Eff ects of policy options for human resources for health: Articles Summary
advertisement

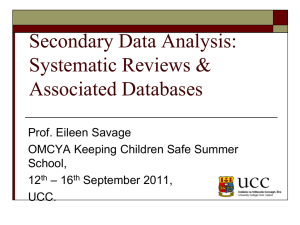
Articles Effects of policy options for human resources for health: an analysis of systematic reviews Mickey Chopra, Salla Munro, John N Lavis, Gunn Vist, Sara Bennett Summary Lancet 2008; 371: 668–74 See Editorial page 623 See Comment page 629 Health Systems Research Unit, Medical Research Council of South Africa, Cape Town, South Africa (M Chopra MSc, S Munro MA); Norwegian Knowledge Centre for the Health Services, Oslo, Norway (G Vist PhD); Department of Clinical Epidemiology and Biostatistics, McMaster University, Ontario, Canada (J N Lavis MD); and Alliance for Health Policy and Systems Research, World Health Organization, Geneva, Switzerland (S Bennett PhD) Correspondence to: M Chopra, Health Systems Research Unit, MRC, Van Zyl Drive, Parow, Western Cape 7535, South Africa mickey.chopra@mrc.ac.za Background Policy makers face challenges to ensure an appropriate supply and distribution of trained health workers and to manage their performance in delivery of services, especially in countries with low and middle incomes. We aimed to identify all available policy options to address human resources for health in such countries, and to assess the effectiveness of these policy options. Methods We searched Medline and Embase from 1979 to September, 2006, the Cochrane Library, and the Human Resources for Health Global Resource Center database. We also searched up to 10 years of archives from five relevant journals, and consulted experts. We included systematic reviews in English which assessed the effects of policy options that could affect the training, distribution, regulation, financing, management, organisation, or performance of health workers. Two reviewers independently assessed each review for eligibility and quality, and systematically extracted data about main effects. We also assessed whether the policy options were equitable in their effects; suitable for scaling up; and applicable to countries with low and middle incomes. Findings 28 of the 759 systematic reviews of effects that we identified were eligible according to our criteria. Of these, only a few included studies from countries with low and middle incomes, and some reviews were of low quality. Most evidence focused on organisational mechanisms for human resources, such as substitution or shifting tasks between different types of health workers, or extension of their roles; performance-enhancing strategies such as quality improvement or continuing education strategies; promotion of teamwork; and changes to workflow. Of all policy options, the use of lay health workers had the greatest proportion of reviews in countries with a range of incomes, from high to low. Interpretation We have identified a need for more systematic reviews on the effects of policy options to improve human resources for health in countries with low and middle incomes, for assessments of any interventions that policy makers introduce to plan and manage human resources for health, and for other research to aid policy makers in these countries. Introduction Quality health care depends on policies to ensure that health workers who are capable of delivering such care are available in sufficient numbers.1 Challenges related to human resources for health are particularly acute in countries with low and middle incomes. These challenges include an absolute shortage of qualified staff, especially in sub-Saharan Africa; an inequitable distribution of health workers, with too few in remote rural areas; and staff absenteeism and poor motivation that are probably caused by low pay, poor supervision and support, and unsatisfactory working conditions.2 Ways to address these challenges, which have increasingly been recognised as primary barriers to scaling up the delivery of effective health services, have been outlined.1–4 To make the best use of scarce resources, policy makers who are charged with the provision of effective and equitable health care need evidence that will help them to identify and select policy options. Frameworks to conceptualise the key issues related to human resources for health have been developed,1,2 and evidence about improving the performance of health workers has been reviewed.5 However, the full range of possible policy options has not been reviewed. 668 Policy makers need systematic reviews to help them to identify, select, appraise, and synthesise research findings.6 Systematic reviews could increase confidence for policy makers about the probable effects of different policy options and reduce the risk of high opportunity costs associated with implementation of inappropriate policies.7 Systematic reviews can inform policy makers about how a particular policy option was implemented in other contexts, and about how they could assess it in their own context,6 but might not be applicable in countries with low and middle incomes, where human resources are problematic.8 For example, the effects of performance-based pay or contracting of private practitioners are dependent on capacity to manage such measures, which varies between health systems; some countries with low or middle incomes have very little capacity to manage such policies. However, criteria have been developed to assist policy makers to assess the applicability of research to different settings. We aimed to list all possible policy options (grouped by key objectives); to identify effects and outcomes for which evidence exists and those for which it is lacking; and to synthesise conclusions for countries with low or middle incomes. www.thelancet.com Vol 371 February 23, 2008 Articles Methods We adapted, expanded, and combined several existing frameworks to generate a comprehensive list of possible policy options, grouped by key objectives and their possible effects, and by outcomes for human resources for health.1,2 We further refined the list by soliciting input from both researchers and policy makers. We searched Medline Ovid and Embase Ovid, from 1979 to September, 2006; the Cochrane Library (which includes both the Cochrane Database of Systematic Reviews and the Database of Reviews of Effectiveness); and the Human Resources for Health Global Resource Center database. We searched for systematic reviews and metaanalyses of manpower and personnel in developing countries. We used the following subject headings and text words: “health manpower”, “foreign professional personnel”, “foreign medical graduates”, “emigration”, “immigration”, “migration”, “human resources”, “health manpower”, “foreign personnel”, “foreign graduate”, “brain drain”, “border crossing”, “health personnel”, “personnel management”, “health services needs and demand”, “resource allocation”, “health care rationing”, and “international educational exchange”. We searched back issues of Bulletin of the World Health Organization, Health Policy and Planning, Human Resources for Health, Human Resources for Health Development, and Implementation Science for ten years, or since the earliest publication if this was more recent. We searched the reference lists of the reviews that we identified. We also asked experts about existing reviews and those that were underway or being updated. Two researchers independently assessed the titles and abstracts that were identified by the searches. Studies that did not meet one or more of our inclusion criteria were excluded at this stage. The remaining articles were retrieved and assessed in full text. We included systematic reviews if they were published in English; if they examined the effects of policy options that could affect the supply, distribution, efficiency, and performance of health workers; and if their methods sections contained explicit selection criteria. If a systematic review had been updated we only included the most recent version. We gave financial assistance to two review teams (the systematic review about underserved areas9 and the systematic review about use of lay health workers10) to complete their work in time to be included. Two researchers independently determined eligibility, extracted data, and assessed quality for each review. We extracted information on the background and origin (setting and country) and characteristics of each of the studies that were included in the systematic reviews. We collected information about the quality of analysis and the main results of the systematic reviews. We also assessed whether the policy options reviewed in the studies were equitable, suitable for scaling up, and applicable to countries with low and middle incomes. Disagreements www.thelancet.com Vol 371 February 23, 2008 between researchers were resolved by discussion. We developed forms to use for standardised data extraction, and used a checklist for quality assessment of the systematic reviews. We evaluated whether the quality of the evidence for each important outcome was either high, moderate, low, or very low according to four main criteria: study design, study limitations, consistency, and directness.11,12 We used a so-called GRADE evidence profile to summarise these results for each of the critical outcomes in the comparison and the average profile for the systematic reviews were assessed.11,12 Supply (quantity) of health workers Distribution of health workers Efficient use Performance of health of health workers workers Training interventions Increase numbers of new students Yes Recruit foreign graduates Yes Recognise previous learning Yes Improve curriculum content Yes Yes Yes9 Adjust relative numbers of specialist, generalist, and midlevel training positions Yes Refine admission criteria Yes9 Yes Use reserved entry or quotas for specific groups Yes Yes Introduce conditional scholarships Yes Yes Diversify location of training sites Yes9 Yes Involve communities (eg, in selection of trainees) Yes Yes Recruit and train faculty Yes Introduce training approaches (eg, problem-based learning) Yes Regulatory mechanisms Recognise overseas qualifications Yes Introduce temporary employment regulations Yes Yes9 Yes Yes Expand roles of midlevel workers Yes Require service in underserved regions Yes9 Restrict migration of workers Yes Ensure competence Yes Introduce malpractice regulations Yes Financial mechanisms Increase trainee salaries Yes Yes Raise wages Yes Yes Provide non-wage benefits Yes Yes Introduce incentives for return of skilled migrants Yes Establish retirement policies Yes Align pay with performance Yes Yes Yes13 Alter remuneration methods (eg, fee for service, list, or salary) Yes Yes Yes13,14 Provide technology and supplies Yes Yes Yes Adjust relative remuneration Provide incentives for workers in underserved regions Yes9,15 (Continues on next page) 669 Articles Supply (quantity) of health workers Distribution of health workers Efficient use Performance of health of health workers workers (Continued from previous page) Organisational mechanisms Change recruitment policies Introduce performance management systems Yes Change workflow or workload Yes16–18 Yes Increase numbers of nurses Yes Yes19–21 Improve information flow or use electronic health records Yes22 Yes Allow medical care for staff (eg, HIV/ AIDS treatment) Yes Yes Employ lay health workers Yes10 Yes10 Yes10 Use private-sector workers Yes Integrate health-care services Yes23 Decentralise health care Yes Yes Promote team work Yes22,24 Use community health planning Yes24,25 Yes Substitute or extend roles of health workers Yes10,26–32 Involve the community Adopt quality improvement and continuous education strategies Yes25,33–38 Macro policies and mechanisms in other sectors Estimate human resource needs and plan for supply Yes Yes Yes Regulate the civil service Yes Yes Yes Table 1: Policy options that could affect outcomes for human resources in health 759 potentially relevant articles identified and screened 725 articles excluded 716 not relevant 9 not systematic reviews 34 articles retrieved for more detailed evaluation 6 articles excluded 5 not relevant 1 near-duplicate 28 systematic reviews of effects analysed Figure: Study profile Role of the funding source The sponsor of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication. 670 Results Table 1 shows policy options grouped by key objectives in human resources for health—namely, training, regulations, financing, organisational mechanisms, and macro policies and mechanisms in other sectors. The possible effects of the policy options were grouped by key outcomes for human resources for health, as described by WHO.1 Our search yielded 759 references, of which 28 systematic reviews of effects were deemed eligible for analysis (figure). Of these 28, only a few included studies from countries with low and middle incomes, and some reviews were of low quality (table 2). Most of these systematic reviews focused on policy options to alter the organisation of human resources; only a few investigated training interventions, financial mechanisms, or regulations. We identified no reviews about wider country-level policies or policies in other sectors that might affect human resources for health care. The main organisational mechanisms investigated in these trials were substitution or extension of the roles of health workers, and strategies to improve quality of health care and implement continuous education. Only one review addressed the effects of training and regulatory mechanisms on improving the distribution of health workers to underserved regions (table 2).9 The review reported that no studies of effects met their eligibility criteria, and none of the studies were from countries with low and middle incomes. However, the investigators did note that changes in the admission policies of medical schools (eg, bias towards male applicants or those with an interest in general practice or with a service orientation) and the establishment of medical schools in rural areas were associated with an increased proportion of graduates working in rural settings and underserved areas.9 In terms of financial policies, one systematic review examined the effects of performance-based incentives,11 and two the effects of remuneration methods on the performance of health workers.13,14 We identified reviews that compared renumeration methods such as fundholding, in which providers are paid for each patient registered, and capitation, in which providers are paid according to the population size covered. Compared with capitation, implementation of a fee-for-service method was associated with more primary-care visits, more visits to specialists, more diagnostic and curative services, and higher compliance with the recommended number of visits, together with fewer hospital referrals and fewer repeat prescriptions.14 Our search identified some low-quality evidence that suggested attempts to control costs through freezing the fee-per-service were countered by increased numbers of patients seen, and low-quality evidence that managed-care interventions did reduce costs.13 Compared with salaried remuneration, introduction of a fee-for-service method resulted in www.thelancet.com Vol 371 February 23, 2008 Articles Quality Studies reviewed Studies in countries with low and middle incomes Training interventions and regulatory mechanisms No reliable evidence to support policies that have been introduced to address the urban–rural gap.9 Little research on the short-term or long-term effect of measures to require service in underserved areas, or of incentives such as scholarships or bursaries with commitments for return of service.9 Average 32 0 Average 89 Not reported 4 Not available Low 10 Not reported Outreach visits with education for health-care professionals were effective, as were education and reminders.16 Assistance from nurse facilitators to design and implement office routines to increase uptake of screening programmes were effective.16 Reminder interventions were effective for physicians.16 Average 65 Not reported Organisational change (such as use of separate clinics devoted to prevention, use of planned-care visit for prevention, or specific prevention activities by non-physician staff) was more effective than financial incentives and reminders for patients.17 Patient education and feedback were least effective.17 High 108 Not reported Staffing with higher registered nurses reduced hospital-related mortality, failures to rescue, cardiac arrest, hospital-acquired pneumonia, and other adverse events.19 Low 94 0 Lower patient-to-nurse ratios and richer mixes of skills reduced inpatient mortality.20 Low 43 0 Nurse staffing was associated with patient safety; nurse characteristics and organisational factors were moderating factors.21 Low 73 Mixed results for electronic patient records for nurses and doctors.22 Data entry into a centralised computer increased physician time used for records.22 Low 23 Not reported Lay health workers can improve uptake of immunisation in children and reduce child morbidity and mortality, compared with usual care.10 Lay High health workers can also effectively promote exclusive breastfeeding up to 6 months of age, but are less effective in high-income countries than others.10 Lay health workers can improve treatment of tuberculosis compared with institution-based directly observed therapy.10 No clear evidence for other uses of lay health workers.10 48 17 (35%) Financial mechanisms Fund-holding interventions negatively affected the workloads of general practitioners.13 The effects of freezes on fee-for-service tariff were countered by increased workload.13 Managed care reduced costs of admission by 20%.13 High Compared with capitation, fee-for-service remuneration caused a greater reduction in hospital referrals and repeat prescriptions; achieved higher compliance with a recommended number of visits; and resulted in more patient visits and greater continuity of care.14 However, patient satisfaction with access to physicians was lower with fee-for-service remuneration than with salaried payment.14 Financial incentives for rural service were effective in attracting practitioners to serve in rural areas.15 Of those offered financial incentives to stay in rural practice, 29% of physicians remained in practice after 8 years, and 80% of physicians who left an index practice left rural practice.15 Organisational mechanisms Integrated primary health care services had mixed effects, but had apparent cost savings.23 Average Joint decisions by medical teams reduced average length of hospital stay for patients, but with no difference in mortality rates, or the type of care to High which patients were released.22 Staff in intervention wards were more satisfied than others, had stronger perceptions of teamwork, and better understanding of patient care.22 4 4 (100%) 2 1 (50%) Patients kept more appointments because of pharmacist services, but with little or no reduction in use of health services, and mixed effects on prescription of inappropriate drugs by pharmacists.26 Average 25 0 Some evidence that replacement model (where a primary care provider refers patients to a mental health worker) reduced psychotropic prescribing and mental-health referral in the short term, and inconsistent evidence that it reduced consultation rates.27 Some evidence that the consultant-liaison model for mental health services had a direct effect on prescribing when part of complex, multifaceted interventions.27 High 38 0 Substitution of midwives or general practitioners for obstetricians did not increase the risk of anaemia, urinary tract infection, caesarean section, malpresentation, or perinatal mortality.18 Substitution reduced of pregnancy-induced hypertension and pre-eclampsia.18 Less frequent antenatal visits did not affect preterm delivery, low birthweight, size for gestational age, pre-eclampsia, induction of labour, caesarean section, antenatal haemorrhage, admission to neonatal intensive care unit, perinatal mortality, or maternal mortality. Reduced visits cost per pregnancy were beneficial to both service and patient.18 Average 10 3 (30%) Use of care assistants led to greater organisational effectiveness.28 Some evidence that substitution of nurses for doctors could be effective.28 Low Little evidence about the effects of different skill mixes across other groups of health workers and professions, or development of new roles.28 Combinations of reminders and patient-directed interventions had moderate effects.34 Educational materials, educational meetings, and audit and feedback in combination might have, at best, a small effect on implementation of guidelines.34 Audit and feedback alone had modest effects on guideline implementation.34 Patient-mediated interventions could improve performance.34 Reminders have a moderate effect on implementation of guidelines.34 Educational materials and educational outreach were relatively ineffective.34 High Patient satisfaction was higher in patients cared for by nurses than by doctors.29 Nurses had much longer consultations and undertook more investigations.29 Nurse practitioners were as accurate as doctors in interpreting radiographs.29 37 Not reported 235 5 (2%) Average 34 1 (3%) Substitution of nurses for doctors at first contact and ongoing care made no difference to patient outcomes.30 Patient compliance, rates of consultation or direct costs did not differ.30 Tests and investigations for patients who needed urgent attention were the same or better, as was the process of care outcomes.30 Nurse-led care produced higher patient satisfaction and knowledge.30 Average 16 Not reported Insufficient evidence on the financial and opportunity costs of extended roles for health professionals.31 Evidence of effect of extended roles is limited.31 Extended scope of practice interventions can improve ease and speed of access to specialist services.31 Low 21 Not reported (Continues on next page) www.thelancet.com Vol 371 February 23, 2008 671 Articles Quality Studies reviewed Studies in countries with low and middle incomes (Continued from previous page) Substitution of more highly trained professionals by general practitioners in accident and emergency rooms reduced use of such facilities.32 General practitioners made less use of diagnostic investigations and made fewer referrals to secondary services. High 33 0 Education in evidence-based medicine had some positive effect on improved knowledge and attitudes, but little change in behaviour.33 Low 17 Not reported Increased ratio of primary health-care physicians to doctors39 was associated with lower mortality, neonatal death and rate of low birthweight babies.39 Gatekeeper system resulted in lower health-care costs and lower rate of increase in outpatient costs.39 Gatekeeper groups had lower rates of service utilisation.39 Low 47 Not reported Audit and feedback had small to moderate effects.35 Audit and feedback were less effective than reminders and opinion leaders, but more effective High than incentives.35 The contribution of audit and feedback in multifaceted interventions was small.35 118 4 (3%) Guidelines used by professionals allied to medicine did not differ from standard physician care.37 Guidelines and dissemination and/or implementation strategy vs. no guidelines effective or partially effective.37 No difference between guidelines plus dissemination and/or an intervention with opinion leaders and lectures vs. guidelines pus dissemination and/or implementation strategy with opinion leaders.37 Average 18 0 Planned educational activities had small to moderate effects on practice with interactive workshops alone or combined with didactic sessions.36 Use of didactic sessions did not show effects in practice.36 Average 32 4 (1%) Some evidence that professional performance was improved by revision of professional roles and computer systems for knowledge management.38 Some evidence that patient outcomes were improved by multidisciplinary teams, integrated care services, and computer systems.38 Cost savings were reported from integrated care services.38 Low 36 Not reported High=high quality, well designed study. Average=average quality study, with only minor limitations. Low=low quality study, with major limitations. Table 2: Main findings of systematic reviews of effects of policy options on human resource outcomes more patient visits, greater continuity of care, and higher compliance with the recommended number of visits; however, patients were less satisfied with access to their physician.14 One review reported that immunisation coverage increased in response to a performance-based incentive for doctors.11 One of the two systematic reviews that examined the effects of financial incentives for work in underserved regions was of poor quality,15 and the other identified no studies that met its inclusion criteria.9 Despite its limitations, the first review showed that students in a high-income country who were given funding on the condition that they did rural service were more likely to practise in rural regions at the end of their training than others.15 Two high-quality systematic reviews16,17 showed that organisational interventions that change workflow or workload can increase efficiency in high-income country settings. One review showed that use of nurse facilitators to design and implement office routines helped to improve uptake of preventive-screening procedures, whereas physician education and combined interventions were ineffective.16 The other review also showed that organisational changes, such as the establishment of a separate clinic devoted to prevention and screening activities, the use of a planned-care visit for prevention, or the designation of specific prevention responsibilities to non-physician staff, were much more effective than were educational approaches. Three systematic reviews, that surveyed observational studies from high-income countries, consistently showed that increased numbers of nursing staff were associated with improved inpatient outcomes.19–21 Use 672 of electronic health records was shown to have variable effects on efficiency in high-income country settings, where such interventions tend to be easier to implement than in countries with low and middle incomes.22 One systematic review10 of 48 randomised controlled trials, of which three were from South America, six from Africa, and seven from Asia, examined the use of lay health workers (also called community health workers). 39 trials examined policies that used lay health workers to increase numbers of health workers and extend services (ie, to do activities not usually provided by health professionals).10 Only four trials examined whether lay health workers could be used to broaden the distribution of services (eg, to serve remote or disadvantaged populations) or to increase efficiency (eg, to substitute for care provided by health professionals).10 The review found high quality evidence that supervision of directly observed therapy for tuberculosis patients by lay health workers produced better completion rates than supervision by institution-based therapy by nurses (p=0.05).10 We identified moderatequality evidence that an intervention with lay health workers reduced child mortality and morbidity,10 and good-quality evidence that use of lay health workers also resulted in greater uptake of immunisation in children, and promoted exclusive breastfeeding (but not the initiation of breastfeeding or any breastfeeding up to 6 months of age).10 One systematic review23 did not find any consistent benefit of integration of services in countries with low and middle incomes. Teamwork, defined as interventions to improve collaboration between doctors and nurses, www.thelancet.com Vol 371 February 23, 2008 Articles was shown to be a promising intervention, with the potential to reduce costs and have a positive effect on practitioners and patients.24 However, this review was based on two studies, only one of which was in a country with a low or middle income (Thailand). Eight systematic reviews10,26–32 examined the effects of substitution, extension of roles, or task shifting, and concluded that substituting nurses for physicians can result in comparable or better patient outcomes and satisfaction. However, these results might not be applicable to countries with low and middle incomes.30 Cost reductions could be offset by greater numbers of tests and admissions, but this would depend on the pay differentials between doctors and nurses in different settings.28 Extension of the role of general practitioners into emergency care settings reduced not only the use of such facilities, but also use of diagnostic investigations and referrals to secondary services.29 Substitution of cheaper care assistants for nurses can have mixed effects in high-income country settings but these effects have typically been shown in low-quality studies.28 Extension of the role of pharmacists in high-income country settings did not change the outcomes from those of services delivered by other health professionals.23 Substitution of lay health workers for health professionals could have mixed effects in countries with low and middle incomes.10 Six systematic reviews5,33–38 from high-income countries addressed quality improvement and continuous education strategies that aim to improve the knowledge, attitudes, and behaviours of health workers (such as audit with feedback). These can achieve, on average, a 10% improvement in performance. However, the effects for any single strategy can vary and few studies have been done in countries with low and middle incomes. Quality improvement and continuous education strategies that focus on organisational strategies (such as multidisciplinary teams for patient care and integrated care services) can improve patient outcomes in high-income country settings. Discussion Despite the widespread recognition that health workers are critical to achieving both health-related Millennium Development Goals and national health goals, and that they constitute by far the greatest expenditure in the health sector, the amount of synthesised research evidence about the effects of relevant policy options to guide policy makers in countries with low and middle incomes is inadequate. We identified a small amount of high-quality synthesised research evidence about the effects of a few policy options for improvement of human resources for health. These include organisational mechanisms that could increase efficiency (such as substitution or shifting tasks between different types of health workers, or extension of their role); organisational mechanisms that could enhance the www.thelancet.com Vol 371 February 23, 2008 performance of health workers (such as quality improvement or continuing education strategies); and organisational mechanism that could both increase efficiency and enhance performance (such as promotion of teamwork and changes to workflow). Some policy options (such as the use of lay health workers) were investigated in countries with a range of incomes, from high to low. However, since most research was done only or mainly in high-income countries, it might have little applicability to countries with low and middle incomes. This might be especially true for policy options that depend on strong organisational and management systems (eg, payment for performance or changes in workflow), or on particular price or wage differentials (eg, substitution of lower cadres of workers for nurses, or nurses for doctors). Moreover, in many domains, high-quality evidence about effects was lacking, either because studies had not been systematically reviewed (or reviewed to a high quality); because a systematic review identified no studies that met their inclusion criteria (eg, for studies of financial mechanisms); or both (eg, for policy options that address the supply and distribution of health workers). The main limitations of our study were that our search might have missed potentially eligible systematic reviews since a wide range of terminology is used to describe policy options for human resources for health; publications on this topic are poorly indexed; and we used 1979 as the base year for our search. We also excluded systematic reviews that were published in languages other than English. The systematic reviews that we identified had their own limitations, including the potential for publication bias against negative findings, their occasionally poor quality, and their limited applicability to countries with low and middle incomes. Other types of systematic reviews and other considerations will also aid policy-making processes. Policy makers need information about cost-effectiveness, relationships, mechanisms, and meanings. For example, is delivery of a programme by nurse practitioners more cost-effective than delivery by physicians? Are medical students from regions with few human resources more likely than other students to return to practise in these regions? Why would a scheme for remuneration of health workers lead to unexpected outcomes? How have training programmes been viewed and experienced by health workers? Moreover, policy makers must also contend with values and beliefs; stakeholder power; institutional constraints; flows of donor funding; and other types of information such as local assessments of need, costs, and the availability of resources. Contributors MC, SM, JL, and SB conceived of and designed the study. MC, SM, and GV analysed systematic reviews. MC, SM, SB, and JL drafted the manuscript. All authors have seen and approved the final version. 673 Articles Conflict of interest statement We declare that we have no conflict of interest. Acknowledgments We thank Uta Lehmann, David Sanders, and Jimmy Volmink for their assistance with development of the conceptual framework. References 1 WHO. 2006 World Health Report. Geneva, Switzerland: World Health Organization, 2006. 2 Joint Learning Initiative. Human resources for health: overcoming the crisis. Cambridge MA, USA: Harvard University Press, 2004. 3 WHO. 1997 World Health Report. Geneva, Switzerland: World Health Organization, 1997. 4 WHO. 2000 World Health Report. Geneva, Switzerland: World Health Organization; 2000. 5 Rowe AK, de Savigny D, Lanata CF, Victora CG. How can we achieve and maintain high-quality performance of health workers in low-resource settings? Lancet 2005; 366: 1026–35. 6 Lavis JN, Posada FB, Haines A, Osei E. Use of research to inform public policymaking. Lancet 2004; 364: 1615–21. 7 Egger M, Smith GD, Sterne JA. Uses and abuses of meta-analysis. Clin Med 2001; 1: 478–84. 8 Haines A, Kuruvilla S, Borchert M. Bridging the implementation gap between knowledge and action for health. Bull World Health Organ 2004; 82: 724–31. 9 Volmink J, Grobler L, Marais B. Which interventions are effective for increasing the proportion of health professionals practicing in underserved areas? Cape Town, South Africa: Medical Research Council, 2006. 10 Lewin SA, Babigumira SM, Bosch–Capblanch X, et al. Lay health workers in primary and community health care: human resource implications from a systematic review of trials. Cape Town, South Africa: Medical Research Council, South Africa; 2006. 11 Atkins D, Briss P, Eccles M, et al. Systems for grading the quality of evidence and the strength of recommendations II: pilot study of a new system. BMC Health Services Research. 2005; 5: 25. 12 Atkins D, Best D, Briss PA, et al, for the Grade Working Group. Grading quality of evidence and strength of recommendations. BMJ 2004; 328: 1490. 13 Chaix–Couturier C, Durand–Zaleski I, Jolly D, Durieux P. Effects of financial incentives on medical practice: results from a systematic review of the literature and methodological issues. Int J Qual Health Care 2000 Apr; 12: 133–42. 14 Gosden T, Forland F, Kristiansen IS, et al. Capitation, salary, fee-for-service and mixed systems of payment: effects on the behaviour of primary care physicians. Cochrane Database Syst Rev 2000; 3: CD002215. 15 Sempowski IP. Effectiveness of financial incentives in exchange for rural and underserviced area return-of-service commitments: systematic review of the literature. Can J Rural Med 2004; 9: 82–88. 16 Jepson R, Clegg A, Forbes C, Lewis R, Sowden A, Kleijein J. The determinants of screening uptake and interventions for increasing uptake: a systematic review. Health Technol Assess 2000; 4: 1–133. 17 Stone EG, Morton SC, Hulscher ME, et al. Interventions that increase use of adult immunization and cancer screening services: a meta-analysis. Ann Intern Med 2002; 136: 641–51. 18 Villar J, Carroli G, Khan-Neelofur D, Piaggio G, Gülmezoglu M. Patterns of routine antenatal care for low-risk pregnancy. Cochrane Database Syst Rev 2001; 4: CD000934. 19 Kane RL, Shamliyan T, Mueller C, Duval S, Wilt TJ. Nurse staffing and quality of patient care. Minneapolis, MN, USA: US Agency for Healthcare Research and Quality, 2007. 674 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 Lang TA, Romano P, Hodge M, Kravitz R, Olson V. Nurse–patient ratios: a systematic review on the effects on nurse staffing on patient, nurse employee and hospital outcomes. J Adv Nurs 2004; 24: 326–37. Sanchez–McCutcheon A, McPhee M, Davidson JM, Doyle–Waters M, Mason S, Winslow W. Evaluation of patient safety and nurse staffing. Ottawa, ON, Canada: Canadian Health Services Research Foundation, 2005. Poissant L, Pereira J, Tamblyn R, Kawasumi Y. The impact of electronic health records on time efficiency of physicians and nurses: a systematic review. J Am Med Inform Assoc 2005; 12: 505–16. Briggs CJ, Capdegelle P, Garner P. Strategies for integrating primary health services in middle- and low-income countries: effects on performance, costs, and patient outcomes. Cochrane Database Syst Rev 2001; 4: CD003318. Zwarenstein M, Bryant W. Interventions to promote collaboration between nurses and doctors. Cochrane Database Syst Rev 2000; 3: CD000072. Wensing M, Wollersheim H, Grol R. Organizational interventions to implement improvements in patient care: a structured review of reviews. Implement Sci 2006; 1: 2. Beney J, Bero L, Bond C. Expanding the role of outpatient pharmacists: effects on health services utilisation, costs, and patient outcomes. Cochrane Database Syst Rev 2000; 3: CD000336. Bower P, Sibbald B. On-site mental health workers in primary care: effects on professional practice. Cochrane Database Syst Rev. 2000; 3: CD000532. Buchan J, Dal Poz MR. Skill mix in the health care workforce: reviewing the evidence. Bull World Health Organ. 2002; 80: 575–80. Horrocks S, Anderson E, Salisbury C. Systematic review of whether nurse practitioners working in primary care can provide equivalent care to doctors. BMJ 2002; 324: 819–23. Laurant M, Reeves D, Hermens R, Braspenning J, Grol R, Sibbald B. Substitution of doctors by nurses in primary care. Cochrane Database Syst Rev 2005; 2: CD001271. McPherson K, Kersten P, George S, et al. A systematic review of evidence about extended roles for allied health professionals. J Health Serv Res Policy 2006; 11: 240–7. Roberts E, Mays N. Accident and emergency care at the primary-secondary interface: a systematic review of the evidence on substitution. London, UK: King’s Fund, 2006. Coomarasamy A, Khan KS What is the evidence that postgraduate teaching in evidence based medicine changes anything? A systematic review. BMJ 2004; 329: 1017. Grimshaw J, Thomas RE, MacLennan G, et al. Effectiveness and efficiency of guideline dissemination and implementation strategies. Health Technol Assess 2004; 8: 1–72. Jamtvedt G, Young JM, Kristoffersen DT, O’Brien MA, Oxman AD. Audit and feedback: effects on professional practice and health care outcomes. Cochrane Database Syst Rev 2003; 3: CD000259. Thomson O’Brien M, Freemantle N, Oxman AD, Wolf F, Davis DA, Herrin J. Continuing education meetings and workshops: effects on professional practice and health care outcomes. Cochrane Database Syst Rev 2001; 2: CD003030. Thomas L, Cullum N, McColl E, Rousseau N, Soutter J, Steen N. Guidelines in professions allied to medicine. Cochrane Database Syst Rev 2000; 2: CD000349. Wensing M, Wollersheim H, Grol R. Organizational interventions to implement improvements in patient care: a structured review of reviews. Implement Sci 2006; 1: 2. Engström S, Foldevi M, Borgquist L. Is general practice effective? A systematic literature review. Scand J Prim Health Care 2001; 19: 131–44. www.thelancet.com Vol 371 February 23, 2008