Cabrillo College BLUE SHIELD HMO (SISC) - MEDICAL PLAN OPTIONS
advertisement
 - MEDICAL PLAN OPTIONS")
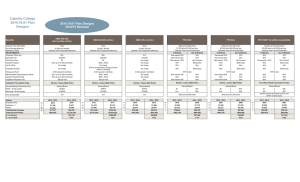
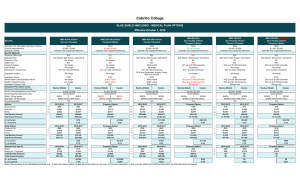
Cabrillo College BLUE SHIELD HMO (SISC) - MEDICAL PLAN OPTIONS Effective October 1, 2016 Benefits Calendar Year Deductible (Individual / Family) Out-of-Pocket Maximum Individual / Family MAJOR MEDICAL Physician Office Visit Specialist Visit Preventive Care Urgent Care Inpatient Hospital Lab & X-Ray Chiropractic / Acupuncture Outpatient Surgery Emergency Room Mental Health Care/Substance Abuse Inpatient Hospital Facility Outpatient Physician Visit Outpatient Prescription Drugs Showing In-Network Benefits Only Rx Out of Pocket Maximum (Ind / Fam) (At participating Pharmacies only) Retail - 30 day supply Mail order - 90 day supply Annual Deductible HMO $10-0 w/Chiro Current / Renewal HMO $20-250 w/Chiro Proposed Option HMO $25-500 w/Chiro Current / Renewal HMO $30-20% Zero Facility w/Chiro Proposed Option HMO $30-20% Zero Facility w/Chiro Current / Renewal HMO $30-20% - SaveNet Zero Facility w/Chiro Proposed Option None $1,000 / $2,000 Calendar Year Copayment Maximum None $1,500 / $3,000 Calendar Year Copayment Maximum None $2,000 / $4,000 Calendar Year Copayment Maximum None $1,500 / $3,000 Calendar Year Copayment Maximum None $1,500 / $3,000 Calendar Year Copayment Maximum None $1,500 / $3,000 Calendar Year Copayment Maximum $10 $10 referral / $30 Access+ self-referral No charge $10 No charge No charge $10 / 30 visits (combined) No charge $100 No charge No charge $10 $20 $20 No charge $20 No charge No charge $20 / 30 visits (combined) No charge $100 $250 / Admit $250 / Admit $20 $25 $25 referral / $30 Access+ self-referral $0 $25 $500 / Admit No charge $10 / 30 visits (combined) $150 at an Ambulatory Surgery Center; $100 $500 / Admit $500 / Admit $25 per visit $30 $30 referral / $45 Access+ self-referral $0 $30 20% up to $1,500 p/member No charge $10 / 30 visits (combined) No charge $150 20% up to $1,500 p/member 20% up to $1,500 p/member $30 per visit $30 $30 referral / $45 Access+ self-referral $0 $30 20% up to $1,500 p/member No charge $10 / 30 visits (combined) No charge $150 20% up to $1,500 p/member 20% up to $1,500 p/member $30 per visit $30 $30 referral / $45 Access+ self-referral $0 $30 20% up to $1,500 p/member No charge $10 / 30 visits (combined) No charge $150 20% up to $1,500 p/member 20% up to $1,500 p/member $30 per visit Navitus (Retail) Navitus (Retail) Navitus (Retail) Navitus (Retail) Navitus (Retail) Actives Costco Navitus (Retail) Costco Costco Costco Costco Costco $1,500 / $2,500 Generic/Brand $1,500 / $2,500 Generic/Brand $2,500 / $3,500 Generic/Brand $2,500 / $3,500 Generic/Brand $2,500 / $3,500 Generic/Brand $2,500 / $3,500 Generic/Brand $5/$10 $0/$10 $0/$20 (Costco Mail Order) N/A $5/$20 $0/$20 $0/$50 (Costco Mail Order) N/A $9/$35 $0/$35 $0/$90 (Costco Mail Order) N/A $9/$35 $0/$35 $0/$90 (Costco Mail Order) N/A $9/$35 $0/$35 $0/$90 (Costco Mail Order) N/A $9/$35 $0/$35 $0/$90 (Costco Mail Order) N/A 2015-2016 2016-2017 Proposed Option 2015-2016 2016-2017 Proposed Option 2015-2016 2016-2017 Proposed Option Employee Only 13 $980 $982 $879 101 $792 $813 $762 40 $742 $762 $735 Employee + 1 13 $1,900 $1,902 $1,718 51 $1,554 $1,594 $1,492 7 $1,453 $1,492 $1,437 Family 11 $2,653 $2,654 $2,411 90 $2,186 $2,243 $2,097 28 $2,043 $2,097 $2,019 Total Monthly Premium 37 $66,623 $66,686 $60,282 242 $355,986 $365,277 $341,784 75 $97,055 $99,640 $95,991 $799,476 $800,232 $723,384 $4,271,832 $4,383,324 $4,101,408 $1,164,660 $1,195,680 $1,151,892 Total Annual Premium $ ∆ to Current $756 -$76,848 $111,492 -$281,916 $31,020 % ∆ to Current 0.1% -9.6% 2.6% -6.4% 2.7% Early Retiree Employee Only Employee + 1 Family Total Monthly Premium Total Annual Premium 4 5 2 11 2015-2016 2016-2017 Proposed Option $980 $1,900 $2,653 $18,726 $224,712 $982 $1,902 $2,654 $18,746 $224,952 $879 $1,718 $2,411 $16,928 $203,136 $ ∆ to Current % ∆ to Current $240 0.1% Retirees Over Age 65 Retiree Retiree plus 1 dependent 8 Total Monthly Premium Total Annual Premium 8 $ ∆ to Current % ∆ to Current 0 10 4 0 14 2016-2017 Proposed Option $792 $1,554 $2,186 $14,136 $169,632 $813 $1,594 $2,243 $14,506 $174,072 $762 $1,492 $2,097 $13,588 $163,056 -$21,816 -9.7% $4,440 2.6% 2015-2016 2016-2017 Proposed Option $674 $1,348 $723 $1,446 $579 $1,158 8 $5,392 $64,704 $5,784 $69,408 $4,632 $55,584 8 $4,704 7.3% 2015-2016 0 -$13,824 -19.9% 0 1 0 1 2016-2017 Proposed Option $742 $1,453 $2,043 $1,453 $17,436 $762 $1,492 $2,097 $1,492 $17,904 $735 $1,437 $2,019 $1,437 $17,244 $468 2.7% 2015-2016 2016-2017 Proposed Option $462 $924 $511 $1,022 $509 $1,018 0 $3,696 $44,352 $4,088 $49,056 $4,072 $48,864 0 $4,704 10.6% 0 -$192 -0.4% -3.7% 2015-2016 -$11,016 -6.3% Note: This summary is for informational purpose only. It does not amend, extend, or alter the current policy in any way. In the event information in this summary differs from the Plan Document, the Plan Document will prevail. -$43,788 -$660 -3.7% 2015-2016 2016-2017 Proposed Option $460 $920 $509 $1,018 $509 $1,018 $0 $0 $0 $0 $0 $0 $0 0.0% $0 0.0% Cabrillo College BLUE SHIELD PPO (SISC) - MEDICAL PLAN OPTIONS Effective October 1, 2016 PPO 80-E Current / Renewal PPO 80-G Proposed Option PPO 80-J Current / Renewal PPO 80-K Proposed Option PPO HDHP -B w/HSA Compatibility Current / Renewal $300 / $600 $1,000 / $3,000 Calendar Year Out-of-Pocket Max In Network Out of Network Ded waived; $20 50% Ded waived; $20 50% Ded waived; 100% Not Covered Ded waived; $20 50% 80% $600 p/day 80% Not Covered Not Covered 80% 1 $500 / $1,000 $2,000 / $4,000 Calendar Year Out-of-Pocket Max In Network Out of Network Ded waived; $20 50% Ded waived; $20 50% Ded waived; 100% Not Covered Ded waived; $20 50% 80% $600 p/day 80% Not Covered Not Covered 80% 1 $750 / $1,500 $3,000 p/ind; $6,000 per fam Calendar Year Out-of-Pocket Max In Network Out of Network Ded waived; $30 50% Ded waived; $30 50% Ded waived; 100% Not Covered Ded waived; $30 50% 80% $600 p/day 80% Not Covered Not Covered 80% 1 $1,000 / $2,000 $3,000 p/ind; $6,000 per fam Calendar Year Out-of-Pocket Max In Network Out of Network Ded waived; $30 50% Ded waived; $30 50% Ded waived; 100% Not Covered Ded waived; $30 50% 80% $600 p/day 80% Not Covered Not Covered 80% 1 $3,000 / $5,200 $5,000 p/ind or $10,000 per fam Calendar Year Out-of-Pocket Max In Network Out of Network 90% 50% 90% 50% Ded waived; 100% Not Covered 90% 50% 90% $600 p/day 90% Not Covered Not Covered 90% 1 Benefits Calendar Year Deductible (Individual / Family) Out-of-Pocket Maximum Individual / Family MAJOR MEDICAL Physician Office Visit Specialist Visit Preventive Care Urgent Care Inpatient Hospital Lab & X-Ray Chiropractic / Acupuncture Outpatient Surgery 80% $350 p/day 2 $100 per visit + 20% (waived if admitted) Ded waived; $20 50% 80% $600 p/day Ded waived; $20 50% Emergency Room Mental Health Care/Substance Abuse Inpatient Hospital Facility Outpatient Physician Visit Outpatient Prescription Drugs Showing In-Network Benefits Only Rx Out of Pocket Maximum (Ind / Fam) (At participating Pharmacies only) Retail - 30 day supply Mail order - 90 day supply Annual Deductible Navitus (Retail) Costco $1,500 / $2,500 (In-network Only) Generic/Brand $7/$25 $0/$25 $0/$60 (Costco Mail Order) $300 p/ind; $600 p/fam Actives $350 p/day 2 80% 80% $100 per visit + 20% (waived if admitted) 80% 50% 80% $600 p/day 80% 50% Navitus (Retail) Costco $1,500 / $2,500 (In-network Only) Generic/Brand $7/$25 $0/$25 $0/$60 (Costco Mail Order) $300 p/ind; $600 p/fam $350 p/day 2 $350 p/day 2 80% 90% $350 p/day 2 $100 per visit + 20% (waived if admitted) Ded waived; $30 50% 80% $600 p/day Ded waived; $30 50% $100 per visit + 20% (waived if admitted) Ded waived; $30 50% 80% $600 p/day Ded waived; $30 50% $100 per visit + 10% (waived if admitted) 90% 50% 90% $600 p/day 90% 50% Navitus (Retail) Navitus (Retail) Rx w/ Blue Shield Contracted Provider Costco $2,500 / $3,500 (In-network Only) Generic/Brand $9/$35 $0/$35 $0/$90 (Costco Mail Order) $750 p/ind; $1,500 p/fam Costco $2,500 / $3,500 (In-network Only) Generic/Brand $9/$35 $0/$35 $0/$90 (Costco Mail Order) $750 p/ind; $1,500 p/fam Combined with Medical OOP Maximum Generic/Brand $9/$35 after the deductible $18/$90 (Blue Shield Mail Order)after the deductible $3,000 medical deductible must be met 2015-2016 2016-2017 Proposed Option 2015-2016 2016-2017 Proposed Option Employee Only 27 $968 $971 $915 14 $861 $864 $852 23 $701 $734 Employee + 1 15 $1,807 $1,814 $1,707 10 $1,607 $1,614 $1,591 4 $1,323 $1,389 Family 10 $2,679 $2,681 $2,521 13 $2,382 $2,387 $2,353 4 $1,998 $2,093 Total Monthly Premium 52 $80,031 $80,237 $75,520 37 $59,090 $59,267 $58,427 31 $29,407 $30,810 $960,372 $962,844 $906,240 $709,080 $711,204 $701,124 $352,884 $369,720 Total Annual Premium 2015-2016 $ ∆ to Current $2,472 -$56,604 $2,124 -$10,080 % ∆ to Current 0.3% -5.9% 0.3% -1.4% Early Retiree Employee Only Employee + 1 Family Total Monthly Premium Total Annual Premium 19 16 0 35 2015-2016 2016-2017 Proposed Option $968 $1,807 $2,679 $47,304 $567,648 $971 $1,814 $2,681 $47,473 $569,676 $915 $1,707 $2,521 $44,697 $536,364 $ ∆ to Current % ∆ to Current $2,028 0.4% Retirees Over Age 65 Retiree Retiree plus 1 dependent 37 Total Monthly Premium Total Annual Premium 40 $ ∆ to Current % ∆ to Current 3 2 1 0 3 2016-2017 Proposed Option $861 $1,607 $2,382 $3,329 $39,948 $864 $1,614 $2,387 $3,342 $40,104 $852 $1,591 $2,353 $3,295 $39,540 -$33,312 -5.8% $156 0.4% 2015-2016 2016-2017 Proposed Option $531 $1,062 $580 $1,160 $576 $1,152 5 $22,833 $273,996 $24,940 $299,280 $24,768 $297,216 5 $25,284 9.2% 2015-2016 0 -$2,064 -0.7% $16,836 4.8% 1 0 0 1 2016-2017 $701 $1,323 $1,998 $701 $8,412 $734 $1,389 $2,093 $734 $8,808 $396 4.7% 2016-2017 Proposed Option $485 $970 $534 $1,068 $568 $1,136 0 $2,425 $29,100 $2,670 $32,040 $2,840 $34,080 0 Note: This summary is for informational purpose only. It does not amend, extend, or alter the current policy in any way. In the event information in this summary differs from the Plan Document, the Plan Document will prevail. 2015-2016 -$564 -1.4% 2015-2016 $2,940 10.1% 0 $2,040 6.4% 2016-2017 2015-2016 2016-2017 $485 $970 $496 $992 $0 $0 $0 $0 $0 0.0%