warm fresh water. Initial signs and symptoms of PAM begin 1 to 14 days after infection and include sudden onset of headache, fever, nausea, vomiting, and stiff neck accompanied by positive Kernig’s and Brudzinski’s signs. In some cases, abnormalities in taste or smell, nasal obstruction and nasal discharge might be seen. Other symptoms might include photophobia, mental-state abnormalities, lethargy, dizziness, loss of balance, other visual disturbances, hallucinations, delirium, seizures, and coma. After the onset of symptoms, the disease progresses rapidly and usually results in death within 3 to 7 days. Although a variety of treatments have been shown to be active against amebae in vitro and have been used to treat infected persons, most infections have still been fatal. Laboratory-confirmed N. fowleri infection is defined as the detection of N. fowleri 1) Organisms in CSF, biopsy, or tissue specimens, or 2) Nucleic acid (e.g,. polymerase chain reaction) in CSF, biopsy, or tissue specimens, or 3) Antigen (e.g., direct fluorescent antibody) in CSF, biopsy, or tissue specimens. Case classification Confirmed: a clinically compatible illness that is laboratory confirmed.* * When available, molecular characterization should be documented (e.g., genotype). Comment N. fowleri might cause clinically similar illness to bacterial meningitis, particularly in its early stages. Definitive diagnosis by a reference laboratory might be required. Unlike Balamuthia mandrillaris and Acanthamoeba spp., Naegleria fowleri is commonly found in CSF. 2) Balamuthia mandrillaris Disease Clinical description B. mandrillaris is an opportunistic free-living ameba that can invade the brain through the blood, probably from a primary infection in the skin (from ulcers or dermatitis), sinuses, or via organ transplantation. The incubation period is not well-characterized but has been observed to range from 2 weeks to months or possibly years. Once in the brain, the amebae can cause meningoencephalitis and/or granulomatous amebic encephalitis (GAE). B. mandrillaris GAE often has a slow, insidious onset and develops into a subacute or chronic disease lasting several weeks to months; however, B. mandrillaris infections associated with organ transplantation have an especially rapid clinical course. B. mandrillaris GAE affects both immunocompetent persons and persons who are immunosuppressed from a variety of causes (e.g., HIV/AIDS, organ Page 5 of 10 transplantation). Initial symptoms of B. mandrillaris GAE might include headache, photophobia, and stiff neck accompanied by positive Kernig’s and Brudzinski’s signs. Other symptoms might include nausea, vomiting, low-grade fever, muscle aches, weight loss, mental-state abnormalities, lethargy, dizziness, loss of balance, cranial nerve palsies, other visual disturbances, hemiparesis, seizures, and coma. Painless skin lesions appearing as plaques a few millimeters thick and one to several centimeters wide have been observed in some patients, especially patients outside the U.S., preceding the onset of neurologic symptoms by 1 month to approximately 2 years. Once the disease progresses to neurologic infection, it is generally fatal within weeks or months; however, a few patients have survived this infection. Laboratory criteria for diagnosis Laboratory-confirmed B. mandrillaris infection is defined as the detection of B. mandrillaris 1) Organisms in CSF, biopsy, or tissue specimens, or 2) Nucleic acid (e.g,. polymerase chain reaction) in CSF, biopsy, or tissue specimens, or 3) Antigen (e.g., direct fluorescent antibody) in CSF, biopsy, or tissue specimens. Case classification Confirmed: a clinically compatible illness that is laboratory confirmed.* * When available, molecular characterization should be documented (e.g., genotype). Comment B. mandrillaris and Acanthamoeba spp. can cause clinically similar illnesses and might be difficult to differentiate using commonly available laboratory procedures. Definitive diagnosis by a reference laboratory might be required. A negative test on CSF does not rule out B. mandrillaris infection because the organism is not commonly present in the CSF. 3) Acanthamoeba Disease (excluding keratitis) Clinical description The genus Acanthamoeba includes several species of opportunistic free-living amebae that might invade the brain through the blood, probably from a primary infection in the skin (from ulcers or dermatitis) or sinuses. Once in the brain, the amebae cause granulomatous amebic encephalitis (GAE). Acanthamoeba GAE has a slow and insidious onset and develops into a subacute or chronic disease lasting several weeks to months. Acanthamoeba GAE affects both immunocompetent persons and persons who are immunosuppressed from a variety of causes (e.g., HIV/AIDS, organ transplantation). Initial symptoms of Acanthamoeba GAE might include headache, photophobia, and stiff neck accompanied by positive Kernig’s and Brudzinski’s signs. Other symptoms might include nausea, vomiting, low-grade fever, muscle aches, weight loss, mental-state abnormalities, lethargy, dizziness, loss of balance, cranial nerve palsies, other visual disturbances, hemiparesis, seizures, and coma. Once the disease progresses to neurologic Page 6 of 10 infection, it is generally fatal within weeks or months. However, a few patients have survived this infection. Laboratory-confirmed Acanthamoeba spp. infections (excluding keratitis) are defined as the detection of Acanthamoeba spp. 1) Organisms in CSF, biopsy, or tissue specimens, or 2) Nucleic acid (e.g,. polymerase chain reaction) in CSF, biopsy, or tissue specimens, or 3) Antigen (e.g., direct fluorescent antibody) in CSF, biopsy, or tissue specimens. Case classification Confirmed: a clinically compatible illness that is laboratory confirmed.* *When available, species designation and molecular characterization (e.g., genotype) should be documented. Comment Acanthamoeba and B. mandrillaris can cause clinically similar illnesses and might be difficult to differentiate using commonly available laboratory procedures. Definitive diagnosis by a reference laboratory might be required. Several species of Acanthamoeba are associated with infection (i.e., A. castellanii, A. culbertsoni, A. hatchetti, A. healyi, A. polyphaga, A. rhysodes, A. astonyxis, A. lenticulata and A. divionensis). A negative test on CSF does not rule out Acanthamoeba infection because the organism is not commonly present in the CSF. 4) Acanthamoeba keratitis Clinical description Acanthamoeba keratitis is a local infection of the cornea (outer layer of the visual pathway of the eye) caused by a microscopic, free-living ameba belonging to the genus Acanthamoeba. Symptoms include foreign body sensation, photophobia, decreased visual acuity, tearing, pain, and redness of the eye. It occurs most typically among healthy, contact lens users, but can occur in anyone. Although treatable with topical medications, affected individuals are at risk for permanent visual impairment or blindness. Acanthamoeba organisms are ubiquitous in nature and can be found in bodies of water (e.g., lakes and oceans), soil, and air. Laboratory-confirmed Acanthamoeba spp. keratitis infections are defined as the detection of Acanthamoeba spp. 1) Organisms in corneal scraping, or biopsy specimens, or 2) Nucleic acid (e.g., polymerase chain reaction) in corneal scraping, or biopsy specimens, or 3) Antigen (e.g., direct fluorescent antibody) in corneal scraping, or biopsy specimens. Page 7 of 10 Case classification Confirmed: a clinically compatible illness that is laboratory confirmed.* *When available, species designation and molecular characterization (e.g., genotype) should be documented. Probable: a clinically compatible illness with positive identification of Acanthamoeba trophozoites or cysts using confocal microscopy. B. Classification Tables Table VII-B. Criteria for defining a case of free-living amebae infection. Criterion Clinical Evidence Primary amebic meningoencephalitis Granulomatous amebic encephalitis Corneal keratitis Laboratory evidence Isolation of N. fowleri, Acanthamoeba spp., or Balamuthia spp. in culture from clinical specimen Detection of N. fowleri, Acanthamoeba spp., or Balamuthia spp. antigen or nucleic acid from clinical specimen Positive identification of Acanthamoeba trophozoites or cysts using confocal microscopy. Confirmed N. fowleri causing PAM Confirmed Balamuthia mandrillaris Disease N O O Confirmed Probable Confirmed Acanthamoeba Acanthamoeba Acanthamoeba Keratitis Keratitis Disease (excluding keratitis) N N O O O O O O O O N N Notes: S = This criterion alone is Sufficient to classify a case. N = All “N” criteria in the same column are Necessary to classify a case. Page 8 of 10 O = At least one of these “O” (Optional) criteria in each category (e.g., clinical evidence and laboratory evidence) in the same column—in conjunction with all “N” criteria in the same column—is required to classify a case VIII. Period of Surveillance Surveillance should be ongoing. IX. Data sharing/release and print criteria Data will be used to determine the burden of illness due to free-living amebae infections, monitor trends in illness over time, assess the effectiveness of control measures, and monitor progress in prevention. Information may be distributed among states and territories or to CDC according to jurisdiction specific protocols. Unusual situations may increase the need for communication. For example, multi-state investigation of transplantation-related infections might require sharing of data among health departments and/or state and federal agencies in several jurisdictions involved in investigations. State-specific data on cases, if shared with CDC, will be verified prior to publication. Only de-identified case data will be released by CDC to the general public X. References 1. Primary amebic meningoencephalitis--Arizona, Florida, and Texas, 2007. Centers for Disease Control and Prevention (CDC). MMWR Morb Mortal Wkly Rep. 2008 May 30;57(21):573-7. 2. The epidemiology of primary amoebic meningoencephalitis in the USA, 1962-2008. Yoder JS, Eddy BA, Visvesvara GS, Capewell L, Beach MJ. Epidemiol Infect. 2010 Jul;138(7):968-75. Epub 2009 Oct 22. 3. Pathogenic and opportunistic free-living amoebae: Acanthamoeba spp., Balamuthia mandrillaris, Naegleria fowleri, and Sappinia diploidea. Visvesvara GS, Moura H, Schuster FL. FEMS Immunol Med Microbiol. 2007 Jun;50(1):1-26. Epub 2007 Apr 11 Page 9 of 10 XI. Coordination Agencies for Response: (1) Centers for Disease Control and Prevention Tom Frieden, MD, MPH Director, CDC 1600 Clifton Road NE; Mailstop D-14 Atlanta, GA 30333 (404) 639-7000 Txf2@cdc.gov XII. Submitting Author: (1) Carina Blackmore, DVM, PhD. Dipl. ACVPM State Public Health Veterinarian Florida Department of Health 4052 Bald Cypress Way Bin A08 Tallahassee FL 32330 850-245-4299 Carina_blackmore@doh.state.fl.us Co-Authors: (1) Tiffani Onifade, MS, PhD. Statewide Coordinator of Food and Waterborne Disease Florida Department of Health 4052 Bald Cypress Way Bin A08 Tallahassee FL 32330 850-245-4116 tiffiani_onifade@doh.state.fl.us (2) Michael J. Beach, PhD Associate Director for Healthy Water, National Center for Emerging and Zoonotic Infectious Diseases Centers for Disease Control and Prevention 1600 Clifton Road NE Atlanta, GA 30333 (770) 488-7763 mbeach@cdc.gov Page 10 of 10