For report Trust Board Meeting: Wednesday 11 March 2015
advertisement

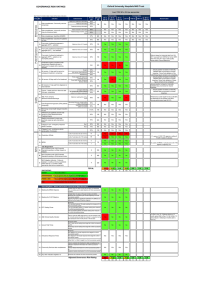
Trust Board Meeting: Wednesday 11th March 2015 TB2015.29 Title Integrated Performance Report – Month 10 Status For report History The report provides a summary of the Trust’s performance against a range of key performance indicators as agreed by the Trust Board. Board Lead(s) Mr Paul Brennan, Director of Clinical Services Key purpose Strategy TB2015.29_Integrated Performance Report M10 Assurance Policy Performance Page 1 of 33 Oxford University Hospitals TB2015.29 Integrated Performance Report Month 10 Executive Summary 1. Key Highlights on performance 2. Areas of exception on performance 3. The percentage of adult inpatients that had a VTE risk assessment in January achieved 95.25% against the standard of 95%. Diagnostic waits over 6 weeks, 24 patients waited over 6 weeks at the end of January, achieving the standard of no more than 1% waiting over 6 weeks. The 18 week RTT Incomplete and Non-Admitted standards were achieved in January at 92.66% and 95.03% against the standards of 90% and 95% respectively. Seven of the eight cancer standards were achieved in December and seven of the eight standards were achieved overall in Q3 meaning the Trust achieved the forecast Monitor score of 4. Patients spending >=90% of time on stroke unit, achieved 73.44% against a standard of 80% in January. MRSA bacteraemia; one case reported in January. Four same sex accommodation breaches reported for January. A/E 4 hour standard of 95%, outturn for January was 83.45%. The 62 day cancer standard was not achieved in December. Delayed Transfers of Care as a percentage of occupied beds is at 11.91% for January against the standard of 3.5%. 18 week RTT Admitted performance was 84.17% against the 90% standard as expected due to the focus on reducing patients waiting over 18 weeks. 8 adult patients waited 52 weeks or more for treatment in January. Staff turnover rate of 13.7%, 3.2% above the standard. Staff sickness absence rate was 3.69%, 0.69% above the standard. The vacancy rate was 7.01%, 2.01% above the standard. Key Standards – in Month 10 3.1. 18 Week RTT, A/E & Cancelled Operations 3.1.1. A/E 95% of patients seen within 4 hours from arrival/transfer/ discharge: Performance at the end of January was 83.45%. February continued to be challenging. 3.1.2. 18 Week Referral to Treatment [RTT] performance: The RTT admitted standard failed in January with performance at 84.17% against the 90% target. The incomplete standard was achieved at 92.66% against the 92% target and the non-admitted standard was achieved at 95.03% against the 95% target. 3.1.3. Eight reported 52 week breaches; of which three patients were admitted in January (two spinal and one plastic patient) and three had non-admitted clock stops (three spinal patients). The remaining two patients, one was admitted in February and one had a follow-up appointment to review treatment options in February. TB2015.29_Integrated Performance Report M10 Page 2 of 33 Oxford University Hospitals TB2015.29 3.2. Activity 3.2.1. Delayed Transfers of Care continue to be a significant concern for the Trust with performance for January at 11.91% against a target of 3.5%. The monthly average for January was 188 delays across the system for Oxfordshire residents. 3.3. Cancer Waits 3.3.1. Cancer waits: 62 day urgent GP referral and screening standard did not achieve the standard in December however all other six cancer standards were achieved. 3.3.2. With the exception of the 62 day standard overall performance for the seven Cancer standards in Q3 was achieved. 4. Monitor Assessment 4.1. The forecast score of 4 for Q3 was achieved. 5. Capacity 5.1. As part of the Winter Plan the Trust was planning to increase acute bed capacity as follows: Bedford/Adams JR 4 beds F Ward Horton 3 beds OCE NOC 10 beds John Warin CH 10 beds 7E 10 beds 5.2. The Bedford/Adams, F Ward and John Warin beds are operational. 5.3. In January staffing levels remained challenging an average of 24 beds per day were closed due to safe staffing, and a decision was made to defer the opening of the additional capacity on 7E. 5.4. In addition, the Tranche 2 Winter Funds (£560,000) have been used to commission capacity in the private sector. Contracts with four nursing homes to procure 29 beds to release beds on the Post-Acute Unit are in place until 31st March 2015. All beds are operational and in use. 6. Workforce 6.1. Turnover increased from 13.25% in December to 13.7% in January and is 3.2% above the KPI target. Reducing staff turnover is a key area of focus. In addition to current recruitment activity, other interventions concerned with improving staff retention include: staff engagement and involvement initiatives; staff recognition and reward; mitigating high cost living; development and implementation of multi-professional Education Training Strategy; implementation of the Leadership and Talent Development Strategic framework; creating and sustaining the right environment. TB2015.29_Integrated Performance Report M10 Page 3 of 33 Oxford University Hospitals 7. TB2015.29 Recommendations The Trust Board is asked to receive the Integrated Performance Report for Month 10. Paul Brennan, Director of Clinical Services Sara Randall, Deputy Director of Clinical Services March 2015 TB2015.29_Integrated Performance Report M10 Page 4 of 33 ORBIT Reporting Trust Board Integrated Performance Report January 2015 At A Glance report Escalation report Data Quality Indicator Graph Legend The data quality rating has 2 components. The first component is a 5 point rating which assesses the level and nature of assurance that is available in relation to a specific set of data. The levels are described in the box below. Rating Required Evidence 1 Standard operating procedures and data definitions are in place. 2 As 1 plus: Staff recording the data have been appropriately trained. 3 As 2 plus: The department/service has undertaken its own audit. 4 As 2 plus: A corporate audit has been undertaken. As 2 plus: An independent audit has been undertaken (e.g. by the Trust's internal or external auditors). 5 Underachieving Standard Plan/ Target Performance The second component of the overall rating is a traffic-light rating to include the level of data quality found through any auditing / benchmarking as below Rating Green Data Quality Satisfactory Amber Data can be relied upon but minor areas for improvement identified. Red Unsatisfactory/significant areas for improvement identified. Page 5 of 33 OUH -At A Glance 2014-15 ORBIT Reporting Operational Access Standards Standard YTD Forecast next Data period Quality RTT - admitted % within 18 weeks 90% Jan-15 84.17% 86.9% 85.2% 3 RTT - non-admitted % within 18 weeks 95% 92% NA Jan-15 Jan-15 Jan-15 95.03% 92.66% 38587 94.7% 91.6% 94.3% 92.5% 38479.3 11.1 6.6 23 18.3 Jan-15 Jan-15 Jan-15 Jan-15 8.67 5.85 27.06 17.98 7.86 5.14 26.1 18.46 8.1 5.3 26.7 18.9 0 Jan-15 10 0 Jan-15 5 RTT - incomplete % within 18 weeks RTT - #waiting on incomplete RTT pathway RTT admitted - median wait RTT - non-admitted - median wait RTT 95th centile for admitted pathways RTT - 95th percentile for non-admitted RTT RTT - # specialties not delivering the admitted standard RTT - # specialties not delivering the nonadmitted standard % Diagnostic waits waiting 6 weeks or more Standard Current Data Period Period Actual YTD Forecast next period Data Quality NA Mar-15 1 2 2 2 Total # of deliveries NA 62% 23% Jan-15 Jan-15 Jan-15 730 65.89% 20.27% 7029 62.9% 21.7% 685.7 64% 20.5% 3 3 5 2 2 3 3 Proportion of Assisted deliveries 15% NA 0% 80% Jan-15 Jan-15 Jan-15 Jan-15 13.84% 0 2.97% 81.58% 15.5% 0 3.7% 79.2% 15.6% 5 4 5 4 0 Jan-15 0 2 5 NA Jan-15 13 112 5 NA Jan-15 15 123 5 0 Jan-15 0 1 5 0% Dec-14 71.12% 66% 69.2% 4 NA 0% Jan-15 Jan-15 72 20.12% 826 25.1% 73 21.3% 5 2 NA Jan-15 78 75.3 2 0% Jan-15 8.22% 13% 8.1% 2 NA Jan-15 76 52 2 0 80% Q4 14-15 Jan-15 4 73.44% 25 82.8% 4.7 82.4% 3 5 0% Jan-15 75.4% 77.5% 72.2% 3 0 5 Jan-15 Jan-15 1 4 7 50 0.7 5 5 5 1% Jan-15 0.25% 1% 0.4% 2 0 Jan-15 3 60 7 4 Zero tolerance RTT waits IP 0 Jan-15 2 163 5.7 4 Zero tolerance RTT waits NP 0 NA Jan-15 Jan-15 3 39 3 No data available 4 2 2 Proportion of normal deliveries Proportion of C-Section deliveries Maternal Deaths 30 day emergency readmission Medication reconciliation completed within 24 hours of admission Medication errors causing serious harm Patient Experience Number of CAS Alerts received by Trust during the month Number of CAS Alerts with a deadline during the month Number of CAS alerts that were closed having breached during the month Dementia CQUIN patients admitted who have had a dementia screen Monthly numbers of complaints received Patient Satisfaction -Response rate (friends & family -Inpatients) Net promoter (friends & family -Inpatients) 5 3.4% 78.9% Number of attendances at A/E depts in a month % <=4 hours A&E from arrival/trans/discharge NA Jan-15 11840 116724 95% Q4 14-15 83.45% 90.4% Last min cancellations - % of all EL admissions 0.5% Jan-15 0.66% 0.5% 0.4% 2 Patient Satisfaction- Response rate (friends & family -ED) Net promoter (friends & family -ED) 0% 0 Jan-15 Jan-15 6.45% 0 5.1% 0 4.2% 0 2 Same sex accommodation breaches 0 Jan-15 0 0 0 NA NA Jan-15 Jan-15 11666 9778 2 3 NA Jan-15 1235 4 % adult inpatients have had a VTE risk assess 95% Q4 14-15 95.25% 94.1% 94.7% 5 NA Jan-15 653 3 Number SIRIs NA Jan-15 7 46 6.3 5 Total number of first outpatient attendances NA 0 0 Jan-15 Jan-15 Jan-15 29.58% 13692 17320 127305 175035 12653.7 16795.7 3 3 2 Number of Patient Falls with Harm Incidents per 100 admissions 0 NA NA Jan-15 Jan-15 Jan-15 2 5.81 4.52 33 5.23 4.86 3.3 5.3 4.7 2 2 3 1st outpatient attends following GP referral 0 Jan-15 10153 101401 9961 2 # acquired, avoidable Grade 3/4 pressure Ulcers NA Jan-15 3 17 3.5 5 Other refs for a first outpatient appointment 0 Jan-15 9032 89393 8488.7 3 0% Jan-15 94.53% 93.3% 93.5% 3 Non-elective FFCEs 0 0 Jan-15 Jan-15 5546 1773 57808 19106 5709.7 1850 2 3 % of Patients receiving Harm Free Care (Pressure sores, falls, C-UTI and VTE) Never Events NA NA Jan-15 Jan-15 1 NA 4 55.6% 1.3 69.2% 5 5 0 0 Jan-15 Jan-15 7563 592 73787 1781 7255.7 326.7 3 3 NA Jan-15 NA NA 3.5% Q4 14-15 11.91% 10.5% 11.2% 5 % patients not rebooked within 28 days zero Urgent cancellations - 2nd time Urgent cancellations Total on Inpatient Waiting List # on Inpatient Waiting List dates less than 18 weeks # on Inpatient Waiting List waiting between 18 and 35 weeks # on Inpatient Waiting List waiting 35 weeks & over % Planned IP WL patients with a TCI date No of GP written referrals Number of Elective FFCEs - admissions Number of Elective FFCEs - day cases Delayed transfers of care: number (snapshot) Delayed transfers of care as % of occupied beds 10966.7 Quality Outcomes Summary Hospital-level Mortality Indicator** Zero tolerance RTT waits AP Ambulance Handovers within 15 minutes Activity Current Data Period Period Actual 5 # patients spend >=90% of time on stroke unit Safety Time to Surgery (% patients having their operation within the time specified according to their clinical categorisation) HCAI - MRSA bacteraemia HCAI - Cdiff Patient Falls per 1000 bed days Cleaning Scores- % of inpatient areas with initial score >92% Flu vaccine uptake 3 Page 6 of 33 Operational Activity Standard Current Data Period Period Actual YTD Forecast next Data period Quality Theatre Utilisation - Total 75% Jan-15 73.34% 72.2% 71.8% 2 Theatre Utilisation - Elective 80% Jan-15 77.92% 76% 76.2% 3 Theatre Utilisation - Emergency 70% Jan-15 59.05% 60.6% 59.8% 2 85% Dec-14 82.71% 78% 80.9% 5 %patients cancer treatment <62-days - Screen 90% Dec-14 89.29% 93.8% 95.5% 5 % patients treatment <62-days of upgrade NA Dec-14 %patients 1st treatment <1 mth of cancer diag 96% Dec-14 96.69% 95.5% 96.7% 5 %patients subs cancer treatment <31days Surg 94% Dec-14 96.55% 95.1% 95.6% 5 Cancer Waits %patients cancer treatment <62-days urg GP Forecast next period Data Quality 75.83% 90% 5 Jan-15 1.78 1.8 5 -7 Jan-15 -5.54 -7 5 3 Jan-15 3 3 5 CIP Performance Compared to Plan 95% Jan-15 90.13% 93% 5 I&E Surplus Margin (%) 1% Jan-15 0.97% 1% 5 Forecast next period Data Quality Current Data Period Period Actual Finance Capital Capital Programme Compared to Plan 90% Jan-15 Financial Risk Capital servicing capacity (times) 1.75 Liquidity ratio (days) defined as Working Capital balance *360/Annual Operating Expenses Monitor Risk Rating ref I&E Standard YTD 5 No data available %patients subs cancer treatment <31-days Drugs %patients subs treatment <31days - Radio 98% Dec-14 100% 100% 100% 5 94% Dec-14 98.7% 89.4% 99.1% 5 %2WW of an urg GP ref for suspected cancer 93% Dec-14 96.05% 94% 94.6% %2WW urgent ref - breast symp 93% Dec-14 98.46% 94.8% 96.8% Workforce Head count/Pay Worked WTE against Plan (displayed as a % of total)** costs Standard Current Data Period Period Actual YTD 0% Jan-15 96.46% 4 Bank usage (displayed as a % of total)** 0% Jan-15 2.16% 5 5 Agency usage (displayed as a % of total)** 0% Jan-15 5.53% 5 5 Total cost of staff ( displayed as a %)** 0% 5% 3% 10.5% 100% 0% 0% Jan-15 Jan-15 Jan-15 Jan-15 Q3 14-15 Q3 14-15 Q3 14-15 102.74% 7.01% 3.69% 13.7% 11.69% 64.19% 80.2% 5 3 5 3 5 4 4 Staff Experience Vacancy rate Sickness absence** Turnover rate Medical Appraisals Non Medical Appraisals Statutory and Mandatory Competence Compliance % staff with up to date Statutory and Mandatory training 13.3% 100% * This measure is collected on a year to date basis and displays the latest available values ** This measure is collected for a 12 month period preceding the latest period shown *** Sickness absence figures shown in period actual reflect the financial year to date Year: 2014-15 Division: Division of Children's & Women's,Division of Clinical Support Services,Division of Corporate Services,Division of Medicine, Rehabilitation & Cardiac,Division of Neuroscience, Orthopaedics, Trauma & Specialist Surgery,Division of Operations & Service Improvement,Division of Research & Development,Division of Surgery & Oncology,Legacy Division of Cardiac, Vascular & Thoracic,Legacy Division of Musculoskeletal and Rehabilitation,TRUST,Trust-wide only,Unknown Directorate: Acute Medicine & Rehabilitation ,Ambulatory Medicine ,Assurance,Biomedical Research,Cardiology, Cardiac & Thoracic Surgery ,Central Trust Services,Chief Nurse Patient Services & Education,Children's ,Children’s,Critical Care, Pre-operative Assessment, Pain Relief and Resuscitation,CRS Implementation,Division of Clinical Support Services,Division of Corporate Services,Division of Medicine, Rehabilitation & Cardiac,Division of Neuroscience, Orthopaedics, Trauma & Specialist Surgery,Division of Operations & Service Improvement,Division of Research & Development,Division of Surgery & Oncology,Estates and Facilities,Finance and Procurement,Gastroenterology, Endoscopy and Theatres (CH),Horton Management,Human Resources and Admin,Legacy Cardiac, Vascular & Thoracic Surgery,Legacy Cardiology,Legacy Division of Cardiac, Vascular & Thoracic,Legacy Division of Musculoskeletal and Rehabilitation,Legacy Rehabilitation & Rheumatology,Legacy- Anaesthetics, Critical Care & Theatres,MARS -Research & Development,Medical Director,Networks,Neurosciences ,OHIS Telecoms & Med Records,Oncology & Haematology ,Oncology & Haematology ,Orthopaedics,Pathology & Laboratories,Pharmacy,Planning & Communications,Private Patients,Radiology & Imaging,Renal, Transplant & Urology,Specialist Surgery ,Strategic Change,Surgery ,Teaching Training and Research,Theatres, Anaesthetics and Sterile Services,Trauma ,Trust wide R&D,Trust-wide only,Unknown,Women's Page 7 of 33 IPF Red Escalation Report FY 2014-15 Capital Programme Compared to Plan What is driving the reported underperformance? Some of the Trust’s capital projects for 2014/15 are starting later than originally anticipated. What actions have we taken to improve performance Standard Current Data Period Period Actual 90% Jan-15 75.83% YTD Forecast next period 90% The capital programme is reviewed regularly by the Business Planning Group. Other schemes will be brought forward from 2015/16 to fill any gap caused by slippage in the 2014/15 projects. Expected date to meet standard Lead Director The Trust expects to spend its planned capital funding in full by the end of the year. Director of Finance & Procurement Page 8 of 33 IPF Red Escalation Report FY 2014-15 RTT - admitted % within 18 weeks What is driving the reported underperformance? What actions have we taken to improve performance Standard Current Data Period Period Actual YTD Forecast next period 90% Jan-15 84.17% 86.9% 85.21% Admitted performance continues Regular meetings are being held with Divisional to be a challenge with January Teams and the Director of Clinical Services. performance deteriorating. Specialties with significant challenges continue Increase elective cancellations to be: due to emergency pressures as Orthopaedics well as reduced theatre staffing. Spinal Ophthalmology Ear Nose & Throat Urology Neurosurgery Additional theatres lists are being undertaken and external providers are being used to support some surgical activity. Expected date to meet standard Lead Director End of February for Trust level standard with risk limited to Orthopaedics and Spinal. Director of Clinical Services Page 9 of 33 IPF Red Escalation Report FY 2014-15 RTT 95th centile for admitted pathways What is driving the reported underperformance? What actions have we taken to improve performance Standard Current Data Period Period Actual YTD Forecast next period 23 Jan-15 27.06 26.1 26.72 January’s reporting period saw an Regular meetings with the Clinical Divisions and increase in the 95th percentile of the Director of Clinical Services to ensure the admitted waits. sustainable recovery plans are being implemented to reduce and treat those patients waiting over 18 weeks. Expected date to meet standard Lead Director End of February for Trust level with risk limited to Orthopaedics and Spinal. Director of Clinical Services Page 10 of 33 IPF Red Escalation Report FY 2014-15 RTT - # specialties not delivering the admitted standard What is driving the reported underperformance? What actions have we taken to improve performance Standard Current Data Period Period Actual 0 Jan-15 10 YTD Forecast next period Ten services did not achieve the Regular meetings are being held with the admitted standard in January and Clinical Divisions and the Director of Clinical are as follows: Services to ensure the sustainable recovery plans are being implemented to reduce and 1. Trauma & Orthopaedics treat those patients waiting over 18 weeks. 2. Ear, Nose & Throat 3. Ophthalmology 4. Neurosurgery 5. Plastic Surgery 6. Urology 7. Gynaecology 8. Dermatology 9. cardiology 10.Other services Expected date to meet standard Lead Director End of February for Trust level standard with risk limited to Orthopaedics and Spinal. Director of Clinical Services Page 11 of 33 IPF Red Escalation Report FY 2014-15 RTT - # specialties not delivering the non-admitted standard What is driving the reported underperformance? What actions have we taken to improve performance Standard Current Data Period Period Actual 0 Jan-15 5 YTD Forecast next period Five services did not achieve the The Trust-wide standard was met for January. non- admitted standard in January and are as follows: Clinical Divisions do have recovery plans in place to ensure all specialties reduce and treat 1. Trauma & Orthopaedics those patients waiting over 18 weeks. 2. Ear, Nose & Throat 3. Ophthalmology 4. Neurosurgery 5. Cardiology Expected date to meet standard Lead Director Trust-wide standard met. Director of Clinical Services Page 12 of 33 IPF Red Escalation Report FY 2014-15 Zero tolerance RTT waits AP What is driving the reported underperformance? The reduction in patients waiting over 52 weeks continued in January. What actions have we taken to improve performance Standard Current Data Period Period Actual YTD Forecast next period 0 Jan-15 3 60 7 There is an action plan in place to reduce the number of patients waiting. Three patients were admitted and treated in January. The services were: Spinal Surgery (2) Plastic (1) Expected date to meet standard Lead Director Quarter 4 with risk limited to Orthopaedics and Spinal. Director of Clinical Services Page 13 of 33 IPF Red Escalation Report FY 2014-15 Zero tolerance RTT waits IP What is driving the reported underperformance? What actions have we taken to improve performance Standard Current Data Period Period Actual YTD Forecast next period 0 Jan-15 2 163 6 Reduction in the number of There is an action plan in place to reduce the incomplete pathways waiting over number of patients waiting. 52 weeks, this is to be expected when clearing the longest waiting patients as a priority. The services were: Spinal Surgery Service (1) Clinical Genetics (1) Expected date to meet standard Lead Director Quarter 4 with risk limited to Orthopaedics and Spinal. Director of Clinical Services Page 14 of 33 IPF Red Escalation Report FY 2014-15 Zero tolerance RTT waits NP What is driving the reported underperformance? What actions have we taken to improve performance A reduction in the non-admitted patients treated over 52 weeks during January. The services were: Spinal Surgery Service (3) There is an action plan in place to reduce the number of patients waiting. Expected date to meet standard Lead Director Quarter 4 with risk limited to Orthopaedics and Spinal. Director of Clinical Services Standard Current Data Period Period Actual YTD Forecast next period 0 Jan-15 3 39 3 Page 15 of 33 IPF Red Escalation Report FY 2014-15 % <=4 hours A&E from arrival/trans/discharge What is driving the reported underperformance? What actions have we taken to improve performance Standard Current Data Period Period Actual YTD 95% Q4 14-15 83.45% 90.4% Forecast next period January performance continues to The Urgent Care Working group continues to meet weekly, with OCCG, OH, OCC and OUH colleagues to be very challenging. improve patient flow across the system. Escalation is in place with significant focus across all clinical teams to minimize the number of patients waiting over four hours. Additional short terms actions include: Staffing reviewed each shift to ensure safe staffing Extended consultant presence in ED Additional consultant led ward rounds and senior decision makers in ED. Increased theatre capacity to manage trauma flow Enhanced diagnostic and Pharmacy provision Monitoring number of admissions and discharges to transfer lounge Escalation beds opened ECIST report has been received and action plans are being implemented. Expected date to meet standard Lead Director Quarter 4 onwards Director of Clinical Services Page 16 of 33 IPF Red Escalation Report FY 2014-15 % patients not rebooked within 28 days What is driving the reported underperformance? What actions have we taken to improve performance Standard Current Data Period Period Actual YTD Forecast next period 0% Jan-15 6.45% 5.1% 4.22% Additional emergency pressures Clinical teams are focused on forward booking. have imposed delays to rebooking patients. Recruitment of key critical theatre staff is ongoing. Staff recruitment remains a significant issue. Expected date to meet standard Lead Director Quarter 4 2014/15 Director of Clinical Services Page 17 of 33 IPF Red Escalation Report FY 2014-15 Delayed transfers of care as % of occupied beds What is driving the reported underperformance? What actions have we taken to improve performance Performance in January has resulted in an overall deterioration of the performance to 11.91%, (145 patients). Daily whole system teleconference calls remain in place, with escalation to Oxfordshire colleagues when system is on RED. Weekly/Daily Urgent Care Summit meeting with OCCG, OH and OCC colleagues to manage system and winter funding arrangements and reprioritize where necessary. Further work is progressing internally to improve the patient flow and discharge process for all patients. Expected date to meet standard Lead Director Standard Current Data Period Period Actual YTD Forecast next period 3.5% Q4 14-15 11.91% 10.5% 11.15% This system has not agreed a date Director of Clinical Services to achieve this standard. Page 18 of 33 IPF Red Escalation Report FY 2014-15 Theatre Utilisation - Emergency What is driving the reported underperformance? What actions have we taken to improve performance A 2.91% improvement on December’s utilisation performance during January. Internal theatre meetings are in place to review utilisation, work is progressing to develop a standardized approach across the Trust to manage the emergency lists. Expected date to meet standard Lead Director Quarter 4 2014/15 Director of Clinical Services Standard Current Data Period Period Actual YTD Forecast next period 70% Jan-15 59.05% 60.6% 59.79% Page 19 of 33 IPF Red Escalation Report FY 2014-15 Same sex accommodation breaches What is driving the reported underperformance? A male patient (level 2 acuity) was admitted via ED on the stroke pathway. He needed to be nursed, assessed and treated within 4 hours on a Hyper Acute Stroke Unit. The only bed space available was within a female only bay. It was clinically justifiable for him to be nursed in a mixed bay. The female patients were either acuity level 1 or 0. It was therefore not clinically justifiable for the female patients to be in a mixed bay. A UNIFY return of 4 DSSA breaches was submitted. What actions have we taken to improve performance Standard Current Data Period Period Actual YTD Forecast next period 0 Q4 14-15 4 25 5 Reinforcement and clarification that it is not clinically justifiable for patients with acuity level 1 or 0 to be in mixed sex accommodation during the day. It is acceptable during the night however. Full DSSA RCA will be undertaken. Expected date to meet standard Lead Director This will be presented to the Divisional Nurse and Chief Nurse by 1 April 2015. Chief Nurse Page 20 of 33 IPF Red Escalation Report FY 2014-15 HCAI - MRSA bacteraemia What is driving the reported underperformance? What actions have we taken to improve performance Standard Current Data Period Period Actual YTD Forecast next period 0 Jan-15 1 7 1 An OUH apportioned MRSA positive blood culture was reported in January 2015 from within the MRC division (General Medicine). Awaiting the final agreed action plan from the OCCG A Post Infection Review (PIR) meeting was held on the 12/02/15 following the PIR and it was agreed that the MRSA Bacteraemia was avoidable. meeting held on The likely source of this MRSA bacteraemia was agreed to be 12/02/15.This will be chronic leg ulcers. The patient had multiple co-morbidities including reported in next chronic peripheral vascular disease, STEMI Feb 2014, chronic MRSA month’s clinical osteomyelitis on long term oral clindamycin suppression as governance infection recommended by the Bone Infection Unit, paraplegia secondary to control report. a T12 spinal cord infarct and pressure sores to buttocks present on admission. The following learning points were identified: Prior to bilateral Angioplasty procedure undertaken in interventional radiology, skin preparation was performed using povidone iodine aqueous. This is not in line with Trust guidelines which recommends the use of Chlorhexidine 2% in alcohol for skin preparation.(povidone iodine alcohol is recommended as an alternative to Chlorhexidine 2% for patients allergic/contraindicated) The scheduled Angioplasty was cancelled on > 3 occasions, delaying treatment of chronic MRSA colonised leg ulcers. The patient was receiving long term oral Clindamycin suppression therapy for chronic MRSA osteomyelitis. However the MRSA was confirmed to be resistant to Clindamycin, microbiology advised the medical team no change in antibiotics was necessary. Expected date to meet standard Lead Director The Trust objective of 0 avoidable MRSA bacteraemia has not been Medical Director met, however measures are in place to reduce the likelihood of any further avoidable MRSA bacteraemia for 2014-15. Page 21 of 33 IPF Red Escalation Report FY 2014-15 Vacancy rate What is driving the reported underperformance? What actions have we taken to improve performance Vacancy rates have risen marginally since the previous month. Continued challenges associated with the recruitment and retention within particular staff groups remain. Actions being taken to reduce the vacancy rate are consistent with those associated with current recruitment and retention initiatives (see Turnover rate section). Expected date to meet standard Lead Director Q4 2014/15 Director of Organisational Development and Workforce Standard Current Data Period Period Actual 5% Jan-15 7.01% YTD Forecast next period Page 22 of 33 IPF Red Escalation Report FY 2014-15 Sickness absence** What is driving the reported underperformance? What actions have we taken to improve performance Sickness absence has risen marginally when compared to the previous month. FirstCare, line managers, Occupational Health and HR continue to work closely on day to day absence management. The introduction of First Care absence management has provided improved data quality, which in turn has resulted in higher recorded periods of absence. The appointment of FirstCare has improved the flow and quality of information to line mangers, who have also benefitted from the automation of some of the process. Standard Current Data Period Period Actual 3% Jan-15 3.69% YTD Forecast next period Regular meetings between FirstCare and Divisional representatives have commenced so that information can be reviewed and actions/strategies agreed. Return to work interviews are key in reducing absence. Managers are now prompted to undertake all reviews within seven days. This monitored centrally and become a KPI. Expected date to meet standard Lead Director Q1 2015/16 Director Of Organisational Development and Workforce Page 23 of 33 IPF Red Escalation Report FY 2014-15 Turnover rate What is driving the reported underperformance? All staff groups with the exception of Estates/Ancillary and Healthcare Scientists have experienced a rise in turnover rates since the start of the financial year. What actions have we taken to improve performance Standard Current Data Period Period Actual 10.5% Jan-15 13.7% YTD Forecast next period 13.34% A range of actions is being taken to close the vacancy gap. These include initiatives to apply targeted recruitment and retention incentives, assist staff with travel and access to work, and to improve the opportunities for person al and professional development. Nursing and Midwifery have the highest percentage of leavers (at c38% of the total). The increase in leaver rates for this staff group will adversely affect those for the Trust. Expected date to meet standard Lead Director Q1 2015/16 Director Of Organisational Development and Workforce Page 24 of 33 IPF Red Escalation Report FY 2014-15 Medical Appraisals What is driving the reported underperformance? What actions have we taken to improve performance The medical appraisal system runs for a 6 month period in Q3 and Q4 of each financial year rather than on the rolling basis applied to non-medical appraisal. This means that reporting against a target for a given quarter is extremely difficult as the time periods do not correlate. Whilst it may therefore appear that the medical appraisal indicator is underperforming this is not in fact the case. All doctors have been assigned an appraiser and progress is tracked centrally. The Medical Director’s Office will be able to report the appraisal status of every doctor by 14th April 2014. A compliance rate in excess of 90% is anticipated. All doctors for whom an appraisal is not submitted within the time period will be followed up individually and remedial action taken where necessary. Expected date to meet standard Lead Director April 2014 Medical Director Standard Current Data Period Period Actual 100% Q3 14-15 11.69% YTD Forecast next period 100% Page 25 of 33 IPF Amber Escalation Report FY 2014-15 CIP Performance Compared to Plan What is driving the reported underperformance? What actions have we taken to improve performance Standard Current Data Period Period Actual 95% Jan-15 90.13% YTD Forecast next period 93% There has been slippage on the Divisions are aware they have to make up any start of some Divisional and cross- slippage in the remainder of the year and their Divisional schemes. performance is being monitored monthly. Regular meetings are being held with Divisional Directors and Divisional General Managers, and a recovery plan is being agreed. Meetings were also held with individual Divisions at the start of November and stretch targets set to offset the shortfall created by the slippage on schemes. There will be significant cost pressures in 2015/16 and savings plans have been drawn up to tackle these. Expected date to meet standard Lead Director Q4 2014/15 Director of Finance & Procurement Page 26 of 33 IPF Amber Escalation Report FY 2014-15 I&E Surplus Margin (%) What is driving the reported underperformance? What actions have we taken to improve performance Standard Current Data Period Period Actual 1% Jan-15 0.97% YTD Forecast next period 1% The under-performance against The Trust currently believes it will meet its key the 1% target surplus is marginal. financial targets for the year but it will be important for the Trust to maintain a tight grip on its expenditure and for Divisional mitigating actions to be implemented effectively. Expected date to meet standard Lead Director The financial plan for 2014/15 is Director of Finance & Procurement phased such that the Trust is not expected to generate a 1% surplus until towards the end of the year. Page 27 of 33 IPF Amber Escalation Report FY 2014-15 Last min cancellations - % of all EL admissions What is driving the reported underperformance? What actions have we taken to improve performance Additional emergency pressures and lack of bed capacity have caused a number on elective cancellations in January. A huge amount of work is on-going to improve patient flow and bed capacity throughout the Trust. ECIST action plan is being implemented. Expected date to meet standard Lead Director February 2015 Director of Clinical Services Standard Current Data Period Period Actual YTD Forecast next period 0.5% Jan-15 0.66% 0.5% 0.45% Page 28 of 33 IPF Amber Escalation Report FY 2014-15 Theatre Utilisation - Total What is driving the reported underperformance? What actions have we taken to improve performance Standard Current Data Period Period Actual YTD Forecast next period 75% Jan-15 73.34% 72.2% 71.76% January has seen a 4.66% Focus continues on productivity for all clinical increase in total theatre utilization teams both on the day and forward booking. compared with December. Recruitment of key critical theatre staff is ongoing. Expected date to meet standard Lead Director Quarter 4 2014/15 Director of Clinical Services Page 29 of 33 IPF Amber Escalation Report FY 2014-15 Theatre Utilisation - Elective What is driving the reported underperformance? What actions have we taken to improve performance Standard Current Data Period Period Actual YTD Forecast next period 80% Jan-15 77.92% 76% 76.24% January has seen a 4.87% increase Clinical teams are focused on improving booking in elective theatre utilization procedures and maximizing productivity. compared to December. Expected date to meet standard Lead Director Quarter 4 2014/15 Director of Clinical Services Page 30 of 33 IPF Amber Escalation Report FY 2014-15 %patients cancer treatment <62-days urg GP ref What is driving the reported underperformance? What actions have we taken to improve performance Capacity at ‘front end’ of pathways to see patients within the 2 week target is quite often limited, and demand is very often hugely variable. Capacity and variability in demand impacts on delivery and reduces the time left within the remaining days of the pathway. Patients choosing to wait longer also significantly impacts on the delivery of this particular target to delay which can’t be adjusted for. Plans in place to increase front end capacity. Working with CCG to increase patient/GP understanding of need to uptake appointments. Working with radiology to match diagnostics to demand. Expected date to meet standard Lead Director February 2015 Director of Clinical Services Standard Current Data Period Period Actual YTD Forecast next period 85% Dec-14 82.71% 78% 80.94% Page 31 of 33 IPF Amber Escalation Report FY 2014-15 %patients cancer treatment <62-days - Screen What is driving the reported underperformance? What actions have we taken to improve performance The screening standard for December failed due to a data/reporting error which has been rectified The standard did achieve actively pursuing change to Open Exeter. Expected date to meet standard Lead Director Standard met Director of Clinical Services Standard Current Data Period Period Actual YTD Forecast next period 90% Dec-14 89.29% 93.8% 95.49% Page 32 of 33 IPF Amber Escalation Report FY 2014-15 # patients spend >=90% of time on stroke unit What is driving the reported underperformance? The figures largely reflect the very busy period of December as many of the patients admitted that month were not discharged until January. We had a higher than average number of new admissions (56 vs. 44 in Nov) coupled with a lack of downstream bed availability. There were also several patients from out of area waiting some time to be repatriated. What actions have we taken to improve performance Standard Current Data Period Period Actual YTD Forecast next period 80% Jan-15 73.44% 82.8% 82.39% Plans are in the process of being developed to improve downstream capacity and increase capacity in ESD. Regrettably, this meant that a significant number of patients were moved to level 4 to accommodate new admissions, thus reducing their time spent on a stroke unit. Additionally, only 5 patients discharged from 5B to ESD, which is a combination of more severe strokes and the limited geographical reach of the service. Expected date to meet standard Lead Director February 2015 Director of Clinical Services Page 33 of 33