EFFICACY OF PEER SUPPORT INTERVENTIONS FOR DEPRESSION: A META-ANALYSIS
advertisement

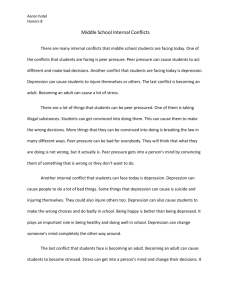
EFFICACY OF PEER SUPPORT INTERVENTIONS FOR DEPRESSION: A META-ANALYSIS Paull N P N. Pfeiffer, Pf iff MD University of Michigan, Dept. of Psychiatry VA Ann Arbor HSR&D/SMITREC Introduction Challenge of Depression 16/6% Lifetime/annual prevalence of major / depressive disorder, U.S. general population1 No. 1 Projected cause of disability worldwide by 20302 5-20 times Risk of suicide compared to general Risk of suicide compared to general population3 $83 billion Cost to U.S. in 20004 1:Kessler JAMA 2003; 2:WHO 2008; 3:CDC & Harris BJP 1997; 4:Greenberg JCP 2003 Current Treatment Limitations Antidepressants and Psychotherapy Small S ll 12 tto moderate d t effect ff t sizes i 1,2 Treatment Time to effectiveness Access resistance3 barriers4 Additional services needed 1: Turner NEJM 2008; 2: Cuijpers BJP 2010; 3: Rush AJP 2006; 4: Chermack Medical Care 2008 Peer-based Peer based Interventions Recommended by DHHS, President’s New Freedom Commission to be included in recovery-base care “Bring together individuals with similar stressors or h l h problems health bl in order d to provide d additional dd l social support” Many varied forms Affordable, Accessible, Available, Acceptable1 1: Kessler Social Policy 1997 Question of Efficacy Prior reviews show limited/mixed / evidence in: General Alcohol medical conditions (i(i.e. e cancer)1 dependence: Alcoholics Anonymous2 Serious Mental Illness: Recovery Inc (now international) GROW3, DBSA international), No prior systematic reviews for depression--likely limits psychiatrist referrals to services4 1: Barlow Int J Group Psychother 2000; 2: Ferri Cochrane 2006; 3: Davidson Clin Psychol-Sci Prac 1999; 4: Powel Psych Services 2000 Methods Study Inclusion Criteria Randomized controlled trials Depressed indi individuals id als A peer peer-based based intervention compared to either usual care or psychotherapy Pre and post depression measurement Search/Selection Strategy Databases: Medline, Psycinfo, CINAHL, CENTRAL Search terms: terms MeSH and free text te t terms related to Depression and Peer/Self-Help/mutual support Limits: adults, peer-review, clinical trial Also searched reference lists of included studies References f reviewed by 2 independent reviewers Data Abstraction Study population characteristics P Peer intervention i i characteristics h i i Pre and post-depression post depression scores Sources of internal bias (i.e. Quality measures) Randomization procedure Blinding Bli di off raters, t procedure d for f blinding bli di Description of participant drop-outs Analyses Pooled effects (standardized mean difference) DerSimonian Heterogeneity Cochran’s Q test of heterogeneity and I2 “Intention Intention to treat treat” Assumed Laird Random Effects model no change from baseline among dropouts Influence analysis Omitted one study at a time (test for outliers) Analyses Publication bias Contour-enhanced funnels plots, Begg and Mazumdar adjusted rank correlation test, Egger regression asymmetry test Stratified analyses based on gender, age, d depression i measure, blinded bli d d assessmentt Results Figure 1: Selection of Studies Search of Relevant Databases Medline: 203 references PsycINFO: 417 references CENTRAL: 142 references CINAHL: 34 references 194 Duplicates excluded 602 Unique studies t di for f review 457 excluded: not a randomized controlled trial 120 excluded: participants p p not depressed, or baseline depression not reported 10 Studies met inclusion criteria 10 excluded: intervention was not peer support 5 excluded: no usual care or psychotherapy control Table 1. Characteristics of Randomized Trials of Peer Support Interventions for Depression Depression p % Mean Outcome Study N Female Age Primary Study Inclusion criteria Measure Ayen I. et al, 51 100 46-56 BDI > 13, no menstrual period in BDI 2004 (range) last 12 months Peer Support Intervention 12 session weekly PSG Bright JI. et al, l 1999 98 71 46 HSRD > 10 BDI, HRSD 10 session weekly PSG Chen CH. et al, 2000 60 100 29 BDI > 9/10, post-partum BDI Dennis CL.,, 2009 701 100 20-34 (median) EPDS > 9,, post-partum p p EPDS Evans RL. et al, 1995 78 32 54 CES-D > 15, stage II cancer with planned XRT CES-D Kelly JA. et al, 1993 68 0 34 CES-D CES D > 15, HIV positive CES-D CES D 8 session weekly PSG CBT, Usual care Maynard CK. et al, 1993 34 100 45 Depressed women (selfidentified) BDI 12 session weekly PSG CBT, Usual care* Michielin P P. et al, 2007 40 Not reported 56 59 56-59 BDI > 9 9, caregiver for someone with serious mental illness BDI 10 session PSG over 15 weeks CBT Ong Y. et al, 1987 20 85 74 Depressed elderly patients (Feighner research criteria) following inpatient stay Zung depression scale 9 months weekly PSG Usual care Verduyn C. et al, 2003 119 100 30 BDI > 14 , mother of pre-school aged child BDI, HRSD 16 session weekly PSG Control Condition(s) CBT, Usual care CBT 4-5 session weekly PSG Usual care ~10 weeks telephone peer mentor 8 session weekly PSG Usual care CBT, Usual care CBT, Usual care PSG = Peer support group, CBT = group cognitive behavioral therapy, BDI = Beck Depression Inventory, CES-D = Center for Epidemiological Studies Depression scale EPDS = Edinborough Postpartum Depression Scale, HRSD = Hamilton Rating Scale for Depression, HRSD = Hamilton Rating Scale for Depression *P ti t were nott randomized *Patients d i d tto thi this condition diti and d therefore th f it was excluded l d d from f the th meta-analyses t l Peer Support vs. Usual Care SMD (95% CI) Percent Weight Ayen -1.95 (-2.87, -1.02) 9.81 Ch Chen -0.71 0 71 ((-1.23, 1 23 -0.19) 0 19) 16 06 16.06 Evans -0.83 (-1.44, -0.22) 14.45 Kelly -0.70 (-1.36, -0.03) 13.56 Subtotal (I-squared (I squared = 48 48.5%, 5% p = 0 0.121) 121) -0 95 (-1 -0.95 (-1.41, 41 -0.49) -0 49) 53 89 53.89 -0.21 ((-0.37,, -0.05)) 22.06 0.07 (-0.81, 0.95) 10.41 Verduyn -0.25 (-0.91, 0.41) 13.64 Subtotal (I-squared = 0.0%, p = 0.815) -0.21 (-0.36, -0.05) 46.11 Overall (I-squared = 70.8%, p = 0.002) -0.59 (-0.98, -0.21) 100.00 Author of Study Not Blinded Blinded Dennis Ong NOTE: O Weights e g ts are a e from o random a do e effects ects a analysis a ys s -2 -1 Favors Peer Support 0 1 2 Favors Usual Care Peer Support vs. Group CBT Author of Study SMD (95% CI) Percent g Weight Not Blinded 0.60 (0.03, 1.18) 14.42 Bright g (p (professional -led g groups) p ) 0.32 ((-0.30,, 0.95)) 13.07 Bright (paraprofessional -led groups) -0.35 (-1.11, 0.42) 10.22 Evans -0.29 (-0.87, 0.28) 14.47 Kelly -0.36 (-1.01, 0.29) 12.51 Maynard 1.03 (-0.06, 2.12) 5.95 Michielin 0.24 (-0.38, 0.86) 13.19 Subtotal (I -squared = 47.8%, p = 0.074) 0.12 (-0.23, 0.47) 83.82 Verduyn -0.02 (-0.54, 0.49) 16.18 Subtotal (I -squared = .%, p = .) -0.02 (-0.54, 0.49) 16.18 Overall (I -squared = 40.1%, p = 0.111) 0.10 (-0.20, 0.39) 100.00 Ayen Blinded NOTE: Weights are from random effects analysis -2 -1 Favors Peer Support 0 1 2 Favors Group CBT Other Results Intention-to-treat and Influence analyses did not change results No publication bias evident by Egger or Begg test or visuall inspection off funnel f l plot. l Study quality: quality All reported treatment drop-outs 3 of 10 single-blinded 3 of 10 described randomization process Discussion Conclusion DHHS and the President’s New Freedom Commission: peer support should be part of recovery-based mental health care RResults l provide d RCT evidence d to support these h initiatives with regard to depression Limitations Heterogeneity among studies Statistically accounted for by blinding May not be generalizable Usual care and fidelity of group CBT not reported PPotential t ti l for f bias bi in i iindividual di id l studies t di (moderate ( d t quality), publication bias (though not detected), and among reviewers i ((nott bli blinded) d d) Take Homes Peer interventions for depression are underresearched Available evidence suggests peer support may be superior i to t usuall care and d similar i il tto group CBT More research is needed to establish effectiveness and optimal delivery HSR&D/SMITREC Researchers (Valenstein) currently conducting RCT of mutual telephone-based peer support Acknowledgments Collaborators: Marcia Valenstein Mary Rogers J John Piette Michele Heisler