Quantitative Topographic Anatomy of the D.G. Norman A. Getgood
advertisement

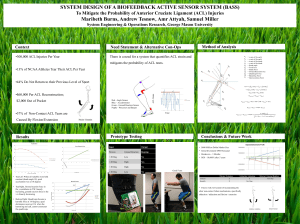
Quantitative Topographic Anatomy of the Femoral ACL Footprint – A Micro-CT Analysis D.G. Norman1* A. Getgood2 J. Bird3 T. Spalding4 & M.A. Williams5 1 School of Engineering, University of Warwick, 2University of Western Ontario, 3University Hospital Lewisham, 4University Hospitals Coventry and Warwickshire NHS Trust, 5WMG INTRODUCTION Anterior Cruciate Ligament (ACL) Reconstruction surgery is the sixth most common orthopaedic surgery in the USA and as a result has become the most studied musculoskeletal system1. Despite this, full recovery after surgery is unsatisfactory with only ≈70% of patients regaining full knee mobility2. Attempting to solve this, clinicians have investigated surgical methods that reconstruct the knee’s original anatomy after rupture3. To accomplish this, physicians need to determine where to attach the newly grafted ligament to the Lateral Intercondylar wall - the ACL footprint. The approach is obviously to place the new ligament in the same location as the old one but this can’t be identified after an ACL rupture so other landmarks are needed. According to Wolff’s Law, there should be thickening (and hence a ridge) around the original ligament attachment area . These ridges, when visible, are often used to place the ligament anatomically. Nevertheless, these ridges, the Lateral Intercondylar Ridge and the Lateral Bifurcate Ridge, (locations illustrated in a diagram published by Ferretti et al 2007) are often not visible and controversy over their actual existence has sparked1. The aim of this project was to use micro-CT to investigate the existence of these ridges to a degree of resolution not explored yet in the literature and validate, or otherwise, their existence. To ensure objectivity, the surface topology was extracted at a high resolution and then used to create relief maps along with other visual methods. Seven cadaveric human knees (66-82 years old) were micro-CT scanned at 60μm and then reconstructed using Nikon’s proprietary software before being imported into VGStudio Max where bone was isolated from tissue SUMMARY Understanding the anatomy of the femoral anterior cruciate ligament (ACL) footprint is important to allow correct placement of the ACL graft. The lateral intercondylar and bifurcate ridges have been proposed as bony landmarks to guide tunnel placement, however, it has been proposed that these ridges can be difficult to find arthroscopically and may be an inconsistent landmark. A new technique utilising high resolution micro CT is described, allowing detailed 3-dimensional quantitative analysis of the femoral footprint of the ACL. Using these 3D images, a qualitative assessment of the landmarks was undertaken by a group of experienced ACL surgeons to determine whether these landmarks can be dependably used to guide correct femoral tunnel placement. Seven cadaveric knees where run through a high-resolution micro-CT scanner following arthroscopic localisation of the centre of the ACL footprint. The images were manipulated using a new extraction technique, leaving the detail of the footprint intact, allowing quantitative analysis of the footprint. These images were displayed on an immersive 3D visualisation wall where experienced ACL surgeons were asked to comment on the presence and morphology of the osseous landmarks. Surface models were created of the distal femur with detailed anatomy of the femoral ACL footprint found to be within 70 microns. A significant variability of the presence and morphology of the osseous landmarks was found within the sample. Qualitative assessment of the ACL footprint also showed significant variability (lateral intercondylar ridge and bifurcate ridge; Fleiss’ Kappa 0.01 and 0.07 respectively). This is the first study to demonstrate the utilisation of micro-CT in the study of the ACL footprint. A novel method of extracting large volumes of data to usable files has been described. Within the study sample, significant variability was observed in the quantitative and qualitative assessment of the osseous landmarks of the femoral ACL footprint. This study has demonstrated that there is a variability in the presence of these landmarks, .therefore other methods to guide placement should be also be used so as to reproducibly place the femoral - _tunnel in the desired position. METHODOLOGY Due to the size of the data (≈40Gb) it was difficult to carry out any analysis. Therefore surface models of the data were created whilst maintaining the resolution. This was done in two processing streams A and B (see diagram) with ‘A’ being the ACL footprint and ‘B’ being the rest of the femur. Volumes were extracted separately as mesh data and then wrapped using a ‘shrink-wrap function’ to extract a closed surface. Finally, the two surfaces are optimised and merged together to create the finished surface model. The surface models were then rendered with a bony texture and were displayed on an immersive 3D visualisation wall. Then ten expert knee surgeons were asked to rate the presences of both the ridges (e.g. “Is the lateral Intercondylar ridge present in this knee?”) on each of the 7 models using a 5 point Likert scale. Analysis of agreement (using Kappa statistics) was then conducted Validation of the surface extraction method was done by laser scanning a sample femur (baseline scan) and then micro-CT scanning the same femur. The micro-CT scanned femur then underwent the developed surface extraction method. The two scanned surfaces were then compared using a deviation analysis which gives a coloured representation of the differences between the ‘actual’ and ‘processed surface’. This allows us to quantify the error of the developed method. To investigate the morphology of the ACL footprint the surface was turned into a relief map. To accomplish this the surface of the ACL footprint is duplicated and smoothed flat to create a baseline surface. The baseline reference surface is overlaid and matched to the original surface. Finally, a coloured deviation analysis is run, which coloured the original surface based on its distance from the corresponding baseline surface. This creates relative relief maps representing the output data. RESULTS Relief maps of the ACL footprint allow an objective approach to identifying the presence of osseous landmarks. On observing all of the relief maps of the ACL footprint, a significant variability of the presence and morphology of the osseous landmarks existed within this sample indicating that they can’t be used reliably for tunnel placement Data size reduced from 40Gb to 20Mb Surface accurate to 70μm±70μm These models developed from micro-CT data were found to be accurate to 70μm±70μm even though the data size was reduced 2000x! Applications for the finished surface models developed as part of this method include; 3D visualization, 3D Printing, Quantitative analysis, Finite Element Analysis, CAD compatibility for medical device design etc. The presence of the osseous landmarks in this sample were identified from both the relief maps and our surgeons responses and compared with previous findings in the literature. Our results disfavour the current consensus Various Statistical methods used to calculate the agreement between our participants yet all showed that there was no statistical agreement between them! Both graphs showing surgeons ratings of the presence of each osseous landmarks also show a range of responses indicating little agreement. Surgeons didn’t agree on the presents of the osseous landmarks in our sample of knees! Surface models could be visualised on a 3D powerwall 3 Inter-rater agreement tests, for multiply raters, giving the coefficients for ‘fair’ agreement for 10 raters for all of ACL footprints examined for both osseous landmarks. Individual ratings, mean and standard deviation for participants ratings between Absolutely Yes’ to ‘Absolutely No’ for the presence of the lateral Intercondylar ridge in each knee. Individual ratings, mean and standard deviation for participants ratings between Absolutely Yes’ to ‘Absolutely No’ for the presence of the lateral bifurcate ridge in each knee. 3D printing could now be done using the developed surface models CONCLUSIONS This present study has described a technique for quantitatively analysing the femoral ACL footprint anatomy, utilising micro-CT imaging. This method been shown to be accurate and could be used to investigate anatomical features of many regions of interest of the musculoskeletal system. Quantitative and qualitative assessment of the femoral footprint showed significant variability of the presence and orientation of osseous landmarks within the subjects in this study. This does question whether these landmarks can be accurately utilised to guide surgical placement of the femoral tunnel in ACL reconstruction. However, further work must be done to investigate age, gender and race variation in a larger sample population before firm conclusions can be made. We recommend that during ACL reconstruction, accurate femoral tunnel placement should be guided by a range of previously described techniques, to get the optimal result. 1 REFERENCES Ziegler, C.G et al., 2010. Arthroscopically Pertinent Landmarks for Tunnel Positioning in Single Bundle and Double Bundle Anterior Cruciate Ligament Reconstruction. The American Journal of Sports Medicine, 39(6) pp.743-5 2 Shafizadeh S, Huber H, Grote S, Hoeher J, Paffrath T, Tiling T et al (2005) Principles of fluoroscopic-based navigation in ACL reconstruction. Oper Tech Orthop 15:70–75 3 Van Eck, F.C., 2010. Does the lateral intercondylar ridge disappear in ACL deficient patients? KSSTA, 18, pp.1184-1188 4 Ferretti, M. et al., 2007. Osseous Landmarks of the Femoral Attachment of the ACL: An Anatomic Study. Arthroscopy: Arthroscopic. 23(11), 5 Farrow, L.D. et al., 2007. Morphology of the Femoral Intercondylar Notch. Journal of Bone and Joint Surgery, 89, pp. 2150–2155 pp.1218-25 6 Huchinson, M.R., Ash, S.A., 2003. Resident’s Ridge: assessing the cortical thickness of the lateral wall and roof of the intercondylar notch. Arthroscopic. FURTHER WORK Secured funding from 1. Consider Cortical thickening 2. Quantify and map thickening under ligament representing graft forces 3. Further analysis of osseous landmarks 4. Validate ruler technique using multimodality imaging techniques 5. Compare NHS and Micro-CT scans ACKNOWLEDGEMENTS Thanks to Manpreet Dhillon, Pete Thompson, Ercihan Kiraci, Abdul-Hadi Abulrub and John Thornby for their assistance. Also thanks to the WMG internship for their financial support. This work has been presented at the BASK, the ESSKA and the _BCUR conference. Vs