For information the Board’s Quality Sub-Committee in the months when Trust

Title
Status
History
Board Lead(s)
Key purpose
Trust Board Meeting: Wednesday 22 January 2014
TB2014.5
Quality Report
For information
This is the monthly Board Quality Report which is considered by the Board’s Quality Sub-Committee in the months when Trust
Board does not meet.
Professor Ted Baker, Medical Director
Strategy Assurance Policy Performance
TB2014.5 Quality Report Page 1 of 18
Oxford University Hospitals TB2014.5
Executive Summary
1. The Board Quality Report (BQR) presents information that is as contemporary as possible, often including the last calendar month.
2. In relation to key quality metrics:
•
2 metrics remain under development (national cleaning score and time to surgery).
•
For 15 (of 54) quality metrics, pre-specified targets have not been achieved and trend data are provided along with brief exception reports.
3. In relation to patient safety and clinical risk:
•
9 SIRI’s were reported in December 2013.
•
A new reporting format is being developed to enable nurse staffing levels to be monitored in near real-time going forward.
4. In relation to Quality Walk Rounds:
•
There were 4 Quality Walk Rounds in December 2013.
5. In relation to clinical effectiveness:
•
The Trust’s SHMI position continues to be favourable (0.95) when compared to HSMR.
•
A further update on the rolling 12 month SHMI (to end-June 2013) should be available to the Board at its meeting on 22 January 2014.
•
A Mortality Review Group has been formed and has now met on three occasions.
•
Implementation of the Trust’s standardised approach to mortality review continues to progress.
6. In relation to CQUIN / Quality Account Priorities:
•
Performance continues to be good against the majority of 2013/14 CQUIN goals and Quality Account Priorities.
•
Evaluation of progress against Quarter 3 targets will be reported in the Board
Quality Report (considered by the Quality Committee) in February 2014.
7. Patient Experience
•
The top positive themes from the Friends and Family Test are:
Positive staff attitude.
Good general quality of care.
Good standard of nursing care.
•
The key themes for improvement across the Trust are
Delays and difficulty in making an appointment.
Poor and uncoordinated discharge.
Staff attitude, behaviour and communication.
Recommendation
The Board is asked to receive this report.
TB2014.5 Quality Report Page 2 of 18
Oxford University Hospitals
Board Quality Report
1. Purpose
TB2014.5
1.1. This paper aims to provide the Board with information on the quality of care provided within the organisation, and on the measures being taken in relation to quality assurance and improvement.
1.2. This Board Quality Report will be received for information by relevant Trust
Committees (Clinical Governance Committee and Trust Management
Executive) following the meeting of the Board.
2. Key Quality Metrics
2.1. A suite of fifty four key quality metrics has been identified for presentation.
These metrics have been chosen as they are clearly linked to the quality of clinical care provided across the organisation and data quality is felt to be satisfactory. Two of these metrics are still under development and are not being presented this month.
2.2. A Quality Dashboard is provided on pages 4 – 5.
2.3. Trend graphs and exception reports are provided from page 6 onwards in relation to metrics where specified thresholds have not been met (‘redrated’) and selected metrics that are amber-rated. Thresholds are drawn from a mixture of sources (national, commissioner and internal). Thresholds in relation to indicators CE16, CE18 and PE04 have been adjusted following feedback from the Quality Committee.
TB2014.5 Quality Report Page 3 of 18
Oxford University Hospitals
BQR
ID
Rating Rating
Last
Period
Descriptor Period Threshold
Source
TB2014.5
Red Amber
PS01
PS02
PS03
PS04
PS05
PS06
97.08%
Green
3
Green
Safety Thermometer (% patients receiving care free of any newly acquired harm) [one month in arrears]
92.88%
Amber
95.31%
Green
9
N/A
45
Green
Amber
Green
Green
Safety Thermometer (% patients receiving care free of any harm - irrespective of acquisition) [one month in arrears]
Number of cases of Clostridium Difficile > 72 hours (cumulative year to date)
VTE Risk Assessment (% admitted patients receiving risk assessment)
Serious Incidents Requiring Investigation (SIRI) reported via STEIS
Number of cases of MRSA bacteraemia > 48 hours (cumulative year to date)
Dec 13
Dec 13
Nov 13
Dec 13
Dec 13
Dec 13
Internal
Internal
National
National
National
95%
91%
95%
N/A
53
1
97%
93%
N/A
N/A
N/A
95.25%
PS07
PS08
PS09
PS10
PS11
PS12
PS13
PS14
PS15
PS17
PS18
PS19
PS20
CE01
PS16
1895
N/A
5.17%
Amber
60
N/A
8
Red
0
Green
85.71%
Amber
96.29%
Green
70.92%
Red
96.1%
Green
Red
Red
Green
Amber
Amber
Amber
Antibiotic prescribing - % prescriptions where indication and duration specified [most recently available figure, undertaken quarterly] admission
Antibiotic prescribing - % compliance with antimicrobial guidelines
[most recently available figure, undertaken quarterly]
% patients receiving stage 2 medicines reconciliation within 24h of
% patients receiving allergy reconciliation within 24h of admission
Total number of incidents reported via Datix
Total number of newly acquired pressure ulcers (category 2,3 and 4) reported via Datix
Falls leading to moderate harm or greater
% of incidents associated with moderate harm or greater
Oct 13
Oct 13
Dec 13
Dec 13
Dec 13
Dec 13
Dec 13
Dec 13
Internal
Internal
Internal
Internal
Internal
Internal
85%
93%
75%
94%
N/A
6.5%
N/A
8
88%
95%
85%
96%
N/A
5%
N/A
7
2.42%
Green
98.66%
Green
16
N/A
0
Green
0.95
N/A
Red
Green
Number of hospital acquired thromboses identified and judged avoidable [two months in arrears]
National Cleaning Score - number of inpatient areas with initial score
< 92%
Sep 13 Internal
% 3rd and 4th degree tears in obstetrics [C&W Division]
Nov 13 Internal
Amber
Green
% radiological investigations achieving 5 day reporting standard [CSS
Division]
Number of CAS alerts received
CAS alerts breaching deadlines at end of month and/or closed during month beyond deadline
Standardised Hospital Mortality Ratio (SHMI) [most recently published figure, quarterly reported as a rolling year ending in month]
Nov 13
Dec 13
Dec 13
Mar 13
Commissioner
Internal
1
N/A
5%
95%
N/A
1
N/A
0
N/A
N/A
98%
N/A
N/A
N/A
CE02
CE03
200
N/A
59.63%
Red
Red
Crude Mortality
Dementia - % patients aged > 75 admitted as an emergency who are screened [one month in arrears]
Nov 13
Nov 13 National
N/A N/A
80% 90%
CE04
CE05
CE06
CE07
76%
Red
92.56%
Amber
88.89%
Green
90.91%
Green
Red
Amber
Green
Green
Statutory and Mandatory Training - % required modules completed
ED - % patients seen, assessed and discharged / admitted within 4h of arrival
Stroke - % patients spending > 90% of admission in specialist stroke environment
Stroke - % patients accessing specialist stroke environment within 4h of arrival
Dec 13 Internal
Dec 13
Dec 13
Dec 13
National
National
National
85% 95%
85%
70%
75%
95%
80%
85%
TB2014.5 Quality Report Page 4 of 18
Oxford University Hospitals
CE08
367
N/A
Transfer Lounge Usage
Nov 13
CE09
CE10
CE11
CE12
CE13
CE14
CE15
CE16
CE17
CE18
CE19
CE20
2.2
Amber
0%
Green
0%
Green
1
Amber
81.55%
Green
4
Amber
0%
Green
89.66%
Amber
100%
Green
1
Amber
438
N/A
Green
Red
N/A
N/A
Green
Amber
Green
Green
Green
Green
Paediatric Surgery - % children having applicable procedures as day case [C&W Division]
Vascular - Median length of stay for patients undergoing elective AAA repair [NOTSS Division]
Vascular - % mortality following elective AAA repair [NOTSS Division]
Cardiology - % patients receiving primary angioplasty within 60 minutes of arrival at hospital [MRC Division] cardiology at tertiary centre [MRC Division]
Division]
Division]
Division]
Division] documented [NOTSS Division]
Cardiology - Mean number of days from referral to admission to
Cardiac surgery-% rate of patients with organ space infections following cardiac surgery via the sternum [MRC Division]
Cardiac Surgery - % mortality following elective primary CABG [MRC
Number of unscheduled returns to theatre within 48 hours [NOTSS
Rheumatology - % relevant patients who have their DAS28 score
Number of unscheduled returns to theatre in gynaecology [C&W
Number of patients admitted to SEU wards from SEU triage [S&O
% SEU patients requiring surgery who receive surgery within 24 hours of decision to operate [S&O Division]
Dec 13 Internal
Nov 13 Internal
Nov 13 Internal
Nov 13 Internal
Dec 13 Internal
Dec 13 Internal
Nov 13 Internal
Dec 13 Internal
Dec 13 Internal
Dec 13 Internal
Nov 13
Internal
CE21
Dec 13 Internal
CE22
CE23
CE24
PE01
PE02
PE03
PE04
PE05
PE06
PE07
PE08
PE09
PE10
96%
Green
64
Green
1
Amber
448
N/A
0
Green
2.87%
Amber
72.4%
Green
21.72%
Green
2.58%
Amber
75
Green
Green
Green
Green
Green
Green
Green
N/A
Green
Neuroscience Intensive Therapy Unit (NITU) readmission rate within
48 hours of discharge [NOTSS Division]
% fractured NOF patients who receive surgery within 36 hours of admission [NOTSS Division]
Amber % deliveries by C-Section [C&W Division]
7 day admission rate following assessment on (and discharge from) paediatric CDU [C&W Division]
Complaints Received
PALS contacts made
Single sex breaches
Friends & Family - Net Promoter Score [one month in arrears]
Friends & Family - proportion extremely likely or likely to recommend [one month in arrears]
Number of complaints received initially graded as RED
71.24%
Green
63.1%
N/A
Green % patients EAU length of stay < 12h [MRC Division]
% Complaints upheld or partially upheld
1
Green
60.71%
Green
Green
Green
Number of legal claims received / inquests opened initially graded as
RED
% patients returning feedback forms in specialist surgery outpatients
[NOTSS Division]
Nov 13 Internal
Nov 13 Internal
Nov 13 Internal
Nov 13 Internal
Oct 13 Internal
Nov 13
Dec 13 National
Nov 13 Internal
Sep 13
Dec 13 Internal
Nov 13 Internal
TB2014.5
N/A N/A
70% 75%
4
5%
3
6%
2
2
4%
5
3%
85% 90%
2
1% 0.5%
4%
1
95% 98%
1
N/A N/A
N/A N/A
2%
Dec 13 Commissioner 70% 72%
Nov 13 Commissioner 33% 23%
4%
63
90% 94%
90
2
N/A N/A
3
65% 70%
N/A N/A
2
2%
70
80
1
2
N/A
45% 60%
How to interpret charts
TB2014.5 Quality Report Page 5 of 18
Oxford University Hospitals TB2014.5
Data are presented in this report in a number of different ways – including statistical process control (SPC) charts, line charts (without confidence intervals / control limits), histograms and cumulative histograms. Graphics have been selected in order to encourage the analysis of trends and to identify when a change in relation to the historical position is likely to be ‘real’ or statistically significant.
SPC charts show a trend line and allow easy reference to the historical mean for that metric at a time at which it was stable and ‘within control’. Where shown, the mean is displayed as a horizontal orange line. In addition, warning limits and control limits are shown where appropriate, above and below the mean. Warning limits are placed at two standard deviations (2SD – dashed black line) and control limits at three standard deviations (3SD – solid black line). If a data point is found beyond the control limit (3SD from the mean) in either direction, the change is statistically significant and is very unlikely to have occurred simply by chance.
There are other patterns within the data that are likely to reflect real change as opposed to random fluctuation – these patterns are known as special cause variations. They include:
2 consecutive points lying beyond the warning limits (unlikely to occur by chance)
7 or more consecutive points lying on the same side of the mean (implies a change in the mean of the process)
5 or more consecutive points going in the same direction (implies a trend)
Patient Safety
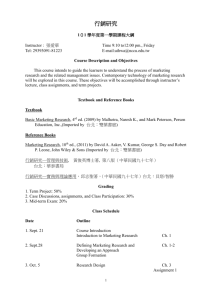
PS02 Safety Thermometer (% patients receiving care free of any harm - irrespective of acquisition) [one month in arrears]
Narrative
TB2014.5 Quality Report Page 6 of 18
Oxford University Hospitals TB2014.5
The proportion of patients receiving care free of new harms remains just below the target threshold of 93%.
(The orange line in the graphic represents average performance and not a RAG threshold).
The proportion of patients without any documented evidence of a pressure ulcer, (ANY origin, category II-IV), harm from a fall in care in the last 72 hours, a urinary infection (in patients with urinary catheter) or new VTE (developed since admission to this organisation). [Owner: A Northover].
Patient Safety
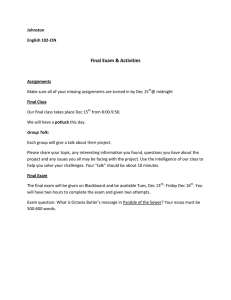
PS04 Serious Incidents Requiring Investigation (SIRI) reported via STEIS Narrative
2 of the 9 SIRIs declared relate to
Hospital Acquired
Thromboses that occurred earlier in the year. Internal investigation has subsequently identified they were potentially avoidable and hence reportable.
The chart shows the number of Serious Incidents Requiring Investigation reported via STEIS (external IT system) per month. If a case is subsequently removed in following consultation with CCG (for example, no harm and SIRI criteria not met after all), the figure will be modified in future graphs. [Owner: N Buchan-Brodie].
Patient Safety
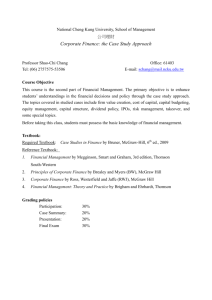
PS09 % patients receiving stage 2 medicines reconciliation within 24h of admission Narrative
TB2014.5 Quality Report Page 7 of 18
Oxford University Hospitals TB2014.5
This will be discussed with the Clinical
Director for pharmacy to identify contributory factors behind December results. It may be that Bank Holidays may have adversely impacted upon this metric.
The chart shows the proportion of inpatients for whom second stage pharmacy-led medicines reconciliation is completed within 24 hours of admission. Spot check audit by pharmacy staff once per month. Approximately 600 patients are included in the audit Trust-wide. Please note that this audit was not performed in May 2013 due to capacity issues in pharmacy. [Owner: P Devenish].
Patient Safety
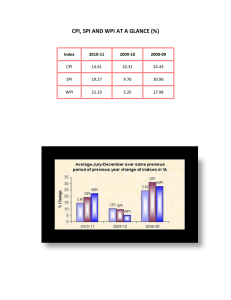
PS11 Total number of incidents reported via Datix Narrative
This minor decrease in reported incidents for a one month period is not considered significant but will continue to be actively monitored.
The baseline (for the purposes of statistical control charts) will be reset once a period of stability has been observed.
The chart shows the number of clinical incidents reported through the Trust’s Datix system, expressed in relation to
Trust activity [Owner: N Buchan-Brodie].
Patient Safety
PS12 % of incidents associated with moderate harm or greater Narrative
TB2014.5 Quality Report Page 8 of 18
Oxford University Hospitals TB2014.5
The proportion of reported incidents is equivalent to our peer organisations but has risen above the local RAG threshold of 5% this month.
The chart shows the proportion of clinical incidents reported through the Trust’s Datix system which was ultimately felt to be associated with moderate harm or greater [Owner: N Buchan-Brodie].
Patient Safety
PS14 Falls leading to moderate harm or greater Narrative
Falls in October 2013 have previously been examined at CGC.
Provisional figures suggest that 9 falls causing moderate harm or greater were reported during
November, and 8 during December
2013. These falls will now be validated independently to assess the level of harm. The graphic will be updated in due course.
Summary findings in relation to these falls over Q3 2013/14 will be used to assist in reviewing and reshaping falls work.
The chart shows the number of inpatient falls leading to harm per month. All falls are reported via the online incident reporting system.
Clinical Effectiveness
CE03 Dementia - % patients aged > 75 admitted as an emergency who are screened
[one month in arrears]
Narrative
TB2014.5 Quality Report Page 9 of 18
Oxford University Hospitals TB2014.5
It has been noted that there is unexpected variation across peer organisations in relation to the nationally published denominator for this indicator giving rise to questions as to its validity. We await further publication of national performance figures.
Elderly patients admitted on a non-elective basis should be screened for dementia using a screening question and / or a simple cognitive test. Performance shown in this graph reflects figures submitted monthly to NHS England. These figures are derived from both EPR and local paper-based systems.
Clinical Effectiveness
CE04 Statutory and Mandatory Training - % required modules completed Narrative
Monitored and actively managed in a number of settings including divisional performance meetings.
Clinical Effectiveness
CE05 ED - % patients seen, assessed and discharged / admitted within 4h of arrival Narrative
TB2014.5 Quality Report Page 10 of 18
Oxford University Hospitals TB2014.5
There have been additional challenges due to the patient complexity and acuity along with increased demands on the service over the winter months.
Noted the Rapid
Nurse Assessment model has improved ambulance turnaround times.
% Patients attending ED who are discharged or admitted within 4 hours of arrival. [Owner: EMT]
Clinical Effectiveness
CE24 7 day admission rate following assessment on (and discharge from) paediatric
CDU [C&W Division]
Narrative
The Division is monitoring performance in this area. The readmission rate has breached an internal
RAG threshold but remains below the historical mean.
Paediatric capacity has been particularly challenging over recent months
(regionally).
Number of patients discharged from CDU and number who are readmitted as emergency inpatients within 7 days to a ward other than CDU.
3. Patient Safety and Clinical Risk
3.1. Information relating to patient safety and clinical risk is provided within the key quality metrics.
TB2014.5 Quality Report Page 11 of 18
Oxford University Hospitals TB2014.5
3.2. Figure 1 below outlines the detail of the 9 Serious Incidents Requiring
Investigation declared during December 2013. The date of the incident should be noted.
3.3. SIRI 2013/044 meets NHS England’s Never Event criteria and is currently under investigation.
Figure 1 .
SIRI ref Division Location
Date of
Incident
Date SIRI
Called Description
2013/044
2013/045
2013/046
2013/047
2013/048
2013/049
C&W
NOTSS
NOTSS
C&W
NOC
Corp
Delivery HGH 26/09/2013 02/12/2013
OHIS 18/12/2013 20/12/2013
Retained vaginal swab following instrumental delivery. Meets
Never Event criteria.
3a 03/12/2013 03/12/2013 Cat 3 pressure ulcer on sacrum.
Fall from bed causing head
Neurosciences 15/12/2013 16/12/2013
Tom's Ward 15/12/2013 19/12/2013 injury.
NAI
Theatres 16/12/2013
04/12/2013
?18/12/2013
Trochar sheath discovered in hip during surgery-retained from previous procedure
Wrong patient identifiable information sent to CCG
2013/050
2013/051
W&C/CSS AICU
MRC
Juniper Ward
HGH
S & O
Haematology
Ward
11/12/2013 18/12/2013 Maternal Death
25/08/2013 19/12/2013 Death following HAT (PE)
2013/052
3.4.
3.5.
09/05/2013 19/12/2013 Death following HAT (PE)
There was no Clinical Risk Management Committee in December 2013. A reviewed process for the closure of SIRI investigations will be implemented in January 2014 as endorsed by the Clinical Governance Committee in
December 2013.
The new SIRI closure process provides a higher level of scrutiny and constructive challenge of draft SIRI reports before submission to the Clinical
Commissioning Group.
3.6. The review process provides an opportunity for the lead investigator and the review panel to discuss the details of the investigation findings, the content of the report, the appropriateness of the recommendations, and to ensure that effective monitoring of effectiveness is considered as part of the recommendations.
Nurse Staffing Levels
3.7. The OUH has, as part of the Shelford Group of hospitals, contributed to the data that has validated the Safer Nursing Care Tool. During 2013, OUH used the tool to review the acuity and dependency of all in-patients in April,
October and December. The data from these exercises have, together with processes of quality assurance and professional judgement, contributed to determining the required levels of nurse establishments.
3.8. This work was supported by the information gathered through the on-going
Divisional Peer Review process and staff focus groups, which highlighted some areas of staff concern related to appropriate nursing staff levels,
TB2014.5 Quality Report Page 12 of 18
Oxford University Hospitals TB2014.5
which supported evidence previously identified through the acuity and dependency review.
3.9. The Trust acknowledges that the process of defining appropriate nurse staffing levels requires the use of evidence based tools moderated by the professional judgement of senior nurses. This is triangulated against human resources and patient quality metrics. The considerations on whether staffing levels are correct are determined not only by the acuity and dependency indicators and metrics, but also the % ratio of registered nurses to care support workers, the ratio of registered nurses to beds and the levels of registered nurses to patients on each shift.
3.10. The Acting Chief Nurse is developing a reporting format with senior nursing staff within the Trust, which will enable the management and monitoring of staff levels by shift in near to real-time, and facilitate teams to mitigate short notice shortfalls and document this through an audit trail. Draft reports are being developed and it is anticipated that these reports will be in use by early 2014/15, and provide reporting both externally on the Trust website and to the Board on a monthly basis.
4. Quality Walk Rounds
4.1 There were 4 quality walk rounds in December 2013. One quality walk round was cancelled at late notice due to Executive Lead (deputy) sickness absence. Another was cancelled due to the late re-scheduling of another meeting and the non-availability of a deputy. Both have been rescheduled.
4.2 Figure 2 reflects the areas within the Trust where a quality walk round was completed.
Figure 2.
Hospital Site Areas Visited
John Radcliffe Hospital
Nuffield Orthopaedic Centre
Kamran’s Ward
Endoscopy
Ward D
John Warin Ward
Churchill Hospital
4.2 Key issues with the potential to affect quality or patient experience identified during the quality walk rounds included concerns regarding: storage and medicines safety and staffing including the challenges of managing vacancies and staffing escalation areas.
4.3 All issues have actions associated with them and these will be monitored through Divisional governance processes.
5. Clinical Effectiveness
5.1 The HSMR for the financial year to date (April 13 – Oct 13) is 93.29 and is currently ranked as ‘better than expected’. Although this is encouraging, it is
TB2014.5 Quality Report Page 13 of 18
Oxford University Hospitals TB2014.5
noted that HSMR figures are often volatile and bear little relation to the
‘rebased’ HSMR for 2013/14 which will not be available until November
2014. SHMI (see below) is not subject to this process of rebasing.
5.2 The latest SHMI was published on 16 October 2013 and is 0.95. There has been a steady reduction since the first SHMI of 1.02 was published in
October 2013. The next release of SHMI data will be on 29th January 2014
(covering the 12 months to June 2013).
6. Mortality Review Group
6.1 The Mortality Review Policy and Toolkit is being considered by the Clinical
Governance Committee on 15th January for final approval.
6.2 Significant progress has been made with the implementation of the standardised mortality review process. Divisional reports on deaths reviewed in Quarter 3 of 2013/14 are due to be considered by Clinical
Governance Committee in February 2014.
6.3 The accurate coding of patients’ comorbidities has a significant effect on mortality indices. This in turn depends on accurate documentation of all diagnoses. The Mortality Review Group are to carry out a review of paper clerking proformas used across the Trust with a view to standardising and improving documentation of co-morbidities, in advance of full EPR adoption.
7. Experience of Patients
7.1 Information relating to the experience of patients is provided within the key quality metrics and related exception reports.
7.2 Table 1 below provides a breakdown of the metrics related to the experience of patients in the month of November 2013.
7.3. The top positive themes from the Friends and Family Test are:
• Positive staff attitude.
• Good general quality of care.
Good standard of nursing care. •
7.4. The key themes for improvement across the Trust are
• Delays and difficulty in making an appointment.
•
•
Poor and uncoordinated discharge.
Staff attitude, behaviour and communication.
TB2014.5 Quality Report Page 14 of 18
Oxford University Hospitals
Table 1.
TB2014.5
Trust overall
75 96
Corporate Not applicable
Not applicable CSS
(CCTDP)
M ED
R
C for both sites
I/P
66
75
95
96
NOTSS
S & O
C & W
74
83
93
95
98
100
1
1
1
3
1
0
16
8
31
20
23
14
434
128
23
69
64
3
4
11
18
1
2
7
N/A
0.06%
0.02%
5%
6%
17%
134
61
19
23
14
9
3
2
3
0.06%
0.05%
0.04%
36%
22%
14%
1
The FFT net promoter score is calculated as follows - proportion of respondents who would be extremely likely to recommend minus proportion of respondents who would not recommend (response categories: “neither likely nor unlikely”, “unlikely” & “extremely unlikely”).
2
In previous reports only formal complaints were included.
TB2014.5 Quality Report Page 15 of 18
Oxford University Hospitals TB2014.5
7.5 The actions and projects to improve patient and carer experience and address the main themes are presented in the table below:
Key Themes Outcome needed Actions Trust Lead
Appointments
Discharge
All routine outpatient appointments within 6 weeks
All urgent and 2 week appointments within 2 weeks
Reduce follow up appointments
Coordinated well planned discharge home
Coordinated well planned transfer of care to community hospitals or social care
Improve and increase patient flow, reduced length of stay and delayed discharges
Improve patient experience and safety
Outpatient
Reprofiling Project
The Discharge
Assurance & Oversight
Group has reviewed and improved the discharge policy and procedures across the entire discharge process within all professional groups
(including the implementing estimated discharge dates on date of admission and process for ordering
TTOs and the requirement for doctors to write up prescriptions before estimated date of discharge).
Improving waiting times for TTOs. Medication dispensing robots have been implemented at the JR and Churchill; the trust is introducing ordering of medications on hand held devices.
The Discharge Liaison
Nurse is leading a peer review of discharge processes and improving processes for communication between care providers. Oxford
Health NHS Foundation
Trust and OUH NHS trust review PALS enquiries/complaints about discharges involving both services.
Timeline and milestones
Live from 18 Nov 2013 with ENT initially rollout to all specialities progressing as plan.
Dashboard to measure improvement
Patient Experience dashboard
Discharge Assurance
Oversight Group lead: group meets monthly
Policy lead: Deputy
Director of Clinical
Services. Policy to be reviewed by TME on 12th
December.
Pharmacy actions lead:
Clinical Director of
Pharmacy.
Robots timescales:
Current activity.
Hand held devices timescales: JR February
2014; Horton June 2014
Peer review and care providers lead: Discharge
Liaison Nurse, Project completion date 31st
October 2014.Trust wide emphasis for Winter
2013/14.
Deputy Director of Clinical
Services
Deputy Director of Clinical
Services
TB2014.5 Quality Report Page 16 of 18
Oxford University Hospitals
Key Themes Outcome needed Actions
Staff attitude and behaviour, communication
Working with and including patients and their families in patients care, including timely information.
Clear communication between hospital departments.
Proactive support to patients and their families to resolve concerns and problems
Customer Care -
service Excellence
Programme
TB2014.5
Timeline and milestones
Good progress is being made. The programme is being developed with close collaboration with the pilot sites and jointly led by the Nursing
Directorate and the
Workforce Directorate.
Task and finish Group formed.
Patient Experience feedback forms produced for the customer care pilot teams in Blue
Outpatients, Radiology and an online survey for
Patient Contact Centre.
To be used from
20/01/2014.
The content of the training will incorporate
Trust Values in Action, baseline patient feedback views from staff in the pilot areas, proactive patient and stakeholder direct and indirect feedback with a particular emphasis on vulnerable patients.
Trust Lead
Safeguarding
Adults and
Patient Services manager
Head of
Organisational
Development
8. Quality Account / CQUIN
8.1 This section sets out performance against the 2013/14 quality priorities defined in the Trust Quality Account.
8.2 The majority of the quality priorities are meeting project timelines. Formal evaluation of Quarter 3 achievements is in process, and will be reported at the
February Quality Committee.
8.3 The 2014/15 CQUIN guidance was released by NHS England in late
December 2013. Discussion around the development of goals for the coming year is underway both internally and with commissioners.
9. Infection Control
9.1 Reported Clostridium Difficile and MRSA bacteremia are within expected limits.
Each reported case undergoes an indepth review, and are discussed at the
Infeciton Control Committee.
9.3 The infection control service reviews all cases of C. diff identified within the
Trust. The majority of the patients who have developed C. diff have recently
TB2014.5 Quality Report Page 17 of 18
Oxford University Hospitals TB2014.5 completed a course of antibiotics for unavoidable infections that required treatment. The OUH Trust remains beneath its ascribed C. diff ceiling.
10. Concerns raised by Staff
10.1 Quality concerns raised by staff outside normal line management routes are reported in the minutes of Clinical Governance Committee, considered by both
Trust Management Executive and the Quality Committee.
10.2 Concerns were raised during the peer review program in relation to the transfer of patients from JR to Churchill sites both in general, and specifically in relation to insulin infusion (which may be stopped during patient transfer with potential for adverse impact if transfer arrangements are prolonged).
11. Recommendations
11.1 The Committee is asked to receive this report.
Professor Edward Baker
Medical Director
Report Prepared By:
Annette Anderson
Head of Clinical Governance
January 2014
TB2014.5 Quality Report Page 18 of 18