Document 13201754
advertisement

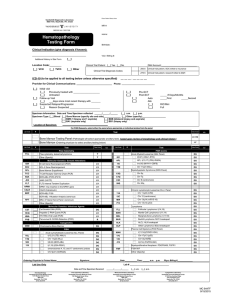
REFERRING CLIENT/COLLECTION CENTER (VPLS) VPLS CLIENT ACCOUNT Nurse/Amb = VUH-VPLS vANDERBILT pATHOLOGY LABORATORY SERVICES (615) 936-0510 Nashville: • Continental U.S .: (800)551-5227 BILL TO: SEND SPECIMEN(S) TO: Client Account Lab Use Only VUMC Case Label 4607 The Vanderbilt Clinic 1301 Medical Center Drive Patient (Billing information must be attached .) Nashville TN 37232-531 0 PATIENT NAME (LAST) (FIRST) SEX DATE COLLECTED TIME COLLECTED 1- I SERUM 0 1- I I I -I PLASMA 0 1-1 L . __ _ _ _ _ _ _ _ 0 3G _, (CLIENT) SAMPLE ID § ~~I URINE FOR LAB USE ONLY 3G MtU## PATIENT ID NUMBER I PHONE NUMBER (M.I.) DATE OF BIRTH DFEMALE DMALE I REFERRING PHYSICIAN RE~p'flif 3G .___ _ _ _ _ _ __, (REFERENCE) OTHER URINE TOTAL VOLUME PLEASE INCLUDE COMPLETE PATIENT BILLING INFORMATION (FACE SHEET) WITH SAMPLE ~R=E~FE~R~R~I~N~G~P~A~T~H~O~L~O~G~I~S~T~=------~-----------------------------ICD-10Code: ________________ REQUIRED PATIENT INFORMATION: D i a g n o s i s : - - - - - - - - - - - - - - Date of Original Dx:_ _ _ ___ PATIENT HISTORY: U AMUMDS U ALL (Circle B or T) LJLymphoma U Plasma Cell Myeloma [_J Myeloproliferative Neoplasm , Specify: [_J Unknown U Other: CLINICAL CONTEXT: U Initial Visit I Diagnosis U Follow-Up Visit U Relapse I Progression- reason suspected : GROWTH FACTOR TREATMENT (Within Last Week): U Yes UNo PRIOR TEST RESULTS: U WBC:-:-------Date/Time: :-::-:-:----U Karyotype I FISH , Specify:_ _ _ _ _ _ _ __ U FLT3 -------LJNPM1 _ _ _ _ _ _ __ LJBCRABL_ _ _ _ _ __ [.:.._jJAK-2 SAMPLE SUBMITTED: Option 1: U Option 2: U Option 3: LJ LJ Bone Marrow Aspirate LJ Peripheral Blood LJ Fluid I Tissue Source: _ _ _ _ _ _ _ _ __ BONE MARROW TESTING PANEL (VU Pathologist will select appropriate tests based upon review of morphology and clinical history) Please submit bone marrow smear if this option is requested A LA CARTE TEST ORDERING (Ordering physician select ancillary testing below) HOLD FOR TESTING (VU Lab: Flow+Grow & Hold) [Client Lab: Fax final orders to 615-343-7961] CYTOGENETICS CYG CHROMOSOME ANALYSIS (Karyotype) FLOW CYTOMETRY ANALYSIS FCL FLOW CYTOMETRY LEUKEMIA I LYMPHOMA MOLECULAR GENETICS AML SNAPSHOT PANEL AMS IGR B-CELL CLONALITY (IGH) B2A BCRABL mRNA COPY NUMBER BC2 BCL-2 GENE REARRANGEMENT BONE MARROW ENGRAFTMENT RFL FL3 FL T3 INTERNAL TANDEM DUPLICATION JK2 JAK2 MUTATION V617F NPM NPM1 INSERTION MUTATION T-CELL CLONALITY TCC FISH ANALYSIS -either order panel or individual markers : Acute Lymphoblastic Leukemia (pre-B ALL Panel) LLP _TEL t(12;21) (TEL-AML1) _11M Chr 11q23 (MLL) _922 t(9;22) (BCR-ABL) _ 119 t(1;19) (E2A-PBX1) 4, 10 and 17 Centromeres (Hyperdiploidy) 9P21 (CDKN2A) FLK Acute Myeloid Leukemia (AML Panel) 821 t(8;21 ) (AML 1-ETO) _ APL APL: t(15;17) (PML-RARA) 116 inv(16) (MYH1 1-CBFB) _11M Chr 11q23 (MLL) MDV Myelodysplastic Syndrome (MDS Panel) C5Q Chr 5q C7Q Chr 7q C8C Chr 8 (centromere) 200 Chr 20 FISH ANALYSIS CONT'D- either order panel or individual markers: 922 Chronic Myeloid Leukemia (CML): t(9,22) Chronic Lymphocytic Leukemia (CLL) Panel LCL 11A Chr 11q23 (ATM) _ 12C Chr 12 (centromere) _ MIR Chr 13q14 (miR15-16) _ P13 Chr 17p13 (p53) LYM Lymphoma FLL Follicular Lymphoma: t(14;1 8) MAN Mantle Cell Lymphoma: t(11; 14) MZL Marg inal Zone Lymphoma : t(11 ; 18) BUR Burkitt Lymphoma : MYC breakapart ALK ALCL: ALK breakapart OLP Other Lymphoma : BCL6 breakapart PMY Plasma Cell Myeloma (PCM Panel) MAN t(11 ;14)(CCND1 -IGH ) _ 17C Chr 17p13 (p53) _ 13C Chr13q14(RB) 414 t(4;14) (FGFR3-IGH) Other Myeloproliferative Neoplasm : PDGFRA/8 OMN FISH M IF FMF OTH OTHER (specify): _ _ _ _ _ _ _ _ _ ___ OTHER TESTS Please write-in test(s) requested:_ _ _ _ _ _ _ _ _ _ __ FOR MORE INFO OR ASSISTANCE: VMC HEMEPATH : 1-800-551 -5227, x7 VPLS ADMIN OFFICE: 1-800-551-5227 , x3 VISIT VPLS ON-LINE AT: www.labVU.com Q Vanderbilt Universitv Medical Center FORM NO. 60-002-664 (REV 07110)