Benefits HMO $25-500 w/Chiro HMO $10-0 w/Chiro
advertisement

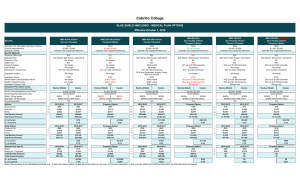
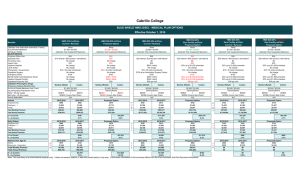
Cabrillo College 2014.10.01 Plan Designs 2014.10.01 Plan Designs 2014/15 Renewal Benefits Calendar Year Deductible Out-of-Pocket Maximum Individual / Family MAJOR MEDICAL HMO $30-20% Zero Facility w/Chiro HMO $25-500 w/Chiro HMO $10-0 w/Chiro PPO 80-E PPO 80-J PPO HDHP -B w/HSA Compatibility None $1,500 per member Calendar Year Copayment Maximum None $2,000 / $4,000 Calendar Year Copayment Maximum None $1,000 / $2,000 Calendar Year Copayment Maximum $300 p/ind; $600 p/fam $1,000 p/ind; $3,000 per fam Calendar Year Out-of-Pocket Max $750 p/ind; $1,500 p/fam $3,000 p/ind; $6,000 per fam Calendar Year Out-of-Pocket Max $2,500 p/ind; $5,000 p/fam $5,000 p/ind or $10,000 per fam Calendar Year Out-of-Pocket Max In Network Out of Network In Network Out of Network In Network $30 $25 $10 Ded waived; $20 50% Ded waived; $30 50% 90% 50% $30/$45 $25/$30 $10/$30 Ded waived; $20 50% Ded waived; $30 50% 90% 50% Physician Office Visit Specialist Visit Out of Network Preventive Care $0 $0 No charge Ded waived; 100% Not Covered Ded waived; 100% Not Covered Ded waived; 100% Not Covered Inpatient Hospital 20% up to $1,500 p/member $500 / Admit No charge 80% $600 p/day 80% $600 p/day 90% $600 p/day Lab & X-Ray No charge No charge 80% 50% 80% 50% 90% 50% Outpatient Surgery No charge No charge 80% $350 p/day 80% $350 p/day 90% $350 p/day $100 (waived if admitted) $150 (waived if admitted) No charge $150 at an Ambulatory Surgery Center; $300 at a Hospital $100 (waived if admitted) Mental Health Care/Substance Abuse 20% up to $1,500 p/member $500 / Admit No charge Ded waived; $20 50% Ded waived; $30 50% 90% Inpatient Hospital Facility 20% up to $1,500 p/member $500 / Admit No charge 80% 50% 80% 50% 90% 50% Outpatient Physician Visit $30 per visit $25 per visit $10 Ded waived; $20 50% Ded waived; $30 50% 90% 50% Navitus / Costco (Mail Order) Navitus / Costco (Mail Order) Navitus / Costco (Mail Order) Navitus / Costco (Mail Order) Navitus / Costco (Mail Order) Generic/Brand Generic/Brand Generic/Brand Generic/Brand Generic/Brand Retail - 30 day supply $9/$35 $9/$35 $5/$10 $7 $25 $9 $35 Mail order - 90 day supply $18/$90 $18/$90 $10/$20 $14 $60 $18 $90 N/A N/A N/A Emergency Room Outpatient Prescription Drugs (At participating Pharmacies only) Annual Deductible Actives $100 copay $100 copay $100 copay $300 p/ind; $600 p/fam 50% Rx w/ Blue Shield Contracted Provider Generic/Brand $7 $25 $14 $60 $2,500 medical deductible must be met before co-pays apply $750 p/ind; $1,500 p/fam 2013 - 2014 2014 - 2015 31 $670 $724 97 2013 - 2014 $721 2014 - 2015 $771 14 2013 - 2014 $910 2014 - 2015 $975 28 2013 - 2014 $910 2014 - 2015 $956 15 2013 - 2014 $807 2014 - 2015 $848 25 2013 - 2014 $643 2014 - 2015 $681 Employee + 1 7 $1,309 $1,417 49 $1,412 $1,512 15 $1,766 $1,890 17 $1,690 $1,778 12 $1,500 $1,578 2 $1,209 $1,281 Family 26 $1,995 87 $1,985 $2,130 15 $2,470 $2,641 9 $2,515 $2,645 11 $2,231 $2,348 3 $1,835 $1,943 Total Monthly Premium 64 $1,838 $77,721 $84,233 233 $311,820 $334,185 44 $76,280 $81,615 54 $76,845 $80,799 38 $54,646 $57,484 30 $23,998 $25,416 $932,652 $1,010,796 $3,741,840 $4,010,220 $915,360 $979,380 $922,140 $969,588 $655,752 $689,808 $287,976 $304,992 Employee Only Total Annual Premium $ ∆ to Current $78,144 $268,380 $64,020 $47,448 $34,056 $17,016 % ∆ to Current 8.4% 7.2% 7.0% 5.1% 5.2% 5.9%